
Abstract
This study examined the relationship between recalled exposure to the We Can Do This COVID-19 Public Education Campaign (the Campaign) and COVID-19 vaccine confidence (the likelihood of vaccination or vaccine uptake) in the general population, including vaccine-hesitant adults (the “Movable Middle”). Analyses used three waves of a triannual, nationally representative panel survey of adults in the U.S. fielded from January to November 2021 (n = 3,446). Proportional odds regression results demonstrated a positive, statistically significant relationship between past 4-month Campaign recall and vaccine confidence, controlling for lagged reports of Campaign recall and vaccine confidence; concurrent and lagged fictional campaign recall; survey wave; and sociodemographics. Results indicated that as one moves from no Campaign recall to infrequent recall, there is a 29% increase in the odds of being in a higher vaccine confidence category. Findings offer evidence of the impact of a COVID-19 public education campaign on increasing vaccine confidence.
The COVID-19 pandemic represents one of the most challenging public health issues of the 21st century. As of February 6, 2023, the pandemic has led to more than 102 million COVID-19 cases and more than 1 million COVID-19 deaths in the United States (U.S.) alone (Centers for Disease Control and Prevention [CDC], Citation2023). The pandemic has been tied to dramatic changes in daily life, including poorer physical and mental health status, social functioning, and quality of life (Jacobs et al., Citation2020); declines in physical activity and sleep (Giuntella, Hyde, Saccardo, & Sadoff, Citation2021); and negative impacts on hours worked and unemployment (U.S. Government Accountability Office [GAO], Citation2022); and was accompanied by significant job loss, food insecurity, and financial instability (Center on Budget and Policy Priorities [CBPP], Citation2022).
Vaccination is the best method available to prevent severe symptoms, hospitalization, and death due to COVID-19 (CDC, Citation2022b). From mid-December 2020 to the end of March 2022, it has been estimated that COVID-19 vaccines have prevented more than 66 million COVID-19 cases and 17 million COVID-19–related hospitalizations, saving more than 2 million lives and almost $900 billion in health care costs in the U.S. alone (Schneider et al., Citation2022). Recent research has shown that compared to unvaccinated adults, vaccinated adults without a booster are 5 times less likely to be hospitalized and 14 times less likely to die from COVID-19 (CDC, Citation2022a; The White House, Citation2022), and both the vaccines and booster shots have demonstrated effectiveness against reinfection resulting in hospitalization (CDC, Citation2021a). These findings underscore the importance of widespread vaccination against COVID-19 to protect against infection, hospitalization, and death.
Despite the availability of free COVID-19 vaccines, many American adults were initially vaccine hesitant. Some adults reported concerns about the speed of the vaccines’ development and testing (Cassata, Citation2021), perceived by many as rushed. Others expressed skepticism about vaccination due to low levels of trust in the government, medicine, and science (Kennedy, Tyson, & Funk, Citation2022; Latkin, Dayton, Yi, Konstantopoulos, & Boodram, Citation2021); for Black Americans and other people of color, this can be attributed, in part, to the traumatic legacy of events such as the Tuskegee Syphilis Study (Scharff et al., Citation2010) and discriminatory practices in medical contexts (Williams & Rucker, Citation2000). Other obstacles to COVID-19 vaccination include low concern about potentially severe consequences from the virus and distrust in political leadership (Lalot, Heering, Rullo, Travaglino, & Abrams, Citation2020), perceptions that preventive behavior enforcement infringes on personal freedoms (Lithwick, Citation2020), and rampant misinformation in the form of conspiracy theories, false content, and COVID-19 facts presented in misleading ways (Agley & Xiao, Citation2021).
In January 2021, after a limited supply of COVID-19 vaccines had been made available to priority groups, 32.2% of adults indicated that they would wait to get vaccinated for one or several reasons (U.S. Department of Health and Human Services [HHS], 2021a). By April 2021, COVID-19 vaccines were available to all American adults (HHS, Citation2022); in that month, although 62.9% of adults reported having received at least one dose of a COVID-19 vaccine or indicated that they would get a vaccine as soon as they could, 20.7% of adults reported that they would wait to get vaccinated for one or several reasons (HHS, Citation2021b). The continued gap in COVID-19 vaccination rates among adults in the U.S. warranted efforts to educate the public about vaccination to increase vaccine uptake.
The We Can Do This COVID-19 Public Education Campaign
Public education campaigns are a valuable tool for reaching and engaging large segments of the population through routine mass media use and are thus well suited for educating the public about COVID-19 vaccines to increase vaccination. Such campaigns influence campaign-targeted outcomes (e.g., vaccine confidence and uptake) through the dissemination of advertisements on media channels and have been shown to influence a range of health behaviors (Hornik, Citation2002a; Noar, Citation2006; Noar, Palmgreen, Chabot, Dobransky, & Zimmerman, Citation2009; Swanton, Allom, & Mullan, Citation2015; Wakefield, Loken, & Hornik, Citation2010; Yadav & Kobayashi, Citation2015).
The U.S. Department of Health and Human Services (HHS) launched the We Can Do This COVID-19 Public Education Campaign (the Campaign) in April 2021 to increase COVID-19 vaccine confidenceFootnote1 and, ultimately, vaccine uptake among American adults ages 18 and older.Footnote2 As children became eligible for vaccines and adults became eligible for booster shots, the Campaign expanded to increase vaccine confidence among parents (for their eligible children) and booster-eligible adults. To effectively reach target audiences, the Campaign deployed a multimedia and multi-channel strategy that evolved over time. Initially, the Campaign comprised 30- and 60-second radio and audiovisual advertisements disseminated through digital and social media channels and has since expanded to include a rich mix of media channels and tactics, including engagement with influencers, trusted messengers, and partner organizations to deliver relevant, persuasive communications to vaccine-hesitant audiences. The Campaign also launched national and local TV advertisements, engaging simultaneously with the general adult population and with specific racial and ethnic audiences through tailored, geographically targeted communications in various languages. While there is no COVID-19-specific standard for public education campaign size, CDC’s Best Practices User Guide for Health Communications in Tobacco Prevention and ControlFootnote3 suggests that tobacco prevention and control campaigns should regularly reach at least 75% of their audience to elicit changes in targeted, population-level outcomes such as behavior and behavioral constructs (CDC, Citation2014). The Campaign reached over 90% of U.S. adults (thereby exceeding the CDC benchmark), disseminating billions of advertising impressions through a paid media channel mix composed largely of TV and digital (including social) media (Nielsen, Citation2021).
Theoretical Framework
The success of a public education campaign and of its evaluation rests, in part, on the health behavior of interest and frequency with which the behavior should be performed (Wakefield, Loken, & Hornik, Citation2010), as well as the theoretical framework on which it is situated (Hornik & Yanovitzky, Citation2003). The Campaign is grounded in a theoretical framework that combines several theories of behavior change and communication, with the expectation that exposure to Campaign messages prompts change in cognitions antecedent to Campaign-targeted behavior (Hornik, Citation2002b).
According to theories of message effects and persuasion, messages that are motivationally relevant elicit more resource allocation to message encoding and storage, facilitating greater recall (Lang, Citation2000) and more durable persuasive effects (Petty & Cacioppo, Citation1986; Petty & Wegener, Citation1999). Given the salience of COVID-19 messaging, it is feasible that Campaign messages that educate audiences about targeted topics (e.g., the benefits of vaccination) are readily encoded in individuals’ memories, enabling subsequent changes in Campaign-targeted outcomes. Focal behavior change theories include the theory of planned behavior (previously, the theory of reasoned action; Fishbein & Ajzen, Citation2011), the health belief model (Rosenstock, Strecher, & Becker, Citation1988, Citation1988), and the transtheoretical (stages of change) model (Prochaska & DiClemente, Citation1983). Together, these theories suggest that a common set of variables, which includes beliefs, attitudes, and behavioral intentions, underlie behavior. The changes in cognitions elicited by Campaign exposure are not only expected to induce change in behavioral constructs of interest (e.g., vaccination intentions) by providing the information needed to make decisions about a salient, motivationally-relevant topic (COVID-19 vaccination), but also to lead to downstream effects on vaccination behavior.
This study aimed to assess potential Campaign impact by examining the relationship between recalled Campaign exposure and COVID-19 vaccine confidence among American adults. During the study period (January 21–November 3, 2021), the Campaign additionally aimed to influence the “Movable Middle” segment of the population—vaccine-hesitant individuals who had not yet decided whether to get a COVID-19 vaccine. We additionally focused our reporting of results on those pertaining to the Movable Middle.
Methods
Data
Analyses were conducted with data from the first three waves of the COVID-19 Attitudes and Beliefs Survey (CABS), a nationally representative, probability-sampled longitudinal survey of American adults administered every 4 months starting in January 2021. The 35-minute, web-based survey measures COVID-19 vaccination; attitudes and beliefs relevant to COVID-19 and preventive behaviors; recalled Campaign exposure; sociodemographic characteristics; and other items. This study was approved by the Biomedical Research Alliance of New York (protocol 20-077-821).
Respondents were recruited through the NORC at the University of Chicago’s national, probability-based AmeriSpeak research panel (NORC, Citation2019).Footnote4 A total of 4,398 respondents completed the Wave 1 survey (fielded January–February 2021), of whom 3,962 completed the Wave 2 survey (fielded May–June 2021), and 3,642 completed the Wave 3 survey (fielded September–November 2021). Wave-to-wave panel retention was high, with 90%–92% of respondents from waves 1 and 2 participating in the subsequent waves. The study sample comprised 3,446 respondents who completed at least the first two survey waves and for whom there was no missing data for the independent and dependent variables.
Measures
Dependent Variable
The dependent variable was vaccine confidence, defined as the self-reported likelihood of getting a COVID-19 vaccine (among unvaccinated respondents) or whether a respondent had received at least one dose of a COVID-19 vaccine.Footnote5 Vaccine confidence was developed by combining two items—likelihood of COVID-19 vaccination (1=very unlikely, 5=very likely) and COVID-19 vaccine uptake (1=received at least one dose of a COVID-19 vaccine)—and was coded into three categories: (1) Vaccine Confident respondents indicated they had received at least one dose of a COVID-19 vaccine or, if they were unvaccinated, reported that they are very likely to get vaccinated; (2) Movable Middle respondents indicated they had not received at least one dose of a COVID-19 vaccine and reported that they are somewhat likely, neither likely nor unlikely, or somewhat unlikely to get vaccinated;Footnote6 and (3) Vaccine Refuser respondents indicated they had not received at least one dose of a COVID-19 vaccine and reported that they are very unlikely to get vaccinated.
Independent Variables
The primary independent variable was aided recallFootnote7 of exposure to the Campaign over the past 4 months (Campaign recall). Respondents were shown an image collage, audio, and/or audiovisual clips of paid Campaign content that aired during the 4 months before the fielding of each survey wave (see example in Figure S1) and were asked to indicate whether they recalled having seen or heard the Campaign and, if so, the frequency of their recalled exposure (0=never, 4=very often). Respondents were defined as having no Campaign recall if they reported not having not seen or heard any Campaign content in the past 4 months. Respondents were defined as having infrequent Campaign recall if they reported having seen or heard Campaign content rarely or sometimes in the past 4 months. Respondents were defined as having frequent Campaign recall if they reported having seen or heard Campaign content often or very often in the past 4 months.
Campaign-Relevant Covariates
As a complement to our Campaign recall measures and to account for potential acquiescence or agreement bias (the tendency to select a positive response option more frequently than circumstances warrant; Bentler, Jackson, & Messick, Citation1971) on Campaign recall reporting, we assessed recall of a plausible, fictional COVID-19 campaign that had never been in market (see supplemental materials for details). Respondents were defined as having any fictional campaign recall if they reported having seen or heard the fictional campaign rarely, sometimes, often, or very often.
In the months before the Wave 1 survey fielding, when COVID-19 vaccines were not available to all American adults, HHS advertising focused on the promotion of COVID-19 preventive measures other than vaccination (e.g., face mask use, social distancing) through the Slow the Spread campaign messaging. After Wave 1, in April 2021, the Campaign’s focus shifted with the introduction of the We Can Do This campaign to increasing COVID-19 vaccine confidence, including uptake. To account for differences in the Campaign content that aired before each survey wave along with other historical shifts in the environment, we included survey wave as a covariate (dichotomized; Wave 2 = 0 and Wave 3 = 1).
Sociodemographic Covariates
Research has shown that a range of sociodemographic characteristics are associated with COVID-19 vaccine hesitancy and uptake (Edwards, Biddle, Gray, & Sollis, Citation2021; Murphy et al., Citation2021; Rane et al., Citation2022). Analyses controlled for a series of key sociodemographic factors (assessed in Wave 1) that might confound the relationship between Campaign recall and vaccine confidence. Sociodemographic covariates included respondent age (18–24, 25–44, 45–64, 65+), gender (male, female), race/ethnicity (non-Hispanic White, American Indian or Alaskan Native, non-Hispanic Asian American or Pacific Islander, non-Hispanic Black, Latino, non-Hispanic Multiple Races or Other IdentityFootnote8), education (no college, some college, bachelor’s degree or higher), annual household income (less than $50,000; $50,000–$74,999; $75,000–$99,999; $100,000 and greater), political ideology (liberal, moderate, conservative), U.S. Census Region of residence (Northeast, Midwest, South, West),Footnote9 rurality (urban, suburban, rural), essential worker status (essential worker, non-essential worker), and having a preexisting health condition (preexisting health condition, no condition). Household income, essential worker status, and preexisting health condition were all assessed in Wave 1. See supplemental materials for details about rurality, essential worker, and preexisting health condition variables. The other sociodemographic variables reflect metadata obtained from the NORC AmeriSpeak panel frame.
Analyses
The primary analysis was a proportional odds, or ordered logistic regression model, with within-person cluster-adjusted standard errors, in which vaccine confidence at each wave (waves 2 and 3) was predicted by past 4-month Campaign recall, as assessed at that wave. The model specified variables representing lagged (by one wave) vaccine confidence and past 4-month Campaign recall as predictor variables to effectively treat both vaccine confidence and Campaign recall as change variables. The model controlled for current and lagged fictional campaign recall and for current survey wave. We expected that if the relationship between Campaign recall and vaccine confidence remained significant when controlling for fictional campaign recall, it would be unlikely that the relationship between Campaign recall and vaccine confidence would reflect response bias. Further, controlling for lagged vaccine confidence controls for the possibility that those who are more vaccine confident at the current time are more likely to recall the Campaign because of their vaccine confidence. Both concurrent and lagged versions of vaccine confidence and past 4-month Campaign recall variables were polynomial contrast coded (Davis, Citation2010), with each specified as both linear and quadratic predictors. Both concurrent and lagged versions of fictional campaign recall, survey wave, and all sociodemographic covariates were dummy coded. The model was weighted using survey weights that corresponded with the wave during which the dependent variable was measured (see supplemental materials for weighting details).
The analysis data set was formatted in long form with a separate row per wave per respondent-observation and included all valid responses from respondents who completed at least two survey waves. The analysis was conducted in R statistical software (R Core Team, Citation2022) using the polr function from the MASS package (Venables & Ripley, Citation2002), with assistance from the sandwich (Zeileis, Citation2006; Zeileis, Köll, & Graham, Citation2020) and parameters (Lüdecke, Ben-Shachar, Patil, & Makowski, Citation2020) packages.
Results
Descriptive Results
presents the sociodemographic characteristics of the study sample.
Table 1. Sociodemographic Characteristics of the Study Sample as of January–February 2021
Just over half of the study sample (56.3%) was 45 years old or older, and the gender of respondents was evenly split (51.8% female). Most respondents were non-Hispanic White (69.4%), with smaller proportions of respondents identifying as either Hispanic/Latino (17.6%) or non-Hispanic Black (13.0%). Approximately two-thirds (65.7%) of respondents reported they did not have a college degree, and most respondents reported a household income of less than $75,000 per year (65.2%). Although the plurality of respondents were politically moderate (37.1%), just over one-third (35.2%) of respondents identified as conservative, and less than one-third (27.7%) of respondents identified as liberal. Respondents were fairly distributed across U.S. Census Regions. Nearly half of respondents reported living in suburban areas (44.7%), and more than one-third (37.2%) reported living in urban areas. Approximately one-third (32.7%) of respondents reported being an essential worker, and two-thirds (65.3%) of respondents indicated that they had a preexisting health condition.
presents descriptive statistics for key study variables across all three waves.
Table 2. Vaccine Confidence, Campaign Recall, and Fictional Campaign Recall Among the Study Sample
The percentage of respondents who were Vaccine Confident nearly doubled from Wave 1 (46.5%) to Wave 3 (79.5%), with concomitant reductions in the Movable Middle (from 35.8% to 10.3%) and Vaccine Refusers categories (from 17.7% to 10.2%) across the three survey waves.Footnote10 To quantify the stability of within-respondent vaccine confidence, we estimated the Spearman rank correlation of vaccine confidence between waves. The correlation was 0.62 between waves 1 and 2 and 0.81 between waves 2 and 3, indicating that within respondents, vaccine confidence was relatively stable across waves and increased over time. The magnitude of these correlations was largely driven by the fact that respondents in the Vaccine Confident category remained Vaccine Confident across waves.
In contrast with vaccine confidence, past 4-month Campaign recall peaked in Wave 2 after the introduction of the We Can Do This campaign, with over half of respondents (57.4%) reporting having seen or heard the Campaign. Compared to Wave 2, Campaign recall was slightly lower in Wave 1 (52.7%; Slow the Spread) and in Wave 3 (52.0%; We Can Do This). Past 4-month Campaign recall was less consistent across waves compared to vaccine confidence, with moderate Spearman rank correlations of 0.26 between waves 1 and 2 and 0.34 between waves 2 and 3.
Relatively few respondents reported fictional campaign recall in waves 1–3 (fictional campaign recall ranged from 10.4% to 13.6% across waves) and showed low levels of within-respondent stability similar to Campaign recall, with Spearman rank correlations of 0.26 between waves 1 and 2 and 0.32 between waves 2 and 3.
Modeling Results
presents the results of the proportional odds logistic regression model.
Table 3. Results from Ordered Logistic Regression Model Predicting Vaccine Confidence
Campaign Recall
Results showed a significant, positive linear relationship between past 4-month Campaign recall and vaccine confidence (β = 0.26, z = 2.12, p = .034). For each increase in the past 4-month Campaign recall category endorsement (e.g., from no recall to infrequent recall, from infrequent recall to frequent recall), there was a 29% increase in the oddsFootnote11 of being in a higher category of vaccine confidence, controlling for lagged reports of past 4-month Campaign recall and vaccine confidence; concurrent and lagged fictional campaign recall; survey wave; and a range of sociodemographic covariates. The quadratic effect of past 4-month Campaign recall on vaccine confidence was not statistically significant.
Campaign-Relevant and Vaccine Confidence-Relevant Covariates
Results showed that lagged vaccine confidence (linear and quadratic) was positively associated with current vaccine confidence (β = 3.42, z = 21.19, p < .001 and β = 0.57, z = 6.57, p < .001, respectively), indicating that respondents who were in a higher category of vaccine confidence in the previous wave were more likely to be in a higher category of vaccine confidence in the current wave. The effect of lagged vaccine confidence on current vaccine confidence was stronger at higher levels of vaccine confidence, suggesting that respondents who were Vaccine Confident in the previous wave were more likely to remain Vaccine Confident in the current wave, compared to the likelihood that Movable Middle respondents in the previous wave would remain in the Movable Middle in the current wave.
demonstrates a significant association between survey wave and current vaccine confidence (β = 0.29, z = 2.54, p = .011), such that there was an increase in vaccine confidence during latter historical periods of the pandemic compared to the former periods, irrespective of a respondent’s reported Campaign recall and previous vaccine confidence.
Sociodemographic Covariates
Results reported in indicate that, relative to corresponding reference groups, respondents were more likely to be in a higher category of vaccine confidence if they reported being 65 years old or older, being non-Hispanic Black or Hispanic/Latino, having a bachelor’s or a higher degree, having a household income of more than $100,000, and/or having a preexisting health condition. In comparison, respondents were more likely to be in a lower category of vaccine confidence if they indicated being politically moderate or conservative; living in the Midwestern, Southern, or Western regions of the U.S.; and/or living in a rural area.
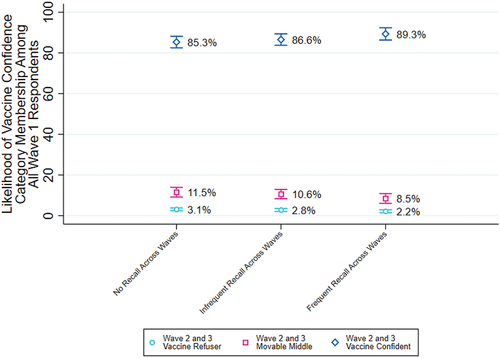
illustrates the likelihood of vaccine confidence category membership in waves 2 and 3, among all respondents, by Campaign recall category. Those who reported no Campaign recall in a given wave were estimated to have an 85% likelihood of being Vaccine Confident in that same wave, whereas those who reported frequent Campaign recall in a given wave were estimated to have an 89% likelihood of being Vaccine Confident in that same wave.
Figure 1. Likelihood of Vaccine Confidence Category Membership in Waves 2 and 3, Among All Wave 1 Respondents, by Campaign Recall Category.
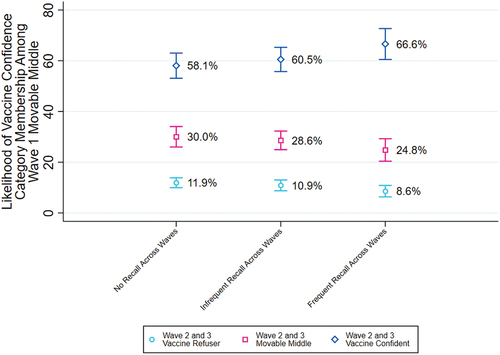
As noted above, respondents who were Vaccine Confident in the previous wave were more likely to remain Vaccine Confident in the current wave, compared to the likelihood that Movable Middle respondents in the previous wave would remain in the Movable Middle in the current wave. Since nearly half of respondents at Wave 1 were Vaccine Confident (46.5%; see ), largely reflects the many respondents that remained Vaccine Confident across waves. To show this effect more clearly for the Wave 1 Movable Middle, a target audience for the Campaign, we created , which illustrates the likelihood of vaccine confidence category membership in waves 2 and 3, among Wave 1 Movable Middle respondents, by Campaign recall category. Those who reported no Campaign recall in a given wave were estimated to have a 58% likelihood of being Vaccine Confident in that same wave, whereas those who reported frequent Campaign recall in a given wave were estimated to have a 67% likelihood of being Vaccine Confident in that same wave.
Figure 2. Likelihood of Vaccine Confidence Category Membership in Waves 2 and 3, Among Wave 1 Movable Middle Respondents, by Campaign Recall Category.
Sensitivity Analyses
We conducted sensitivity analyses to assess whether (1) the removal of respondents who reported fictional campaign recall from the data changed the observed relationship between Campaign recall and vaccine confidence, (2) model adjustments accounting for multiply imputed data produced substantially different results, and (3) relaxing the proportional odds assumption in the regression model changed the conclusions inferred from the original model (see supplemental materials for detailed description and model results). Results from these analyses did not differ substantively from those produced by the original regression model; accordingly, we did not alter the original model.
Discussion
Results demonstrate a positive, significant relationship between past 4-month Campaign recall and vaccine confidence, such that greater Campaign recall predicted greater vaccine confidence. This association remained significant when controlling for lagged versions of Campaign recall and vaccine confidence variables, concurrent and lagged fictional campaign recall, survey wave, and a range of sociodemographic covariates. These results include a key Campaign audience—adults in the Movable Middle in Wave 1. For this group, frequent Campaign recall was associated with a change in the likelihood of being Vaccine Confident, despite the fact that Vaccine Confidence in waves 2 and 3 was relatively high for Wave 1 Movable Middle respondents across all recall categories (ranging from 58% in the no recall group to 67% in the frequent recall group).Footnote12 Together, these findings suggest that exposure to the Campaign positively influenced vaccine confidence across audiences, including among the Movable Middle. In light of the evidence that lower levels of COVID-19 vaccine hesitancy and greater intention to vaccinate against COVID-19 predict greater likelihood of subsequent COVID-19 vaccination (Latkin et al., Citation2022), findings suggest that increased vaccine confidence resulting from Campaign exposure led to increased COVID-19 vaccination.
Study findings do not reflect the influence of the Campaign on two other Campaign goals/target audiences: parent confidence in getting their children vaccinated against COVID-19, and COVID-19 booster confidence among fully vaccinated adults. These represent promising avenues for future evaluation research. Whereas this study did not examine the relationship between Campaign recall and vaccine confidence by sociodemographic subgroups, future research could examine these relationships (see supplemental materials for a discussion of reported differences in vaccine confidence by sociodemographic subgroups). Future research could also assess the impact of audience-tailored messaging on vaccine confidence and uptake among key audiences (e.g., non-Hispanic Black, Hispanic/Latino adults).
Limitations
Although research indicates that recalled campaign exposure correlates with exposure opportunities (Kranzler, Gibson, & Hornik, Citation2017; Southwell, Barmada, Hornik, & Maklan, Citation2002), self-reported Campaign recall is subject to recall bias and may not accurately reflect actual exposure to the ads assessed and, more broadly, to the Campaign. Accordingly, results may not fully capture Campaign impact on vaccine confidence. To complement this research, we examined the relationship between exogenous, or external, measures of probable Campaign exposure (e.g., digital impressions) and vaccine uptake (Williams et al., Citationaccepted). Future research could assess whether opportunities for exposure combined with self-reported recall improve the prediction of vaccine confidence over time. Although analyses controlled for several potentially confounding variables, the relationship between Campaign recall and vaccine confidence may be subject to the influence of unmeasured confounders not included in our analyses. This relationship may also be subject to response bias due to differences in materials used to assess Campaign and fictional campaign recall. Nonresponse bias may limit inferences made about the general population; we attempted to address this bias with survey weights. As Campaign recall and vaccine confidence were assessed concurrently, they may share error variance associated with a given wave due to wave-specific factors. The use of predictor and outcome variables assessed simultaneously may pose a threat to the internal validity of findings and causal ordering. See supplemental materials for a discussion of the limitations listed above.
Conclusion
COVID-19 vaccines are safe and effective, and widespread vaccination protects against infection, hospitalization, and death. The We Can Do This campaign was implemented to increase COVID-19 vaccine confidence among American adults. This study shows that more Campaign recall led to more vaccine confidence, with individuals who reported frequent recall at any point in time having statistically higher odds of becoming Vaccine Confident than individuals who reported infrequent recall; the same positive and statistically significant relationship applied to individuals reporting infrequent recall as compared to no recall. Further, study results show the Campaign positively influenced vaccine confidence among the Movable Middle – the Campaign’s target audience. Findings indicate that, similar to their influence on other health behaviors (Anker, Feeley, McCracken, & Lagoe, Citation2016; Wakefield, Loken, & Hornik, Citation2010), public education campaigns play a key role in influencing COVID-19 vaccine confidence in the U.S. Additionally, findings offer the first evidence of COVID-19 campaign impact on vaccine confidence, using longitudinal data from a nationally representative sample of U.S. adults. Applied to the population at large, these results suggest exposure to the Campaign is associated with large-scale change in COVID-19 vaccine confidence. Although results suggest that the Campaign has attenuated the burden of COVID-19 in the U.S. by increasing vaccine confidence, which is predictive of vaccine uptake, additional research may be warranted to establish evidence that the Campaign has increased COVID-19 vaccination, thereby reducing COVID-19–attributed morbidity and mortality.
Acknowledgements
The authors gratefully acknowledge our colleagues at the HHS Office of the Assistant Secretary for Public Affairs, the HHS Office of the Assistant Secretary for Planning and Evaluation, especially Trinidad Beleche, Nicholas Holtkamp, and Lok Wong Samson, the Centers for Disease Control and Prevention, especially Lynn Sokler, and the Fors Marsh-led team of agencies contributing to the implementation and evaluation of this campaign. We thank the thousands of research participants who made this study possible.
Disclosure Statement
This publication represents the views of the authors and does not represent the U.S. Department of Health and Human Services position or policy. No potential conflicts of interest were reported by the authors.
Additional information
Funding
Notes
1 Vaccine confidence is the likelihood of getting a COVID-19 vaccine (among unvaccinated individuals) or whether an individual has received at least one dose of a COVID-19 vaccine. We use vaccine confidence as the outcome of interest in this study as the We Can Do This campaign explicitly aimed to increase vaccine confidence.
2 Between December 2020–March 2021, as COVID-19 vaccination authorization advanced, vaccination availability grew. During this period and before Campaign implementation, HHS administered advertising to promote other COVID-19 preventive measures such as face mask use and social distancing.
3 CDC guidelines were informed by tobacco control and prevention campaigns.
4 Please see the supplemental materials for a description of the survey methodology.
5 We used vaccine confidence as the dependent variable in lieu of vaccine uptake given the timing of the Wave 1 survey fielding (January–February 2021), which occurred before April 19, 2021, when all American adults were eligible to receive a COVID-19 vaccine. It is feasible that some respondents would have received a vaccine before taking the Wave 1 survey but were unable to do so given limited vaccine availability. By combining vaccine uptake and likelihood of vaccination, the vaccine confidence variable more accurately captured intent to vaccinate among respondents who were Vaccine Confident in Wave 1 but unable to get vaccinated before the Wave 1 survey fielding.
6 We defined the Movable Middle by collapsing the middle three categories representing likelihood of vaccination, as these categories tended to change in similar ways across waves. Respondents who reported that they are very unlikely to get vaccinated tended to show more between-wave stability compared to the three middle vaccine likelihood categories; for this reason, we separated them into a Vaccine Refuser category.
7 Aided recall has also been referred to as recognition, or the ability to “respond to a closed-ended question about past engagement with specific content when presented that content once again” (Southwell, Citation2005, p. 114).
8 Due to small sample sizes, respondents who reported their race/ethnicity as American Indian or Alaska Native, non-Hispanic Asian American or Pacific Islander, and non-Hispanic Multiple Races or Other Identity were omitted from analyses.
9 A list of states within each of the four U.S. Census Regions is provided here: https://www2.census.gov/geo/pdfs/maps-data/maps/reference/us_regdiv.pdf.
10 The Wave 1 survey was fielded from January–February 2021, and the Wave 3 survey was fielded from September–November 2021.
11 This value was computed using the values reported in , exponentiating the log odds of the Campaign recall coefficient (linear).
12 It is worth noting that there are many factors outside the Campaign that may have increased respondent Vaccine Confidence across waves (e.g., increases in pro-vaccine beliefs, increased access to COVID-19 vaccines over time, normative influence from friends and family members who were vaccinated). These factors and others may partially explain respondents’ greater likelihood of become Vaccine Confident in subsequent waves.
References
- Agley, J., & Xiao, Y. (2021). Misinformation about COVID-19: Evidence for differential latent profiles and a strong association with trust in science. BMC Public Health, 21(1), 89. doi:10.1186/s12889-020-10103-x
- Anker, A. E., Feeley, T. H., McCracken, B., & Lagoe, C. A. (2016). Measuring the effectiveness of mass-mediated health campaigns through meta-analysis. Journal of Health Communication, 21(4), 439–456. doi:10.1080/10810730.2015.1095820
- Austin, P. C., White, I. R., Lee, D. S., & van Buuren, S. (2021). Missing data in clinical research: A tutorial on multiple imputation. The Canadian Journal of Cardiology, 37(9), 1322–1331. doi:10.1016/j.cjca.2020.11.010
- Bagozzi, R. P., & Yi, Y. (1990). Assessing method variance in multitrait-multimethod matrices: The case of self-reported affect and perceptions at work. The Journal of Applied Psychology, 75(5), 547. doi:10.1037/0021-9010.75.5.547
- Bentler, P. M., Jackson, D. N., & Messick, S. (1971). Identification of content and style: A two-dimensional interpretation of acquiescence. Psychological Bulletin, 76(3), 186–204. doi:10.1037/h0031474
- Berg, M. B., & Lin, L. (2021). Predictors of COVID-19 vaccine intentions in the United States: The role of psychosocial health constructs and demographic factors. Translational Behavioral Medicine, 11(9), 1782–1788. doi:10.1093/tbm/ibab102
- Cassata, C. (2021). Here’s How It Was Possible to Develop COVID-19 Vaccines So Quickly. Healthline. https://www.healthline.com/health-news/heres-how-it-was-possible-to-develop-covid-19-vaccines-so-quickly
- CBPP. (2022). The COVID-19 Economy’s Effects on Food, Housing, and Employment Hardships. https://www.cbpp.org/sites/default/files/8-13-20pov.pdf
- CDC. (2014). Best practices user guides: Health communications in tobacco prevention and control. https://www.cdc.gov/tobacco/stateandcommunity/guides/pdfs/health-communications-508.pdf
- CDC. (2022a). COVID data tracker: Rates of laboratory-confirmed COVID-19 hospitalizations by vaccination status. Centers for Disease Control and Prevention.
- CDC. (2022b). COVID-19 Vaccine Effectiveness Research. https://www.cdc.gov/vaccines/covid-19/effectiveness-research/protocols.html
- CDC. (2023). COVID Data Tracker. Centers for Disease Control and Prevention. https://covid.cdc.gov/covid-data-tracker
- Davis, M. J. (2010). Contrast coding in multiple regression analysis: Strengths, weaknesses, and utility of popular coding structures. Journal of Data Science, 8(1), 61–73. doi:10.6339/JDS.2010.08(1).563
- Edwards, B., Biddle, N., Gray, M., & Sollis, K. (2021). COVID-19 vaccine hesitancy and resistance: Correlates in a nationally representative longitudinal survey of the Australian population. PLoS One, 16(3), e0248892. doi:10.1371/journal.pone.0248892
- El-Mohandes, A., White, T. M., Wyka, K., Rauh, L., Rabin, K., Kimball, S. H. … Lazarus, J. V. (2021). COVID-19 vaccine acceptance among adults in four major US metropolitan areas and nationwide. Scientific Reports, 11(1), 21844. doi:10.1038/s41598-021-00794-6
- Fishbein, M., & Ajzen, I. (2011). Predicting and changing behavior: The reasoned action approach. New York: Psychology Press.
- GAO. (2022). Science & Tech Spotlight: Long COVID. https://www.gao.gov/products/gao-22-105666
- Giuntella, O., Hyde, K., Saccardo, S., & Sadoff, S. (2021). Lifestyle and mental health disruptions during COVID-19. Proceedings of the National Academy of Sciences, 118(9), e2016632118. doi:10.1073/pnas.2016632118
- HHS. (2021a). Monthly Outcome Survey (Wave 1) [Unpublished data set.].
- HHS. (2021b). Monthly Outcome Survey (Wave 4) [Unpublished data set.].
- HHS. (2022). COVID-19 Vaccines. HHS.Gov. Texthttps://www.hhs.gov/coronavirus/covid-19-vaccines/index.html
- Hornik, R. C. (Ed.). (2002a). Public health communication: Evidence for behavior change. New York: Routledge.
- Hornik, R. C. (2002b). Exposure: Theory and evidence about all the ways it matters. Social Marketing Quarterly, 8(3), 31–37. doi:10.1080/15245000214135
- Hornik, R., & Yanovitzky, I. (2003). Using theory to design evaluations of communication campaigns: The case of the national youth anti-drug media campaign. Communication Theory, 13(2), 204–224. doi:10.1111/j.1468-2885.2003.tb00289.x
- Jacobs, L. G., Paleoudis, E. G., Bari, D.L. -D., Nyirenda, T., Friedman, T., Gupta, A. … Aschner, J. L. (2020). Persistence of symptoms and quality of life at 35 days after hospitalization for COVID-19 infection. PLoS One, 15(12), e0243882. doi:10.1371/journal.pone.0243882
- Kelly, B. J., Southwell, B. G., McCormack, L. A., Bann, C. M., MacDonald, P. D. M., Frasier, A. M. … Squiers, L. B. (2021). Predictors of willingness to get a COVID-19 vaccine in the U.S. BMC Infectious Diseases, 21(1), 338. doi:10.1186/s12879-021-06023-9
- Kennedy, B., Tyson, A., & Funk, C. (2022). Americans’ trust in scientists, other groups declines. Pew Research Center Science & Society. https://www.pewresearch.org/science/2022/02/15/americans-trust-in-scientists-other-groups-declines/
- Khan, M. M. A., Khan, M. N., Mustagir, M. G., Rana, J., Islam, M. S., & Kabir, M. I. (2020). Effects of underlying morbidities on the occurrence of deaths in COVID-19 patients: A systematic review and meta-analysis. Journal of Global Health, 10(2). doi:10.7189/jogh.10.020503
- Kranzler, E. C., Gibson, L. A., & Hornik, R. C. (2017). Recall of “the real cost” anti-smoking campaign is specifically associated with endorsement of campaign-targeted beliefs. Journal of Health Communication, 22(10), 818–828. doi:10.1080/10810730.2017.1364311
- Lalot, F., Heering, M. S., Rullo, M., Travaglino, G. A., & Abrams, D. (2020). The dangers of distrustful complacency: Low concern and low political trust combine to undermine compliance with governmental restrictions in the emerging Covid-19 pandemic. Group Processes & Intergroup Relations, 25(1), 106–121. doi:10.1177/1368430220967986
- Lang, A. (2000). The limited capacity model of mediated message processing. The Journal of Communication, 50(1), 46–70. doi:10.1111/j.1460-2466.2000.tb02833.x
- Lang, K. M., & Little, T. D. 2018. Principled missing data treatments. Prevention Science:, 19(3), 284–294. 10.1007/s11121-016-0644-5
- Latkin, C., Dayton, L., Miller, J., Yi, G., Balaban, A., Boodram, B. … Falade-Nwulia, O. (2022). A longitudinal study of vaccine hesitancy attitudes and social influence as predictors of COVID-19 vaccine uptake in the US. Human Vaccines & Immunotherapeutics, 18(5), 1–9. doi:10.1080/21645515.2022.2043102
- Latkin, C. A., Dayton, L., Yi, G., Konstantopoulos, A., & Boodram, B. (2021). Trust in a COVID-19 vaccine in the U.S.: A social-ecological perspective. Social Science & Medicine, 270, 113684. 1982. doi:10.1016/j.socscimed.2021.113684
- Lithwick, D. (2020). Refusing to Wear a Mask Is a Uniquely American Pathology. Slate. https://slate.com/news-and-politics/2020/05/masks-coronavirus-america.html
- Lüdecke, D., Ben-Shachar, M. S., Patil, I., & Makowski, D. (2020). Extracting, computing and exploring the parameters of statistical models using R. Journal of Open Source Software, 5(53), 2445. doi:10.21105/joss.02445
- Murphy, J., Vallières, F., Bentall, R. P., Shevlin, M., McBride, O., Hartman, T. K. … Hyland, P. (2021). Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nature Communications, 12(1), 29. doi:10.1038/s41467-020-20226-9
- Nguyen, L. H., Joshi, A. D., Drew, D. A., Merino, J., Ma, W., Lo, C. -H. … Chan, A. T. (2022). Self-reported COVID-19 vaccine hesitancy and uptake among participants from different racial and ethnic groups in the United States and United Kingdom. Nature Communications, 13(1), 636. doi:10.1038/s41467-022-28200-3
- Nielsen (2021). Digital ad ratings and total ad ratings. We Can Do This campaign, P18+ reach for campaign running April 5, 2021-September 26, 2021.
- Noar, S. M. (2006). A 10-year retrospective of research in health mass media campaigns: Where do we go from here? Journal of Health Communication, 11(1), 21–42. doi:10.1080/10810730500461059
- Noar, S. M., Palmgreen, P., Chabot, M., Dobransky, N., & Zimmerman, R. S. (2009). A 10-year systematic review of HIV/AIDS mass communication campaigns: Have we made progress? Journal of Health Communication, 14(1), 15–42. doi:10.1080/10810730802592239
- NORC. (2019). Technical Overview of the AmeriSpeak Panel NORC’s Probability-Based Household Panel. https://amerispeak.norc.org/content/dam/amerispeak/research/pdf/AmeriSpeak%20Technical%20Overview%202019%2002%2018.pdf
- Petty, R. E., & Cacioppo, J. T. (1986). The elaboration likelihood model of persuasion. Advances in Experimental Social Psychology, 19, 123–205.
- Petty, R. E., & Wegener, D. T. (1999). The elaboration likelihood model: Current status and controversies. In Chaiken, S., & Trope, Y. (Eds.), Dual-process theories in social psychology (pp. 37–72). New York: The Guilford Press.
- Prochaska, J. O., & DiClemente, C. C. (1983). Stages and processes of self-change of smoking: Toward an integrative model of change. Journal of Consulting and Clinical Psychology, 51(3), 390–395. doi:10.1037/0022-006X.51.3.390
- Rane, M. S., Kochhar, S., Poehlein, E., You, W., Robertson, M. M., Zimba, R. … for the CHASING COVID Cohort Study Team. (2022). Determinants and trends of COVID-19 vaccine hesitancy and vaccine uptake in a national cohort of US adults: A longitudinal study. American Journal of Epidemiology, 191(4), 570–583. doi:10.1093/aje/kwab293
- R Core Team. (2022). R: A language and environment for statistical computing. R Foundation for Statistical Computing. https://www.R-project.org/
- Rosenstock, I. M., Strecher, V. J., & Becker, M. H. (1988). Social learning theory and the health belief model. Health Education Quarterly, 15(2), 175–183. doi:10.1177/109019818801500203
- Ruiz, J. B., & Bell, R. A. (2021). Predictors of intention to vaccinate against COVID-19: Results of a nationwide survey. Vaccine, 39(7), 1080–1086. doi:10.1016/j.vaccine.2021.01.010
- Scharff, D. P., Mathews, K. J., Jackson, P., Hoffsuemmer, J., Martin, E., & Edwards, D. (2010). More than Tuskegee: Understanding mistrust about research participation. Journal of Health Care for the Poor and Underserved, 21(3), 879–897. doi:10.1353/hpu.0.0323
- Schneider, E. C., Shah, A., Sah, P., Vilches, T., Pandey, A., Moghadas, S. M., & Galvani, A. (2022). Impact of U.S. COVID-19 vaccination efforts: An update on averted deaths. Hospitalizations, and Health Care Costs Through. March 2022. doi: 10.26099/d3dm-fa91
- Siemsen, E., Roth, A., & Oliveira, P. (2010). Common method bias in regression models with linear, quadratic, and interaction effects. Organizational Research Methods, 13(3), 456–476. doi:10.1177/1094428109351241
- Southwell, B. G. (2005). Between messages and people: A multilevel model of memory for television content. Communication Research, 32(1), 112–140. doi:10.1177/0093650204271401
- Southwell, B. G., Barmada, C. H., Hornik, R. C., & Maklan, D. M. (2002). Can we measure encoded exposure? validation evidence from a national campaign. Journal of Health Communication, 7(5), 445–453. doi:10.1080/10810730290001800
- Swanton, R., Allom, V., & Mullan, B. (2015). A meta-analysis of the effect of new-media interventions on sexual-health behaviours. Sexually Transmitted Infections, 91(1), 14–20. doi:10.1136/sextrans-2014-051743
- Venables, W. N., & Ripley, B. D. (2002). Modern applied statistics with S. Fourth Springer. New York. ISBN. https://www.stats.ox.ac.uk/pub/MASS4/.
- Venkatakrishnan, A. J., Pawlowski, C., Zemmour, D., Hughes, T., Anand, A., Berner, G. … Soundararajan, V. (2021). Mapping each pre-existing condition’s association to short-term and long-term COVID-19 complications. NPJ Digital Medicine, 4(1), 1–11. doi:10.1038/s41746-021-00484-7
- Wakefield, M. A., Loken, B., & Hornik, R. C. (2010). Use of mass media campaigns to change health behaviour. The Lancet, 376(9748), 1261–1271. doi:https://doi.org/10.1016/S0140-6736(10)60809-4
- The White House. (2022). Press Briefing by White House COVID-19 Response Team and Public Health Officials. The White House. https://www.whitehouse.gov/briefing-room/press-briefings/2022/02/02/press-briefing-by-white-house-covid-19-response-team-and-public-health-officials-81/
- White, I. R., Royston, P., & Wood, A. M. (2011). Multiple imputation using chained equations: Issues and guidance for practice. Statistics in Medicine, 30(4), 377–399. doi:10.1002/sim.4067
- Williams, C. J., Kranzler, E. C., Luchman, J. N., Denison, B., Fischer, S., Wonder, T., Ostby, R., Vines, M., Weinberg, J., Petrun Sayers, E. L., Kurti, A. N., Trigger, S., Hoffman, L., & Peck, J. F. A. (accepted). The initial relationship between the United States Department of Health and Human Services‘ digital COVID-19 public education campaign and vaccine uptake: An evaluation of campaign effectiveness.
- Williams, D. R., & Rucker, T. D. (2000). Understanding and addressing racial disparities in health care. Health Care Financing Review, 21(4), 75–90.
- Yadav, R. -P., & Kobayashi, M. (2015). A systematic review: Effectiveness of mass media campaigns for reducing alcohol-impaired driving and alcohol-related crashes. BMC Public Health, 15(1), 857. doi:10.1186/s12889-015-2088-4
- Yasmin, F., Najeeb, H., Moeed, A., Naeem, U., Asghar, M. S., Chughtai, N. U. , and Pakpour, A. H. (2021). COVID-19 vaccine hesitancy in the United States: A systematic review. Frontiers in Public Health, 9, 9.https://www.frontiersin.org/article/10.3389/fpubh.2021.770985
- Zeileis, A. (2006). Object-oriented computation of sandwich estimators. Journal of Statistical Software, 16(9), 1–16. doi:https://doi.org/10.18637/jss.v016.i09
- Zeileis, A., Köll, S., & Graham, N. (2020). Various versatile variances: An object-oriented implementation of clustered covariances in R. Journal of Statistical Software, 95(1), 1–36. doi:https://doi.org/10.18637/jss.v095.i01