
Keywords:
1. Introduction
Posture is defined as the orientation of body segments against one another and against gravity. During quiet standing, the body oscillates mostly in the horizontal plane. Stabilometry is the quantification of these oscillations, it is designed to evaluate postural stability. It is usually done by measuring the displacements of the center of pressure using a platform, or by modelling the body center of mass (bCOM) through kinematic or dynamic equipment. Postural stability is studied as a way to assess postural control, which relies on musculoskeletal properties as well as complex neurological patterns and reactions. Multiple postural afferences are involved (proprioceptors, interoceptors, plantar soles, inner ears, eyes). For example, it is well known that closing the eyes leads to greater postural oscillations. Medical history (acute or chronic injuries or diseases, surgeries, etc.) as well as daily habits such as physical exercise have been shown to influence postural control as well. Male professional dancers have better postural control than untrained subjects (Golomer et al. Citation1999), and stabilometry can distinguish professional and amateur dancers (Rein et al. Citation2011). The purpose of this study is to verify the hypothesis that regular dance practice influences healthy women postural stability during quiet standing.
2. Methods
2.1. Population sample
Two groups of fourteen healthy adult women were recruited, reporting no recent pain or injury, constituting the ‘Dancers’ (D) group and the ‘NonDancers’ (ND) group. Subjects of the D group had to practice classical and/or modern dancing regularly for at least 3 years (Rein et al., Citation2011). No significant differences of age, mass and height were reported between the group D (22.7 ± 3.5yo, 56.2 ± 8.0 kg, 158.4 ± 7.0 cm) and the group ND (23.9 ± 2.2yo, 57.0 ± 8.8 kg, 160.3 ± 6.5 cm). Before any experimental involvement, each subject approved the study protocol and signed an informed consent form. The study was approved by the local ethics committee, and complied with the Helsinki declaration.
2.2. Experimental protocol
Wearing underwear, each subject was equipped with 16 spherical markers (8 mm diameter) in order to establish an anthropometric model consistent with De Leva’s method (Marin et al. Citation2017). Each subject was asked to stand in a comfortable position as still as possible, gaze forward focused on a static visual target 3 m away. Two sets of three 30 s videos (Logitech HD Pro C920, 30 Hz, 1920*1080px) were recorded (Marin et al. Citation2017), the first one with eyes opened (EO), the second one with eyes closed (EC).
2.3. Post-treatment protocol
According to Marin et al’s method based on 3D direct linear transformation (2017), each video set was processed in order to obtain the 3D coordinates of the bCOM. The signal was then low-pass filtered (Butterworth first order, 2 Hz cut-off frequency). For each recording, the initial mid-ankle coordinates were chosen as the origin point (O = 0,0,0 mm).
The mean coordinates of the bCOM along the mediolateral (ML), anteroposterior (AP) and vertical axes (respectively X, Y & Z, in mm) were computed, as well as nine stabilisation parameters:
AP & ML ranges (AP_r & ML_r, in mm): differences between the extreme positions of the bCOM;
85% confidence ellipse area (area, in mm2) (Golomer et al. Citation1999);
global, AP & ML excursions (g_e, AP_e, ML_e, in mm): total displacements of the bCOM; - Mean velocities (g_v, AP_v, ML_v, in mm/s).
For each parameter, we calculated the difference between the two conditions (EO-EC) within each group, as well as the difference between the two groups (D-ND) for both conditions. Dependent and independent Student t-tests were used to compare groups and conditions (α = 0.05).
3. Results and discussion
All results were summarized in . Regarding the mean coordinates of the bCOM (X, Y, Z), no significant difference is observed, suggesting that neither vision nor dance practice have any influence on the mean body posture (also referred to as the ‘internal model’).
Table 1. Mean position of the bCOM (X,Y,Z) and stabilisation parameters.
The following paragraphs focus on the stabilisation parameters.
Eyes opened, no significant differences were observed on any parameters between D and ND, suggesting that dance practice does not affect unconstrained postural stability.
Eyes closed, several parameters were significantly higher in ND (AP_r, area, g_v, AP_v), suggesting that dance practice reduces postural sway in more challenging activities. No significant differences were observed regarding any ML parameters. This is consistent with the widely accepted inverted pendulum model, which considers that healthy subjects’ postural sway happens mostly in the sagittal (AP) plane.
illustrates these results comparing both groups velocities (ML_v, AP_v, g_v) in EO and EC.
Figure 1. Comparison of D/ND velocities; bright colors indicate significant differences (p < 0.05).
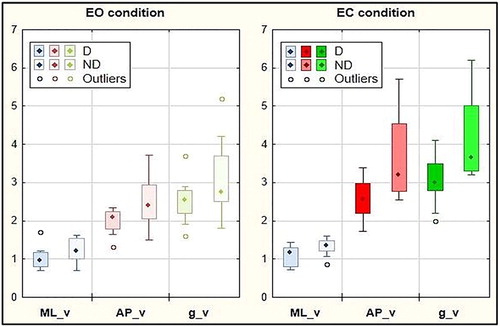
In the ND group, all stabilisation parameters (excepted ML_r) were significantly higher in EC condition. In the D group, most parameters (excepted ML_r, AP_r, area) were also significantly higher in EC condition. However, the increase is much more significant in ND (almost doubled for most parameters, see ).
Those results are consistent with other similar studies assessing the influence of physical activity on postural stability (Schmit et al. Citation2005). We hypothesise that these changes are due to a more efficient prioritization and use of postural afferences (Golomer et al. Citation1999) and/or more efficient postural adjustments resulting in narrower body sway (Rein et al. Citation2011).
4. Conclusions
Regular dance practice seems to improve postural stability, probably by modifying neurological and/or musculoskeletal postural control. Further studies should investigate the use of dance practice as a prevention and rehabilitation tool for health issues altering postural stability.
Acknowledgements
The authors declare no potential conflicts of interests. The authors wish to thank the management of Ecole Supérieure d’Ostéopathie-Paris especially Roger, Christophe and Olivier Caporossi for providing all the necessary equipment for this study; Serge Pin, Laurent Stubbe and Jeanine Sanchez for all their support.
References
- Golomer E, Crémieux J, Dupui P, Isableu B, Ohlmann T. 1999. Visual contribution to selfinduced body sway frequencies and visual perception of male professional dancers. Neurosci Lett. 267(3):189–192.
- Marin T, Houel N, Brikci A, Bertucci W. 2017. Validity of 3D reconstruction of a new tool for postural assessment on a single optical camera. Computer Method Biomech Biomed Eng. 20(suppl 1):125–126.
- Rein S, Fabian T, Zwipp H, Rammelt S, Weindel S. 2011. Postural control and functional ankle stability in professional and amateur dancers. Clin Neurophysiol. 122 (8):1602–1610.
- Schmit J, Regis D, Riley M. 2005. Dynamic patterns of postural sway in ballet dancers and track athletes. Exp Brain Res. 163(3):370–378.