
1. Introduction
Walking impairments are common and represent a major challenge for rehabilitation after stroke (Dobkin Citation2005). To face functional disability due to foot drop consequences, the gold-standard care combines physical rehabilitation with the use of a passive Ankle Foot Orthosis (AFO) (Fatone et al. Citation2009). This rigid device induces substantial restriction of ankle movements that increase joint stiffness and decrease sensory feedback (Kluding et al. Citation2013; Everaert et al. Citation2013). To prevent these limitations, Functional Electrical Stimulation (FES) has been developed as an alternative approach to address foot drop (Thrasher and Popovic Citation2008). A recent meta-analysis showed positive but comparable effects between AFO and FES (Prenton et al. Citation2018). Recent advances in FES electronic hardware and in connected device-based objective measurement methods could lead to a potential improvement in foot drop rehabilitation. The aim of the current study was to investigate the impact of a new generation of FES devices on walking parameters in stroke patients. We compared FES to their spontaneous walk and AFO assisted-walk by using a connected sole to perform quantitative measurements for kinematic, dynamic and behavioral analysis through pressure measurement.
2. Methods
2.1. Material and preparation
This illustrative case from the REWALK pilot study, concerns a 23-year-old woman with severe hemiparesis who presented a massive and stable foot drop after a stroke (>1 year of Follow-up), in a French rehabilitation center. In daily life, the patient was used to walk without any AFO or FES.
2.2. Protocol and experiments
After a familiarization period, three walking standardized tests were performed: the 6-Minute Walk Test (6MWT), the 10-meter Walk Test (10mWT) and the timed “Up & Go” Test (TUG). The gait parameters: cadence, speed, stride length, swing time, stance time and foot pressure were collected in FES, AFO (standard ankle foot orthosis design pre- fabricated from polypropylene) assisted-walk, and spontaneous walk without any orthosis conditions. The Bioness L300-Go, an electronic orthosis which stimulates the common peroneal nerve, was used in the FES condition. Gait parameters were collected from specific connected sole device (FeetMe®) placed inside the patient’s shoes. Then, patient satisfaction and inputs were collected using a standardized specific questionnaire.
3. Results and discussion
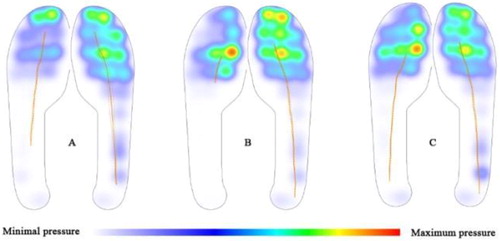
Our descriptive results showed that walking distance is greater in FES and AFO, than no orthesis conditions (322,7 meters (FES); 324,3 meters (AFO); 96,4 meters (no device)). It was also observed that the distribution of foot pressure centers between the impaired limb and the normal limb (mean value on the 6MWT) was more balanced using FES ().
Figure 1. Distribution of foot pressure (KPa) during walking test (A: no device, B: AFO, C: FES).
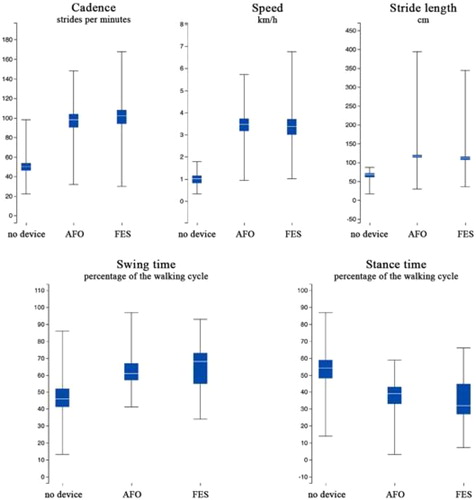
For gait parameters, our results indicated that step length was steadier, with a smaller degree of variability (). The 10mWT showed additional benefits of FES with an increased step length +19.9 cm (+18.1%) for AFO and +40cm (40%) for no device and gait velocity +0.7 km/h (+18.4%) for AFO and +2,7km/h (+70,84%) for no device. Further, perception of wearing an electronic orthosis was positive (VAS 8/10). The patient described her walking performance as smoother and more natural with FES than with AFO.
Figure 2. Gait parameters in the 6MWT.
4. Conclusions
While no consensus were found in the literature about benefits of FES application in post-stroke patient, our illustrative case suggests that FES could be a valuable option to improve gait parameters and quality of life in hemiparetic patients with severe foot drop. The fact that the patient was young (23 yo) and didn’t use any device before the experimentation might be considered as major component of our results. Improvements due to FES would likely be appreciated after a longer habituation or learning period such as after 1, 3 and 6-month follow-up periods. Further investigations are needed to replicate results on a wider population and in ecological conditions.
Acknowledgements
We like to express our gratitude to Alexis Mathieu, FeetMe Monitor® Laurent Baranzelli, Bioness L300 Go for their technical support and Maria Mingorance, Karine Texier, Christophe Lombard for their valuable assistance in carrying out the tests.
References
- Dobkin BH. 2005. Rehabilitation after stroke. N Engl J Med. 352(16):1677–1684.
- Everaert DG, Stein RB, Abrams GM, Dromerick AW, Francisco GE, Hafner BJ, Huskey TN, Munin MC, Nolan KJ, Kufta CV. 2013. Effect of a foot-drop stimulator and ankle-foot orthosis on walking performance after stroke: a multicenter randomized controlled trial. Neurorehabil Neural Repair. 27(7):579–591.
- Fatone S, Gard SA, Malas BS. 2009. Effect of ankle-foot orthosis alignment and foot-plate length on the gait of adults with poststroke hemiplegia. Arch Phys Med Rehabil. 90(5):810–818.
- Kluding PM, Dunning K, O’Dell MW, Wu SS, Ginosian J, Feld J, McBride K. 2013. Foot drop stimulation versus ankle foot orthosis after stroke: 30-week outcomes. Stroke. 44(6):1660–1669.
- Prenton S, Hollands KL, Kenney LPJ, Onmanee P. 2018. Functional electrical stimulation and ankle foot orthoses provide equivalent therapeutic effects on foot drop: a meta-analysis providing direction for future research. J Rehabil Med. 50(2):129–139.
- Thrasher TA, Popovic MR. 2008. Functional electrical stimulation of walking: function, exercise and rehabilitation. Ann Readapt Med Phys. 51(6):452–460.