
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.1. Introduction
Falls during daily activities are one of the most important causes of morbidity in the elderly population. Several descriptors exist to quantify instability. However, these descriptors are limited, and sometimes impossible to calculate in realistic walking conditions on uneven surfaces or during multi-contact phases (Bailly et al. Citation2018). One proposed descriptor is the distance between the body center of mass (BCOM) and the minimal moment axis (MMA) of the external contact wrench The benefits of using such descriptor are first its ability to describe the variation of the angular momentum at the BCOM throughout the phases of the gait cycle, and its capacity to be computed in various locomotion conditions. In addition, this descriptor has shown promising results in previous studies for characterizing instability during gait. For example, Bailly et al. (Citation2018) observed that the distance increases as the walking terrain increases in difficulty. Abiad et al. (Citation2020) also studied the relative position of MMA and BCOM through the vector linking BCOM and its projection on the MMA. They showed that the norm and the anterior-posterior component of this vector can be used to highlight some instability features in the gait of people with amputation. The mean norm of distance and the anterior posterior component of distance calculated on amputees was higher than that calculated on healthy subjects.
Nevertheless, there remain several intriguing questions to be answered about the role of other components of the vector on the mediolateral and vertical directions in detecting instabilities. In this article, we compare the mediolateral and vertical vector components between transfemoral amputees and healthy subjects. The hypothesis is that the parameters associated with the relative position of MMA with respect to BCOM will be higher in amputees.
2. Methods
Under the approval of the ethics committee, the study was composed of five subjects with unilateral transfemoral amputation (44 ± 14 years, 73 ± 17 kg) and fourteen healthy subjects (25.6 ± 5.8 years, 73 ± 8 kg). Each participant was equipped with 47 retro-reflective skin markers tracked at 200 Hz using a Vicon system (Oxford Metrics, UK). Ground reaction forces (GRF) and moments were simultaneously measured at 2 kHz by force plates (AMTI, USA) and filtered with a 4th order Butterworth lowpass with a 15 Hz cut-off frequency. Each subject performed at least one trial at self-selected walking velocity.
To calculate the MMA, along which moment of the external contact forces is minimal, the GRF and moments were used. Three-dimensional BCOM was determined using anthropometric tables for healthy subjects and sound limbs of amputees (Dumas et al. Citation2007). The BCOM of the prosthetic limb is obtained by the method described in Abiad et al. (Citation2020). The components of the vector between BCOM and its projection on the MMA is computed according to the following equation:
(1)
(1)
where
refer to the mediolateral, anterior-posterior and vertical component of GRF, moment at COM and
respectively.
The mean and the range of variation of and
during one gait cycle were extracted.
3. Results and discussion
shows the mean and the range of variation of and
Both the means of
and
were greater for amputee subjects. Considering
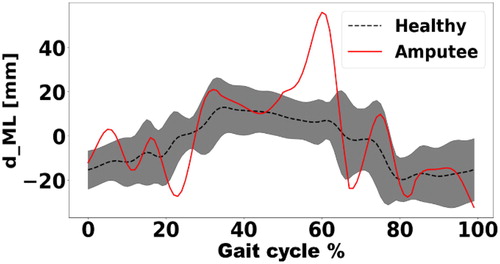
this result agrees with the result found in the previous study of (Sheehan et al. Citation2015) which states that individuals with lower limb amputation are mediolaterally more unstable during walking than able-bodied individuals. Moreover, individuals with unilateral transtibial amputation have a greater mean range of angular momentum in the frontal plane or anterior-posterior direction (Silverman and Neptune Citation2011). shows the shape of the mediolateral vector component for one amputee and on average for healthy subjects. For healthy subjects, this shape is similar to the variation of mediolateral angular momentum derivate (Herr and Popovic Citation2008). EquationEquation (2)
(2)
(2) is an approximation of mediolateral component in EquationEquation (1)
(1)
(1) . The product
is negligible with respect
It shows a relationship between the mediolateral component
and the anterior-posterior component of the angular momentum.
(2)
(2)
where
is the angular momentum derivate in the frontal plane.
Figure 1. Mean and
for amputees and healthy subjects (V:
ML:
).
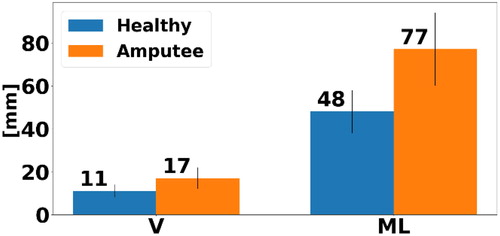
Figure 2. Normalized Average and corridor (+/–1 std) for healthy subjects in black dotted line (b) one typical amputee subject in red.
In Herr and Popovic (Citation2008), it was inferred that the anterior-posterior angular momentum was the second contributor in whole-body angular momentum. Similarly, the mediolateral vector component is the second contributor in the norm of the distance. Considering even though the vertical component value is lower than anterior posterior mediolateral distance, a difference of 6 mm between amputees and healthy subjects could be found.
Finally, the instability in amputees gait appeared through the higher distance along vertical and mediolateral direction.
Limitations of this study include the low number of amputees, heterogeneity of levels of amputation, of prosthetic types and walking speeds.
4. Conclusions
As a conclusion, the distance vector components computed in the two mentioned directions: mediolateral and vertical can differentiate between the amputee and healthy gait. They may detect instabilities that amputees have along the mediolateral and vertical directions. Ongoing works will involve experimental analysis of different instability conditions of gait using instrumented bi-band treadmill. Furthermore, this distance can be used to assess the ability of the prosthesis to provide a functional gait as compared to healthy subjects.
Acknowledgment
We would like to thank Dr Julia Facione, HIA Percy, for the collection of data of people with amputation.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Abiad NA, Pillet H, Watier B. 2020. A mechanical descriptor of instability in human locomotion: experimental findings in control subjects and people with transfemoral amputation. Appl Sci. 10(3):840.
- Bailly F, Carpentier J, Pinet B, Soueres P, Watier B. 2018. A mechanical descriptor of human locomotion and its application to multi-contact walking in humanoids. Proceedings of the 7th IEEE International Conference on Biomedical Robotics and Biomechatronics (Biorob). p. 350–356.
- Dumas R, Chèze L, Verriest J-P. 2007. Adjustments to McConville et al. and Young et al. body segment inertial parameters. J Biomech. 40(3):543–553.
- Herr H, Popovic M. 2008. Angular momentum in human walking. J Exp Biol. 211(Pt 4):467–481.
- Sheehan RC, Beltran EJ, Dingwell JB, Wilken JM. 2015. Mediolateral angular momentum changes in persons with amputation during perturbed walking. Gait Posture. 41(3):795–800.
- Silverman AK, Neptune RR. 2011. Differences in whole-body angular momentum between below-knee amputees and non-amputees across walking speeds. J Biomech. 44(3):379–385.