
1. Introduction
Middle ear surgery requires from the surgeon a high level of expertise because of the very small anatomical parts involved and the proximity of many at-risk structures. To perfectly manage the gesture, training is necessary. Thanks to the possibilities offered by 3D printing, multimaterial artificial bones can be used as educational tools. The 3D models must be close to the real geometry of the anatomic parts but also have to satisfyingly reproduce the surgical sensations during machining. In this article, a comparison of the forces measured during milling of a newly developed 3D model and human temporal bone samples is presented.
2. Methods
2.1. Presentation of the 3D model
Several types of artificial temporal bones are available for surgeons’ training but the level of satisfaction of surgeons is quite controversial and is evaluated most of the time through subjective qualitative procedures (Suzuki et al. Citation2018). In this work, a new 3D-printed model of the temporal bone made of two resins representing hard (bone) and soft (facial nerve, dura-mater, etc.) tissues, and whose morphological validation was conducted by Chauvelot et al. (Citation2020) is considered (see ).
Figure 1. (a) 3D model of temporal bone composed of soft (a [external auditory canal skin]) and hard (b [cortical bone]) resins; (b) cadaveric bone sample.
![Figure 1. (a) 3D model of temporal bone composed of soft (a [external auditory canal skin]) and hard (b [cortical bone]) resins; (b) cadaveric bone sample.](/cms/asset/d13bc4ab-f93e-4a8b-a294-9d6c62d895d4/gcmb_a_1811508_f0001_c.jpg)
2.2. Milling tests
Milling tests were conducted on the 3D model and on three cadaveric temporal bone (TB) samples provided by the Laboratory of Anatomy of the Faculty of Medicine of Nancy (in respect with charters of body donation to science). Pieces of cortical bone of 40 × 20 mm2 corresponding to the mastoidectomy zone were extracted at the fresh state (see ).
Two experimental campaigns were carried out. The first one consisted in manual milling tests performed by an expert surgeon in order to extract the following cutting information: axial and radial depths of cut and linear speed and to allow the surgeon to compare the force response of the 3D model with respect to bone samples. These experiments were driven in real clinical environment using a Zeiss operating microscope, a Medtronic – ‘Indigo High-Speed Otologic Drill’ motor with a straight handpiece, an ‘IPC console’ and an ‘IPC System Multi-function Footpedal’ pedal. Milling paths were linear along × direction (see ) to facilitate the extraction of cutting parameters and all tests were made at least 3 times on each sample.
Figure 2. Illustration of the milling tests carried out in clinical environment.
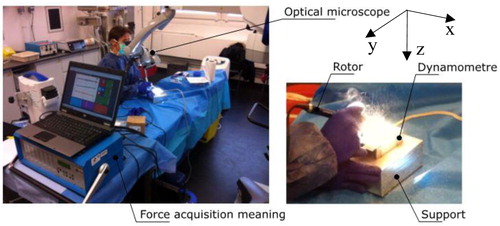
The second series of experiments was conducted on a machining center (CNC machine) using the operative conditions identified during the first campaign. The following surgical drill tools were used: a 4 mm diameter tungsten burring one for roughing operation and a 4 mm abrasive burr for finishing operation. The spindle rotational speed was 30,000 rev/min and a tool inclination angle of 45° was chosen (in agreement with clinical conditions). Cutting forces were measured during surgery using a Kistler Minidyn 9256 C dynamometer coupled to a Kistler 9017 amplifier.
3. Results and discussion
3.1. Results of manual campaign
The manual experimental campaign first aimed at evaluating the linear speed and the depths of cut that would be considered in the tests conducted with the CNC machine. The average values of linear speed varied between 316 and 331 mm/min for roughing and between 218 and 234 mm/min for finishing. The smallest values for each category were obtained for the 3D model but the differences with respect to the values provided with bone were less than 5%. This difference lies in the range of variation of the linear speed which was 242–375 for 3D models and 300–365 for bone samples in roughing, and 189–279 and 211–276, respectively, for finishing. Therefore, values of 200 and 300 mm were chosen in finishing and roughing for milling tests on the machining center.
The forces generated during machining exhibited three components. Their mean values and ranges of variation are reported in . The lower values of forces obtained for finishing were expected as a smaller quantity of material is removed during this operation. Even if discrepancies were observed between real and artificial bone, the 3D model and the bone samples followed the same trend: the highest values were observed in z direction and the smallest ones in y direction. However, it must be noted that the range of variation of all components was quite high, which can be easily understood by the fact that the surgeon permanently adapts his gesture to the local properties of the milled material mainly by varying the force applied on the tool. This high dispersion does not however contradict the conclusions prevently given. For axial and radial engagements, values of 2 and 1.5 mm were extracted and adopted for the second experimental campaign.
Table 1. Force components in roughing and finishing for manual and CNC machining operations.
3.2. Results of milling tests on machining center
The force values obtained using the machining center are also reported in . The comparison of the values with those obtained during the manual milling campaign shows a huge difference, even if the operating conditions are supposed to be close. One possible explanation of this discrepancy is the stiffness difference between the CNC machine and the surgeon’s arm. Indeed, during manual surgery, vibrations are observed on the force signals due to the high rotation frequency of the spindle and the fact that the surgeon has not the possibility to totally compensate these vibrations. An analysis of the topography of the milled surfaces shows that different cutting processes take place in both machining processes, which leads to different levels of force.
The comparison of the values obtained for 3D model and bone samples shows differences for all components of forces and all machining configurations. The forces generated by the milling of 3D models are always lower (except for Fz finishing) than for TB. However, the dispersion of the values obtained for bone specimens is important and the values obtained for 3D models are close to or in the range of variation of the forces obtained for bone.
4. Conclusions
Machining forces were measured during the milling of a new developed 3D model of temporal bone and real bone samples to evaluate the machinability of the 3D model. In the experimental campaign conducted on the CNC machine, the level of forces obtained for the 3D model was close to or in the range of variation of the forces measured during bone milling. However, these tests were not able to reproduce the real milling conditions observed during manual surgery because of the high stiffness of the CNC machine. This study requires further investigations.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Chauvelot J, Laurent C, Le Coz G, Jehl JP, Tran N, Szczetynska M, Moufki A, Bonnet AS, Parietti-Winkler C. 2020. Morphological validation of a novel bi-material 3D-printed model of temporal bone for middle ear surgery education. Ann Transl Med. 8(6):304.
- Suzuki R, Taniguchi N, Uchida F, Ishizawa A, Kanatsu Y, Zhou M, Funakoshi K, Akashi H, Abe H. 2018. Transparent model of temporal bone and vestibulocochlear organ made by 3D printing. Anat Sci Int. 93(1):154–159.