
Introduction
The purpose of this editorial is to present a patient evaluated and treated by physical therapists with co-existing neurogenic and vascular claudication. The differential diagnosis process is presented for this patient with a 1-year history of severe low back and lower extremity pain and disability from common iliac artery occlusion and lumbar stenosis.
Initial presentation and history
A 65-year-old Hispanic male was referred to an outpatient physical therapy clinic with the diagnosis of lumbar foraminal stenosis and a request to ‘evaluate and treat.’ On clinical examination in January 2018, the patient reported insidious onset of severe back, right hip, and leg pain of more than 1-year duration. Patient had been admitted to the hospital in August 2017 following a fall. Imaging confirmed spinal and foraminal lumbar stenosis. The patient’s main complaint was right posterior lateral hip pain, described as stabbing with pressure. The most pain referred distally from the posterior right hip to the knee and occasional pain to his foot (). Pain worsened with standing and walking, bending forward and increased to 10/10 when walking. Walking tolerance was 50 ft with a cane and standing tolerance about 5 min. Pain improved with sitting and resting. There was no sensory deficit in the lower extremity, some mild weakness throughout the right lower extremity. Straight leg raise (SLR) and slump tests were negative. Reflexes were 2 + bilaterally for the lower extremities. Pedal pulses were diminished. No changes in color or temperature of the lower extremities were observed. A treadmill test [Citation1,Citation2] was not performed due to the patient’s limited walking tolerance, and the bicycle test for intermittent claudication [Citation2–Citation4] was not performed as the patient refused to participate bicycling exercise testing due to his high pain level. Oswestry disability index (ODI) was 68, Numerical Pain Rating Scale (NPRS) was 7/10, and sleep was disturbed. Past medical history included Type II diabetes mellitus, hypertension, hypercholesterolemia, and back problems. Family medical history included hypertension, diabetes, heart disease, stroke/transient ischemic attack, heart attack, and paternal history of bilateral lower extremity amputations. The physical therapy diagnosis of spinal stenosis was used to create a conservative management program.
Figure 1. (a) Pain diagram at time of initial evaluation displaying severe back and leg pain pre-stent; (b) post-stent pain diagram with symptoms alleviation.
Diagnosis of right common iliac artery occlusion and management
The patient was treated with a course of aquatic therapy for 1-month with no clinically meaningful improvements to NPRS and ODI. The patient followed up with a neurosurgeon who noticed diminished pedal pulses on the right side and ordered Doppler imaging, which revealed 75% right common iliac artery occlusion, right ankle-brachial index (ABI) of 0.37 and left ABI of 0.88. Normal values for ABI are between 0.9 and 1.4, where values below 0.9 are associated with peripheral arterial disease (PAD) [Citation5,Citation6].
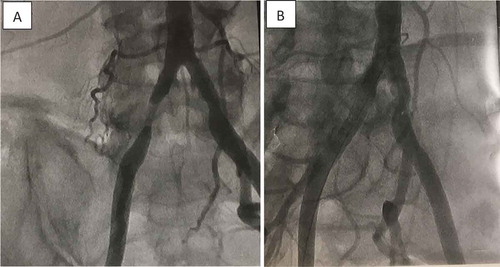
In March 2018, the patient sustained right common iliac artery stenting (), a 30-min outpatient procedure, with immediate and sustained relief of the right leg symptoms. He was re-assessed by the physical therapist mid-April 2018 and reported no right leg pain, the ability to walk without an assistive device for one mile and ODI improved to 32. The patient continued physical therapy for lumbar stenosis to resolve lingering symptoms. Patient improvements were maintained at 6-month follow-up.
Figure 2. (a) Pre-stent angiogram showing 75% right common iliac artery occlusion; (b) post-stent angiogram associated with immediate relieve of back and leg pain.
Discussion
Intermittent claudication is defined as pain in the legs associated with walking [Citation3,Citation7]. Intermittent claudication can have neurogenic or vascular origins, or both. While the prevalence of neurogenic and vascular claudication is well established in the literature, few studies discuss overlapping claudication with both neurogenic and vascular sources [Citation5,Citation8–Citation10]. This case report highlights the need for clinicians to be well versed in the differential diagnosis process to distinguish vascular from neurogenic claudication. A thorough history, examination of risk factors, and evaluation process allowed the physical therapist to identify underlying vascular claudication despite a physician diagnosis of lumbar foraminal stenosis with confirmed imaging studies.
Neurogenic claudication is a common symptom associated with lumbar stenosis and occurs when the nerve roots are directly or indirectly compressed in the spinal canal or foramina due to variations in spinal developmental and by articular degenerative changes, classified as either congenital or acquired [Citation11]. Magnetic resonance imaging (MRI) or computed tomography (CT) can be used to support neurogenic claudication diagnosis, but these imaging studies rarely correlate with lower extremity symptoms [Citation12]. Additionally, practitioners should limit their use due to their cost, and refer to the patient history and physical examination to formulate the diagnosis. Nadeau, et al. [Citation12] determined a constellation of symptoms, including triggering of symptoms with standing, relief with sitting, symptoms located above the knees, and a positive shopping cart sign yielding a positive likelihood ratio of 13 for neurogenic claudication. Symptoms’ alleviation with standing alone and symptoms located below the knees yielded a positive likelihood ratio of 20 for vascular claudication [Citation12]. Recently, clinical classification criteria were developed for neurogenic claudication due to lumbar spinal stenosis where patients are scored on subjective and objective factors [Citation13]. These factors include age >60, pain in both legs, leg pain relieved by sitting, leg pain decreased by spinal flexion, positive 30-s extension test, and negative SLR. Specific scoring instructions can be found in Genevay, et al. [Citation13]. According to the recommended cutoff score, the patient in this case did not meet the criteria for neurogenic claudication due to lumbar stenosis, yet he met some criteria and imaging had already confirmed stenosis was present. The fact that the patient had an increase in symptoms with forward flexion did not fit this picture. This could indicate some of the other examination findings were due to a different source.
Vascular claudication results from insufficient blood flow to match the metabolic demands of the lower extremity musculature [Citation5,Citation12]. Certain risk factors such as age, gender, heredity, smoking, hypertension, diabetes, and dyslipidemia place a patient at higher risk for developing vascular occlusions [Citation6,Citation14]. The patient in this case did have a family history and many of these risk factors himself. The location of the pain can provide insight as to where a possible occlusion may exist. Patients with occlusions to the distal common iliac, external iliac, and/or femoropopliteal arteries can present with calf pain. Patients with occlusions to the proximal common iliac and/or internal iliac arteries can present with low back, hip, buttock, or thigh pain and are more likely to mimic neurogenic claudication, hip osteoarthritis, venous congestion, or bone metastasis, among others, making diagnosis more challenging [Citation14]. Imaging confirmed that this patient’s occlusion was in the common iliac artery. His symptoms were both in his back and in the hip, buttock, thigh, lower leg, and occasionally to the foot. His symptoms, however, worsened with standing. Based on symptoms location and response to standing, the patient’s presentation did not clearly fit vascular claudication, yet his distal pulses were impaired, and imaging confirmed this finding. This was another indicator that the patient had more than one source of his symptoms.
Vascular and neurogenic claudication share similar characteristics, which makes differentiating the two conditions a challenging process (). provides a flowchart for clinicians to follow during the evaluation process to screen for underlying vascular conditions. In addition to symptomology, practitioners should proceed with a general inspection and systemic examination. Limb changes may be evident, including trophic skin lesions, hair loss, temperature changes, muscle atrophy, and diminished or absent pulses. If the patient presents with signs and symptoms of PAD, ABI testing can be used to confirm the diagnosis in an outpatient setting and assist in differentiating between PAD and lumbar spinal stenosis [Citation5,Citation6]. The ABI is measured by dividing the systolic pressure at the ankle by the systolic pressure at the arm. The American Heart Association found 5.5% of Americans are estimated to display ABI < 0.9 indicating PAD [Citation15]. Of these individuals, only 10% presented with intermittent claudication, 40% had no leg pain, and 50% had leg pain that neither involved the calves nor relieve after 10 min of rest [Citation5,Citation12,Citation15–Citation17]. Therefore, intermittent claudication cannot reliably be used to diagnose PAD and other factors need to be considered in the evaluation process. While vascular claudication has low prevalence, proper screening is vital to prevent complications from untreated vascular disease, such as high morbidity, amputation, and even death [Citation18] or the performance of inadequate spinal surgeries [Citation19].
Table 1. Examination findings associated with neurogenic and vascular claudication.
Figure 3. Clinical decision-making for differential diagnosis of neurogenic versus vascular claudication for patients with complaints of lower extremity pain and risk factors for peripheral vascular disease (ABI = Ankle-Brachial Index).
A distracting variable in this case report was the physician diagnosis of lumbar stenosis as well as an MRI confirming the diagnosis. While the patient continued to display symptoms of neurogenic claudication after stenting, the majority of the patient’s symptoms from vascular claudication resolved. Despite a physician’s diagnosis with imaging confirmation, the physical therapist is encouraged to complete a thorough evaluation to screen for underlying disease processes and proceed with appropriate treatment or referral.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Notes on contributors
Erin L. Huml
Erin L. Huml, PT, DPT, graduated from Bellarmine University with a doctor of physical therapy degree. She is a licensed physical therapist practicing in outpatient Physical Medicine and Rehabilitation at University Medical Center in Lubbock, Texas.
Robert A. Davies
Robert A. Davies, PT, DPT, graduated from Texas Tech University Health Sciences Center (TTUHSC) with a doctor of physical therapy degree. He is a licensed physical therapist, outpatient supervisor in Physical Medicine and Rehabilitation at University Medical Center and adjunct faculty to the DPT program at TTUHSC in Lubbock, Texas.
Gary A. Kearns
Gary A. Kearns, PT, ScD is assistant Professor in the doctor of physical therapy program at Texas Tech University Health Sciences Center in Lubbock, Texas. He graduated from the North American Institute for Orthopaedic Manual Therapy Fellowship program and teaches dry needling courses nationally.
Shannon M. Petersen
Shannon M. Petersen, PT, DScPT, is Professor of Physical Therapy at Des Moines University, Des Moines, Iowa. She completed her post-professional doctorate at Andrews University and post-doctoral fellowship in orthopaedic manual physical therapy at Regis University. Dr. Petersen is a Fellow in the American Academy of Orthopaedic Manual Physical Therapists.
Jean-Michel Brismée
Jean-Michel Brismée, PT, ScD, is professor in the post professional doctorate programs (ScD and PhD) at Texas Tech University Health Sciences Center in Lubbock, Texas.
References
- Fritz JM, Erhard RE, Delitto A, et al. Preliminary results of the use of a two-stage treadmill test as a clinical diagnostic tool in the differential diagnosis of lumbar spinal stenosis. J Spinal Disord. 1997;10(5):410–416.
- Goodman CC, Heick J, Lazaro RT. Differential diagnosis for physical therapists: screening for referral. 6th ed. St. Louis (MO): Elsevier; 2018.
- Fokkenrood H, Houterman S, Schep G, et al. Bicycle testing as an alternative diagnostic tool in patients suspected of intermittent claudication. Ann Vasc Surg. 2014;28(3):614–619.
- Dyck P, Doyle JB. “Bicycle Test” of van Gelderen in diagnosis of intermittent cauda equina compression syndrome. J Neurosurg. 1977;46:667–670.
- Jeon C-H, Han S-H, Chung N-S, et al. The validity of ankle-brachial index for the differential diagnosis of peripheral arterial disease and lumbar spinal stenosis in patients with atypical claudication. Eur Spine J. 2012;21(6):1165–1170.
- Bailey MA, Griffin KJ, Scott DJA. Clinical assessment of patients with peripheral arterial disease. Semin Intervent Radiol. 2014;31(4):292–299.
- Cassar K. Peripheral arterial disease. BMJ Clin Evid. 2011;01:211.
- Heidrich H, Hermann H. Concomitant neurological and orthopaedic diseases in the presence of peripheral arterial disease: a prospective study. Vasa. 2006;35:101–105.
- Johansson JE, Barrington TW, Ameli M. Combined vascular and neurogenic claudication. Spine (Phila Pa 1976). 1982;7:150–158.
- Villiers JC. Combined neurogenic and vascular claudication. S Afr Med J. 1980;57:650–654.
- Ciricillo SF, Weinstein PR. Lumbar spinal stenosis. West J Med. 1993;158(2):171–177.
- Nadeau M, Rosas-Arellano MP, Gurr KR, et al. The reliability of differentiating neurogenic claudication from vascular claudication based on symptomatic presentation. Can J Surg. 2013;56(6):372–377.
- Genevay S, Courvoisier DS, Konstantinou K, et al. Clinical classification criteria for neurogenic claudication caused by lumbar spinal stenosis. The N-CLASS criteria. Spine J. 2018;18(6):941–947.
- Mahé G, Kaladji A, Le Faucheur A, et al. Internal iliac artery stenosis: diagnosis and how to manage it in 2015. Front Cardiovasc Med. 2015;2:33.
- Benjamin EJ, Virani SS, Callaway CW, et al. Heart disease and stroke statistics-2018 update: a report from the American Heart Association. Circulation. 2018;137(12):e67–e492..
- McDermott MM, Greenland P, Liu K, et al. Leg symptoms in peripheral arterial disease: associated clinical characteristics and functional impairment. JAMA. 2001;286:1599–1606.
- Armstrong DW, Tobin C, Matangi MF. The accuracy of the physical examination for the detection of lower extremity peripheral arterial disease. Can J Cardiol. 2010;26(10):e346–e350.
- Walker CM, Bunch FT, Cavros NG, et al. Multidisciplinary approach to the diagnosis and management of patients with peripheral arterial disease. Clin Interv Aging. 2015;10:1147–1153.
- Simonetti I, Pratesi C. Intermittent claudication or neurogenic claudication? “Why don’t you speak to me”? Intern Emerg Med. 2006;1(2): 133. discussion 133-4.