
ABSTRACT
The objective of this study was to measure how, why, and where the power adjustable seat height (PASH) system of Quantum’s iLevel® wheelchairs were used. We instrumented iLevel® power wheelchairs for 24 adults to measure wheelchair occupancy, seat height, in-seat activity level, and bouts of mobility. Participants elevated their wheelchair 3.9 (4.4) (mean (SD)) times per day, including 1.0 (1.6) times per day past 9”. Twenty-nine percent of elevation events were transient, lasting < 1 min, while 42% of elevate events lasted >5 minutes. Sixty-seven percent of participants transferred while elevated at least once, typically from heights <5” or >9”, and 14 people changed their seat height between the transfer to and from the wheelchair. Twenty-three of 24 participants wheeled while elevated. Finally, in-seat activity level was greater while elevated. For many participants, the PASH system provided a functional benefit on a daily basis. Individuals elevated 4 times per day for activities including transfers, reach, gaze, or mobility. However, 14 participants did not elevate on at least 1 day. Further study is needed to identify the characteristics of people who will benefit most from a PASH system as well as to document the value associated with PASH system use.
Introduction
People with mobility disabilities are commonly provided wheelchairs to replace ambulation as the most efficient means of mobility. However, these devices frequently become the base from which the individuals function and perform all of their daily tasks. These tasks typically include transfers to other surfaces, performance of activities of daily living (ADLs), school, work and volunteer duties, and engagement in other community-based activities. Typical ADLs require individuals to move within the wheelchair and from the wheelchair to other surfaces, to reach, manipulate objects and interact with other people and the environment. For those who require power wheelchairs, a power adjustable seat height (PASH) system is a power elevating seat added onto their power wheelchair base that can raise the seat from a standard seat height up 10–12” with a user-operated control. PASH systems are one option to adjust how individuals interact with their environment when performing ADLs by providing a means to level transfer heights, raise the surface from which to initiate standing and improve access to objects by minimizing overhead reach.
Wheelchair users have identified the ability to reach in their environment as one of the most important functional tasks they need to perform (Holliday, Mihailidis, Rolfson, & Fernie, Citation2005; Mills et al., Citation2002). The objects and spaces that wheelchair users access in a typical environment exist at varying heights. Some items in a home such as toilet seats, light switches, counters, and cabinets, are typically set at standard heights. Even items at a standard height, however, vary from toilets that are often shorter than the typical power wheelchair seat-to-floor heights of 16–19”, and cabinets, which are well above the height one can reach from a seated height in a typical power wheelchair. Therefore, wheelchair users have been found to perform overhead arm activities 5 times more often than ambulatory control subjects (Newsam et al., Citation2007). Chronic orthopedic impairments are associated with repetitive movements of the glenohumeral joints in a wide range of motion, especially above 60⁰ (Musculoskeletal disorders and workplace factors: A critical review of epidemiologic evidence for work-related musculoskeletal disorders of the neck, the upper-limb, and low back, Citation1997; Requejo et al., Citation2008). Difficulty in reaching tasks for children with severe cerebral palsy was found to increase as shoulder flexion increased (Furuya et al., Citation2015), suggesting overhead reach is more difficult and inefficient for this population of wheelchair users. Although reach is rated as extremely important to wheelchair users, repetitive overhead reach is unavoidable from those functioning from a seated position and can lead to injury and possibly decreased independence. Varying seat height during reaching tasks may reduce the difficulty of such tasks.
In addition to difficulty reaching objects in the environment, wheelchair users experience cervical hyperextension when interacting with people and objects in their environment. Kirby et. al reported that wheelchair users had to extend their cervical spines by 11° to look at the average seated male and 27° in order to make eye contact with the average height standing male (Kirby, Fahie, Smith, Chester, & Macleod, Citation2004). Direct eye contact with other individuals has been shown to have positive impacts on memory, cognition, and socialization (Conty, George, & Hietanen, Citation2016; Oda, Niwa, Honma, & Hiraishi, Citation2011; Schreiber & Hausenblas, Citation2016). Sabari et al. found that subjects seated in a power wheelchair at the minimum seat height used a greater arc of motion (≥60°) at the shoulder during a reaching task and a larger range of cervical extension (≥27°) during a functional reach and visual task, respectively, than they did at a maximum seat height via the use of a PASH system (Sabari, Shea, Chen, Laurenceau, & Leung, Citation2016).
Transfer surfaces also vary in height, and while some transfer surfaces may be level with the wheelchair, many, including the bed, toilet, living room seating, and vehicles, often require the wheelchair user to transfer to a non-level surface. Wang et. al measured ground reaction forces and shoulder and elbow muscle activity during lateral transfers at three different heights (Wang, Kim, Ford, & Ford, Citation1994). They concluded that transferring to a level seat height requires less upper extremity muscle effort than either higher or lower transfers. Given that the prevalence of shoulder pain in wheelchair users is estimated between 40% and 60% (Bossuyt et al., Citation2018; Finley & Rodgers, Citation2004; Kentar et al., Citation2018), that improved transfer technique has been shown to reduce pain and injury during transfers (Hogaboom, Worobey, & Boninger, Citation2016), and the above findings that level transfers are the least stressful on the shoulders, it stands to reason that a PASH system should provide an important benefit for users who perform lateral transfers to do so across level surfaces.
Sit-to-stand transfers are also impacted by seat height. The peak mechanical load and the peak hip and knee joint moments increase inversely to seat height within the range of high (23.6” or 60 cm) to normal (15.8” or 40 cm) seat height during sit to stand transfers (Yoshioka, Nagano, Hay, & Fukashiro, Citation2014). Numerous other studies have corroborated the decreased moments of the hip and knee rising from a higher seat height (Burdett, Habasevich, Pisciotta, & Simon, Citation1985; Munton, Ellis, & Wright, Citation1984; Rodosky, Andriacchi, & Andersson, Citation1989; Schenkman, Riley, & Pieper, Citation1996). Nakamura et. al found that the peak VO2 increased during sit-to-stand at decreased seat heights in healthy young women (Nakamura, Nagasawa, Sawaki, Yokokawa, & Ohira, Citation2016). In summary, raising the seat height for a sit-to-stand transfer has the potential of decreasing stress on the lower extremities, as well as on the cardiopulmonary system. Furthermore, fall risk is a concern during lateral and sit-to-stand transfers (Rapp, Becker, Cameron, Konig, & Buchele, Citation2012) that may be reduced by the ability to adjust seat height.
While anecdotal evidence suggests PASH systems are performing the functions described above amongst others, little is known about how often wheelchair users adjust the vertical height of their wheelchair seat, to what heights they adjust it, or for what purpose(s) the feature is actually used in everyday life. An early study reported six power wheelchair users accessed the seat elevation feature 4 ± 4 times a day for 22.5% of the day (Ding et al., Citation2008). The only other study to date to have measured seat elevation in power wheelchair users did so across 13 participants and did not clearly define what movement was required to count as elevating (Wu et al., Citation2017). They reported that participants elevated between 0.3 and 2.5 times per day. A more recent study measured changes in seat height in a manual wheelchair with “on the fly” adjustable seating functions and found that across eight participants, individuals changed their position approximately 8.7 times per day (Mattie, Borisoff, Miller, & Noureddin, Citation2017).
More information across a larger number of participants about how the PASH feature is used will allow for a better understanding of the potential benefits of PASH systems. Therefore, the objective of this study was to measure how, why, and where the seat elevating function of Quantum’s iLevel® wheelchairs were used.
Methods
Participants
Potential participants were recruited nationally using a combination of electronic and print advertisements as well as word of mouth. Adults who used a Quantum Rehab power wheelchair with an iLevel® system as their primary mobility device were eligible for participation. Potential participants who were unable to transfer or provide their own assistance for transfer, did not speak English, or did not use an Android or Apple smartphone were excluded from the study.
Protocol
This study received IRB approval at the Georgia Institute of Technology. Subjects provided informed consent in advance of participation. Once consented, participants were instructed to install the mEMA (ilumivu) app on their smartphone and complete a short survey asking about their demographics and wheelchair use. A Quantum representative then instrumented the participant’s wheelchair in his or her home with a series of sensors and a data logger to measure wheelchair use. These included:
Seat sensor
An array of six Force-Sensitive Resistors that was placed under the wheelchair cushion to measure wheelchair occupancy and center of pressure.
String potentiometer
The string from this variable resistor connected the wheelchair base to the seat and measured the height of the seat.
Data logger
A custom data logger fabricated by Quantum Rehab was connected to the wheelchair controller and attached to the back of the wheelchair. It recorded wheel speed data from the controller and seat height from the potentiometer at 1 Hz whenever the controller was powered on or the seat sensor identified the chair as occupied. Seat sensor data were recorded at 4 Hz during the same time periods.
Instrumentation was left on the wheelchair to collect data for 2–4 weeks (depending on subject and representative availability). During the instrumentation period, the subject did not have to interact with the data logging equipment at all. During this time, an ecological momentary assessment (mEMA) was conducted twice a day. This survey approach asked the user two questions about their PASH system use at randomized times between 12–2 PM and 6–8 PM local time. They were asked to select where they used their PASH in the past 6 h (Home, Work or School, Community, and/or No Use) and why they used their PASH in the past 6 h (Communication, Reach, Gaze, Transfers, Mobility, and/or No Use). At the end of the study duration, equipment was removed by the representative and returned to Georgia Tech for analysis.
Following the instrumentation period, a researcher called each participant to complete the Community Integration Questionnaire (CIQ). The CIQ is a measure of home integration, social integration (frequency of participation in activities outside the home) and productivity (involvement in employment, education and volunteer activities) that has been validated in populations with physical disabilities (Gontkovsky, Russum, & Stokic, Citation2009; Hirsh, Braden, Craggs, & Jensen, Citation2011; Willer, Ottenbacher, & Coad, Citation1994). The CIQ was used to describe our cohort and determine if level of community integration and participation was related to PASH feature use. A higher score indicates greater integration, participation, and productivity (Hirsh et al., Citation2011).
Data analysis
The following metrics were calculated to describe wheelchair use.
Time in Chair: Total number of hours the wheelchair was occupied per day.
# Transfers: Total number of times an individual transferred in or out of their wheelchair per day. The chair needed to be unoccupied for 2 min to be characterized as a transfer.
# Times Participant Elevated: Number of times that seat height was increased by at least 1” on a given day.
# Times Participant Elevated > 9”: Number of times that seat height was elevated above 9” on a given day.
Metrics of wheelchair mobility were also computed according to methods described previously (Sonenblum & Sprigle, Citation2017; Sonenblum, Sprigle, Harris, & Maurer, Citation2008; Sonenblum, Sprigle, & Lopez, Citation2012). These included the distance wheeled daily, number of bouts of mobility, and % mobile – the percent of time that the wheelchair was occupied that the participant was wheeling. Metrics describing bouts included the typical bout distance, duration, and velocity.
To determine if there was a relationship between feature use and community integration, the Pearson correlation coefficient was calculated between the number of times participants elevated daily and the Total CIQ score.
Our data did not document the intended purpose of every change in seat height, but some of the activities completed while elevated could be measured directly. In order to investigate what individuals did with their seat elevated, seat height was identified during transfers by measuring the average seat height in the 60 s before and after transfers (identified as the 60 s before and after an unoccupied segment). Seat height during a bout of mobility was measured as the average height during the bout.
Individual’s in-seat activity level was described using center of pressure movement. Center of pressure (CoP) movement was defined as the sum of the movement of the center of pressure on the seat mat over a 5-s window. Movements greater than 10 cm were considered active, and the frequency of active segments were reported (Sonenblum & Sprigle, Citation2017; Sonenblum, Sprigle, & Martin, Citation2016). Using this definition, activity was characterized by shifts in the center of pressure that results from leaning and reaching and other postural movements, the intent of which we could not assess. In-seat activity level while elevated was compared with center of pressure movement while the chair was below 1”.
Results
Study participants
Twenty-six participants were enrolled in the study, but only data from 24 are presented in this paper. Data logging equipment from one participant was lost in transit and an equipment problem led to no data being collected on the remaining participant. Of the 24, 22 completed the demographics questionnaire and are represented in . The population was evenly split between men and women, with an average age of 47 years old. On average, this cohort included predominantly experienced wheelchair users. All but one had been using a wheelchair for more than 2 years. However, only three of the participants had a PASH system included on their first wheelchair, 8 of 24 participants had used a PASH system for 6 months or less and 13 of 24 were still in their first year with a PASH system.
Table 1. Subject characteristics
Overview of wheelchair use and behavior
We recorded 453 days of data across the 24 participants. On 25% of these days (113 days), participants spent less than 4 h in their wheelchair. Ten different subjects had at least a single day with less than 4 h in the chair. On 268 days (59%) participants spent more than 8 h in the chair. The average day included a mean (SD) of 8.4 (4.9) hours in the wheelchair (), but most participants either spent more than eight or less than 6 h in the chair daily (). During an average day, participants transferred 8.5 (6.0) times in and out of their wheelchair ().
Table 2. Typical daily use of the wheelchair and PASH system across 453 days of data
Figure 1. Typical daily wheelchair use identified two groups in our population – those who used their chair fewer than 6 h per day, and those who used it more than 8 h per day
Elevating
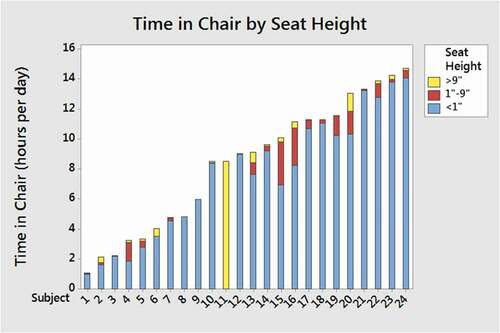
On average, participants elevated their wheelchair 3.9 (4.4) times per day, with an average of 1.0 (1.6) elevation per day extending past 9” (). Ten participants used their wheelchair in an elevated position every single day of the study, while the remaining 14 had at least one day in which they did not use the elevating feature. We documented 1943 events in which participants elevated their seat above 1”. Across these events, the most common elevated position was maximally elevated (>9”) (). Twenty-nine percent of elevation events lasted less than 1 min, meaning they were relatively transient events. Forty-two percent of elevate events lasted more than 5 min. The mean overall time spent elevated daily for each participant is shown in . Subject 11 is clearly an outlier, as she remained maximally elevated constantly and did not change position at all. However, because the goal of the paper included describing how the PASH feature was used, and this represented a unique example of use, this outlier was not excluded from analysis.
Figure 2. Distribution of seat height across all seat position changes of at least 1”. Note that this represents the distribution of instances of position changes, not time at each position
Figure 3. Daily time in chair for each subject colored according to seat height category shows some subjects spent a small total time at elevated positions while others spent a significant portion of their day elevated
On a typical day, study participants wheeled 55 bouts of mobility covering 1.2 km. This represented 11.4% of the time they were seated in their wheelchairs. Over 33,000 total bouts were recorded across all study participants. The median bout lasted 22 s and traveled 8.5 m at a speed of 0.39 m/s. ().
Table 3. Daily wheelchair mobility and typical bout characteristics in the iLevel wheelchair
CIQ score
Participants’ total CIQ score on average (mean (SD)) was 14.7 (2.9). Individual’s CIQ score was not correlated with the number of times they elevated daily, with a correlation of −0.287 (p = .195).
Activity while elevated
The purposes and conditions for changing seat height was investigated using both self-report and interpretation of the measurements. Both are presented below.
mEMA self-report iLevel use
The mEMA app proved difficult to use and only 15 participants responded to the survey alerts at least once. Of those, two only responded once and the other 13 responded repeatedly. Responses suggested that participants typically used their seat elevator in the home, with only four participants reporting use of PASH in the community more than half the time. demonstrates the frequency with which the participants reported each of the different purposes for use, with gaze and reach being reported most often and mobility and communication least often. Participants were more likely to always or never report using their PASH for transfers, while other purposes could be used intermittently.
Figure 4. Histograms describe the frequency with which each participant selected each purpose of PASH use in response to the mEMA survey
Objective measurements of iLevel use
Transfers
Ten out of the 15 (67%) mEMA responders self-reported using their PASH for transfers at least once during the study period, which was consistent with the 16 of 24 (67%) participants who transferred while elevated at least once while instrumented. In fact, the frequency with which mEMA responders self-reported using their PASH for transfers was correlated with the daily number of elevated transfers (Pearson correlation = 0.622, p = .013). Most transfers took place at heights less than 5” or greater than 9” (), and 14 people changed their seat height between the transfer out of the wheelchair and the return transfer at least one time.
Figure 5. Distribution of seat height during transfers shows that most transfers take place at seat heights less than 5” or greater than 9”. Six different subjects transferred from >9”
Mobility
While few participants reported using their iLevel® for the purpose of mobility, 23 of 24 (95.8%) participants wheeled while elevated during the study. In fact, nine participants wheeled more than 20% of their bouts elevated. Across all bouts recorded in the study, seat heights of less than 5” and greater than 9” were the most common for wheeling (). There were no differences in the typical bout distances or speeds when elevated compared with not elevated, but as restricted by the wheelchair hardware, the maximum speed while elevated was reduced from 6.0 mph to 3.2 mph. Furthermore, the percent of bouts wheeled faster than 1 m/s while elevated was 1.9% compared with 3.9% while not elevated.
Figure 6. Distribution of seat height across all elevated bouts of mobility during study period. Twenty-one participants wheeled bouts from >9”
In-seat activity level
Overall across all days and seat heights, participants had a frequency of active segments 17.7 (25) times per hour they were seated in their wheelchair (Median = 9.5 per hour). Comparing the in-seat activity level while elevated (57.7 (333.5)) to the level when the chair was below 1” (19.0 (29.5)), however, shows an increased in-seat activity level while elevated.
Case study
In order to highlight different types of PASH feature use, three example participants were selected who sat in their wheelchairs for at least 8 h per day but with different frequencies and durations of seat elevator use. The three example participants are all white men who lived with a spouse or other family and had been using a wheelchair for at least 5 years. None were employed at the time of the study, although Subject B reported that he was enrolled as a student (we believe it was in an online program).
Subject A: 35-year-old with a diagnosis of Spinal Muscular Atrophy Type II (with common symptom of hypotonia, muscle weakness of lower extremities greater than upper extremities, and postural deformities) and had been using a wheelchair for 30 years, including 5 years in a wheelchair with a PASH system.
Subject B: 21-year-old with a diagnosis of Spinal Muscular Atrophy Type II (with common symptom of hypotonia, muscle weakness of lower extremities greater than upper extremities, and postural deformities). He had been using a wheelchair for 16 years including 10 years with a PASH system.
Subject C: 75-year-old with a diagnosis of facioscapulohumeral muscular dystrophy with progressive weakness of the face, upper arms, and shoulders, as well as the legs. He had been using a wheelchair for 5 years and had only used a PASH system for 7 months.
Subject A represents someone who elevates for extended durations. On average, he spent more than 13 h per day in his wheelchair, although this was quite variable (ranging from 10.9 to 16.6 hours per day). He did not wheel many bouts of mobility during that time. On his average day, he elevated his seat only three times, but spent approximately 20% of his day in an elevated position (, ). He most commonly reported using his PASH system for gaze and communication, fairly stationary activities. This was consistent with the low frequency of CoP movements while elevated. He did not transfer frequently (most days only getting into and out of the chair 1–2 times), but he typically transferred out from a maximally elevated position by means of a dependent transfer. The higher seat to floor height of approximately 3 ft. with the chair maximally elevated, reduced the risk for injury to him and his caregiver (in this case, his father) while lifting him for transfers. From the CIQ, we learned that he did not perform any home integration skills such as meal preparation or housework and did not shop outside of the home but was active with leisure activities, visiting friends and volunteering. Overall his CIQ score was a 13, which is much lower than the mean of 17 reported for participants with muscular dystrophy in (Hirsh et al., Citation2011).
Table 4. Behavior on mean day for three example subjects (except elevated bouts and transfers, which are described across all bouts and transfers performed by those subject in the study, respectively)
Subject B had a very similar diagnosis and functional level to Subject A, but used his wheelchair very differently. He spent only 8.5 h per day in the wheelchair, wheeled fewer bouts than Subject A, and on many days did not use the elevate feature at all. Because he used it rarely and for very short durations, the CoP frequency during those very short durations was much higher (For example, if he elevated, it may have been exclusively for a transfer, which includes a lot of CoP movement). During his 8.5 h in the chair, he transferred in and out 6.8 times per day on average, and occasionally transferred from a maximally elevated (10”) position (7 times total) and transferred from 0” the remaining times (n = 124). Subject B did not complete the mEMA surveys, so he did not provide feedback about the purpose of PASH use. Like Subject A, he did not perform any home integration skills such as meal preparation or housework, but he did perform errands and was active with leisure activities and visiting friends outside the home. Overall his CIQ score was much higher at 18, which was consistent with the averages reported in (Hirsh et al., Citation2011).
Subject C was a much more dynamic user of his wheelchair, spending approximately 14 h per day in the chair, transferring 10.1 times per day, wheeling more than 100 bouts and elevating on average almost 7 times per day. Subject C only spent 7.9% of his time elevated despite elevating more frequently, meaning he elevated in a more transient fashion. He most commonly reported using his PASH system for mobility, reach and transfers. Consistent with this, he was more active while elevated, with a very high CoP frequency while elevated. He also wheeled 21% of his bouts while elevated and performed almost all of his transfers while elevated. This subject has the same reduced CIQ score (13) as Subject A, but achieved that score by assisting with grocery shopping, shopping, leisure activity and visiting with family and friends.
Discussion
Although there has been limited work done to study the use of PASH systems, the wheelchair use in this population of power wheelchair users can be compared to that of previously studied populations. Overall, the amount of time this cohort spent in their wheelchairs (mean = 8.5 h) was less than seen in many previous studies of persons using power wheelchairs (Ding, Cooper, Cooper, & Kelleher, Citation2007; Ding et al., Citation2008; Sonenblum & Sprigle, Citation2011; Sonenblum et al., Citation2008) and manual wheelchairs (Mattie et al., Citation2017; Sonenblum et al., Citation2016; Tolerico et al., Citation2007; Yang, Chang, Hsu, & Chang, Citation2009). However, there appeared to be two subgroups in this study, one who used their wheelchair for less than 6 h per day, which was unlike the populations previously studied, and those who used their wheelchair between 8 and 16 h per day, which was much more consistent with the previously published values between 10 and 12 h per day (Ding et al., Citation2007, Citation2008; Sonenblum & Sprigle, Citation2011; Sonenblum et al., Citation2008) in power wheelchairs and between 8 and 11 h per day (Mattie et al., Citation2017; Sonenblum et al., Citation2016; Tolerico et al., Citation2007; Yang et al., Citation2009) in manual wheelchairs. It is also important to note that the current population was significantly less integrated than the average population with physical disabilities studied using the CIQ (Hirsh et al., Citation2011).
The high variability measured in this study, both within and across subjects is consistent with all previous measurements of wheelchair use (e.g., Mattie et al., Citation2017; Sonenblum et al., Citation2016). In Sonenblum et. al, the authors identified different types of ways that people engaged with their tilt-in-space systems (Sonenblum & Sprigle, Citation2011). Mattie et. al used a similar approach in their study of changes in seat elevation (Mattie et al., Citation2017). In the present study, the majority of participants behaved liked the habitual group in the Sonenblum et. al study, in that they spent more than 80% of their time with the seat positioned at <1”. Only four participants spent their day at multiple positions with more than 20% of their time at positions other than <1”. This made it challenging to identify other types of users if they exist, although clearly, some users changed the seat height more frequently than others, and some used it in a more transient fashion than others. A larger population may be needed to identify other behavior types.
For many participants, the PASH system provided a functional benefit on a daily basis. Whether providing assistance with transfers, reach, gaze, or mobility, individuals engaged the feature 4 times per day. Participants who completed the mEMA were reasonably good at representing their purpose of feature use when used for transfers. For some participants, changing seat height for transfers might be routine, such as for Subject A transferring into bed on a daily basis, but for others, such as Subject B, the use during transfers was more intermittent. Excess fatigue, a change in caregiver, or a different environment can make a typically manageable transfer otherwise impossible without the ability to change seat height. Similarly, the fact that 14 participants changed seat height between transfers reinforced the need for flexibility in seat height during the day.
Wheeling while elevated was interesting, as few participants regularly identified mobility as the purpose for elevation, yet all but one participant wheeled while elevated. Those who never identified mobility as a purpose identified gaze, reach and communication most often as their purposes for elevating, and may have wheeled as part of those functions. For example, they might have needed to access multiple areas above shoulder level within a space, or improve their line of sight or be more visible for safety reasons while driving their wheelchair.
Despite the uses of the PASH system clearly demonstrated by some participants, 14 participants had at least 1 day with no use of the PASH system and a few participants did not spend time elevated on more than half of the days of the study (). These findings offer two opportunities. First is the opportunity to increase awareness to health-care professionals about types of use of PASH systems to improve training at delivery. Beyond making sure the user has access to the feature, training them in how they might use different heights to assist with lateral, sit-to-stand transfers and dependent transfers, reach, gaze, safety and visibility while wheeling, amongst others, might improve individual’s adoption and use of the feature. The second opportunity is to carefully consider who has the potential to benefit from the technology. The construct of matching person and technology (Scherer & Craddock, Citation2002) includes technology utilization in step two of the assessment process, recognizing the value of utilization in selecting technology. A potential new user, or someone who has had a PASH system and is considering another one on their next wheelchair, should be presented with the tradeoffs. If they are currently or are likely to be an infrequent user of the PASH system, they will need to weigh the value of that infrequent use in their life versus the increased cost, complexity, weight, and other potential tradeoffs to determine whether it is the appropriate technology. That is to say, for some users, infrequent use may provide such significant value when needed that it outweighs the increased costs. But for some users who are currently or likely to be infrequent users, the increased cost, complexity and weight of the feature may be too burdensome to be worthwhile. The population in the present study was too small to identify characteristics of individuals who were a better or worse match for the technology. In fact, the case series highlighted two users (Subjects A and B) who, on paper, were nearly identical, but had very different use of their PASH systems. A future study of a larger population might be a first step to help identify characteristics that would be useful in matching the technology with the user. Instrumentation of users’ wheelchairs may also be beneficial to see if, when and how an individual is using the feature, if there are changes in the use of the feature over time and whether transfer training and/or ADL training may be applicable. And of course, discussion with the user about how they use the feature is important. The data indicated that users are fairly reliable about feature use with respect to transfers, but less so with respect to how often they drive while elevated.
Study limitations
The small sample size makes it difficult to describe overall behavior types and characterize feature use according to populations, especially with such a diverse group in terms of function and diagnosis. While median values would not be influenced by Subject 11, mean values are inherently influenced by outliers. However, the impact would be counterintuitive, as the primary metrics of analysis, number of times participants elevated, would be slightly reduced by Subject 11, as she remained elevated constantly and did not change position. The impact was not significant, as the mean values were still greater than the median values. While this study was limited to PASH systems from a single manufacturer, the technology performs similar to technologies available from other manufacturers so we expect results to be comparable. There is always a sampling bias in that individuals who do not use their feature at all may be reluctant to agree to participate in a research study measuring feature use and very active users may be too busy to participate in research. Finally, many participants in the study were relatively new to using a PASH system, in that many were still in their first year with a PASH system. Many subjects may have been used to life in a power wheelchair at a single height as they only received a PASH system on a subsequent wheelchair, and had not integrated it into their daily routine. Whether feature use would be different after more time with the system, additional training, or for individuals who received a PASH system on their first wheelchair would be interesting to explore in a future study.
Conclusions
In conclusion, of the 24 participants monitored in this study, the majority used their PASH systems for functional activities throughout the day, albeit in varying frequencies and durations. Two-thirds of participants elevated for transfers, which included lateral transfers, sit-to-stand transfers, and dependent transfers, where benefits to safety and health have the potential to be significant. But at the same time, there were days observed in which the PASH system was not used by many participants.
Further research is needed to identify the characteristics of people who will benefit most from a PASH system as well as to document the value associated with PASH system use. Additionally, knowledge translation to clinicians and suppliers should support improved efforts to match the technology with the users, helping users weigh the value of their potential for elevating versus the increased cost, complexity, weight of the PASH system. Finally, results presented here should support improved training of those receiving the technology.
Acknowledgments
We would like to thank John Yaron for his efforts developing the data logger, Quantum employees and Georgia Tech students who assisted with the study logistics, especially Jim Apolinaro, Tony Parlopiano, and Natasha Halarnkar, and all the Quantum representatives who instrumented participants’ wheelchairs for the study.
Additional information
Funding
Related Research Data
References
- Bossuyt, F. M., Arnet, U., Brinkhof, M. W. G., Eriks-Hoogland, I., Lay, V., Muller, R., … Swi, S. C. I. S. G. (2018). Shoulder pain in the Swiss spinal cord injury community: Prevalence and associated factors. Disability and Rehabilitation, 40(7), 798–805. doi:https://doi.org/10.1080/09638288.2016.1276974
- Burdett, R. G., Habasevich, R., Pisciotta, J., & Simon, S. R. (1985). Biomechanical comparison of rising from two types of chairs. Physical Therapy, 65(8), 1177–1183. doi:https://doi.org/10.1093/ptj/65.8.1177
- Conty, L., George, N., & Hietanen, J. K. (2016). Watching eyes effects: When others meet the self. Consciousness and Cognition, 45, 184–197. doi:https://doi.org/10.1016/j.concog.2016.08.016
- Ding, D., Cooper, R. A., Cooper, R., & Kelleher, A. (2007). Monitoring seat feature usage among wheelchair users. Conference Proceedings of the IEEE Engineering in Medicine and Biology Society, 2007, 4364–4367. doi:https://doi.org/10.1109/IEMBS.2007.4353304
- Ding, D., Leister, E., Cooper, R. A., Cooper, R., Kelleher, A., Fitzgerald, S. G., & Boninger, M. (2008). Usage of tilt-in-space, recline, and elevation seating functions in natural environment of wheelchair users. Journal of Rehabilitation Research & Development, 45(7), 973–984. doi:https://doi.org/10.1682/JRRD.2007.11.0178
- Finley, M. A., & Rodgers, M. M. (2004). Prevalence and identification of shoulder pathology in athletic and nonathletic wheelchair users with shoulder pain: A pilot study. Journal of Rehabilitation Research and Development, 41(3B), 395–402.
- Furuya, M., Ohata, K., Izumi, K., Matsubayashi, J., Tominaga, W., & Mitani, A. (2015). Effect of the angle of shoulder flexion on the reach trajectory of children with spastic cerebral palsy. Research in Developmental Disabilities, 36C, 413–418. doi:https://doi.org/10.1016/j.ridd.2014.10.037
- Gontkovsky, S. T., Russum, P., & Stokic, D. S. (2009). Comparison of the CIQ and CHART short form in assessing community integration in individuals with chronic spinal cord injury: A pilot study. NeuroRehabilitation, 24(2), 185–192. doi:https://doi.org/10.3233/NRE-2009-0467
- Hirsh, A. T., Braden, A. L., Craggs, J. G., & Jensen, M. P. (2011). Psychometric properties of the community integration questionnaire in a heterogeneous sample of adults with physical disability. Archives of Physical Medicine and Rehabilitation, 92(10), 1602–1610. doi:https://doi.org/10.1016/j.apmr.2011.05.004
- Hogaboom, N. S., Worobey, L. A., & Boninger, M. L. (2016). Transfer technique is associated with shoulder pain and pathology in people with spinal cord injury: A cross-sectional investigation. Archives of Physical Medicine and Rehabilitation, 97(10), 1770–1776. doi:https://doi.org/10.1016/j.apmr.2016.03.026
- Holliday, P. J., Mihailidis, A., Rolfson, R., & Fernie, G. (2005). Understanding and measuring powered wheelchair mobility and manoeuvrability. Part I. Reach in confined spaces. Disability and Rehabilitation, 27(16), 939–949. doi:https://doi.org/10.1080/09638280500052799
- Kentar, Y., Zastrow, R., Bradley, H., Brunner, M., Pepke, W., Bruckner, T., … Akbar, M. (2018). Prevalence of upper extremity pain in a population of people with paraplegia. Spinal Cord, 56(7), 695–703. doi:https://doi.org/10.1038/s41393-018-0062-6
- Kirby, R. L., Fahie, C. L., Smith, C., Chester, E. L., & Macleod, D. A. (2004). Neck discomfort of wheelchair users: Effect of neck position. Disability and Rehabilitation, 26(1), 9–15. doi:https://doi.org/10.1080/09638280310001621451
- Mattie, J., Borisoff, J., Miller, W. C., & Noureddin, B. (2017). Characterizing the community use of an ultralight wheelchair with “on the fly” adjustable seating functions: A pilot study. PLoS One, 12(3), e0173662. doi:https://doi.org/10.1371/journal.pone.0173662
- Mills, T., Holm, M. B., Trefler, E., Schmeler, M., Fitzgerald, S., & Boninger, M. (2002). Development and consumer validation of the functional evaluation in a wheelchair (FEW) instrument. Disability and Rehabilitation, 24(1–3), 38–46.
- Munton, J. S., Ellis, M. I., & Wright, V. (1984). Use of electromyography to study leg muscle activity in patients with arthritis and in normal subjects during rising from a chair. Annals of the Rheumatic Diseases, 43(1), 63–65. doi:https://doi.org/10.1136/ard.43.1.63
- Musculoskeletal disorders and workplace factors: A critical review of epidemiologic evidence for work-related musculoskeletal disorders of the neck, the upper-limb, and low back (NIOSH Publication No. 97-141). (1997).
- Nakamura, K., Nagasawa, Y., Sawaki, S., Yokokawa, Y., & Ohira, M. (2016). Effect of different seat heights during an incremental sit-to-stand exercise test on peak oxygen uptake in young, healthy women. Journal of Sports Science & Medicine, 15(3), 410–416.
- Newsam, C., Requejo, P., Isaacs, J., Balikian, T., Hall, S., & Valenzuela, S. (2007). Comparison of overhead arm activity in wheelchair users and non-wheelchair-users during an 8-hour workday. Paper presented at the American Spinal Injury Association Meeting, Tampa, FL. doi:https://doi.org/10.1094/PDIS.91.4.0467B
- Oda, R., Niwa, Y., Honma, A., & Hiraishi, K. (2011). An eye-like painting enhances the expectation of a good reputation. Evolution and Human Behavior, 32(3), 166–171. doi:https://doi.org/10.1016/j.evolhumbehav.2010.11.002
- Rapp, K., Becker, C., Cameron, I. D., Konig, H. H., & Buchele, G. (2012). Epidemiology of falls in residential aged care: Analysis of more than 70,000 falls from residents of bavarian nursing homes. Journal of the American Medical Directors Association, 13(2), 187 e181–186. doi:https://doi.org/10.1016/j.jamda.2011.06.011
- Requejo, P., Mulroy, S., Haubert, L. L., Newsam, C., Gronley, J., & Perry, J. (2008). Evidence-based strategies to preserve shoulder function in manual wheelchair users with spinal cord injury. Topics in Spinal Cord Injury Rehabilitation, 13(4), 86–119. doi:https://doi.org/10.1310/sci1304-86
- Rodosky, M. W., Andriacchi, T. P., & Andersson, G. B. (1989). The influence of chair height on lower limb mechanics during rising. Journal of Orthopaedic Research, 7(2), 266–271. doi:https://doi.org/10.1002/jor.1100070215
- Sabari, J., Shea, M., Chen, L., Laurenceau, A., & Leung, E. (2016). Impact of wheelchair seat height on neck and shoulder range of motion during functional task performance. Assistive Technology, 28(3), 183–189. doi:https://doi.org/10.1080/10400435.2016.1140692
- Schenkman, M., Riley, P. O., & Pieper, C. (1996). Sit to stand from progressively lower seat heights – Alterations in angular velocity. Clinical Biomechanics, 11(3), 153–158.
- Scherer, M., & Craddock, G. (2002). Matching Person & Technology (MPT) assessment process. Technology and Disability, 14(3), 125–131.
- Schreiber, K., & Hausenblas, H. (2016). What eye contact can do to you: For better or worse, the gaze of others has a powerful effect on our behavior. Retrieved from https://www.psychologytoday.com/us/blog/the-truth-about-exercise-addiction/201609/what-eye-contact-can-do-you
- Sonenblum, S. E., & Sprigle, S. (2011). Distinct tilting behaviours with power tilt-in-space systems. Disability and Rehabilitation: Assistive Technology, 6(6), 526–535. doi:https://doi.org/10.3109/17483107.2011.580900
- Sonenblum, S. E., & Sprigle, S. (2017). Wheelchair use in ultra-lightweight wheelchair users. Disability and Rehabilitation: Assistive Technology, 12(4), 396–401. doi:https://doi.org/10.1080/17483107.2016.1178819
- Sonenblum, S. E., Sprigle, S., Harris, F. H., & Maurer, C. L. (2008). Characterization of power wheelchair use in the home and community. Archives of Physical Medicine and Rehabilitation, 89(3), 486–491. doi:https://doi.org/10.1016/j.apmr.2007.09.029
- Sonenblum, S. E., Sprigle, S., & Lopez, R. A. (2012). Manual wheelchair use: Bouts of mobility in everyday life. Rehabilitation Research and Practice, 2012, 753165. doi:https://doi.org/10.1155/2012/753165
- Sonenblum, S. E., Sprigle, S., & Martin, J. S. (2016). Everyday sitting behavior of full time wheelchair users. Journal of Rehabilitation Research and Development, 53(5), 585–598. doi:https://doi.org/10.1682/JRRD.2015.07.0130
- Tolerico, M. L., Ding, D., Cooper, R. A., Spaeth, D. M., Fitzgerald, S. G., Cooper, R., … Boninger, M. L. (2007). Assessing mobility characteristics and activity levels of manual wheelchair users. Journal of Rehabilitation Research and Development, 44(4), 561–572.
- Wang, Y. T., Kim, C. K., Ford, H. T., 3rd, & Ford, H. T., Jr. (1994). Reaction force and EMG analyses of wheelchair transfers. Perceptual and Motor Skills, 79(2), 763–766. doi:https://doi.org/10.2466/pms.1994.79.2.763
- Willer, B., Ottenbacher, K. J., & Coad, M. L. (1994). The community integration questionnaire. A comparative examination. American Journal of Physical Medicine & Rehabilitation, 73(2), 103–111.
- Wu, Y. K., Liu, H. Y., Kelleher, A., Pearlman, J., Ding, D., & Cooper, R. A. (2017). Power seat function usage and wheelchair discomfort for power wheelchair users. The Journal of Spinal Cord Medicine, 40(1), 62–69. doi:https://doi.org/10.1080/10790268.2016.1192360
- Yang, Y. S., Chang, G. L., Hsu, M. J., & Chang, J. J. (2009). Remote monitoring of sitting behaviors for community-dwelling manual wheelchair users with spinal cord injury. Spinal Cord, 47(1), 67–71. doi:https://doi.org/10.1038/sc.2008.72
- Yoshioka, S., Nagano, A., Hay, D. C., & Fukashiro, S. (2014). Peak hip and knee joint moments during a sit-to-stand movement are invariant to the change of seat height within the range of low to normal seat height. Biomedical Engineering Online, 13(1), 27. doi:https://doi.org/10.1186/1475-925X-13-27