
Abstract
This study proposes and tests a model to provide a more comprehensive understanding of the contribution of chronological age versus age-related ability and motivation factors in explaining recall of online cancer information among older patients (n = 197). Results revealed that recall is not a matter of chronological age per se, but rather a matter of ability and motivation. Age-related ability and motivation factors explained 37.9% of the variance in recall. Health literacy, involvement with the webpage, and satisfaction with the emotional support were positively associated with recall. Furthermore, recall was negatively related to frailty, anger, future time perspective, and perceived cognitive load. The findings pose relevant opportunities for tailoring interventions to improve online information provision for older cancer patients.
Providing information to patients suffering from a severe disease such as cancer is crucial for optimal care. Patients need information to prepare for their treatment, to cope with their illness, and to manage their disease in daily life (De Haes & Bensing, Citation2009). Recall of information, the ability to reproduce and remember information, is a prerequisite to follow up on medical instructions that are needed for daily life disease management (Kravitz et al., Citation1993). Patients should have sufficient understanding of their situation to make informed decisions and adhere to medical regimens. Recall of information has therefore been associated with better medication adherence (Linn, Van Dijk, Smit, Jansen, & Van Weert, Citation2013; Puts et al., Citation2014) and improved well-being (McGuire, Citation1996). Accurate recall of information is especially important for older patients, because they often deal with multiple diseases at the same time, such as cancer, diabetes, and, heart problems (World Health Organization, Citation2014), and thus need to memorize more complex medical information about treatment and disease. However, older age is often associated with poorer recall performance (Jansen et al., Citation2008), also when it concerns recall of online information (Bol et al., 2015).
Patients increasingly turn to the Internet to find disease-relevant information (Fiksdal et al., Citation2014). However, using online technologies for medical information might not be clearly understood by all individuals, such as older adults. Research has shown that older people often see themselves as less able and are often less motivated to utilize the Internet for medical information (Bodie & Dutta, Citation2008). This may hamper accurate uptake and recall of information. At the same time, older individuals differ in how much they recall from, for example, online medical sources. This might be explained by the fact that individual differences increase when people get older (Dannefer, Citation1988). It has therefore been suggested that “age alone is a meaningless demographic” (Lippincott, Citation2004, p. 160). Chronological age may simply function as a catch-all term that consists of many different factors that together help understand systematic differences in older adults recall performances. In recognizing the heterogeneity of the older aged, this paper aims to explore to what extent chronological age versus age-related factors predict recall of online information in older adults. To this end, we will (1) present an overview of factors that, according to previous studies, may be predictive of (online) information recall in older adults, and (2) empirically test which of these factors relate to recall of online information among an older cancer patient population. Understanding these relationships can inform interventions to tailor online information to older patients.
Recall of Online Cancer Information in Older Patients
According to the elaboration likelihood model (ELM: Petty & Cacioppo, Citation1986) and the limited capacity model of motivated mediated messages (LC4MP: A. Lang, Citation2000), information processing is influenced by two overarching factors: ability and motivation. The ability to process information depends on one’s skills and proficiencies, while motivation refers to one’s desire and willingness to process information (MacInnis, Moorman, & Jaworski, Citation1991). Since the current literature lacks a unifying framework aiming at understanding older adults’ ability and motivation to recall information in a cancer communication context, we used the ELM and LC4MP as a guiding framework to identify age-related factors that are expected to predict recall of information. In doing so, we conducted a scoping review to identify ability-related and motivation-related factors relevant for older patients’ recall of online cancer information (scoping review details are available upon request). We distinguished between personal characteristics and message experience characteristics relevant for patients’ ability and motivation to recall information.
Personal Characteristics
Ability
Our review revealed numerous personal characteristics in ability that explain one’s ability to recall information. Given the heterogeneous nature of the older aged, it is expected that older individuals highly differ on personal characteristics relevant for ability, which consequently explains the variance in recall of online cancer information. We expect that some characteristics negatively influence recall of information due to age-related decline, while others positively influence recall due to age-related compensatory mechanisms.
Negative age-related factors as identified by our scoping review are educational level, health literacy, e-health literacy, working memory, frailty, and emotional state. Earlier research has suggested that older adults often have completed lower levels of education (Bostock & Steptoe, Citation2012), which has been found to influence recall of information (Wagner, Wuensch, Friess, & Berberat, Citation2014). Furthermore, health literacy, i.e., “the degree to which individuals can obtain, process, understand, and communicate about health-related information needed to make informed health decisions (Berkman, Davis, & McCormack, Citation2010, p. 16),” declines with age (Baker, Gazmararian, Sudano, & Patterson, Citation2000), which consequently affects recall negatively (McCray, Citation2005). Likewise, older adults low e-health literacy skills, that is “the ability to seek, find, understand, and appraise health information from electronic sources and apply the knowledge gained to addressing or solving a health problem (Norman & Skinner, 2006a, e9),” might also explain why older patients poorly recall information from online sources.
In addition, the negative association between age and recall has also been explained by cognitive and emotional factors, such as working memory, frailty, and emotional state. Age-related decline in working-memory capacity has been widely associated with poor recall of information (Brown & Park, Citation2003). Moreover, older persons often experience simultaneous loss of resources in several domains of functioning, which is referred to as frailty. As frailty is associated with cognitive decline (Buchman, Boyle, Wilson, Tang, & Bennett, Citation2007), it is expected to also negatively influence one’s ability to recall information. Being diagnosed with cancer may elicit emotional states, such as feelings of anxiety, stress, depression, and anger, which might negatively affect recall of information (Christianson, Citation1992; Schwabe & Wolf, Citation2010). According to the attentional narrowing hypothesis, emotionally arousing situations require attentional resources, which leaves fewer resources available for peripheral information, such as treatment information (Christianson & Loftus, Citation1991; Kessels, Citation2003).
On the other hand, some age-related factors positively influence recall of information. These are emotion regulation and prior knowledge. Older people are generally better able to regulate their emotions (Carstensen, Fung, & Charles, Citation2003), which has been found to compensate for cognitive decline in memory (Carstensen & Mikels, Citation2005), and thus positively affects recall. Moreover, older adults have substantial knowledge and experience with illness, which may compensate for age-related decline in information processing (Brown & Park, Citation2003).
Motivation
Secondly, motivation influences older patients’ recall of information in three ways. First, socioemotional selectivity theory suggests that older people generally perceive less time left in life, causing older adults to shift from having knowledge-related goals, i.e., acquisitive behavior geared toward learning, to having more emotional-related goals, i.e., behavior related to emotion regulation (Carstensen, Isaacowitz, & Charles, Citation1999). This implies that they might be less willing to process information, and thus recall information. Second, some older people are more motivated to process information since they generally have a higher need for cognition, that is, the tendency to engage in and enjoy effortful cognitive endeavors (Cacioppo, Petty, & Kao, Citation1984). Third, a monitoring coping style, i.e., the extent to which individuals are approaching potentially negative information to cope with their illness, also influences information processing preferences (Miller, Citation1995): having a higher monitoring coping style could positively affect recall of online cancer information. We thus expect that future time perspective, need for cognition, and a monitoring coping style are positively related to recall of online cancer information among older patients.
Message Experience Characteristics
Ability
Regardless of what a message looks like, individuals can vary in their experience with a message, which may influence the ability to recall information. Since people have limited information processing capacity, it is necessary to be critical in allocating resources to processing information. Cognitive load theory states that the human working memory is limited in the amount of information it can hold and recall (Van Gerven, Paas, Van Merriënboer, Hendriks, & Schmidt, Citation2003). Older adults’ ‘total cognitive capacity’ is generally smaller (Van Gerven, Paas, Van Merriënboer, & Schmidt, Citation2000), but expected to vary across individuals. Factors such as required cognitive resources to process information and perceived cognitive load might thus affect their ability to process information and, consequently, accurate recall of information. We expect that more required resources and higher perceived cognitive load are inversely associated with older patients’ recall of online cancer information.
Motivation
Message experience can also contribute to a person’s motivation to engage in effortful information processing (A. Lang, Citation2006), and consequently recall of information. For instance, involving and emotionally satisfying messages are known to increase patients’ motivation to put cognitive effort into the processing of online information (Bol et al., 2014; Petty & Cacioppo, Citation1986). It has been argued that information is more deeply processed, and thus better recalled, when people are involved with the information (Petty & Cacioppo, Citation1986), and when they are emotionally satisfied with the information (Bol et al., 2014). We thus expect that increased website involvement and satisfaction with the emotional support from the website are positively related to recall of online cancer information among older cancer patients.
The Current Study
To summarize, we discussed personal and message experience characteristics that the literature suggested to be relevant for older adults’ ability and motivation to recall information. To address our first goal, an overview of the aforementioned age-related factors is presented in a conceptual model (see ). To address our second goal, we will empirically test which of these age-related factors contribute to recall of information among an older cancer patient population.
Fig. 1. Conceptual model of ability and motivation factors to recall online cancer information categorized as personal and message experience characteristics.
Methods
Participants
A heterogeneous group of cancer patients was recruited between April and May 2015 from 2 hospitals, a large online panel of cancer patients, and a panel from the research institute. Eligible patients were aged 65 years or older, had sufficient command of Dutch, had no cognitive impairments, had access to the Internet, had not participated in a previous study related to this study’s research line, and had had at least one consultation with their oncologist. Hospital patients who had a follow-up consultation between March 2013 and March 2015 were selected by the local oncology assistants and approached for study participation by telephone. After briefly informing patients about the study, those interested received an email including information about the study and a link to an online questionnaire. For the online panels, the panel managers invited eligible patients by an email that included the same information and link to the online questionnaire. The study was approved by the institutional review board of the research institute, as well as the medical ethics committee and local feasibility advisory committee of the two participating hospitals
Procedure
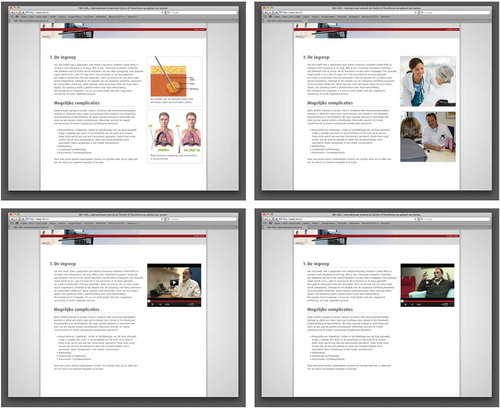
To mimic natural searching behavior and information processing online, we provided patients within the online questionnaire with various webpage designs for patients to actively look for their preferred online information. Hence, five different webpage designs containing the same information, but differing in design (i.e., text, illustrations, video), were presented in a random order on a storyboard within the online questionnaire (see ). Participants were asked to choose the version they would have chosen if they were searching information online. This way, we were able to unravel associations between age-related factors and recall of information, which would reflect patients’ natural behavior when visiting a website. The informational text addressed a relatively unknown treatment, radio frequency ablation (RFA), which is a minimally invasive method to treat metastases in the lung. The webpages’ presentation mode differed as follows: (1) text-only information; (2) text and medical illustrations (i.e., illustrations that explain text); (3) text and non-medical illustrations (i.e., illustrations that are text irrelevant but aim to enhance enjoyment); (4) text and a video in which a doctor explained the RFA treatment; and (5) text and a video in which a patient explained the RFA treatment. The videos in the latter two versions reflected the text. For the video with the doctor, the spoken text was equal to the written text on the webpage. For the video with the patient, minimal stylistic changes were made (i.e., information was presented from a first-person perspective) (for video scripts, see Bol et al., 2013). Besides clicking on videos, the webpages were not interactive. Patients were exposed to the online information of their choice as long as they wanted. However, after turning to the next page with the recall questions, patients were unable to return to the previous page to consult the webpage again. The online questionnaire continued with assessing age-related personal and message experience characteristics deemed relevant for ability and motivation as introduced in our conceptual model.
Fig. 2. Webpages containing RFA treatment information presented in text and medical illustrations (top left), text and non-medical illustrations (top right), text and a video with a doctor (bottom left), and text and a video with a patient (bottom right). Webpage with text-only information is not displayed, since it is equal to the webpages shown in this figure without the illustrations or videos.
Dependent Variable
Recall of information was assessed by eleven open-ended questions reflecting the content of the webpage (Authors, 2014), based on the Netherlands Patient Information Recall Questionnaire (NPIRQ: Jansen et al., Citation2008). Questions included “How much time does RFA treatment take?” and “Can you name the types of sedations that are possible during RFA treatment?”. Answers were to be reported in a text box below each question. They were manually scored based on a codebook. Each answer received a score of 0 (not recalled), 1 (partially recalled), or 2 (completely recalled). A second coder coded the recall scores of 38 patients (19.3%) to establish intercoder reliability (mean kappa = .96, range = .88 – 1.00). Percentages of accurate recall were calculated based on the total recall sum score (range = 0 – 22).
Personal Characteristics
Ability
Education was divided into the lower educational level (0 = primary, lower vocational, preparatory secondary vocational, intermediate secondary vocational education, senior secondary vocational and university preparatory vocational education) and the higher educational level (1 = higher vocational education and university). Health literacy was measured with the SAHL-D (Pander Maat, Essink-Bot, Leenaars, & Fransen, Citation2014), which consists of 22 health-related words, such as psoriasis, hemophilia, and defibrillation, of which the correct meaning could be selected out of four multiple choice options, including the answer option “I do not know.” One point was allocated for each correct answer, resulting in a scale ranging from 0 to 22. E-health literacy was measured using the eHEALS (Norman & Skinner, Citation2006b), an 8-item scale with items such as “I know how to use the Internet to answer my health questions,” reported on a 5-point scale (1 = “strongly disagree,” 5 = “strongly agree,” Cronbach’s α = .94). Working memory was measured with eleven items of the BRIEF-SR (adapted version: Guy, Gioia, & Isquith, Citation2004). Items included “I have difficulties memorizing things, even for a few minutes,” and were provided with the answer options “never,” “sometimes,” and “always.” (Cronbach’s α = .83) Higher scores represent lower levels of working memory. Patients’ frailty in the physical, cognitive, social, and psychosocial domain was assessed using the Groningen Frailty Indicator (Schuurmans, Steverink, Lindenberg, Frieswijk, & Slaets, Citation2004). Scores range between 0 and 15. Higher scores indicate higher levels of frailty. Emotional state was measured using the six-item short-form of the STAI (STAI-6: Marteau & Bekker, Citation1992), including items such as “I feel calm” and “I feel tense,” measured on a 4-point scale (1 = “not at all,” 2 = “somewhat,” 3 = “moderately,” 4 = “very much,” α = .85). Additionally, the Emotion Thermometers Tool (Mitchell, Baker‐Glenn, Granger, & Symonds, Citation2010) assessed current emotional states using three visual-analogue scales guided with the question “How much stress/anger/depression have you experienced during the past week on a scale of 0 to 10?” (range 0 = ‘none’ to 10 = ‘an extreme amount’). Emotional regulation was measured with 10 items of the BRIEF-SR (adapted version: Guy et al., Citation2004). Items included “I get upset by minor things” (1 = “never,” 2 = “sometimes,” 3 = “always,” Cronbach’s α = .81). Higher scores indicate lower levels of emotion regulation. Patients were asked about their prior medical knowledge (i.e., general medical knowledge, medical knowledge about lung cancer, and medical knowledge about RFA treatment) on a 7-point scale (1 = “no knowledge,” 7 = “much knowledge,” Cronbach’s α = .79).
Motivation
Future time perspective was measured by ten items, such as “There are only limited possibilities in my future” (7-point Likert scale ranging from “not at all true” to “very much true,” Cronbach’s α = .90) (F. R. Lang & Carstensen, Citation2002). Higher scores indicate more perceived time left in life. A shortened version of the need for cognition scale was used to measure the tendency to enjoy and engage in thinking (Cacioppo & Petty, Citation1982; Pieters, Verplanken, & Modde, Citation1987). Items included “I find satisfaction in deliberating hard and for long hours,” assessed on a 7-point scale, ranging from “strongly disagree” to “strongly agree” (Cronbach’s α = .78). Monitoring coping style was measured with an adapted version of the Threatening Medical Situation Inventory (Miller, Citation1987; Van Weert et al., Citation2009), using three items, such as “I planned to read as much as possible about my disease,” measured on a 5-point scale (1 = “not at all applicable to me,” 5 = “strongly applicable to me,” Cronbach’s α = .73).
Message Experience Characteristics
Ability
Perceived cognitive load was assessed by one item asking “How much effort did it take to study the web content about RFA?”, to be rated on a 7-point scale ranging from “very little effort” to “a lot of effort” (Paas, Tuovinen, Tabbers, & Van Gerven, Citation2003). Required cognitive resources were assessed by two items of Keller and Block (Citation1997) required resources scale, asking patients to rate the webpage information on a 5-point semantic differential. Items were “easy to comprehend/difficult to comprehend,” and “easy to follow/difficult to follow.” We added two items, asking whether the information “included no medical jargon/much medical jargon,” and “required no prior knowledge/much prior knowledge” (Cronbach’s α = .87).
Motivation
Four items, such as “I was highly involved in evaluating the site,” reflected website involvement (Dutta‐Bergman, Citation2004) (7-point scale, ranging from “strongly disagree” to “strongly agree,” Cronbach’s α = .89). Satisfaction with the emotional support from the website was assessed with a subscale of the Website Satisfaction Scale (Authors, 2014). The four items included, e.g., “The website increases self-confidence” and were measured on a 7-point scale ranging from “totally disagree” to “totally agree” (Cronbach’s α = .96).
Statistical Analysis
Analyses were performed using SPSS version 22 (SPSS, Inc., Chicago, IL). Results were considered significant at a p-value of < .05. Descriptive statistics were used to describe the older cancer patient population. To examine predictors of recall of information, we conducted a multiple linear regression analysis. Five blocks were entered as separate blocks: (1) chronological age, (2) “personal characteristics relevant for ability” variables, (3) “personal characteristics relevant for motivation” variables, (4) “message experience characteristics relevant for ability” variables, and (5) “message experience characteristics relevant for motivation” variables. Chronological age was included as a predictor to test its contribution in predicting recall as compared to age-related ability and motivation factors.
Initially, the choice patients made regarding the mode of delivery of the webpage was included as a predictor as well to account for possible variety in recall due to variety in mode of delivery. However, web choice was not included in the final model, as inclusion did not change the results of the final model. Furthermore, the multiple linear regression model was also executed for the subsample of patients recruited from hospitals to assure that sampling patients online had not affected the final model. The analysis showed only a slight difference between the two models, i.e., when only considering patients from hospitals, website involvement did no longer significantly predict recall.
As the analysis revealed a violation of the assumption of homogeneity of variance for the variables “knowledge” and “required resources,” we log transformed these variables. Afterwards, assumptions of linearity, normality, homoscedasticity, independent errors (Durbin-Watson = 2.191), and multicollinearity (VIF < 10) were met for all variables. One case showed a standardized residual greater than 3 and was therefore removed. Rerunning the analysis, however, did not change the results.
Results
Patient Recruitment and Characteristics
shows the recruitment flow and reasons for exclusion and non-response. Of the 794 patients from the two hospitals, 410 patients (51.6%) were approached to participate in the survey. Of the approached patients, 243 (59.3%) met all inclusion criteria, of which 217 (89.3%) agreed to participate. Of consenting patients, 149 (68.7%) completed the survey, of which 137 (91.9%) were eligible for analysis. For the online panels, 344 patients were approached. In total, 136 patients (39.5%) started the online survey of which 77 (56.6%) completed the survey. Of those, 60 (77.9%) were eligible for analysis.
Fig. 3. Flowchart of participant recruitment. 1Newly diagnosed with cancer (n = 238), deceased (n = 110), participated in previous study (n = 27), cognitive impairment according to medical status (n = 9). 2Deceased (n = 57), no access to Internet or computer (n = 56), could not be reached through telephone (n = 52), did not speak Dutch (n = 2). 3Struggles with Internet use (n = 13), felt too sick or too tired (n = 6), had no time (n = 5), unknown (n = 2). 4Started but did not finish for unknown reasons (n = 52), felt too sick or too tired (n = 5), deceased (n = 5), had no access to Internet or computer (n = 3), had no cancer (n = 2), struggled with questionnaire (n = 1). 5Questionnaire filled out by someone else (n = 7), not exposed to webpage material due to technical issues (n = 2), used other source to answer recall questions (n = 1), did not meet age criterion (< 65 yrs.; n = 2). 6Started but did not finish for unknown reasons (n = 48), did not meet age criterion (< 65 yrs.; n = 11). 7Did not meet age criterion (< 65 yrs.; n = 14), used other source to answer recall questions (n = 2), duplicate entry (n = 1).
The majority of the included patients were male (65.0%), and the mean age was 71 years old (M = 71.03, SD = 4.42). Patients were on average diagnosed 3.5 years ago (M = 42.97 [months], SD = 62.14), and most patients received treatment with curative intent (63.0%). The majority of patients were diagnosed with lung cancer (65.5%), followed by urological cancers (19.3%), and gastroenterological cancers (13.7%). Common treatments among this group of older cancer patients were chemotherapy (48.2%), surgery (43.7%), and radiotherapy (40.6%). Patient characteristics are shown in .
Table 1. Sociodemographic and medical background characteristics and personal and message experience characteristics of older cancer patients (n = 197)
Recall of Information
Overall, patients recalled 33.6% of the information on average (M = 7.38, SD = 4.78, range = 0 – 20). Patients from online panels on average recalled 38.5% of the information correctly (M = 8.47, SD = 4.30, range = 0 – 15). Patients from hospitals had a lower average recall score of 31.4% (M = 6.91, SD = 4.91, range = 0 – 20), F(1, 195) = 4.54, p = .034, ηp2 = .02.
Predictors of Recall of Information
Chronological age accounted for 2.0% of the variance in recall (ΔR2 = .002, p = .551), indicating that chronological age did not predict recall of information. “Personal characteristics relevant for ability” accounted for 28.9% of the variance in recall (ΔR2 = .289, p < .001), suggesting a large contribution to recall of online information. “Personal characteristics relevant for motivation” did not predict information recall (ΔR2 = .020, p = .174). “Message experience characteristics relevant for ability” accounted for 7.6% of the variance in recall (ΔR2 = .076, p < .001). “Message experience characteristics relevant for motivation” accounted for 5.5% of the variance in recall (ΔR2 = .055, p < .001).
The final linear model (see ) including all potential predictors of information recall accounted for 37.9% of the variance in recall of online information (p < .001). Chronological age did not predict recall of information (β = .01, p = .876). Instead, age-related personal and message experience factors relevant for ability and motivation predicted recall. Among personal characteristics influencing ability were lower levels of frailty (β = -.17, p = .049) and anger (β = -.20, p = .022), as well as higher levels of health literacy (β = .18, p = .016). Among personal characteristics influencing motivation were future time perspective (β = -.16, p = .020): the less perceived future time, the more patients recalled. Of the experienced message variables that influenced ability, the less perceived cognitive load perceived was associated with better recall (β = -.28, p = .001). Of the message experience variables influencing motivation, website involvement (β = .12, p = .046) and satisfaction with the emotional support from the website (β = .19, p = .003) positively predicted recall, i.e., high levels of website involvement and satisfaction were related to better recall.
Table 2. Final linear model of personal and message experience predictors of recall of information
Discussion
We aimed to provide a more comprehensive understanding of the contribution of chronological age versus age-related factors in explaining recall of online cancer information among older patients. Potential recall predicting factors were categorized in terms of personal and message experience characteristics as relevant for older patients’ ability and motivation to recall online cancer information. Our main finding is that, among older cancer patients, recall of online cancer information is not a matter of chronological age per se, but rather a matter of ability and motivation, both constituting of personal and message experience characteristics. These age-related ability and motivation factors explained 37.9% of the variance in recall of online information. Personal characteristics relevant for ability contributed most to explaining recall of information, followed by message experience characteristics relevant for ability, and message experience characteristics relevant for motivation. Chronological age and personal characteristics relevant for motivation did not contribute to recall of information. These results indicate that in older age recall of online cancer information is related to a wide variety of age-related factors but not to chronological age.
Of the personal characteristics relevant for ability, frailty, and anger were negatively associated recall of information. At the same time, higher levels of health literacy were positively associated. This was in line with our expectations. Yet, contrary to our expectation was the finding that of the personal characteristics relevant for motivation, future time perspective was negatively related to recall of information. We had argued that older adults experiencing little time left in life might be less willing to process information. We based this expectation on the theoretical assumptions of the socioemotional selectivity theory. Now, we tentatively argue that information might be essential especially for patients approaching the end of life, as they have to decide what treatment strategy is preferred given their limited time perspective. This can render information more important and enhance their willingness to process, and consequently recall information.
In terms of message experience characteristics relevant for ability, experiencing higher levels of perceived cognitive load to process the information was related to less recall. Perceived cognitive load was the strongest recall predictor in our model. In addition, message experience characteristics relevant for motivation positively related to accurate recall of information. As expected, we found that website involvement and satisfaction with the emotional support from the website were positively associated with recall, suggesting that the more involved with processing online content and the more satisfied with the perceived emotional support from such content, the better patients recalled information from online cancer sources.
Other personal characteristics relevant for ability (i.e., working memory, anxiety, stress, depression, emotion regulation, prior medical knowledge, e-health literacy, educational level) and motivation (i.e., need for cognition, monitoring coping style), as well as message experience characteristics relevant for ability (i.e., required cognitive resources), did not correlate with recall of information in the final model. Nevertheless, our results revealed the most important age-related processes in recall of online cancer information.
Implications for Theory and Practice
Our findings relate to the ELM and LC4MP, which explicate that information processing is influenced by ability and motivation (A. Lang, Citation2000; Petty & Cacioppo, Citation1986). In line with the LC4MP, our study underlines the importance of considering ability and, to some extent, motivation from both a personal and message experience perspective. Importantly, we made a first attempt to specify age-related personal and message experience factors that are relevant for ability and motivation. Whereas earlier work focused on conceptualizing ability and motivation (e.g., A. Lang, Citation2000; Petty & Cacioppo, Citation1986), we focused on categorizing important recall-predicting concepts to operationalize ability and motivation to recall online cancer information among older patients.
By identifying ability and motivation factors that predict recall of information, we are able to use these as criteria to select those older patients that are most at risk for poor recall of online cancer information and, consequently, for other health outcomes. These criteria tell us more about the process of aging than chronological age per se. Our findings suggest that we should consider age-related factors such as frailty, anger, health literacy, future time perspective, perceived cognitive load, website involvement, and satisfaction with the emotional support from the website. This poses opportunities for tailoring interventions. Chronological age cannot be changed, but addressing relevant age-related factors may help to improve information provision for older cancer patients. Further research is needed to explore how these factors can be translated into practical tools that support the individual older patient.
Limitations
This study also has limitations. First, the design was cross-sectional, rather than longitudinal or experimental, meaning that a causal relationship between age-related factors and recall of information cannot be assumed. We were able to confirm the model for our patient sample and the subsample of patients recruited from hospitals, but further research is desirable to test the generalizability and robustness of our results in a heterogeneous group of cancer patients. Our model should therefore be tested among other subsets of cancer patients.
Furthermore, our theoretical model is limited by message characteristics that are experienced by the message recipient. We wanted to keep the information on the webpage as constant as possible to ensure that recall was a function of the age-related factors introduced rather than a function of various message-related factors that would interfere with age-related factors. For instance, if this study would have aimed to determine the role of text complexity, length, or type, we would have had to create different types of information, which calls for different research designs, such as experiments (Bol et al., 2014; Van Weert et al., 2011).
Further research might also invite patients to browse on a website rather than viewing one webpage only. For example, e-health literacy might have played a larger role when patients had to visit a full website rather than one webpage. This suggests that some age-related factors only predict recall under certain conditions, but it can also mean that some do not predict recall at all. We therefore suggest to test the proposed model in different settings.
Conclusions
Our study aimed at gaining a more comprehensive understanding of online cancer information recall among older cancer patients. Our proposed model indeed explained a substantial amount of variance in online information recall by introducing age-related factors in ability and motivation rather than chronological age. Yet, further research should explore other factors, such as message-related factors, to optimize the model in explaining recall information among older cancer patients. Moreover, ways to translate these findings into practice are needed to tailor communication to older cancer patients’ ability and motivation to recall online cancer information. As the Internet is increasingly used as a source of cancer information, new strategies for delivering cancer information on the Internet must be developed that accommodate a diverse and heterogeneous group of older cancer patients.
Acknowledgments
We wish to thank the participating hospitals (Netherlands Cancer Institute and Deventer hospital) and, in particular, the oncology assistants Daphne Robert and Annette Hemels for their assistance during data collection. We also thank Melanie de Looper, Stephanie Immerzeel, Kirsten Hamelink, Maartje Hendriks, and Ashley den Toom for helping to recruit participants. Furthermore, we would like to thank kanker.nl for their help with recruiting patients online. We thank Remco Sanders, Remao Tummers, Melanie de Looper, Kirsten Hamelink, Joost Daams, and Stefano Giani for their assistance in reviewing the literature for recall predictors. Moreover, we like to thank Renske van Bronswijk for translating the English need for cognition items into Dutch, and Melanie de Looper for partly coding the recall scores and assessing the intercoder reliability. Last but not least, we would like to show our gratitude to all patients willing to participate in this study.
Funding
This study was funded by the Dutch Cancer Society (KWF, grant no. UVA 2014-7288). KWF management was not involved in the study design, data collection, data analysis and interpretation, and manuscript preparation
Additional information
Funding
References
- Baker, D. W., Gazmararian, J. A., Sudano, J., & Patterson, M. (2000). The association between age and health literacy among elderly persons. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 55(6), S368–S374. doi:10.1093/geronb/55.6.S368
- Berkman, N. D., Davis, T. C., & McCormack, L. (2010). Health literacy: What is it? Journal of Health Communication, 15(S2), 9–19. doi:10.1080/10810730.2010.499985
- Bodie, G. D., & Dutta, M. J. (2008). Understanding health literacy for strategic health marketing: EHealth literacy, health disparities, and the digital divide. Health Marketing Quarterly, 25(1–2), 175–203. doi:10.1080/07359680802126301
- Bol, N., Smets, E. M. A., Eddes, E. H., De Haes, H. C. J. M., Loos, E. F., & Van Weert, J. C. M. (2015). Illustrations enhance older colorectal cancer patients’ website satisfaction and recall of online cancer information. European Journal of Cancer Care, 24(2), 213–223. doi:10.1111/ecc.12283
- Bol, N., Smets, E. M. A., Rutgers, M. M., Burgers, J. A., De Haes, J. C. J. M., Loos, E. F., & Van Weert, J. C. M. (2013). Do videos improve website satisfaction and recall of online cancer-related information in older lung cancer patients? Patient Education and Counseling, 92(3), 404–412. doi:10.1016/j.pec.2013.06.004
- Bol, N., Van Weert, J. C. M., De Haes, J. C. J. M., Loos, E. F., De Heer, S., Sikkel, D., & Smets, E. M. A. (2014). Using cognitive and affective illustrations to enhance older adults’ website satisfaction and recall of online cancer-related information. Health Communication, 29(7), 678–688. doi:10.1080/10410236.2013.771560
- Bostock, S., & Steptoe, A. (2012). Association between low functional health literacy and mortality in older adults: Longitudinal cohort study. BMJ (Clinical Research Ed.), 344, e1602. doi:10.1136/bmj.e1602
- Brown, S. C., & Park, D. C. (2003). Theoretical models of cognitive aging and implications for translational research in medicine. The Gerontologist, 43(suppl 1), 57–67. doi:10.1093/geront/43.suppl_1.57
- Buchman, A. S., Boyle, P. A., Wilson, R. S., Tang, Y., & Bennett, D. A. (2007). Frailty is associated with incident alzheimer’s disease and cognitive decline in the elderly. Psychosomatic Medicine, 69(5), 483–489. doi:10.1097/psy.0b013e318068de1d
- Cacioppo, J. T., & Petty, R. E. (1982). The need for cognition. Journal of Personality and Social Psychology, 42(1), 116–131. doi:10.1037/0022-3514.42.1.116
- Cacioppo, J. T., Petty, R. E., & Kao, C. F. (1984). The efficient assessment of need for cognition. Journal of Personality Assessment, 48(3), 306–307. doi:10.1207/s15327752jpa4803_13
- Carstensen, L. L., Fung, H. H., & Charles, S. T. (2003). Socioemotional selectivity theory and the regulation of emotion in the second half of life. Motivation and Emotion, 27(2), 103–123. doi:10.1023/A:1024569803230
- Carstensen, L. L., Isaacowitz, D. M., & Charles, S. T. (1999). Taking time seriously: A theory of socioemotional selectivity. American Psychologist, 54(3), 165–181. doi:10.1037//0003-066X.54.3.165
- Carstensen, L. L., & Mikels, J. A. (2005). At the intersection of emotion and cognition. Current Directions in Psychological Science, 14(3), 117–121. doi:j.0963-7214.2005.00348.x/j.0963-7214.2005.00348.x
- Christianson, S.-A. (1992). Emotional stress and eyewitness memory: A critical review. Psychological Bulletin, 112(2), 284–309. doi:10.1037/0033-2909.112.2.284
- Christianson, S.-A., & Loftus, E. F. (1991). Remembering emotional events: The fate of detailed information. Cognition & Emotion, 5(2), 81–108. doi:10.1080/02699939108411027
- Dannefer, D. (1988). What’s in a name?: An account of the neglect of variability in the study of aging. In J. E. Birren, & V. L. Bengtson (Eds.), Emergent theories of aging (pp. 356–384). New York, NY: Springer Publishing Co.
- De Haes, J. C. J. M., & Bensing, J. (2009). Endpoints in medical communication research, proposing a framework of functions and outcomes. Patient Education and Counseling, 74(3), 287–294. doi:10.1016/j.pec.2008.12.006
- Dutta‐Bergman, M. J. (2004). The impact of completeness and web use motivation on the credibility of e‐Health information. Journal of Communication, 54(2), 253–269. doi:10.1111/j.1460-2466.2004.tb02627.x
- Fiksdal, A. S., Kumbamu, A., Jadhav, A. S., Cocos, C., Nelsen, L. A., Pathak, J., & McCormick, J. B. (2014). Evaluating the process of online health information searching: A qualitative approach to exploring consumer perspectives. Journal of Medical Internet Research, 16(10), e224. doi:10.2196/jmir.3341
- Guy, S. C., Gioia, G. A., & Isquith, P. K. (2004). BRIEF-SR: Behavior rating inventory of executive function–Self-Report version: Professional manual. Lutz, FL: Psychological Assessment Resources.
- Jansen, J., Butow, P. N., Van Weert, J., Van Dulmen, S., Devine, R. J., Heeren, T. J., … Tattersall, M. H. N. (2008). Does age really matter? Recall of information presented to newly referred patients with cancer. Journal of Clinical Oncology, 26(33), 5450–5457. doi:10.1200/JCO.2007.15.2322
- Jansen, J., Van Weert, J., Van der Meulen, N., Van Dulmen, S., Heeren, T., & Bensing, J. (2008). Recall in older cancer patients: Measuring memory for medical information. The Gerontologist, 48(2), 149–157. doi:10.1093/geront/48.2.149
- Keller, P. A., & Block, L. G. (1997). Vividness effects: A resource-matching perspective. Journal of Consumer Research, 24(3), 295–304. doi:10.1086/209511
- Kessels, R. P. C. (2003). Patients’ memory for medical information. Journal of the Royal Society of Medicine, 96(5), 219–222. doi:10.1258/jrsm.96.5.219
- Kravitz, R. L., Hays, R. D., Sherbourne, C. D., DiMatteo, M. R., Rogers, W. H., Ordway, L., & Greenfield, S. (1993). Recall of recommendations and adherence to advice among patients with chronic medical conditions. Archives of Internal Medicine, 153(16), 1869–1878. doi:10.1001/archinte.1993.00410160029002
- Lang, A. (2000). The limited capacity model of mediated message processing. Journal of Communication, 50(1), 46–70. doi:10.1111/j.1460-2466.2000.tb02833.x
- Lang, A. (2006). Using the limited capacity model of motivated mediated message processing to design effective cancer communication messages. Journal of Communication, 56(s1), S57–S80. doi:10.1111/j.1460-2466.2006.00283.x
- Lang, F. R., & Carstensen, L. L. (2002). Time counts: Future time perspective, goals, and social relationships. Psychology and Aging, 17(1), 125–139. doi:10.1037//0882-7974.17.1.125
- Linn, A. J., Van Dijk, L., Smit, E. G., Jansen, J., & Van Weert, J. C. M. (2013). May you never forget what is worth remembering: The relation between recall of medical information and medication adherence in patients with inflammatory bowel disease. Journal of Crohn’s & Colitis, 7(11), e543–e550. doi:10.1016/j.crohns.2013.04.001
- Lippincott, G. (2004). Gray matters: Where are the technical communicators in research and design for aging audiences? IEEE Transactions on Professional Communication, 47(3), 157–170. doi:10.1109/TPC.2004.833687
- MacInnis, D. J., Moorman, C., & Jaworski, B. J. (1991). Enhancing and measuring consumers’ motivation, opportunity, and ability to process brand information from ads. The Journal of Marketing, 55(4), 32–53. doi:10.2307/1251955
- Marteau, T. M., & Bekker, H. (1992). The development of a six‐item short‐form of the state scale of the Spielberger State—Trait Anxiety Inventory (STAI). British Journal of Clinical Psychology, 31(3), 301–306. doi:10.1111/j.2044-8260.1992.tb00997.x
- McCray, A. T. (2005). Promoting health literacy. Journal of the American Medical Informatics Association, 12, 152–163. doi:10.1197/jamia.M1687
- McGuire, L. C. (1996). Remembering what the doctor said: Organization and adults’ memory for medical information. Experimental Aging Research, 22(4), 403–428. doi:10.1080/03610739608254020
- Miller, S. M. (1987). Monitoring and blunting: Validation of a questionnaire to assess styles of information seeking under threat. Journal of Personality and Social Psychology, 52(2), 345–353. doi:10.1037/0022-3514.52.2.345
- Miller, S. M. (1995). Monitoring versus blunting styles of coping with cancer influence the information patients want and need about their disease. Cancer, 76(2), 167–177. doi:10.1002/1097-0142
- Mitchell, A. J., Baker‐Glenn, E. A., Granger, L., & Symonds, P. (2010). Can the distress thermometer be improved by additional mood domains? part I. initial validation of the emotion thermometers tool. Psycho‐Oncology, 19(2), 125–133. doi:10.1002/pon.1523
- Norman, C. D., & Skinner, H. A. (2006a). eHEALS: The eHealth literacy scale. Journal of Medical Internet Research, 8(4), e27. doi:10.2196/jmir.8.4.e27
- Norman, C. D., & Skinner, H. A. (2006b). eHealth literacy: Essential skills for consumer health in a networked world. Journal of Medical Internet Research, 8(2), e9. doi:10.2196/jmir.8.2.e9
- Norman, C. D., & Skinner, H. A. (2006b). eHealth literacy: Essential Skills for Consumer Health in a Networked World. Journal of Medical Internet Research, 8(2), e9. doi:10.2196/jmir.8.2.e9
- Paas, F., Tuovinen, J. E., Tabbers, H., & Van Gerven, P. W. M. (2003). Cognitive load measurement as a means to advance cognitive load theory. Educational Psychologist, 38(1), 63–71. doi:10.1207/S15326985EP3801_8
- Pander Maat, H., Essink-Bot, M. L., Leenaars, K. E. F., & Fransen, M. P. (2014). A short assessment of health literacy (SAHL) in the Netherlands. BMC Public Health, 14(1), 990. doi:10.1186/1471-2458-14-990
- Pander Maat, H., Essink-Bot, M. L., Leenaars, K. E. F., & Fransen, M. P. (2014). A short assessment of health literacy (SAHL) in the netherlands. BMC Public Health, 14(1), 990. doi:10.1186/1471-2458-14-990
- Petty, R. E., & Cacioppo, J. T. (1986). The elaboration likelihood model of persuasion. Advances in Experimental Social Psychology, 19(1), 123–205. doi:10.1016/S0065-2601(08)60214-2
- Pieters, R. G. M., Verplanken, B., & Modde, J. M. (1987). ‘Neiging tot nadenken’: Samenhang met beredeneerd gedrag. Nederlands Tijdschrift Voor De Psychologie, 42(2), 62–70.
- Puts, M. T., Tu, H. A., Tourangeau, A., Howell, D., Fitch, M., Springall, E., & Alibhai, S. M. (2014). Factors influencing adherence to cancer treatment in older adults with cancer: A systematic review. Annals of Oncology, 25(3), 564–577. doi:10.1093/annonc/mdt433
- Schuurmans, H., Steverink, N., Lindenberg, S., Frieswijk, N., & Slaets, J. P. J. (2004). Old or frail: What tells us more? The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 59(9), M962–M965. doi:10.1093/gerona/59.9.M962
- Schwabe, L., & Wolf, O. T. (2010). Learning under stress impairs memory formation. Neurobiology of Learning and Memory, 93(2), 183–188. doi:10.1016/j.nlm.2009.09.009
- Van Gerven, P. W. M., Paas, F., Van Merriënboer, J. J. G., Hendriks, M., & Schmidt, H. G. (2003). The efficiency of multimedia learning into old age. British Journal of Educational Psychology, 73(4), 489–505. doi:10.1348/000709903322591208
- Van Gerven, P. W. M., Paas, F. G. W. C., Van Merriënboer, J. J. G., & Schmidt, H. G. (2000). Cognitive load theory and the acquisition of complex cognitive skills in the elderly: Towards an integrative framework. Educational Gerontology, 26(6), 503–521. doi:10.1080/03601270050133874
- Van Weert, J., Jansen, J., De Bruijn, G. J., Noordman, J., Van Dulmen, S., & Bensing, J. M. (2009). QUOTEchemo: A patient-centred instrument to measure quality of communication preceding chemotherapy treatment through the patient’s eyes. European Journal of Cancer, 45(17), 2967–2976. doi:10.1016/j.ejca.2009.06.001
- Wagner, J., Wuensch, A., Friess, H., & Berberat, P. (2014). Surgeon–Patient communication in oncology. European Journal of Cancer Care, 23(5), 585–593. doi:10.1111/ecc.12177
- World Health Organization. (2014). Ageing and life course: Facts about ageing. Retrieved from http://www.who.int/ageing/about/facts/en/