
Abstract
Objective: While destabilization periods characterized by high variability and turbulence in a patient’s psychological state might seem obstructive for psychotherapy, a complex systems approach to psychopathology predicts that these periods are actually beneficial as they indicate possibilities for reorganization within the patient. The present study tested the hypothesis that destabilization is related to better treatment outcome.
Method: 328 patients who received psychotherapy for mood disorders completed daily self-ratings about their psychotherapeutic process. A continuous measure of destabilization was defined as the relative strength of the highest peak in dynamic complexity, a measure for variability and turbulence, in the self-ratings of individual patients.
Results: Destabilization was found to be related to better treatment outcome. When improvers and non-improvers were analyzed separately, destabilization was found to be related to better treatment outcome in improvers but not in non-improvers.
Conclusions: Destabilization in daily self-ratings of the psychotherapeutic process is associated with better treatment outcome. The identification of destabilization periods in process-monitoring data is clinically relevant. During destabilization, patients are believed to be increasingly sensitive to the effects of therapy. Clinicians could tailor their interventions to these sensitive periods.
Obiettivo: Mentre i periodi destabilizzanti caratterizzati da un'elevata turbolenza nello stato psicologico dei pazienti possono sembrare un ostacolo per la psicoterapia, un approccio sui sistemi complessi in psicopatologia predice che questi periodi sono realmente benefici nel momento in cui indicano la possibilita' per una riorganizzazione interna del paziente. Lo studio in questione ha testato le ipotesi che la destabilizzazione è relativa a un migliore outcome di trattamento.
Metodo: 328 pazienti che hanno ricevuto psicoterapia per disturbi dell'umore hanno completato misure giornaliere circa il loro andamento psicoterapeutico. Una misura continua di destabilizzazione è stata definita come la forza relativa al picco maggiore nella complessita' dinamica, una misura per la variabilita' e turbolenza, nell'autovalutazione dei pazienti.
Risultati: Si è riscontrato che la destabilizzazione era relativa a un migliore outcome del trattamento. Quando coloro che miglioravano e coloro che non miglioravano erano analizzati separatamente, la destabilizzazione era relativa a un migliore esito di trattamento in coloro che miglioravano ma non in coloro che non miglioravano.
Conclusioni: La destabilizzazione in questionari autovalutativi giornalieri del processo/ andamento psicoterapeutico è associata ad un migliore esito di trattamento. L'identificazione dei periodi di destabilizzazione nel processo di monitoraggio dei dati è clinicamente rilevante. Durante i momenti destabilizzanti, i pazienti hanno creduto di essere sempre piu' sensibili agli effetti della terapia. I clinici potrebbero personalizzare i loro interventi sulla base di questi periodi di alta sensibilita'.
Resumo
Objetivo: Enquanto os períodos de desestabilização sejam caracterizados por alta variabilidade e turbulência no estado psicológico do paciente pode parecer obstrutivo para a psicoterapia, um sistema de abordagem complexa para psicopatologia prevê que esses períodos sejam realmente benéficos, pois indica possibilidades de reorganização no paciente. O presente estudo testou a hipótese de que a desestabilização está relacionada a melhores resultados do tratamento. Método: 328 pacientes que receberam psicoterapia para transtornos do humor realizaram autoavaliações diárias sobre seu processo psicoterapêutico. Uma medida contínua de desestabilização foi definida como a força relativa do pico mais alto na complexidade dinâmica, uma medida de variabilidade e turbulência, nas autoavaliações de pacientes individuais. Resultados: Verificou-se que a desestabilização estava relacionada a um melhor resultado do tratamento. Quando os melhoradores e não-melhoradores foram analisados separadamente, verificou-se que a desestabilização estava relacionada ao melhor resultado do tratamento nos melhoradores, mas não nos não melhoradores. Conclusões: A desestabilização nas autoavaliações diárias do processo psicoterapêutico está associada a um melhor resultado do tratamento. A identificação de períodos de desestabilização nos dados de monitoramento de processos é clinicamente relevante. Durante a desestabilização, acredita-se que os pacientes sejam cada vez mais sensíveis aos efeitos da terapia. Os clínicos podem adaptar suas intervenções a esses períodos sensíveis.
Significância clínico-metodológica deste artigo: Embora os períodos de desestabilização, caracterizados por alta variabilidade e turbulência no estado psicológico do paciente, possam parecer obstrutivos para a terapia, a teoria de sistemas complexos sugere que esses períodos são realmente benéficos, pois oferecem oportunidades para explorar novos modos de funcionamento. O presente estudo constatou que a desestabilização está relacionada ao melhor resultado do tratamento em um grande grupo de pacientes que receberam psicoterapia para transtornos do humor. O conceito de desestabilização pode beneficiar a tomada de decisão terapêutica e a personalização do tratamento. Possíveis implicações clínicas, como ajustar os esforços de intervenção para períodos de desestabilização, são discutidas.
目的: 雖然病人心理狀態呈現高變異與動盪的不穩定時期,可能會對心理治療造成 阻礙,但採用一套心理病理學的複雜系統方法可以預測這個時期實際上是有幫助的, 因為它們展現病人進行內在重組的可能性。本研究驗證不穩定性與更好的治療結果是有相關的假設。方法: 328 位因情感性疾患接受心理治療的病人完成接受心理治療歷程的每日自我評估。所謂不穩定性的連續測量是指動態複雜度最高峰的相對強 度,即在個別病人的自我評估中測量其變異性和動盪性。結果: 發現不穩定性與更 好的治療效果有關。當針對有改善組與無改善組分別進行分析時,發現有改善組之不穩定性與較佳療效有關,而無改善組則發現無關。結論: 不穩定性與更好的治療 效果有關。若能在歷程檢視的資料中辨識出不穩定性的時期則對臨床實務至關重大。在不穩定性時期,病人反而對治療效果更加敏感。治療師可以針對這些敏感的時期介入其處遇。
Clinical or methodological significance of this article: While destabilization periods, characterized by high variability and turbulence in a patient’s psychological state, might seem obstructive for therapy, complex systems theory suggests that these periods are actually beneficial as they provide opportunities to explore new modes of functioning. The present study found destabilization to be related to better treatment outcome in a large group of patients who received psychotherapy for mood disorders. The concept of destabilization can benefit therapeutic decision making and personalization of treatment. Possible clinical implications, such as timing intervention efforts to periods of destabilization, are discussed.
Introduction
Psychotherapy, irrespective of therapeutic school, is an effective intervention for mood disorders such as depression (Robinson, Berman, & Neimeyer, Citation1990; Wampold & Imel, Citation2015). The effect sizes of psychotherapy, however, are small and have likely been overestimated in the past (Cuijpers, van Straten, Bohlmeijer, Hollon, & Andersson, Citation2010). This means that many patients do not benefit, even from the best available evidence-based treatments. In order to improve the effectiveness of psychotherapy, it is important to understand how psychotherapy works and empirically test possible mechanisms of change (Kazdin, Citation2007, Citation2009). In this study, we conceptualize psychopathology as an attractor state in a complex system of interacting cognitions, behaviors, emotions, and physiology. We propose destabilization of such an attractor state as a possible explanation for how clinical improvement in psychotherapy occurs and test the hypothesis that destabilization is positively related to better treatment outcome.
Kazdin (Citation2009) defines mechanism as follows: “the basis for the effect, i.e., the processes or events that are responsible for the change; the reason why change occurred or how change came about.” From the complex systems perspective that we endorse, the reason why change occurred and the reason how change came about are two very different kinds of processes. While there is much attention in psychotherapy literature for possible reasons why change occurs, e.g. the causal role of certain factors in treatment such as the therapeutic relationship (Norcross & Wampold, Citation2011), accounts of—and evidence for—how proposed causal factors lead to change are generally lacking. There are multiple reasons proposed for this. First, it might simply be that too little psychotherapy research addresses mechanisms of change (Kazdin, Citation2007). Many studies focus on treatment efficacy, i.e., if a certain treatment works, instead of how treatment works. These studies, often adopting randomized-controlled trial designs, are important for establishing treatment effects, but they do not provide evidence for possible mechanisms of change (Kazdin, Citation2007). Second, the results from studies that do address mechanisms of change are often limited by methodological shortcomings and lack plausibility in describing how a mechanism influences outcomes (Kazdin, Citation2007; Lorenzo-Luaces & DeRubeis, Citation2018; Stiles & Shapiro, Citation1994). For example, although there is strong evidence for a positive relation between therapeutic alliance and treatment outcome, a mechanistic account of this relation needs a plausible explanation of how exactly alliance leads to symptom reduction (Kazdin, Citation2005). Third, and perhaps most important, the study of how change in psychotherapy occurs is impeded by a lack of understanding of what psychopathology actually is (Bosman, Citation2017; Kendler, Zachar, & Craver, Citation2011). Without a clear conceptualization of what psychopathology is, the question of how psychotherapy leads to change is difficult to address.
The previously dominant idea that psychopathology is a latent factor that causes symptoms via biological mechanisms has become widely criticized because (1) until now, biological correlates of these latent factors have not been found (Kapur, Phillips, & Insel, Citation2012; van Os, Delespaul, Wigman, Myin-Germeys, & Wichers, Citation2013; cf. Wolfers et al., Citation2018) and (2) latent factors are not necessary to explain correlated symptoms when symptoms can have causal influences on one another (Borsboom & Cramer, Citation2013; Borsboom, Cramer, Schmittmann, Epskamp, & Waldorp, Citation2011). In addition, patients with the same diagnosis often have very different symptom profiles, which challenges the view of mental disorders as entity-like categories overall (Fried & Nesse, Citation2015). As an alternative for this “medical disease” or “latent factor” model, researchers have theorized that psychopathology should be seen as an attractor state in a complex system of interacting cognitions, emotions, behavior and physiology (Cramer et al., Citation2016; Hayes, Yasinski, Ben Barnes, & Bockting, Citation2015; Nelson, McGorry, Wichers, Wigman, & Hartmann, Citation2017; Schiepek, Citation2003). Such a complex systems approach to mental disorders provides a new perspective on possible mechanisms of change for psychotherapy (Hayes & Strauss, Citation1998).
Complex systems consist of components that interact over time in a nonlinear manner. As a function of environmental demands, system components coordinate their behavior in different ways, thereby generating patterns that are more or less adapted to their current environment (Haken, Citation1983, Citation1992; Schöner & Kelso, Citation1988). When a pattern is maintained by the system, the pattern can be called an attractor state, i.e., a state to which the system is attracted (Thelen & Smith, Citation2006). From this perspective, psychopathology, such as psychosis or depression, can be seen as an attractor state in the psychological system in which a patient is “stuck” (Cramer et al., Citation2016; Holtzheimer & Mayberg, Citation2011; Nelson et al., Citation2017). Clinical improvement is then defined as a so-called order transition, a system-wide reorganization, from a pathological state towards a more healthy and adaptive state (Gelo & Salvatore, Citation2016; Hayes, Laurenceau, Feldman, Strauss, & Cardaciotto, Citation2007; Schiepek, Heinzel, Karch, Plöderl, & Strunk, Citation2016). Thus, from this perspective, a mental disorder is actually not disorder, but another mode of order (i.e., stable state), that can be judged to be pathological by existing norms (Bosman, Citation2017).
For an order transition towards clinical improvement to take place, the attraction of the existing, pathological, state first needs to diminish. In other words, the existing pattern needs to “break loose” before the order transition towards a new pattern can take place (Van Orden, Kloos, & Wallot, Citation2011). This process is called destabilization and can be identified as a relatively short period of increased variability and turbulence in a system’s behavior over time (Thelen & Smith, Citation1994). Several researchers have hypothesized that destabilization of a patient’s psychological state can be an explanation for how change in psychotherapy occurs (Hayes & Strauss, Citation1998; Hayes et al., Citation2015; Mahoney, Citation1991; Schiepek, Tominschek, & Heinzel, Citation2014).
Before we review past studies on the relation between destabilization and treatment outcome, it is important to explain two nuances in the interpretation of destabilization in the context of psychotherapy. First, it must be noted that complex systems theories do not predict all clinical improvement to take place via order transitions. Improvement can also occur within the same attractor state, this type of change has been referred to as “parametric” or “first-order change,” and occurs gradually compared to the more abrupt change that occurs in an order transition (Gelo & Salvatore, Citation2016; Kelso, Citation1997; Thelen & Smith, Citation1994). Clinical improvement via an order transition towards a more healthy state, however, is likely to be larger and more enduring than parametric change, in which the attraction of the pathological state is still strongly present. Second, while destabilization of an existing (pathological) attractor state signals an increased likelihood for change, destabilization alone is not sufficient for change to occur (Gelo & Salvatore, Citation2016; Lichtwarck-Aschoff, Hasselman, Cox, Pepler, & Granic, Citation2012). The system can also return to the old attractor state after destabilization. Therefore, destabilization might be best understood as a window of opportunity; a period in which a patient can explore new configurations and possibly make the transition to a more healthy state of being (Hayes, Laurenceau, et al., Citation2007; Mahoney, Citation1991).
The relation between destabilization and treatment outcome has been examined in the past for different patient groups, using different research methods. These studies all employ continuous measures of destabilization that are used for between-subject comparisons, i.e., whether patients with higher destabilization have a better treatment outcome compared to patients with lower destabilization. In 1998, Hayes and Strauss linked destabilization in observational data of therapy sessions to clinical improvement in patients with mood disorders. Interestingly, high destabilization was also related to high emotional intensity within the same session, suggesting that destabilization is a period of emotional turmoil (cf. Mahoney, Citation1991; Strunk, Citation2004; Walter et al., Citation2010). Two more recent studies including patients with personality disorders receiving cognitive therapy (Hayes & Yasinski, Citation2015) and youth with aggression problems receiving a combination of child-focused cognitive behavioral therapy and parent management therapy (Lichtwarck-Aschoff et al., Citation2012), found again a relation between destabilization and better treatment outcome. In these studies, destabilization indices were calculated from coded observational data using a dispersion analysis and recurrence quantification analysis, respectively. Additionally, studies measuring destabilization from time series data of frequent (e.g., daily) self-ratings found destabilization to be related to better treatment outcome for patients with obsessive-compulsive disorder (Schiepek et al., Citation2014), mood disorders (van de Leemput et al., Citation2014), and mixed diagnoses (Haken & Schiepek, Citation2010, pp. 416–422). Last, synchronous destabilization in self-ratings of patients and therapists about their therapeutic interaction was found to be characteristic for successful therapies (Gumz, Bauer, & Brähler, Citation2012).
While evidence that destabilization is related to better treatment outcome is accumulating, it must be noted that many studies included small samples of patients. Especially in the domain of process-outcome relations in psychotherapy, replication in larger samples is necessary (Kazdin, Citation2007). The study by van de Leemput et al. (Citation2014) does include many patients but here destabilization indices were only measured during a baseline period before the start of treatment, leaving destabilization periods within the treatment process unconsidered. The present study, therefore, tested the relation between destabilization and treatment outcome in a large sample (N = 328) of patients with mood disorders receiving psychotherapy, thereby considering the entire treatment period. It was hypothesized that stronger destabilization would be related to better treatment outcome. In addition, it was hypothesized that this association would be stronger for improvers than for non-improvers. For improvers, we hypothesized that high destabilization indicates an order transition, a system-wide reorganization that is related to better treatment outcome compared to when improvement is parametric and such reorganization did not take place. For non-improvers, destabilization did not take place, or possible destabilization might not have resulted in an order transition towards clinical improvement, and the relation between destabilization and treatment outcome should be weaker or absent (for preregistration of hypothesis and analysis see: Olthof, Hasselman, & Lichtwarck-Aschoff, 2018) Footnote1 .
Methods
Participants
Data for the present study were collected as part of routine clinical practice at four clinics in Germany and Austria. The study sample consisted of 328 patients (181 females), aged between 18 and 69 years (M = 43.80, SD = 11.04), with a primary diagnosis for one of the following mood disorders: bipolar disorder (7.0%), major depressive disorder single episode (45.1%), major depressive disorder recurrent (47.3%) or persistent mood disorder (0.6%) as classified with the International Statistical Classification of Diseases and Related Health Problems, tenth edition (ICD-10; World Health Organization, Citation1992). During treatment, patients completed the Therapy Process Questionnaire (TPQ; Schiepek, Aichhorn, & Strunk, Citation2012) on a daily basis using the Synergetic Navigation System (SNS; Schiepek, Aichhorn, et al., Citation2016), an online monitoring system for clinical change processes. The resulting self-ratings were accessible for therapists and could be used for feedback. All patients received different integrative treatment programs that combined therapeutic elements from different theoretical approaches. The dataset described here was compiled from self-ratings of patients that completed the self-ratings on at least 80% of their treatment days. Patients gave informed consent to participate in process-monitoring with the SNS and for empirical use of their data. Ethical approval for the application of the SNS to patient monitoring and the usage of the retrieved data was given by the ethical committee of the Salzburg County Governance.
Materials
The TPQ is a questionnaire developed for daily self-ratings of patients receiving psychotherapy (Schiepek, Aichhorn, et al., Citation2016). We used data from 23 items of the TPQ which correspond to five factors: (1) Therapy Progress, (2) Problem Intensity, (3) Relationship Quality and Trust in Therapists, (4) Dysphoric Affect, and, (5) Relationships with Fellow Patients (Schiepek et al., Citation2012). The items of the Dysphoric Affect scale and one item of the Problem Intensity scale were answered on a visual analog scale, the other items on a 7-point Likert scale. An example item from the Problem Intensity scale (translated to English) is “Today my problems bothered me”, with the response scale ranging from 1 (not at all) to 7 (very much). An example item from the Dysphoric Affect scale (translated to English) is “Today, I felt sad”, with a visual analog response scale ranging from 0 (not at all) to 100 (very much). Examples from the other scales include: “Today I came closer to the solution for my problems” (Therapy Progress), “I perceive the work with my therapist(s) as helpful” (Relationship Quality and Trust in Therapists), and “I can trust the other patients” (Relationship with Fellow Patients), all answered on a 7-point Likert scale ranging from 1 (not at all) to 7 (very much). The Problem Intensity scale of the TPQ was used to establish a measure of treatment outcome, the items of the other scales of the TPQ were used to establish a measure of destabilization (see below).
Data-analysis
Time series characteristics
The daily self-ratings had a median length of 59 days (range = 30–318). The median amount of missing days was 1 (range = 0–13), corresponding to a percentage of 1.37% (range = 0–12.94%). Because missing values are not allowed in the computation of destabilization indicators, missing days where imputed with values estimated by an ARIMA state space representation with Kalman smoothing as available in the function na.kalman() of the R-package imputeTS (Moritz & Bartz-Beielstein, Citation2017; R Core Team, Citation2017).
Treatment outcome
To assess treatment outcome we computed a pre-treatment score by averaging the scores on the Problem Intensity scale of the TPQ of the first week of treatment for every patient. Post-treatment scores where determined by averaging the scores on the Problem Intensity scale for the last week of treatment. Using the averages of the first and last week, in contrast to using only the measures of the first and last day, ensures a more reliable measure of treatment outcome as scores on the Problem Intensity scale fluctuated considerably over the course of treatment and taking only the first and last day of treatment could lead to biased results (cf. Schiepek, Aichhorn, et al., Citation2016). Diagnose-specific outcome measures were sometimes used in the routine practice of the clinics involved in the present study, but the instruments differ per clinic and there are many missing values on these measures. The Problem Intensity scale was used since these scores were available for all patients in the sample. An advantage of this measure is that it assesses the experience of problems, instead of the presence of symptoms, which makes it a suitable outcome measure for the heterogeneous patient sample of this study.
Improver status
We computed an index of improver status, in order to investigate the relation between destabilization and treatment outcome for improvers and non-improvers separately. Improvers and non-improvers were classified using the reliable change index, in which the significance of the difference between the post-treatment score and pre-treatment score is determined while correcting for the reliability of the questionnaire scale (Jacobson & Truax, Citation1991). The pre- and post-treatment scores were based on the Problem Intensity scale of the TPQ as described in the paragraph above. Internal consistency was calculated using Cronbach’s alpha’s. The internal consistency was 0.90 for pre and 0.93 for post, which is in line with previous findings (Schiepek et al., Citation2012). The standard deviation of the pre-scores for Problem Intensity was 1.15. Following the formula from Jacobson and Truax (Citation1991), a decrease in Problem Intensity (which ranged from 0 to 6) of 1.01 or higher was defined as a reliable improvement. A decrease smaller than 1.01 was defined as non-improvement. The patient sample analyzed here was classified with 107 improvers and 221 non-improvers.
Destabilization
To derive a continuous measure of the degree of destabilization, we used the dynamic complexity algorithm, a measure of instability that is suitable for relatively short time series, such as daily self-ratings of the psychotherapeutic progress (Schiepek, Citation2003; Schiepek & Strunk, Citation2010). Dynamic complexity is a multiplication of a fluctuation measure F, which is sensitive to the fluctuation intensity of a time series and a distribution measure D, which is sensitive to the random scattering of values between the theoretical minimum and maximum of a measurement scale (for technical details and a validation study see: Schiepek & Strunk, Citation2010). Dynamic complexity was computed for every item of the TPQ (except for the items of the Problem Intensity scale, which were used as the outcome measure) and every patient, using a 7-day overlapping moving window. This resulted in time series of dynamic complexity values for each item, which were then summed together in order to create one dynamic complexity profile for every patient.
Large peaks in the dynamic complexity profile indicate possible destabilization phases in a patient’s change process. Therefore, a destabilization predictor was computed based on the peak strength in the dynamic complexity profile. This predictor, Peak Complexity, was defined as the relative strength of the highest peak in the dynamic complexity profile. By dividing the maximum dynamic complexity value with the mean dynamic complexity value for every patient separately, we derived a measure of Peak Complexity that is corrected for inter-individual differences in the mean level of dynamic complexity. The first and last week of treatment were not included in the calculation of Peak Complexity.
Statistical models
The relation between Peak Complexity and Problem Intensity was assessed with three linear mixed-effects models.Footnote 2 The first model included Problem Intensity as a continuous outcome variable and Time (pre/post) as a categorical predictor. The effect of Peak Complexity on treatment outcome was modeled by the interaction of Time*Peak Complexity. Patients in the sample had a wide range of total treatment durations. Therefore, a potential effect of Duration was modeled by the interaction Time*Duration. The main effects of Peak Complexity and Duration were also included, but note that these are not of primary interest, because without the interaction with Time, they predict the average of the Problem Intensity pre-score and post-score. The nesting of repeated measures within patient was modeled by the inclusion of a random intercept for patient ID. The nesting of patients within treatment centers was modeled by the inclusion of a random intercept for the treatment center. The second model was similar to the first model, but only included improvers. The third model was similar to the first and second model, but only included non-improvers. Analyses were performed with the function lmer() available in the R-package lme4 (Bates, Mächler, Bolker, & Walker, Citation2015; R Core Team, Citation2017). The distributions of Duration and Peak Complexity were both found to be positively skewed (see for a visualization of the loglinear fit on the untransformed Peak Complexity data) and were therefore log-transformed and mean-centered prior to the analyses.Footnote 3
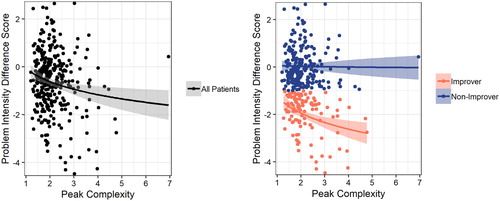
Figure 1. The relation between Peak Complexity and Problem Intensity reduction. Higher Peak Complexity is related to a greater reduction in Problem Intensity (left). When patients are divided in improvers and non-improvers, Peak Complexity is related to stronger Problem Intensity reduction in improvers but not in non-improvers (right).
Results
The results of the full model predicting Problem Intensity for all patients show that Peak Complexity was significantly related to treatment outcome (see ). The estimated average Problem Intensity pre-scores was 3.00 (intercept of the model). The average decrease in Problem Intensity over the course of therapy was 0.64 points (the effect of Time). For patients with a Peak Complexity that was one point higher than the average Peak Complexity, Problem Intensity decreased on average with an additional 0.95 points (β Time*Peak Complexity = −0.95, t (325) = −3.06, p = .001). Model-based Problem Intensity values for different quantiles of Peak Complexity are presented in . Duration was not related to decrease of Problem Intensity over time. The main effect of Duration shows that patients with longer therapy durations overall had higher scores on Problem Intensity (pre- and post-scores combined).
Figure 2. Model-based predictions of mean Problem Intensity scores in the first and last week of treatment, for three levels of Peak Complexity: Low (first quantile), Medium (second quantile) and High (third quantile).
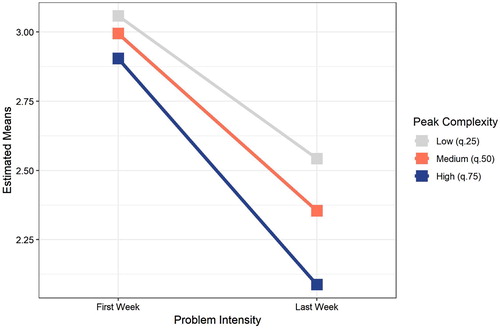
Table I. Results mixed-effects models predicting treatment outcome.
The results of the “improver model” showed that Peak Complexity was significantly related to treatment outcome in improvers. The estimated average Problem Intensity pre-score was 3.59. The average decrease in Problem Intensity over the course of therapy was 2.01 points for improvers (the effect of Time). For improvers with a Peak Complexity that was one point higher than the average Peak Complexity, Problem Intensity decreased on average with an additional 1.04 points (β Time*Peak Complexity = −1.04, t (104) = −3.30, p < .001). Again, there was a main effect of Duration showing that improvers with longer therapy durations overall had higher scores on Problem Intensity (pre- and post-scores combined).
The results of the non-improver model showed that Peak Complexity was not significantly related to treatment outcome in non-improvers. The estimated average Problem Intensity per-score was 2.72. The average decrease in Problem Intensity over the course of therapy was 0.03 for non-improvers (the effect of Time). The significant main effect of Peak Complexity shows that non-improvers with high Peak Complexity had on average lower Problem Intensity scores (modeled over both pre- and post-scores). Combined with the fact that the pre-score is relatively low for non-improvers, this effect suggests a possible floor effect in the relation between Peak Complexity and Problem Intensity, as non-improvers with high Peak Complexity have very low scores on Problem Intensity in general. Last, this model shows the same main effect for Duration as the other models.
Discussion
The present study tested the relation between destabilization and treatment outcome in patients with mood disorders. As hypothesized, we found that higher destabilization was related to better treatment outcome. This is in line with previous research findings (Hayes & Strauss, Citation1998; Hayes & Yasinski, Citation2015; Lichtwarck-Aschoff et al., Citation2012; Schiepek et al., Citation2014). The relation between destabilization and outcome was different for improvers and non-improvers, with destabilization being significantly related to treatment outcome in improvers, but not in non-improvers. This effect was previously found in a study described by Haken and Schiepek (Citation2010, pp. 416–422). The results of our study support the idea that destabilization can be a mechanism for how change occurs in psychotherapy. The destabilization of an existing pathological state opens up the possibility for a system-wide reorganization in the patient, which may result in an order transition towards a more healthy and adaptive state of functioning and thus significant reduction of symptom severity at post treatment.
The difference in the relation between destabilization and treatment outcome for improvers and non-improvers can be interpreted as follows. For improvers, higher destabilization signals the occurrence of an order transition, a system-wide reorganization that leads to a considerably large clinical improvement. Low destabilization in improvers, however, might indicate that these patients’ improvement occurred within the same attractor state (parametric or first-order change), resulting in improvement that is less strong (Hayes, Feldman, et al., Citation2007; Strunk & Schiepek, Citation2014; Thelen & Smith, Citation1994). In non-improvers, low destabilization likely indicates that the existing pathological state of these patients was resilient to the effects of psychotherapy and hence therapy was ineffective: change did not occur for these patients. The fourth combination, non-improvers that did show high destabilization might be especially interesting. Theory suggests that these patients have had a destabilization period in their therapeutic process in which there was a possibility for clinical improvement, but that this improvement did not take place. In other words, destabilization did not result in a transition towards a more healthy state. It is possible that these patients “fell back” to their old state or made a transition towards another pathological state, e.g., from a depressed to an anxious state (Gelo & Salvatore, Citation2016; Wichers, Schreuder, Goekoop, & Groen, Citation2019). This interpretation, however, should be read with caution, since the results of the models showed a possible floor effect in the relation between destabilization and treatment outcome in the non-improvers.
The main strength of this study is that we tested the relation between destabilization during psychotherapy and treatment outcome in a large sample of patients. By using daily self-reports, we could compute destabilization strength on an individual level based on the highest peak in dynamic complexity, accounting for inter-individual differences in average dynamic complexity. The results of the present study are therefore an important contribution to the growing body of multimethod support for the relation between destabilization and treatment outcome. This study also has several limitations. First, we cannot differentiate whether the relation between destabilization and treatment outcome is linear, i.e., more destabilization relates to a proportional better treatment outcome, or logistic, when destabilization is higher, there is an increased likelihood of better treatment outcome (via an order transition). In the first scenario, we would interpret our results as showing that more destabilization represents a stronger order transition with a more drastic system-wide reorganization, resulting in a proportional better treatment outcome. In the second scenario, we would interpret our results as showing that patients with higher destabilization are more likely to have experienced one or multiple order transitions, and that we, therefore, find a relation with treatment outcome. These explanations are complementary and both can be true. The relation between destabilization and transition is surely probabilistic, with destabilization signaling an increased likelihood for order transitions. At the same time, we expect stronger destabilization to indicate a larger reorganization process, possibly leading to more drastic clinical improvement. Future research could compare these two explanations using an intra-individual analysis of long time series data of patients that show multiple transitions. Second, in this study we related destabilization to treatment outcome, thereby focusing on the slowest measurable timescale of the psychotherapeutic process. In line with previous research, the relative strength of the highest destabilization peak was used as a between-subject indicator of destabilization strength (Schiepek et al., Citation2014). The results of the present study show that high destabilization at some point in therapy is related to better treatment outcome. A limitation of this approach is that we do not know when those destabilization peaks took place nor whether patients had multiple high peaks or only one (for a case study with multiple destabilization peaks see: Fartacek, Schiepek, Kunrath, Fartacek, & Plöderl, Citation2016). Additionally, we do not know how long possible destabilization periods lasted. From theory, we know that destabilization periods should be short relative to the timescale of the process (Haken, Citation2006; Thelen & Smith, Citation1994). In psychotherapy, this means at least that destabilization should only occur during a relatively short period in the therapy, and not during the whole therapy (Hayes et al., Citation2015; Schiepek, Eckert, Aas, Wallot, & Wallot, Citation2016).
Our findings have several clinical implications. First, our findings support the notion that therapists should see periods of instability in a patient's psychotherapeutic process generally as positive instead of obstructive (Hayes, Laurenceau, et al., Citation2007; Mahoney, Citation1991). While destabilization periods might be accompanied by emotional turmoil and a temporal worsening of symptom severity in patients, these periods signal opportunities for change and may, in the long run, be essential for sustainable clinical improvement (Hayes, Feldman, et al., Citation2007, Citation2015). It should be noted, however, that destabilization is indicative for change in general, which can also be undesirable, such as relapse into depression (Wichers & Groot, Citation2016) or suicide ideation (Fartacek et al., Citation2016). Still, in the context of psychotherapy, destabilization often indicates the destabilization of the pathological state for which the patient sought help, which is a desirable type of destabilization. For clinicians that work with patients that are at-risk for crises with negative outcomes, destabilization should be seen as an early-warning signal for possible future crises (Scheffer et al., Citation2009).
Second, the identification of destabilization periods may be used for dynamic personalization of intervention efforts. In another study, we related destabilization to transitions in daily measures of Problem Intensity (sudden gains and losses) on an intra-individual level and found that higher dynamic complexity predicted an increased risk for sudden gains and losses in the upcoming four days (Olthof et al., Citationin press). This finding shows that it is possible to identify destabilization in real-time before a transition has taken place, which opens up possibilities for personalization of treatment. During destabilization, relatively small influences can have disproportionally large effects (Haken, Citation2006). Therefore, destabilization is a promising target period in which patients are increasingly sensitive to the effects of psychological interventions (Granic, Citation2005). Destabilization indicators in frequent process-monitoring data can thus be used for therapeutic decision making and intervention efforts may be allocated to the destabilization periods in a patient’s change process. These intervention efforts can either be aimed at eliciting a transition, or preventing a transition. In the context of psychotherapy, intervention efforts should generally be aimed at supporting the exploration of new possible states of functioning, and, eventually, at supporting a possible transition (Hayes, Laurenceau, et al., Citation2007). For clinicians working with at-risk individuals, intervention during destabilization should generally be aimed at prevention of negative outcomes. The hypothesis of increased sensitivity during destabilization has been supported by studies in psychological domains such as motion science (Kelso, Schöner, Scholz, & Haken, Citation1987) and cognitive psychology (Stephen, Dixon, & Isenhower, Citation2009), but no studies exist that have investigated this effect in psychotherapy. Future research should test whether patients are indeed more sensitive to the effects of interventions during periods of destabilization.
Last, it is essential to realize in clinical settings that an order transition towards clinical improvement does not mark the end of treatment. After the transition towards a more healthy state, the new state should stabilize again in order to prevent relapse. Therapeutic guidance is also in this part of the change process essential. In this case, the existing (more healthy) attractor state should not be challenged, but supported, for example by supervised practice of new behaviors (Schiepek, Eckert, et al., Citation2016). Altogether, a successful therapy may thus be seen as a three-step sequence where (1) a stable pathological state is destabilized, leading to (2) a period of instability where an order transition towards improvement takes place, which is followed by (3) stabilization of a more healthy state, leading to enduring clinical improvement (cf. Hayes et al., Citation2015).
Overall, the present study provides support for the notion that destabilization periods and order transitions can explain how clinical change takes place in psychotherapy. However, the questions of why this change occurs remain unanswered. Here, we briefly elaborate on possible causal influences that might induce destabilization and transition in the context of psychotherapy. In the first place, destabilization and transition should be seen as phenomena that arise from the self-organizing processes of the elements within a given system (Haken, Citation1983). These self-organizational processes are driven by both internal fluctuations, that are always present as a consequence of the “loose coupling” between system elements, and external influences, such as those provided by therapy (Thelen & Smith, Citation2006). Changing internal and external influences can weaken the existing attractor and give rise to new attractors, thereby opening up possibilities for new self-organized states to emerge. For some order transitions in limb movement that have been studied extensively, causal influences that lead to destabilization and transition are known and can be modeled as so-called control parameters (e.g. see, Haken, Kelso, & Bunz, Citation1985; Kelso et al., Citation1987; Schmidt, Turvey, & Carello, Citation1990; Thelen & Ullrich, Citation1991). For example, Thelen and colleagues found that the transition towards stepping behavior in young infants can be explained with the ratio between the infant’s leg weight and leg strength as control parameter (Thelen & Smith, Citation1994, Citation2006; Thelen & Ullrich, Citation1991). Even more intuitive examples of control parameters can be found in “classical” phase transitions that are studied in physics. For example, heat is a control parameter for the phase transition that is observed when boiling water. At the critical point of 100 °C (with normal air pressure), water changes from a liquid state to a gaseous state.
For transitions in psychotherapy, however, the control parameters are more difficult to determine. There are likely to be many control parameters, with individual differences, that are also influenced by the patient’s existing state via feedback loops (Schiepek et al., Citation2017). Hypothesized psychological control parameters, such as motivation to change or external stressors, are impossible to isolate and be subjected to experimental control. While empirical research on control parameters is thus difficult, modeling studies may enhance our understanding of their role in psychotherapy and clinical change (e.g., Cramer et al., Citation2016; Schöller, Viol, Aichhorn, Hütt, & Schiepek, Citation2018).
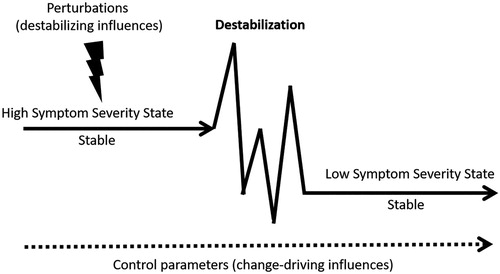
Besides via control parameters, that often change on a slow timescale, therapy can also influence patients’ change process via real-time treatment activities that “perturb” the existing state of the patient. Via these perturbations, treatment might contribute to the destabilization of the existing state. One treatment technique that is hypothesized to have destabilizing effects is exposure (Hayes, Feldman, et al., Citation2007). Exposure challenges and disturbs the existing state of a patient and might contribute to destabilization and reorganization within the patient system (Carey, Citation2011). Unlike control parameters, perturbations in the context of psychotherapy can be subjected to experimental control. Future studies should test the possible destabilizing influences of treatment techniques such as exposure. For example, researchers could study whether dynamic complexity in frequent self-ratings rises following exposure sessions. An overview of the hypothesized role of control parameters, perturbations, and destabilization in psychotherapy is given in (cf. Schiepek, Eckert, et al., Citation2016; Strunk & Schiepek, Citation2014; Tschacher & Haken, Citation2019).
Figure 3. Conceptual illustration of the role of control parameters, perturbations and destabilization in psychotherapy. An order transition from high symptom severity towards low symptom severity takes place via a period of destabilization. Therapeutic and other external influences act as perturbations or control parameters on the patient.
Conclusion
We found destabilization to be related to better treatment outcome for patients with mood disorders receiving psychotherapy. The results suggest that clinical improvement in successful therapy takes place via order transitions as found in complex systems. The stability of a patient’s psychological state, as measured with process-monitoring data, may be used to inform therapeutic decision making as patients may be increasingly sensitive to psychological intervention during destabilization periods.
Acknowledgments
We thank Prof. Dr. Wolfgang Aichhorn, Dr. Barbara Stöger-Schmidinger, Dr. Helmut Kronberger, Dr. Brigitte Krawanja, Dr. Brigitte Matschi, Dr. Fide Ingwersen, Elke Pauly, and Jens-Peter Rose for their contribution to the data collection.
Disclosure statement
Günter Schiepek is director of the Center for Complex Systems, publisher and developer of the SNS monitoring system that was used for data collection.
ORCID
Merlijn Olthof http://orcid.org/0000-0002-5975-6588
Fred Hasselman http://orcid.org/0000-0003-1384-8361
Guido Strunk http://orcid.org/0000-0002-0607-5105
Benjamin Aas http://orcid.org/0000-0001-5628-5912
Günter Schiepek http://orcid.org/0000-0003-3482-801X
Anna Lichtwarck-Aschoff http://orcid.org/0000-0002-4365-1538
Notes
1 Preregistration of this study is available at the Open Science Framework: DOI 10.17605/OSF.IO/XKU9C.
2 The open materials for this study including data preparation, analysis, figures, and comments are available at the Open Science Framework: DOI 10.17605/OSF.IO/3T94V. Note that the reported models are different from the preregistered model. Reasons for adjustment and results of the preregistered model are included in the open materials.
3 Analysis where Peak Complexity and Duration were not transformed yielded the similar results for all models (see open materials). Also, analysis without outliers in Peak Complexity (patients with Peak Complexity values that were more than three standard deviations larger than the average Peak Complexity) yielded similar results for all models (see open materials).
Related Research Data
References
- Bates, D. , Mächler, M. , Bolker, B. , & Walker, S. (2015). Fitting linear mixed-effects models using lme4. Journal of Statistical Software , 67 (1), 1–48.
- Borsboom, D. , & Cramer, A. O. J. (2013). Network analysis: An integrative approach to the Structure of psychopathology. Annual Review of Clinical Psychology , 9 (1), 91–121. doi: 10.1146/annurev-clinpsy-050212-185608
- Borsboom, D. , Cramer, A. O. J. , Schmittmann, V. D. , Epskamp, S. , & Waldorp, L. J. (2011). The small world of psychopathology. PLoS ONE , 6 (11), doi: 10.1371/journal.pone.0027407
- Bosman, A. M. T. (2017). Disorders are reduced normativity emerging from the relationship between organisms and their environment. In K. Hens , D. Cutas , & D. Horstkötter (Eds.), Parental responsibility in the context of neuroscience and genetics (pp. 35–54). Switzerland : Springer International Publishing.
- Carey, T. A. (2011). Exposure and reorganization: The what and how of effective psychotherapy. Clinical Psychology Review , 31 (2), 236–248. doi: 10.1016/j.cpr.2010.04.004
- Cramer, A. O. J. , van Borkulo, C. D. , Giltay, E. J. , van der Maas, H. L. J. , Kendler, K. S. , Scheffer, M. , & Borsboom, D. (2016). Major depression as a complex dynamic system. Plos One , 11 (12), e0167490.
- Cuijpers, P. , van Straten, A. , Bohlmeijer, E. , Hollon, S. D. , & Andersson, G. (2010). The effects of psychotherapy for adult depression are overestimated: A meta-analysis of study quality and effect size. Psychological Medicine , 40 (2), 211. doi: 10.1017/S0033291709006114
- Fartacek, C. , Schiepek, G. , Kunrath, S. , Fartacek, R. , & Plöderl, M. (2016). Real-time monitoring of non-linear suicidal dynamics: Methodology and a demonstrative case report. Frontiers in Psychology , 7 , 130. doi: 10.3389/fpsyg.2016.00130
- Fried, E. I. , & Nesse, R. M. (2015). Depression sum-scores don’t add up: Why analyzing specific depression symptoms is essential. BMC Medicine , 13 (1), doi: 10.1186/s12916-015-0325-4
- Gelo, O. C. G. , & Salvatore, S. (2016). A dynamic systems approach to psychotherapy: A meta-theoretical framework for explaining psychotherapy change processes. Journal of Counseling Psychology , 63 , 379–395. doi: 10.1037/cou0000150
- Granic, I. (2005). Timing is everything: Developmental psychopathology from a dynamic systems perspective. Developmental Review , 25 , 386–407. doi: 10.1016/j.dr.2005.10.005
- Gumz, A. , Bauer, K. , & Brähler, E. (2012). Corresponding instability of patient and therapist process ratings in psychodynamic psychotherapies. Psychotherapy Research , 22 , 26–39. doi: 10.1080/10503307.2011.622313
- Haken, H. (1983). Synergetics: An introduction. Non-equilibrium phase transition and self-self organisation in physics, chemistry and biology . Berlin : Springer Verlag.
- Haken, H. (1992). Synergetics in psychology. In W. Tschacher , G. Schiepek , & E. J. Brunner (Eds.), Self-organization and clinical psychology. Springer series in synergetics (pp. 32–54). Berlin : Springer.
- Haken, H. (2006). Synergetics of brain function. International Journal of Psychophysiology , 60 (2), 110–124. doi: 10.1016/j.ijpsycho.2005.12.006
- Haken, H. , Kelso, J. A. S. , & Bunz, H. (1985). A theoretical model of phase transitions in human hand movements. Biological Cybernetics , 51 , 347–356. doi: 10.1007/BF00336922
- Haken, H. , & Schiepek, G. (2010). Synergetik in der psychology [Synergetics in psychology] (2nd ed.). Göttingen : Hogrefe.
- Hayes, A. M. , Feldman, G. C. , Beevers, C. , Laurenceau, J. , Cardaciotto, L. , & Lewis-Smith, J. (2007). Discontinuities and cognitive changes in an exposure-based cognitive therapy for depression. Journal of Consulting and Clinical Psychology , 75 (3), 409–421. doi: 10.1037/0022-006X.75.3.409
- Hayes, A. M. , Laurenceau, J.-P. , Feldman, G. , Strauss, J. L. , & Cardaciotto, L. (2007). Change is not always linear: The study of nonlinear and discontinuous patterns of change in psychotherapy. Clinical Psychology Review , 27 , 715–723. doi: 10.1016/j.cpr.2007.01.008.Change
- Hayes, A. M. , & Strauss, J. L. (1998). Dynamic systems theory as a paradigm for the study of change in psychotherapy: An application to cognitive therapy for depression. Journal of Consulting and Clinical Psychology , 66 , 939–947. doi: 10.1037/0022-006X.66.6.939
- Hayes, A. M. , & Yasinski, C. (2015). Pattern destabilization and emotional processing in cognitive therapy for personality disorders. Frontiers in Psychology , 6 , 107.
- Hayes, A. M. , Yasinski, C. , Ben Barnes, J. , & Bockting, C. L. H. (2015). Network destabilization and transition in depression: New methods for studying the dynamics of therapeutic change. Clinical Psychology Review , 41 , 27–39. doi: 10.1016/j.cpr.2015.06.007
- Holtzheimer, P. E. , & Mayberg, H. S. (2011). Stuck in a rut: Rethinking depression and its treatment. Trends in Neurosciences , 34 (1), 1–9. doi: 10.1016/j.tins.2010.10.004
- Jacobson, N. S. , & Truax, P. (1991). Clinical significance: A statistical approach to defining meaningful change in psychotherapy research. Journal of Consulting and Clinical Psychologv , 59 (1), 12–19. doi: 10.1037/0022-006X.59.1.12
- Kapur, S. , Phillips, A. G. , & Insel, T. R. (2012). Why has it taken so long for biological psychiatry to develop clinical tests and what to do about it. Molecular Psychiatry , 17 (12), 1174–1179. doi: 10.1038/mp.2012.105
- Kazdin, A. E. (2005). Treatment outcomes, common factors, and continued neglect of mechanisms of change. Clinical Psychology: Science and Practice , 12 (2), 184–188. doi: 10.1093/clipsy/bpi023
- Kazdin, A. E. (2007). Mediators and mechanisms of change in psychotherapy research. Annual Review of Clinical Psychology , 3 , 1–27. doi: 10.1146/annurev.clinpsy.3.022806.091432
- Kazdin, A. E. (2009). Understanding how and why psychotherapy leads to change. Psychotherapy Research , 19 , 418–428. doi: 10.1080/10503300802448899
- Kelso, J. A. S. (1997). Dynamic patterns: The self-organization of brain and behavior . MIT press.
- Kelso, J. A. S. , Schöner, G. , Scholz, J. P. , & Haken, H. (1987). Phase-locked modes, phase transitions and component oscillators in biological motion. Physica Scripta , 35 (1), 79–87. doi: 10.1088/0031-8949/35/1/020
- Kendler, K. S. , Zachar, P. , & Craver, C. (2011). What kinds of things are psychiatric disorders? Psychological Medicine , 41 (6), 1143–1150. doi: 10.1017/S0033291710001844
- Lichtwarck-Aschoff, A. , Hasselman, F. , Cox, R. F. A. , Pepler, D. , & Granic, I. (2012). A characteristic destabilization profile in parent-child Interactions associated with treatment efficacy for aggressive children. Nonlinear Dynamics, Psychology, and Life Sciences , 16 , 353–379.
- Lorenzo-Luaces, L. , & DeRubeis, R. J. (2018). Miles to go before we sleep: Advancing the understanding of psychotherapy by modeling complex processes. Cognitive Therapy and Research , 42 (0), 212–217. doi: 10.1007/s10608-018-9893-x
- Mahoney, M. J. (1991). Human change processes: The scientific foundations of psychotherapy . New York : BasicBooks.
- Moritz, S. , & Bartz-Beielstein, T. (2017). imputeTS: Time series missing value imputation in R. The R Journal , 9 (1), 207–218.
- Nelson, B. , McGorry, P. D. , Wichers, M. , Wigman, J. T. W. , & Hartmann, J. A. (2017). Moving from static to dynamic models of the onset of mental disorder. JAMA Psychiatry , 74 , 528–534. doi: 10.1001/jamapsychiatry.2017.0001
- Norcross, J. C. , & Wampold, B. E. (2011). Evidence-based therapy relationships: Research conclusions and clinical practices. Psychotherapy , 48 , 98–102. doi: 10.1037/a0022161
- Olthof, M. , Hasselman, F. , Strunk, G. , van Rooij, M. , Aas, B. , Helmich, M. A. , … Lichtwarck-Aschoff, A. (in press). Critical fluctuations as an early-warning signal for sudden gains and losses in patients receiving psychotherapy for mood disorders. Clinical Psychological Science .
- R Core Team . (2017). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. Retrieved from https://www.r-project.org/
- Robinson, L. A. , Berman, J. S. , & Neimeyer, R. A. (1990). Psychotherapy for the treatment of depression: A comprehensive review of controlled outcome research. Psychological Bulletin , 108 , 30–49. doi: 10.1037/0033-2909.108.1.30
- Scheffer, M. , Bascompte, J. , Brock, W. A. , Brovkin, V. , Carpenter, S. R. , Dakos, V. , … Sugihara, G. (2009). Early-warning signals for critical transitions. Nature , 461 (7260), 53–59. doi: 10.1038/nature08227
- Schiepek, G. (2003). A dynamic systems approach to clinical case formulation. European Journal of Psychological Assessment , 19 , 175–184. doi: 10.1027//1015-5759.19.3.175
- Schiepek, G. , Aichhorn, W. , Gruber, M. , Strunk, G. , Bachler, E. , & Aas, B. (2016). Real-time monitoring of psychotherapeutic processes: Concept and compliance. Frontiers in Psychology , 7 , 604.
- Schiepek, G. , Aichhorn, W. , & Strunk, G. (2012). Der Therapie-Prozessbogen (TPB)—Faktorenstruktur und psychometrische daten. Zeitschrift für Psychosomatische Medizin und Psychotherapie , 58 , 257–266. doi: 10.13109/zptm.2012.58.3.257
- Schiepek, G. , Eckert, H. , Aas, B. , Wallot, S. , & Wallot, A. (2016). Integrative psychotherapy: A feedback-driven dynamic systems approach . Göttingen : Hogrefe.
- Schiepek, G. , Heinzel, S. , Karch, S. , Plöderl, M. , & Strunk, G. (2016). Synergetics in psychology: Patterns and pattern transitions in human change processes. In A. Pelster , & G. Wunner (Eds.), Selforganization in complex systems: The past, present, and future of synergetics. Understanding complex systems (pp. 181–208). Switzerland : Springer International.
- Schiepek, G. , & Strunk, G. (2010). The identification of critical fluctuations and phase transitions in short term and coarse-grained time series—a method for the real-time monitoring of human change processes. Biological Cybernetics , 102 , 197–207. doi: 10.1007/s00422-009-0362-1
- Schiepek, G. , Tominschek, I. , & Heinzel, S. (2014). Self-organization in psychotherapy: Testing the synergetic model of change processes. Frontiers in Psychology , 5 , 1089. doi: 10.3389/fpsyg.2014.01089
- Schiepek, G. , Viol, K. , Aichhorn, W. , Hütt, M. T. , Sungler, K. , Pincus, D. , & Schöller, H. J. (2017). Psychotherapy is chaotic– (not only) in a computational world. Frontiers in Psychology , 8 , 379. doi: 10.3389/fpsyg.2017.00379
- Schmidt, R. C. , Turvey, M. T. , & Carello, C. (1990). Phase transitions and critical fluctuations in the visual coordination of rhythmic movements between people. Journal of Experimental Psychology: Human Perception and Performance , 16 , 227–247.
- Schöller, H. , Viol, K. , Aichhorn, W. , Hütt, M. , & Schiepek, G. (2018). Personality development in psychotherapy : A synergetic model of state-trait dynamics. Cognitive Neurodynamics , 12 (5), 441–459.
- Schöner, G. , & Kelso, J. A. S. (1988). A dynamic pattern theory of behavioral change. Journal of Theoretical Biology , 135 , 501–524. doi: 10.1016/S0022-5193(88)80273-X
- Stephen, D. G. , Dixon, J. A. , & Isenhower, R. W. (2009). Dynamics of representational change: Entropy, action, and cognition. Journal of Experimental Psychology: Human Perception and Performance , 35 , 1811–1832. doi: 10.1037/a0014510
- Stiles, W. B. , & Shapiro, D. A. (1994). Disabuse of the drug metaphor: Psychotherapy process-outcome correlations. Journal of Consulting and Clinical Psychology , 62 , 942–948.
- Strunk, G. (2004). Organisierte Komplexität: Mikroprozess-Analysen der Interaktionsdynamik zweier Psychotherapien mit den Methoden der nichtlinearen Zeitreihenanalyse. Otto-Friedrich-Universität Bamberg. Online publiziert 2005. Retrieved from http://www.opus-bayern.de/uni-bamberg/volltexte/2005/64/pdf/Strunk_Dissertation.pdf
- Strunk, G. , & Schiepek, G. (2014). Therapeutisches Chaos: Eine Einführung in Die Welt der Chaostheorie und der Komplexitätswissenschaften (Vol. 2). Göttingen : Hogrefe Verlag.
- Thelen, E. , & Smith, L. B. (1994). A dynamic systems approach to the development of cognition and action . Cambridge : The MIT Press.
- Thelen, E. , & Smith, L. B. (2006). Dynamic system theories. In W. Damon & R. M. Lerner (Eds.), Handbook of child psychology. Volume one: Theoretical models of human development (6th ed, pp. 258–313). Hoboken, NJ : John Wiley & Sons.
- Thelen, E. , & Ullrich, B. D. (1991). Hidden skills: A dynamic systems analysis of treadmill stepping during the first year. Monographs of the Society for Research in Child Development , 56 (1), 1–103.
- Tschacher, W. , & Haken, H. (2019). The process of psychotherapy: Causation and chance . Cham : Springer Nature.
- van de Leemput, I. A. , Wichers, M. , Cramer, A. O. J. , Borsboom, D. , Tuerlinckx, F. , Kuppens, P. , … Scheffer, M. (2014). Critical slowing down as early warning for the onset and termination of depression. Proceedings of the National Academy of Sciences , 111 , 87–92. doi: 10.1073/pnas.1312114110
- Van Orden, G. C. , Kloos, H. , & Wallot, S. (2011). Living in the pink: Intentionality, wellbeing, and complexity. In C. Hooker (Ed.), Handbook of the philosophy of science (pp. 639–682). Amsterdam : Elesvier.
- van Os, J. , Delespaul, P. , Wigman, J. , Myin-Germeys, I. , & Wichers, M. (2013). Beyond DSM and ICD: Introducing “precision diagnosis” for psychiatry using momentary assessment technology. World Psychiatry , 12 , 113–117. doi: 10.1002/wps.20046
- Walter, S. , Schiepek, G. , Schneider, S. , Strunk, G. , Kaimer, P. , & Mergenthaler, E. (2010). The synchronization of plan activations and emotion-abstraction patterns in the psychotherapeutic process: A single-case study. Psychotherapy Research , 20 (2), 214–223. doi: 10.1080/10503300903277437
- Wampold, B. E. , & Imel, Z. E. (2015). The great psychotherapy debate: The evidence for what makes psychotherapy work . New York : Routledge.
- Wichers, M. , & Groot, P. C. , Psychosystems, ESM Group , & EWS Group (2016). Critical slowing down as a personalized early warning signal for depression. Psychotherapy and Psychosomatics , 85 (2), 114–116. doi: 10.1159/000441458
- Wichers, M. , Schreuder, M. J. , Goekoop, R. , & Groen, R. N. (2019). Can we predict the direction of sudden shifts in symptoms? Transdiagnostic implications from a complex systems perspective on psychopathology. Psychological Medicine , 49 , 380–387.
- Wolfers, T. , Doan, N. T. , Kaufmann, T. , Alnæs, D. , Moberget, T. , Agartz, I. , … Marquand, A. F. (2018). Mapping the heterogeneous phenotype of schizophrenia and bipolar disorder using normative models. JAMA Psychiatry , 75 , 1146–1110.
- World Health Organization . (1992). International statistical classification of diseases and related health problems, 10th revisions (ICD-10) . Geneva : WHO.