
1. Introduction
For the last 15 years, stroke has been a leading cause of death and adult disability. A stroke is an interruption of blood supply in the brain causing brain cells death. It leads to physical and cognitive impairments, which can affect attention, orientation or memory depending on the damaged part of the brain (Sun et al. Citation2014). Particularly, it concerns patient suffering from hemiparesis for which stroke can induce physical impairment, generally at the upper limb, but can also impact cognitive functions. Thus, post strokes rehabilitation is a key parameter in order to reduce lasting disability. Through intense and frequent focused therapy and training, a significant reduction of lasting disability can be obtained (Teasell and Kalra Citation2005) However, such rehabilitation programs require supervision of trained professionals for a large amount of time, which can be difficult to set up.
Due to the high prevalence of stroke today and its increasing tendency, the use of robotics in rehabilitation program is an area of interest. Many robots providing assistance to reach the therapy’s goal have been developed (Poli et al. Citation2013). In the case of non-physical therapy, Social Assistive Robots (SAR) appear to be a promising tool for post strokes rehabilitation. These robotics solutions provide a contact-free assistance focused on social exchange (motivation speech, encouragements, companionship). Several robots have already been developed and used to provide companionship for elderly people or to help pediatricians study social development and behaviors of children.
The robot NAO (SoftBank Robotics, Paris) is a humanoid robot equipped with different tactile sensors on its hand, feet and head, as well as sonars and inertial units to perceive its environment and locate itself in space. The robot is also equipped with cameras, microphones and speakers to interact with humans, making it able to recognize faces, voices and objects. NAO is already used in healthcare for helping children with diabetes (Coninx et al. Citation2016). The robot teaches children how to manage their diabetes by helping them keeping a diary as well as asking them questions and quizzes when they visit the hospital. This preliminary study focuses on the potential role of a social assistive robot, NAO, in a contact free poststroke rehabilitation therapy. The aim of this work is to propose a physical rehabilitation exercise assisted by NAO for patient suffering from hemiparesis working on arm amplitude, precision and memory.
2. Methods
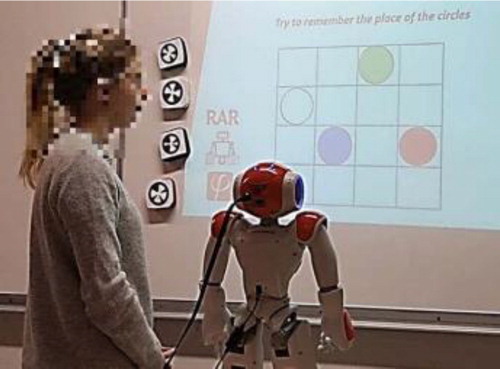
The exercise was based on NaoMarks which are specific landmarks designed to be detected and recognized by NAO robots. In this study NaoMarks were printed on magnetics blocks of different color. In this exercise, a black grid (4x4) was projected on a magnetic board. NAO robot was elevated on a table and placed in front of the screen at 70 cm in order to visualize the complete grid. The patient is seated (or could be standing up, depending of the evolution of the therapy) between the robot and the board. The position of the hemiparesis patient could be adapted according to its dominant side.
At the beginning of the session, NAO explained the exercise. Different color marks appeared on the grid that the patient needed to memorize them. After a specific and adapted time, the color marks disappeared and the patient had to correctly put the NaoMarks associated to the color on the grid. presents the setup of the exercise. During the session several information were computed by NAO in order to evaluate the improvement of the patient during the therapy.
Figure 1. Setup of the exercise. The patient has to correctly put the NaoMarks on a grid based on a color system with the help of NAO.
3. Results and discussion
The main advantage of this exercise is that it could be personalized in function of the patients’ needs. One goal was to work on upper limbs amplitude represented by the distance between the patient and the color marks. Depending on the level of impairment, color marks could be placed closer or further from the patient to reduce, or increase, respectively the patient’s reach. This point could also be improved by a larger grid. However, in this case, the difficulty may be too important for patients on whom therapy needs to focus more on the cognitive aspect. Moreover, the difficulty to reach distant points could also allow to study how the patient compensate motion. These information could be of interest for the therapist, to understand how to intervene on the rehabilitation in order to avoid too much solicitations on the limbs.
The second goal of this exercise is to work on cognitive aspect through the memory. The difficulty could be easily adapted through the apparition time of the color marks, the number or the different colors of the marks. The difficulty of the test could be personalized. Starting with only one or two marks and an apparition time long enough for the patient and ending with several marks and a shorter apparition time.
The third goal of this exercise is to evaluate the precision of the patient. If the exercise focuses on the motion amplitude or the memory, it is possible to evaluate the precision using NAO’s feedback. Precision could be presented as function of the number of mistakes, the distance between the errored NaoMark and the target, and the number of iterations before reaching the goal. Precision could be improved by motivational speeches given by NAO through specific hints about the line or the column of the target. Beyond the previous three objectives, this protocol can give other information to evaluate the progress of patients. As a therapy is generally constituted by multiple session, all the different measured information and the complete time to finish the activity, could be compared between each session. These indications could be used to evaluate the progress but also give a customized motivational feedback to the patient. Indeed, lack of compliance in rehabilitation exercises are due to a lack of motivation (Matarić et al. Citation2007).
This protocol can also be studied through human-robot interaction. Indeed, this exercise is aiming at assisting the therapist. As this exercise could be done with minimal supervision, it allows the therapist to be able to take care of several patients at the same time.
Moreover, in a specific case, this protocol could be performed at home. NAOs feedback could be sent easily to the therapist to follow the evolution of the patient’s performances. This protocol allows also to assist the patient: NAO will provide companionship and a continuous monitoring of the patient thorough the exercise. As a simple humanoid robot, NAO has already proved to be accepted by patient in rehabilitation. In addition to the playful side of NAO, the robot interaction could be personalized and will help the patient performing in his task by correcting his mistakes and giving him specific support.
Nevertheless this protocol must be validated clinically by the therapists and the patients. The user’s profile, preferences and personality can influence the therapy compliance and the degree of implication. The study of Tapus et al. (Citation2008) proposed to develop this idea of adding a user-robot personality matching in their social assistive robot for rehabilitation. This personalization could help to reach better results for this exercise.
4. Conclusions
This paper presents a possible use of social assistive robot in rehabilitation therapy. The exercise proposed allows the clinician to have objective indicators on the patient’s condition. NAO’s companionship and interactions could help the engagement of the patient in his therapy and so improving his compliance.
References
- Coninx A, Baxter P, Oleari E, Bellini S, Bierman B, Blanson Henkemans O, Cañamero L, Cosi P, Enescu V, Ros Espinoza R, et al. 2016. Towards long-term social child-robot interaction: using multi-activity switching to engage young users. J Human-Robot Interact. 1(2):33–53.
- Matarić MJ, Eriksson J, Feil-Seifer DJ, Winstein CJ. 2007. Socially assistive robotics for post-stroke rehabilitation. J Neuroeng Rehabil. 4:5
- Poli P, Morone G, Rosati G, Masiero S. 2013. Robotic technologies and rehabilitation: new tools for stroke patients’ therapy. BioMed Res Int. 2013:1–8.
- Sun JH, Tan L, Yu JT. 2014. Post-stroke cognitive impairment: epidemiology, mechanisms and management. Ann Transl Med. 2(8):80
- Tapus A, Ţăpuş C, Matarić MJ. 2008. User-robot personality matching and assistive robot behavior adaptation for post-stroke rehabilitation therapy. Intel Serv Robotics. 1(2):169–183.
- Teasell RW, Kalra L. 2005. What’s new in stoke rehabilitation. Stroke. 36(2):215–217.