
1. Introduction
Open bite is an abnormal dental condition in which maxillary teeth do not occlude those in the mandible in any mandibular position. This condition could severely affect the ability of patients to develop physiological chewing and affect their quality of life (Guedes et al. Citation2014). Treatment of open bite is challenging for orthodontics practitioners (Smithpeter et al. Citation2010). Almost 25% of actual treatments will relapse, sometimes few days after the end of treatment (Greenlee et al. Citation2011; Foletti et al. Citation2018).
Anterior open bite is commonly associated with tongue thrusting and atypical swallowing (Burford and Noar Citation2003). Many authors have investigated the effect of tongue re-education for the treatment of anterior open bite and showed its positive effect with limited relapses (Smithpeter et al. Citation2010; Van Dyck et al. Citation2015). Tongue re-education is indeed a recognized way to close open bite. However, it is deeply dependent to steady patients’ daily compliance.
The Tongue Right Positioner (TRP) is a sensory-motor tongue stimulation device that rapidly establishes mature swallowing and decreases tongue thrust. It is a non-removable oral device fitted on maxillary molar teeth. In young orthodontic patients, establishing mature swallowing is associated with an increase of antero-posterior diameter of the pharynx (Mauclaire et al. Citation2015). Further studies showed that these previous effects are stable 10 months after TRP removal and are also associated with a stable increase in nasal patency (Mauclaire et al. Citation2017). Finally, TRP treatment is associated with the decrease of Apnea Hypopnea Index of adults with Obstructive Sleep Apnea (Wulleman et al. Citation2019). Our hypothesis is that TRP profoundly changes functional and structural traits of the oropharyngeal area by preventing tongue thrust and probably enhances velo-pharyngo-lingual muscles tone, thereby decreasing risks of sleep apnea. The aim of this study is to investigate the effects of reduced tongue thrust associated with TRP treatment on closure of open bite.
2. Methods
2.1. Patients
10 patients from 3 orthodontic clinics (2 in France and 1 in Japan) have been included in this retrospective case report. All patients suffered of anterior open bite, most with long history of orthodontic treatment before TRP setting (minimum 1 year, maximum 7 years). 8 patients were aged between 9 and 15 years old with an average age of 12,0 ± 2,3 years. Two patients are young adults of 19 and 22 years old.
2.2. TRP treatment
TRP has been fitted by orthodontists for the indication of open bite treatments with atypical swallowing and tongue thrusting. Patients have been followed-up every month and photographs of teeth have been reported in patient’s file.
2.3. Outcomes
Closure of open bite has been assessed by measuring four distances 1) between teeth 12 and 42; 2) between teeth 11 and 41; 3) between teeth 21 and 31 and finally 4) between teeth 22 and 32 (). Distance has been normalized using the length of teeth 11 (n, ). A ratio between normalized variables from picture taken after TRP fitting to picture taken before TRP fitting has been calculated to generate a percentage of closure of open bite. A negative percentage shows shorter distance between teeth during TRP treatment. The average of the four percentages give the percentage of closure of open bite.
Figure 1. Distance measured to assess open bite.
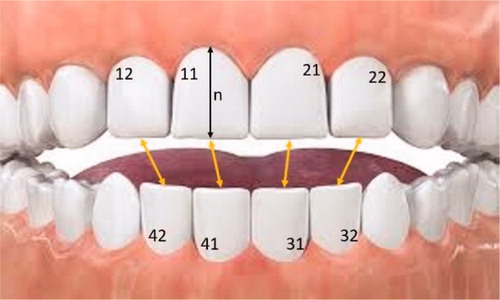
The middle of each teeth is considered as the reference point for distance measurements. n = normalized distance.
3. Results and discussion
The percentage of open bite closure varied from −22% obtained in 1 month to −100% obtained in 12 months. In average the percentage of open bite closure was 61,6 ± 29,2%.
3 out of the 10 patients had complete closure of their open bite after a period of time of minimum 3 months and maximum of 12 months, independently from their age. The other patients had an open bite closure percentage between −22 and −62% obtained within 11,5 months.
Based on these data, TRP treatment is associated with a closure of anterior open bite. This closure seems to be fast as complete closure could be obtained within few months.
We hypothesize that TRP activates upper airways protection reflex. It prevents atypical swallowing and stimulates the tongue at rest to ascend toward the palate. This new position prevents the tongue from thrusting and interposing between anterior teeth. Absence of tongue thrust may be the major element favoring closure of open bite as previously shown (Foletti et al. Citation2018). This result suggests that correcting tongue functions and redirecting tongue forces applied inside mouth with TRP quickly changes teeth position. In this process the TRP is expected to be a good appliance to quickly close anterior open bite. No data concerning stability of the closure are presented.
4. Conclusions
Based on these data, TRP treatment is associated with a rapid closure of anterior open bite. Follow-up of these patients will enable assessing the average time of closure of open bite and stability of this closure after TRP removal.
References
- Burford D, Noar JH. 2003. The causes, diagnosis and treatment of anterior open bite. Dental Update. 30(5):235–241.
- Foletti J-M, Antonarakis GS, Galant C, Courvoisier DS, Scolozzi P. 2018. Is atypical swallowing associated with relapse in orthognathic patients? A retrospective study of 256 patients. J Oral Maxillofac Surg. 76(5):1084–1090.
- Greenlee GM, Huang GJ, Chen SS, Chen J, Koepsell T, Hujoel P. 2011. Stability of treatment for anterior open-bite malocclusion: a meta-analysis. Am J Orthod Dentofacial Orthop. 139(2):154–169.
- Guedes RS, Piovesan C, Antunes JLF, Mendes FM, Ardenghi TM. 2014. Assessing individual and neighborhood social factors in child oral healthrelated quality of life: a multilevel analysis. Qual Life Res. 23(9):2521–2530.
- Mauclaire C, Vanpoulle F, Belattar A, Saint-Georges-Chaumet Y. 2017. Importance of the lingual reeducation by the tongue right positioner on the upper airways permeability in young orthodontic patients. Sleep Med. 40(2017):e288.
- Mauclaire C, Vanpoulle F, Saint-Georges-Chaumet Y. 2015. Physiological correction of lingual dysfunction with the “Tongue Right Positioner”: beneficial effects on the upper airways. Int Orthod/Coll Eur D’orthod. 13(3):370–389.
- Smithpeter J, Covell D, Jr, Covell D. 2010. Relapse of anterior open bites treated with orthodontic appliances with and without orofacial myofunctional therapy. Am J Orthod Dentofac Orthop. 137(5):605–614.
- Van Dyck C, Dekeyser A, Vantricht E, Manders E, Goeleven A, Fieuws S, Willems G. 2015. The effect of orofacial myofunctional treatment in children with anterior open bite and tongue dysfunction: a pilot study. Eur J Orthod. 38(3):227–234.
- Wulleman P, Belattar A, Coulson S, Vanpoulle F, Mauclaire C, Saint-Georges-Chaumet Y. 2019. Effet de la rééducation linguale avec Tongue Right Positioner sur le SAOS. Méd Sommeil. 16(1):43.