
1. Introduction
The quantification of gait symmetry is extremely important in several clinical contexts. Among the many indices used to describe gait symmetry, the Harmonic Ratio (HR), which is based on a stride-by- stride spectral analysis of trunk accelerations, is often used (Bellanca et al. Citation2013). Recently, an improved version of this index (iHR) has been proposed, relying on a rigorous mathematical definition and on values ranging from 0 to 100% (Pasciuto et al. Citation2017). The influence of acceleration realignment procedures (Buckley et al. Citation2017), as well as of the number of considered strides and harmonics on HR and/or iHR values have been assessed in the literature, and standardized guidelines have been proposed in this respect (minimum of 20 strides and 20 harmonics should be considered) (Riva et al. Citation2014; Pasciuto et al. Citation2017). Concerning stride segmentation approaches, several methods are usually adopted in the literature, based on different signals (ground reaction forces, pelvis or shank accelerations or angular velocities), thus corresponding to different instants of time within the gait cycle. The whole signal has also been considered, to avoid the propagation of errors due to inaccurate segmentation (Riva et al. Citation2013). Nevertheless, despite its role in the computation of iHR, the impact of the stride segmentation method has never been addressed, especially in people characterized by high gait asymmetry, such as people with lower- limb amputation. Thus, the aim of this study was to investigate the influence of different stride segmentation methods and of the absence thereof on iHR values obtained during gait in people with transfemoral amputation.
2. Methods
2.1. Participants & protocol
This study was granted ethical approval (CPP IDF VI, N° 2014-A01938-39) and seven people with transfemoral amputation (5 males, age: 47.3 ± 9.9 years, mass: 74.5 ± 11.9 kg) gave written informed consent prior to their participation. They were instrumented with a pair of pressure insoles (Novel, 100 Hz) and two inertial measurement units (Xsens, 100 Hz) located on their lower trunk (L4/L5 level) and prosthetic shank. Participants walked a minimum of three times at their self-selected speed along an 8- meter linear pathway. At the beginning of each trial, they were required to stay in a static posture for 3 seconds and to perform a kicking task for synchronization purpose.
2.2. Data processing
Proper alignment of the trunk unit with craniocaudal (CC), anteroposterior (AP), and mediolateral (ML) anatomical axes was ensured through a verticalization procedure during the initial static posture of each trial (Bergamini et al. Citation2014). Only steady state strides were considered by discarding the first and last strides of each trial. The iHR was then computed, for each stride and each anatomical axis, using four different segmentation methods, representative of the state of the art:
Insoles (IS) (used as a reference): based on the timings of initial foot contacts, determined using a 20 N threshold on the insole signals;
Shank (SS): based on local maxima in the measured ML shank angular velocity signals, roughly corresponding to the middle of the swing phase;
Trunk (TS): based on the local maxima in the measured ML lower-trunk angular velocity signals, occurring slightly after initial contacts;
Zijlstra (ZS): based on an algorithm which identifies initial contacts in the AP acceleration measured at the lower-trunk (Zijlstra and Hof Citation2003).
In addition, no stride segmentation (NS) was also considered, corresponding to the calculation of the iHR on the whole signal for each gait trial, from the first to the last initial contacts detected by the insoles.
For each patient and each segmentation method, the medians and interquartile ranges (IQRs) of the iHR were computed. The IQR/median ratio (IMR) was also calculated to estimate the iHR reliability.
2.3. Statistics
A Shapiro-Wilk test was performed on the iHR medians and IMR. According to the results of this test, a one-way Repeated Measures ANOVA, or a Friedman test, was performed to investigate if significant differences existed between IS and the other methods (SS, TS, ZS, NS). Pairwise comparisons were analyzed using post-hoc paired t-tests or Wilcoxon signed-rank tests and considering a Holm-Bonferroni correction. Finally, Pearson’s or Spearman’s correlations were used to investigate correlations between iHR values obtained with IS and the other four methods. The significance level (α) was set to 0.05 for all statistical tests.
3. Results and discussion
A total of 405 strides pertaining to the steady-state phase of gait were analysed.
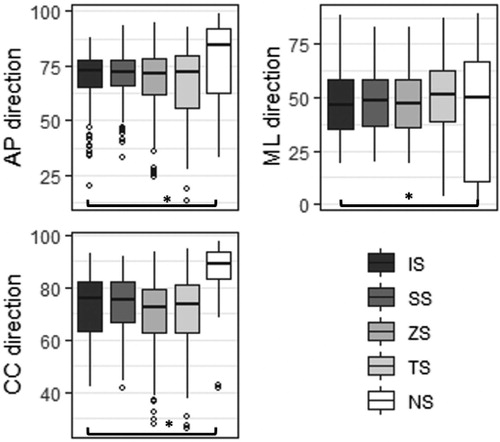
Regarding the iHR obtained with IS, results were consistent with those obtained in the literature for the same population (Pasciuto et al. Citation2017) (). Only iHR scores obtained without segmentation (NS) were significantly different to those obtained using IS, for all three axes (; p < 0.0125). Furthermore, iHR scores derived from SS, TS, and ZS were very strongly and significantly correlated with the reference iHRs (r > 0.97, p < 0.05). Conversely, correlations between IS- and NS-based iHRs were only moderate and not significant in two out of three directions.
Figure 1. Median and IQR values of the iHR scores for each segmentation method and anatomical axis (AP, ML, CC). Significant differences are marked with an asterisk*.
Concerning the iHR reliability, consistently with previous findings (Pasciuto et al. Citation2017), IMR values were found to be higher in the ML than in AP or CC direction (). No statistically significant difference was found between IMRs obtained with IS and any other methods, for each axis. Nevertheless, TS-based iHR IMRs tended to be higher than those obtained with the other segmentation methods.
Table 1. Mean and standard deviations of the iHR IMRs, for each segmentation method and anatomical axis (AP, ML, CC).
4. Conclusions
This study showed that computing iHR on the whole acceleration signal provides significantly different results than using any of the assessed stride segmentation method. When using stride segmentation methods, care should be taken to ensure that the method chosen provides a reliable segmentation for the specific population under study. In particular, special attention must be paid when using pelvis accelerations due to feet impacts attenuation and inherent signal variability at trunk level (Trojaniello et al. Citation2015).
Additional information
Funding
References
- Bellanca JL, Lowry KA, VanSwearingen JM, Brach JS, Redfern MS. 2013. Harmonic ratios: a quantification of step to step symmetry. J Biomech. 46(4):828–831.
- Bergamini E, Ligorio G, Summa A, Vannozzi G, Cappozzo A, Sabatini AM. 2014. Estimating orientation using magnetic and inertial sensors and different sensor fusion approaches: accuracy assessment in manual and locomotion tasks. Sensors. 14(10):18625–18649.
- Buckley C, Galna B, Rochester L, Mazzà C. 2017. Quantification of upper body movements during gait in older adults and in those with Parkinson’s disease: impact of acceleration realignment methodologies. Gait Post. 52:265–271.
- Pasciuto I, Bergamini E, Iosa M, Vannozzi G, Cappozzo A. 2017. Overcoming the limitations of the Harmonic Ratio for the reliable assessment of gait symmetry. J Biomech. 53:84–89.
- Riva F, Bisi MC, Stagni R. 2014. Gait variability and stability measures: minimum number of strides and within-session reliability. Comput Biol Med. 50:9–13.
- Riva F, Toebes MJP, Pijnappels M, Stagni R, van Dieën JH. 2013. Estimating fall risk with inertial sensors using gait stability measures that do not require step detection. Gait Post. 38(2):170–174.
- Trojaniello D, Ravaschio A, Hausdorff JM, Cereatti A. 2015. Comparative assessment of different methods for the estimation of gait temporal parameters using a single inertial sensor: application to elderly, post-stroke, Parkinson’s disease and Huntington’s disease subjects. Gait Post. 42(3):310–316.
- Zijlstra W, Hof AL. 2003. Assessment of spatio- temporal gait parameters from trunk accelerations during human walking. Gait Post. 18(2):1–10.