
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.1. Introduction
Treatment of tibial plateau fractures needs stable fixation in order to allow early mobilization and then early full weight bearing. Nowdays, the surgery gestures are been more and more minimally invasive. Minimally invasive surgery is as much about reducing skin incisions as it is about reducing muscle decay and the size and number of implants needed for stabilization.
The most frequent tibial plateau fracture is the Schatzker II type (Kfuri and Schatzker Citation2018) —separation and depressing— which may require a percutaneous locking plate osteosynthesis if the separation is predominant.
A first clinical study shows that there is a decrease in pain using 3.5 mm screws versus. 4.5 mm screws, without mechanical failure (Ehlinger et al. Citation2015). This study aims to prove that there are no mechanical differences in stress distribution between a 4.5 mm and a 3.5 mm construct for distal plate and screws stabilization.
2. Methods
Two models were developed in this work. Their only difference was the screws diameter —3.5 mm and 4.5 mm—.
The 4.5 mm model was built from a clinical case of a tibial plateau fracture with a lateral split depression on a 22-year-old female. The model was composed of four parts: tibial plateau, separated fragment, cement, plate and screws. The geometries were identified and segmented from postoperative CT-scan image with 3D Slicer Software (v4.6.2). Based on the 4.5 mm model, we manually change the screw’s diameter to produce the 3.5 mm model.
The geometries were imported in ANSYS® (16.1, ANSYS, Inc., USA) to be mesh with quadratic tetrahedral elements (Belaid et al. Citation2018) ().
Figure 1. Stress distribution in (a) 4.5 mm vs (b) 3.5 mm distal locking screws.
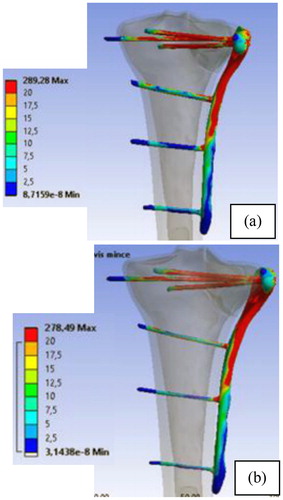
The cancellous bone material behaviour was orthotropic based on the relations between mechanical parameters and local bone density (Rho Citation1996). A titanium alloy material was employed for plate and screws (E = 110 GPa; = 0.3). The applied loading was chosen to simulate a single leg stance during gait, which corresponds to a joint contact force equal to three times the body weight.
The simulation was completed on ANSYS® (16.1, ANSYS, Inc., USA). The stress distribution in the screws and plate was analysed in order to study mechanical effects in terms of rigidity and strength of stabilization of the proximal tibial fracture, with 3.5 mm and 4.5 mm screws.
3. Results and discussion
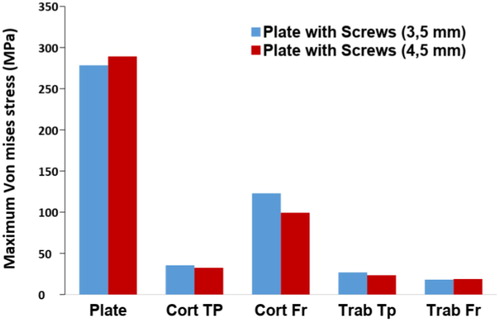
We found that the maximum von Mises stress both models is around 30% of the titanium yield strength. The is no failure risk of the distal locking screws and plate. The shows that there are no significant differences in the maximal von Mises stress in the bone structures. In adequation with the diamond concept (Giannoudis et al. Citation2007), an equivalent mechanical environment allows equivalent bone healing conditions.
Figure 2. Maximum Von Mises stress in: plate, tiblial plateau (TP); fragment (Fr) for cortical (Cort) aned trabecular (Trab) structures.
The reluctance of clinicians to use 3.5 mm screws for tibial plateau fracture is probably due to a misunderstanding with the required use of 4.5 mm screws for plates in shaft fractures (Mukherjee et al. Citation2017).
The interest of the plate in proximal tibia fracture is different from the interest in tibia shaft fractures. In Schatzker II type fractures, it acts as a console. While in shaft fracture it has the role of transmitting stresses under load.
4. Conclusions
As a conclusion, there are no biomechanical differences in stress distribution on medical devices between 4.5 mm and 3.5 mm distal locking screws. As it was already shown that there were no clinically differences neither, it could be interesting to perform prospective and comparative clinical study in order to use 3.5 mm screws.
References
- Belaid D, Vendeuvre T, Bouchoucha A, Brémand F, Brèque C, Rigoard P, Germaneau A. 2018. Utility of cement injection to stabilize split-depression tibial plateau fracture by minimally invasive methods: a finite element analysis. Clin Biomech. 56:27–35.
- Ehlinger M, Adamczewski B, Rahmé M, Adam P, Bonnomet F. 2015. Comparison of the pre-shaped anatomical locking plate of 3.5 mm versus 4.5 mm for the treatment of tibial plateau fractures. Int Orthopaed (Sicot)). 39(12):2465–2471.
- Giannoudis PV, Einhorn TA, Marsh D. 2007. Fracture healing: the diamond concept. Injury. 38:S3–S6.
- Kfuri M, Schatzker J. 2018. Revisiting the Schatzker classification of tibial plateau fractures. Injury. 49(12):2252–2263.
- Mukherjee S, Arambam MS, Waikhom S, Santosha Masatwar PV, Maske RG. 2017. Interlocking nailing versus plating in tibial shaft fractures in adults: a comparative study. J Clin Diagn Res. 11:RC08–RC13.
- Rho J-Y. 1996. An ultrasonic method for measuring the elastic properties of human tibial cortical and cancellous bone. Ultrasonics. 34(8):777–783.