
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Background: Cross education is the contralateral strength gain following unilateral training of the ipsilateral limb. This phenomenon provides an ideal rehabilitation model for acute or chronic rehabilitation; however, previous cross education meta-analyses have been limited to a handful of studies.
Objectives: The present meta-analysis aimed to (1) be as inclusive as possible, (2) compare cross education in young able-bodied, older able-bodied, and patient populations, (3) compare cross education between training modalities, and (4) detail the impact of methodological controls on the quantification of cross education.
Methodology: A review of English literature identified studies that employed unilateral resistance training and reported contralateral strength results. Studies were separated to examine the effect of population, training modality, limb, sex, and familiarization on the magnitude of cross education. The percent strength gain and effect size were calculated for ipsilateral and contralateral limbs.
Results: A total of 96 studies fit the predetermined inclusion criteria and were included in the analysis. The included studies were further divided into 141 units employing separate unilateral training paradigms. These were separated into young, able-bodied (n = 126), older, able-bodied (n = 9), and neuromuscular patients (n = 6). Cross education was an average of 18% (standardized mean difference (SMD) = 0.71) in young, able-bodied participants, 17% (SMD = 0.58) in healthy able-bodied participants, and 29% (SMD = 0.76) in neuromuscular patients.
Conclusion: Cross education was present in young, older, and patient populations and similar between upper and lower limbs and between males and females. Electromyostimulation training was superior to voluntary training paradigms.
Background
Cross education is the strength gain that is found in the contralateral limb following a unilateral training program on the homologous limb. Cross education was first reported in 1894 by Scripture et al. [Citation1] who determined that task steadiness and muscular strength could be improved in the contralateral limb following unilateral training. This phenomenon is of great importance for clinical applications and rehabilitation, and requires further mechanistic investigation. Cross education provides a beneficial rehabilitation model for unilateral injuries or disorders; including, acute injuries or immobilization (casting) of a single limb, and neurologic disorders, such as stroke, affecting the body unilaterally.
Previous research has proposed that cross education can be explained by two distinct, but not necessarily mutually exclusive, hypotheses: ‘cross-activation’ and ‘bilateral access’ [Citation2, Citation3]. The ‘cross-activation’ hypothesis proposes that unilateral activity excites both ipsilateral and contralateral cortical motor areas. With this hypothesis, the unilateral training causes adaptations in both hemispheres, though to a lesser extent in the untrained hemisphere. Alternatively, the ‘bilateral access’ hypothesis suggests that the homologous untrained muscle can access the unilateral adaptations of training through interhemispheric communication from the associated motor areas [Citation2, Citation3].
Previous meta-analyses and systematic reviews have determined that the average contralateral strength gain from cross education is approximately 8–12% [Citation4–7]. This amount corresponds to approximately 35–60% of the strength increase that is found in the ipsilateral (trained) limb [Citation4, Citation6, Citation8]. Manca et al. [Citation7] further separated their estimate of cross education into lower limb (16.4%) and upper limb (9.4%). However, these previous reviews of cross education were limited to 2 [Citation9], 8 [Citation8], 10 [Citation10], 13 [Citation6], 16 [Citation4], and 31 [Citation7] articles. There are several factors that make the review of cross education complicated and limited, including the name discrepancies confounding the search for studies, and the variety of training paradigms. However, the primary reason for the small ‘sample sizes’ of cross education reviews is the stringency of inclusion criteria. The reviews by Munn et al. [Citation6], Carroll et al. [Citation4], Cirer-Sastre et al. [Citation10], and Manca et al. [Citation7], were limited to the analysis of randomized controlled studies. In addition, only studies with full data (means and standard deviations) for each of the ipsilateral experimental, contralateral experimental, and control limbs were included.
The inconsistent terminology and the unintentional examination of cross education using the contralateral limb as a ‘control limb’ for unilateral training has confounded the analysis of the field. Cross education of strength has been referred to by many names including cross-transfer, cross-over, or contralateral training. Similarly, the cross education of skill following unilateral practice is typically referred to as interlateral transfer of learning, bilateral transfer, or intermanual transfer. These studies generally focus on single session practice, rather than training, and the transfer of a skill, rather than strength. Although widely studied, the practice paradigms and the outcome measurements of the cross education of skill vary drastically across studies making them extremely difficult to quantitatively compare. Therefore, this meta-analysis focuses solely on the cross education of strength.
Lastly, variability in training paradigms makes it difficult to compare cross education between studies. There is a considerable variation in the duration (number of sessions), volume (contractions per session), intensity (load), and modality (type of contraction or stimuli) of unilateral training. The reviews by Carroll et al. [Citation4], Munn et al. [Citation6], and Manca et al. [Citation7] limited their analyses to studies employing training intensities greater than 50% maximal strength for a minimum of 2 weeks. Most notably, the previous meta-analyses included only isometric, isokinetic, and dynamic training [Citation4, Citation6, Citation7, Citation10], specifically excluding ‘alternative’ training via electromyostimulation (EMS), transcranial magnetic stimulation, vibration, or acupuncture.
The present analysis prioritized inclusivity over selectivity to capture the greatest overview of the field. A review of literature was undertaken to include as many ‘contralateral strength transfer’ studies as possible, including studies that unintentionally examined cross education by using an untrained contralateral limb as a control for unilateral training. The present analysis included studies using ‘alternative’ training, specifically EMS training (or neuromuscular electrical stimulation (NMES)), since previous meta-analysis have not previously included ‘non-traditional’ forms of strength training. In order to advance the use of cross education for rehabilitation purposes, the analysis was not limited to healthy populations as long as strength was assessed pre and post intervention.
Methods
Definitions
For the purpose of this analysis the term study will refer to an article as referenced. The term unit will refer to a training paradigm within a study, while the term limb will be the designated trained, untrained, or control limb of a participant. For example, one study may have two units within it where one unit was assigned to one type of training (e.g. eccentric training, elbow flexion training, low frequency training, etc.) and another unit was assigned to a separate training paradigm (e.g. concentric training, knee flexion training, high frequency training, etc.).
Literature search
The included studies were collected from an ongoing review of cross education and unilateral training literature. Studies were identified using Google Scholar, PubMed, and Research Gate using the search terms: cross education, cross-transfer, interlimb transfer, and contralateral strength gain. The reference list of each identified study was examined to include previously noted cross education studies not identified in the database search. In addition, studies using unilateral training were identified using search terms including: unilateral strength training, dominant AND non-dominant control limb and were examined for the unintentional observation of cross education where the contralateral limb was designated as a control limb.
Inclusion criteria
The selection of inclusion criteria was designed to be as inclusive as possible for the broadest review possible.
Population. All ages, sexes, and abilities were included in the present review. Units were separated into three groups: (1) young able-bodied (young) participants (< 50 years of age), (2) older able-bodied (older) participants (>50 years of age), and (3) neuromuscular disorder (patient) populations.
Training paradigm. All training types aimed at improving strength were included in the present study, including EMS training which has been previously excluded from cross education meta-analyses. Training modalities (contraction types) were separated into the following categories: isometric, isokinetic, dynamic (including isotonic), EMS, or ‘other’. If two types of voluntary contractions were performed for training, then the unit was placed in the ‘other’ category. The EMS category consists of stimulation alone or superimposed on a voluntary contraction. Any training intensity (load) was included as long as it was greater than 0% maximal strength (i.e. the intention was strength gain, rather than endurance gain). The criteria for number of sessions was >5 sessions to include training stimuli rather than mechanistic examinations.
Outcomes. Studies were included if strength was measured and reported in any manner including: pretraining and posttraining means, mean gain, or percent gain. Studies were further separated into units only where separate training paradigms were employed, rather than separate outcomes. Where one training unit had multiple outcomes, the single outcome that was homologous to the training modality (i.e. closest in contraction type, joint angle, speed of contraction, etc.) was selected, with the exception of EMS, vibration, or electroacupuncture training, where a voluntary contraction was selected. When multiple contraction types were used for training, as well as testing, the contraction type used most in training was selected as the outcome measure.
Sample size. The inclusion criterion for unit sample size was ≥3 to get an appropriate mean and standard deviation for effect size calculation. No control group was required for inclusion in the analysis.
Analysis
Effect size. Where means and standard deviations were reported effect size was calculated for each limb within a unit using The Cochrane Collaboration Review Manager (RevMan V.5.3) [Citation11]. The standardized mean difference (SMD) and 95% confidence intervals were calculated using inverse variance as the statistical method, and random effects as the analysis model. Statistical significance (Z-score) was calculated in RevMan to determine if the effect size is greater than null. Where standard error (SE) was reported it was converted to standard deviation (SD) using the following formula including group sample size (n):
The effect size was calculated where possible for the experimental limbs (trained and untrained) and the control limb(s). If both limbs of the control group were measured (dominant and non-dominant) then each limb was separately used as a control for the experimental limb. If only one control limb was tested then it was included as the control for both the trained and untrained experimental limbs.
Percent gain. Where means were reported the percent gain of the trained and/or untrained limb was calculated according to the following formula:
If only percent gain was reported but not pretraining or posttraining mean values then the percent gain was included as reported.
Cross-body transfer. The magnitude of cross-body transfer was calculated to determine how much of the training effect was transferred to the untrained limb. The calculation was conducted for each unit as follows:
Comparisons. Independent sample t-tests were performed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA) with a 0.05 significance level. The magnitude of percent gain in the untrained (cross education) limb and the trained limb was examined between (1) upper versus lower limb, (2) males versus females, and (3) familiarized versus non-familiarized units. The upper limb training consisted of elbow flexion, wrist flexion and extension, and handgrip exercises amongst others. The lower limb training consisted primarily of knee extension and flexion, and secondarily plantar flexion and dorsiflexion exercises. The effect of sex was examined from units that were composed of only males or only females. Finally, familiarization was taken as reported and included anything from a familiarization contraction or testing procedures familiarization to an entire familiarization session.
Results
Study and unit characteristics
A total of 113 studies were identified and 96 studies were included in the analysis (). The 17 excluded studies did not fit the following criteria: no strength measure (4 studies), no strength data reported for untrained limb (4 studies), no pretest data (4 studies), less than 5 training sessions (2 studies), and less than 3 participants (3 studies). The remaining 96 studies included a total of 141 units. Of those, 126 units (from 87 studies [Citation12–97]) included young, able-bodied participants with a median age of 23 years and a median sample size of 11 (range 3–342) participants. Nine units (from 8 studies [Citation13, Citation27, Citation72, Citation92, Citation93, Citation98–100]) included older, able-bodied participants with a median age of 69 years and a median sample size of 11 (range 6–14).
Figure 1. Flow diagram of the identification and review process.
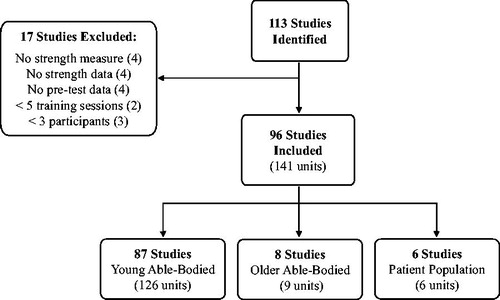
The remaining 6 units (from 6 studies [Citation101–106]) were conducted using neuromuscular patient populations with a median sample size of 10 (range 5–21) participants. The neuromuscular disorder breakdown is as follows: stroke patients (three studies), patients with various neuromuscular disorders (one study), multiple sclerosis (one study), and osteoarthritis patients (one study).
Outcome measures
The training characteristics are presented in for each of the groups. The results of effect size and percent gain for the number of units that fit each criterion are reported for the untrained (cross education) limb in and for the trained limb in . Forest plots are presented for the untrained limb in for the young group and for the older (A) and patient (B) groups.
Figure 2. Forest plot of standardized mean difference (SMD) for each young unit included in the analysis for the untrained (cross education) limb. Light grey lines indicate cutoff values for small (0.2), moderate (0.5), and large (0.8) effect sizes.
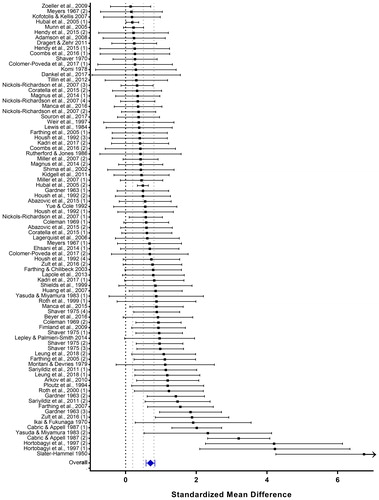
Figure 3. Forest plot of standardized mean difference (SMD) for each older (A) and patient (B) unit included in the analysis for the untrained (cross education) limb. Light grey lines indicate cutoff values for small (0.2), moderate (0.5), and large (0.8) effect sizes. DF: dorsiflexion; KE: knee extension; MS: multiple sclerosis; OA: osteoarthritis.
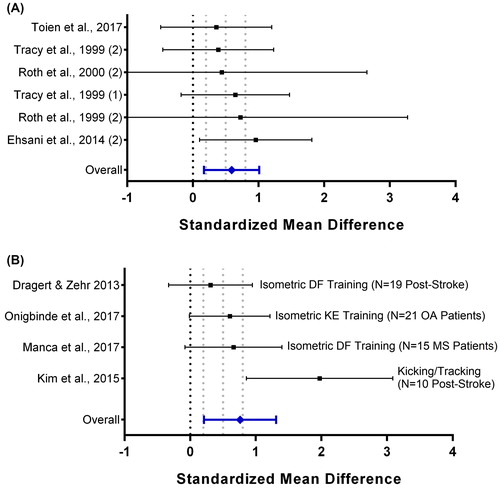
Table 1. Median and range of training characteristics.
Table 2. Effect size (standardized mean difference), percent gain, and controlled percent gain for the untrained (contralateral) limb.
Table 3. Effect size (standardized mean difference), percent gain, and controlled percent gain for the trained (ipsilateral) limb.
The average percent gain (above baseline strength) in the untrained contralateral limb of young participants following unilateral training in the ipsilateral limb was 18%, as calculated from 126 units. A review of 86 units with adequate cross education data (means and standard deviations of the untrained limb) resulted in an effect size of 0.71 (95% CI: 0.60–0.83, p < 0.001). The amount of cross education was similar amongst different training modalities with the exception of EMS training. EMS training was employed in 10 units, which demonstrated an average strength gain of 27%. Six units reported enough data to calculate effect size which was large [Citation107] at 1.57 (95% CI: 0.81–2.33, p < 0.001). This is greater than the small effect size of 0.10 (95% CI: –0.04–0.23, p = 0.16) in the control limb, which corresponded to a mean 2.2% gain.
The average percent gain in the untrained limb of older participants following unilateral training was 15%, as calculated from 9 units. A review of 6 units with adequate cross education data resulted in an effect size of 0.58 (95% CI: 0.22–0.94, p < 0.01). The modes of training included: dynamic (5), isokinetic (2), isometric (1), and resistance tubing (1). The amount of cross education in the Patients subgroup was a 29% strength gain (calculated from 6 units), which corresponded to a large effect size of 0.76 (95% CI: 0.21–1.31, p < 0.01, calculated from 4 units). Five of the studies employed strength training (resistive exercises) of the less-affected limb, one study [Citation102] employed kicking and tracking movements of the less-affected limb while secured to a tilt-table.
The influence of limb, sex, and task familiarization had no influence on the percent gain of the untrained or trained limb, or the cross-body transfer, as presented in .
Table 4. The number of units that fall within each category: sex of the unit, the usage of familiarization, the limb involved, and the presence of a control group from the able-bodied participants.
Discussion
The primary aim of the current meta-analysis was to prioritize inclusivity for the largest systematic analysis of cross education. Secondarily, this meta-analysis aimed to further cross education within the rehabilitation field by quantifying the presence of cross education in young and older able-bodied participants, as well as in patient populations. By carefully identifying the crucial inclusion criteria and reducing inclusion selectivity this meta-analysis was able to include data from 96 studies with 141 units of training groups.
The cross education gain was an 18% increase from baseline strength in young, able-bodied adults; a 15% increase in older, able-bodied participants, and a 29% increase in a patient population consisting of poststroke, neuromuscular disorders, and osteoarthritis patients. The values of cross education are higher than the previous and most widely cited estimates of 8% by Carroll et al. [Citation4], and Munn et al. [Citation6], and higher than the recent estimate of 12% reported by Manca et al. [Citation7] The cross-body transfer to the untrained limb ranged from 52% to 80% of the ipsilateral training effect.
The separation of training modalities allowed for the analysis of cross education and training adaptation from different contraction types with sufficient sample sizes and statistical power. This identified the advanced capabilities of EMS training producing a cross education effect of 27%, of which previous meta-analyses excluded [Citation4, Citation6, Citation7, Citation10]. Compared to cross education produced by isokinetic (20%), dynamic (18%), and isometric (15%) voluntary contractions, it is evident that EMS training produces a superior transfer of strength. The logistical ease of EMS training for varying populations and the associated voluntary strength gains, make it an ideal modality for cross education in rehabilitation settings. Additionally, EMS training provides a viable alternative for patients (e.g. osteoarthritis) where pain or joint stiffness are limiting factors in conventional strength training protocols [Citation108].
The rehabilitative benefits of cross education are present, both as a strength gain and a prevention of strength loss. Andrushko et al. [Citation109] detailed the preventative effects (sparing of muscle atrophy) of unilateral limb training during a period of contralateral limb immobilization. Alternatively, the present meta-analysis has demonstrated the presence of a strength gain in the contralateral (more-affected) limb of patient populations, following unilateral training of the less-affected limb. Dragert and Zehr [Citation101] reported significant improvements in the timed-up-and-go (TUG) test following unilateral dorsiflexion training poststroke, and small but non-significant improvements in the modified Ashworth and Berg balance tests. Similarly, Kim et al. [Citation102] demonstrated significant increases in gait velocity, cadence, stride length, symmetry, and double support periods following unilateral kicking movements of the less-affected limb, poststroke. Manca et al. [Citation103] compared functional gains following direct versus contralateral training of the more-affected versus less-affected limb, respectively. Significant improvements in timed walking tests were seen in both groups. However, the direct training group had larger effects as well as significant improvements on the TUG test, for which contralateral training group did not. Taken together, the contralateral strength gains of cross education are promising for the rehabilitation of functional movements, specifically when the more-affected limb is unable to perform strength training.
There were numerous methodological deficiencies that were identified by previous meta-analyses including the need for control group data [Citation6] and the lack of familiarization [Citation4]. Both of these methodological controls are instituted for the purpose of minimizing ‘quick jumps in strength’ that would over-estimate the magnitude of cross education. The present meta-analysis included 48 control units for the cross education limb reporting an average strength gain of 2.2% (median: 2.1%, range: –6%–11%). Therefore, the inclusion of a control group is important to account for the over-estimation of cross education due to extraneous factors such as task familiarization.
It has been shown that task familiarity and familiarization contractions can increase force approximately 3–11% within a single session [Citation110–113]. Carroll et al. [Citation4] estimated that the effect of familiarization on the overestimation of cross education was approximately 4%. Therefore, it is surprising that there was no significant difference in the strength gain between groups that were familiarized and those that were not. It was hypothesized that a lack of familiarization would overestimate the magnitude of the cross education and training strength gain. The likely reason for the absence of difference in the strength gain is the lack of reporting in the majority of studies as to what was considered to be ‘familiarization’. Since most studies neglected to detail the method of familiarization, any study which noted that its participants were ‘familiarized’, be it a demonstration, a single test contraction, or an entire session, was included in the ‘familiarized’ group.
The large number of units included in the present meta-analysis allowed for the comparison of cross education between upper and lower limbs and between sexes in 135 units of able-bodied participants. Manca et al. [Citation7], separated 31 studies into upper and lower limb training finding a larger magnitude of cross education in the lower limb (16.4%) compared to the upper limb (9.4%). However, the present meta-analysis found no significant difference between cross education in the lower (18%) and upper (17%) limbs. Similarly, there was no significant difference (p = 0.60) in the magnitude of cross education between males (16%) and females (17%), However, comparison between sexes in the trained limb revealed slightly larger (p = 0.06) training adaptations in females (33%) compared to males (26%). This resulted in a slightly larger (p = 0.17) cross-body transfer of strength in males (65% transfer) compared to females (54% transfer).
To date, many studies have assumed an equality between sexes in the magnitude of cross education, often citing the review by Zhou [Citation8], which does not compare sexes. In the literature, only two studies [Citation43, Citation100] included sex comparisons following unilateral training. Both studies also found significant differences between sexes in the magnitude of the training adaptation, but no difference in the magnitude of cross education. This indicates that there is a difference in the amount of transfer (or ratio between trained and untrained limbs) between the sexes, however previous literature is conflicting. Hubal et al. [Citation43] found a significantly higher strength cross-body transfer ratio in females (21%) compared to males (16%). Alternatively, Tracy et al. [Citation100] found a significantly lower strength transfer ratio in females (32% transfer) compared to males (36% transfer).
Conclusion
A review of 141 unilateral training units resulted in a cross education strength gain of 18% in young adults, 15% in older adults, and 29% in a patient population, which is higher than previous estimates [Citation4, Citation6, Citation7] of 8% to 12%. The cross education effect was accompanied by a significant moderate to large effect size in each population. The average cross-body transfer ranged from 48% to 77% slightly higher that previous estimates of 35–60% [Citation4, Citation6]. The present analysis identified: the presence of cross education in young and older able-bodied participants as well as patient populations; the efficacy of EMS training over voluntary modalities; and the equivalence in cross education between upper and lower limbs as well as in males and females. The 15–29% magnitude of cross education is promising for the use of unilateral training in rehabilitation.
Disclosure Statement
No potential conflict of interest was reported by the authors.
Additional information
Notes on contributors
David A. Gabriel
Lara A. Green recently completed her Ph.D. in health biosciences at Brock University examining the phenomenon of cross education. David A. Gabriel completed his Ph.D. in biomechanics at McGill University in 1995. He worked as a post-doctoral fellow in orthopedic biomechanics at the Mayo Clinic until 1997. He is currently a professor at Brock University.
References
- Scripture EW, Smith TL, Brown EM. On the education of muscular control and power. Stud Yale Psychol Lab. 1894;2:114–119.
- Lee M, Carroll TJ. Cross education: possible mechanisms for the contralateral effects of unilateral resistance training. Sports Med. 2007;37(1):1–14.
- Ruddy KL, Carson RG. Neural pathways mediating cross education of motor function. Front Hum Neurosci. 2013;7:1–22.
- Carroll TJ, Herbert RD, Munn J, Lee M, Gandevia SC. Contralateral effects of unilateral strength training: evidence and possible mechanisms. J Appl Physiol. 2006;101(5):1514–1522.
- Hendy AM, Spittle M, Kidgell DJ. Cross education and immobilisation: mechanisms and implications for injury rehabilitation. J Sci Med Sport. 2012;15(2):94–101.
- Munn J, Herbert RD, Gandevia SC. Contralateral effects of unilateral resistance training: a meta-analysis. J Appl Physiol. 2004;96(5):1861–1866.
- Manca A, Dragone D, Dvir Z, Deriu F. Cross-education of muscular strength following unilateral resistance training: a meta-analysis. Eur J Appl Physiol. 2017;117(11):1–2354.
- Zhou S. Chronic neural adaptations to unilateral exercise: mechanisms of cross education. Exerc Sport Sci Rev. 2000;28(4):177–184.
- Ehrensberger M, Simpson D, Broderick P, Monaghan K. Cross-education of strength has a positive impact on post-stroke rehabilitation: a systematic literature review. Top Stroke Rehabil. 2016;23(2):126–135.
- Cirer-Sastre R, Beltrán-Garrido JV, Corbi F. Contralateral effects after unilateral strength training: a meta-analysis comparing training loads. J Sports Sci Med. 2017;16:180–186.
- Review Manager (RevMan); The Nordic Cochrane Centre, The Cochrane Collaboration: Copenhagen, 2014;
- Adamson M, MacQuaide N, Helgerud J, Hoff J, Kemi OJ. Unilateral arm strength training improves contralateral peak force and rate of force development. Eur J Appl Physiol. 2008;103(5):553–559.
- Bemben MG, Murphy RE. Age related neural adaptation following short term resistance training in women. J Sports Med Phys Fitness. 2001;41(3):291–299.
- Beyer KS, Fukuda DH, Boone CH, Wells AJ, Townsend JR, Jajtner AR, et al. Short-Term Unilateral Resistance Training Results in Cross Education of Strength without Changes in Muscle Size, Activation, or Endocrine Response. J Strength Cond Res . 2015;30:1213–23.
- Bezerra P, Zhou S, Crowley Z, Brooks L, Hooper A. Effects of unilateral electromyostimulation superimposed on voluntary training on strength and cross-sectional area. Muscle Nerve. 2009;40(3):430–437.
- Boyes NG, Yee P, Lanovaz JL, Farthing JP. Cross-education after high-frequency versus low-frequency volume-matched handgrip training. Muscle Nerve. 2017;56(4):689–695.
- Abazović E, Kovačević E, Kovač S, Bradić J. The effect of training of the non-dominant knee muscles on ipsi-and contralateral strength gains. Isokinet Exerc Sci. 2015;23(3):177–182.
- Cabric M, Appell H-J. Effect of electrical stimulation of high and low frequency on maximum isometric force and some morphological characteristics in men. Int J Sports Med. 1987;08(04):256–260.
- Cannon RJ, Cafarelli E. Neuromuscular adaptations to training. J Appl Physiol. 1987;63(6):2396–2402.
- Carolan B, Cafarelli E. Adaptations in coactivation after isometric resistance training. J Appl Physiol. 1992;73(3):911–917.
- Coleman AE. Effect of unilateral isometric and isotonic contractions on the strength of the contralateral limb. Res Q Am Assoc Health Phys Educ Recreat. 1969;40(3):490–495.
- Coombs TA, Frazer AK, Horvath DM, Pearce AJ, Howatson G, Kidgell DJ. Cross-education of wrist extensor strength is not influenced by non-dominant training in right-handers. Eur J Appl Physiol. 2016;116(9):1757–1769.
- Colomer-Poveda D, Romero-Arenas S, Vera-Ibáñez A, Viñuela-García M, Márquez G. Effects of 4 weeks of low-load unilateral resistance training, with and without blood flow restriction, on strength, thickness, V wave, and H reflex of the soleus muscle in men. Eur J Appl Physiol. 2017;117(7):1339–1347.
- Coratella G, Milanese C, Schena F. Cross-education effect after unilateral eccentric-only isokinetic vs dynamic constant external resistance training. Sport Sci Health. 2015;11(3):329–335.
- Dankel SJ, Counts BR, Barnett BE, Buckner SL, Abe T, Loenneke JP. Muscle adaptations following 21 consecutive days of strength test familiarization compared with traditional training. Muscle Nerve. 2017;56(2):307–314.
- Dragert K, Zehr EP. Bilateral neuromuscular plasticity from unilateral training of the ankle dorsiflexors. Exp Brain Res. 2011;208(2):217–227.
- Ehsani F, Moghadam AN, Ghandali H, Ahmadizade Z. The comparison of cross–education effect in young and elderly females from unilateral training of the elbow flexors. Med J Islam Repub Iran. 2014;28:138.
- Evetovich TK, Housh TJ, Housh DJ, Johnson GO, Smith DB, Ebersole KT. The effect of concentric isokinetic strength training of the quadriceps femoris on electromyography and muscle strength in the trained and untrained limb. J Strength Cond Res. 2001;15(4):439–445.
- Farthing JP, Borowsky R, Chilibeck PD, Binsted G, Sarty GE. Neuro-physiological adaptations associated with cross-education of strength. Brain Topogr. 2007;20(2):77–88.
- Farthing JP, Chilibeck PD. The effect of eccentric training at different velocities on cross-education. Eur J Appl Physiol. 2003;89(6):570–577.
- Farthing JP, Chilibeck PD, Binsted G. Cross-education of arm muscular strength is unidirectional in right-handed individuals. Med Sci Sports Exerc. 2005;37(9):1594–1600.
- Fimland MS, Helgerud J, Solstad GM, Iversen VM, Leivseth G, Hoff J. Neural adaptations underlying cross-education after unilateral strength training. Eur J Appl Physiol. 2009;107(6):723–730.
- Gardner GW. Specificity of strength changes of the exercised and nonexercised limb following isometric training. Res Q Am Assoc Health Phys Educ Recreat. 1963;34(1):98–101.
- Hellebrandt FA, Parrish AM, Houtz SJ. The influence of unilateral exercise on the contralateral limb. Arch Phys Med Rehabil. 1947;28(2):76–85.
- Hellebrandt FA, Waterland JC. Indirect learning. The influence of unimanual exercise on related muscle groups of the same and the opposite side. Am J Phys Med Rehabil. 1962;41(2):45–55.
- Hortobágyi T, Lambert NJ, Hill JP. Greater cross education following training with muscle lengthening than shortening. Med Sci Sports Exerc. 1997;29(1):107–112.
- Hortobágyi T, Scott K, Lambert J, Hamilton G, Tracy J. Cross-education of muscle strength is greater with stimulated than voluntary contractions. Motor Control. 1999;3(2):205–219.
- Housh DJ, Housh TJ, Johnson GO, Chu WK. Hypertrophic response to unilateral concentric isokinetic resistance training. J Appl Physiol. 1992;73(1):65–70.
- Housh TJ, Housh DJ, Weir JP, Weir L. Effects of eccentric-only resistance training and detraining. Int J Sports Med. 1996;17(2):145–148.
- Housh TJ, Housh DJ, Weir JP, Weir L. Effects of unilateral concentric-only dynamic constant external resistance training. Int J Sports Med. 1996;17(5):338–343.
- Houston M. Muscle performance, morphology and metabolic capacity during strength training and detraining: a one leg model. Eur J Appl Physiol. 1983;51(1):25–35.
- Huang L-P, Zhou S, Lu Z, Tian Q, Li X, Cao L-J, Yu J-H, Wang H. Bilateral effect of unilateral electroacupuncture on muscle strength. J Altern Complement Med. 2007;13(5):539–546.
- Hubal MJ, Gordish-Dressman H, Thompson PD, Price TB, Hoffman EP, Angelopoulos TJ, Gordon PM, Moyna NM, Pescatello LS, Visich PS, others. Variability in muscle size and strength gain after unilateral resistance training. Med Sci Sports Exerc. 2005;37(6):964–72.
- Ikai M, Fukunaga T. A study on training effect on strength per unit cross-sectional area of muscle by means of ultrasonic measurement. Int Z Für Angew Physiol Einschl Arbeitsphysiologie. 1970;28(3):173–180.
- Kadri MA, Noé F, Nouar MB, Paillard T. Effects of training programs based on ipsilateral voluntary and stimulated contractions on muscle strength and monopedal postural control of the contralateral limb. Eur J Appl Physiol. 2017;117(9):1799–1806.
- Kannus P, Alosa D, Cook L, Johnson RJ, Renström P, Pope M, Beynnon B, Yasuda K, Nichols C, Kaplan M. Effect of one-legged exercise on the strength, power and endurance of the contralateral leg. A randomized, controlled study using isometric and concentric isokinetic training. Eur J Appl Physiol Occup Physiol . 1992;64(2):117–126.
- Khouw W, Herbert R. Optimisation of isometric strength training intensity. Aust J Physiother. 1998;44(1):43–46.
- Kidgell DJ, Frazer AK, Rantalainen T, Ruotsalainen I, Ahtiainen J, Avela J, Howatson G. Increased cross-education of muscle strength and reduced corticospinal inhibition following eccentric strength training. Neuroscience. 2015;300:566–575.
- Kidgell DJ, Stokes MA, Pearce AJ. Strength training of one limb increases corticomotor excitability projecting to the contralateral homologous limb. Motor Control. 2011;15(2):247–266.
- Kofotolis ND, Kellis E. Cross-training effects of a proprioceptive neuromuscular facilitation exercise programme on knee musculature. Phys Ther Sport. 2007;8(3):109–116.
- Komi P. Effect of isometric strength training on mechanical, electrical, and metabolic aspects of muscle function. Eur J Appl Physiol. 1978;40(1):117–55.
- Krotkiewski M, Aniansson A, Grimby G, Björntorp P, Sjöström L. The effect of unilateral isokinetic strength training on local adipose and muscle tissue morphology, thickness, and enzymes. Eur J Appl Physiol. 1979;42(4):271–281.
- Lagerquist O, Zehr EP, Docherty D. Increased spinal reflex excitability is not associated with neural plasticity underlying the cross-education effect. J Appl Physiol. 2006;100(1):83–90.
- Lapole T, Canon F, Pérot C. Ipsi- and contralateral H-reflexes and V-waves after unilateral chronic Achilles tendon vibration. Eur J Appl Physiol. 2013;113(9):2223–2231.
- Latella C, Kidgell DJ, Pearce AJ. Reduction in corticospinal inhibition in the trained and untrained limb following unilateral leg strength training. Eur J Appl Physiol. 2012;112(8):3097–3107.
- Lee M, Gandevia SC, Carroll TJ. Unilateral strength training increases voluntary activation of the opposite untrained limb. Clin Neurophysiol. 2009;120(4):802–808.
- Lepley LK, Palmieri-Smith RM. Cross-education strength and activation after eccentric exercise. J Athl Train. 2014;49(5):582–589.
- Lewis S, Nygaard E, Sanchez J, EGEBLAD H, SALTIN B. Static contraction of the quadriceps muscle in man: cardiovascular control and responses to one-legged strength training. Acta Physiol Scand. 1984;122(3):341–353.
- Magnus C, Boychuk K, Kim SY, Farthing JP. At-home resistance tubing strength training increases shoulder strength in the trained and untrained limb. Scand J Med Sci Sports. 2014;24(3):2223–593.
- Manca A, Pisanu F, Ortu E, Natale ERD, Ginatempo F, Dragone D, Tolu E, Deriu F. A comprehensive assessment of the cross-training effect in ankle dorsiflexors of healthy subjects: a randomized controlled study. Gait Posture. 2015;42(1):1–6.
- Manca A, Ginatempo F, Cabboi MP, Mercante B, Ortu E, Dragone D, Natale ERD, Dvir Z, Rothwell JC, Deriu F. No evidence of neural adaptations following chronic unilateral isometric training of the intrinsic muscles of the hand: a randomized controlled study. Eur J Appl Physiol. 2016;116(10):1993–2005.
- Mason J, Frazer AK, Horvath DM, Pearce AJ, Avela J, Howatson G, Kidgell DJ. Ipsilateral corticomotor responses are confined to the homologous muscle following cross-education of muscular strength. Appl Physiol Nutr Metab. 2017;43(1):11–22.
- Mathews DK, Shay CT, Godin F, Hogdon R. Cross transfer effects of training on strength and endurance. Res Q Am Assoc Health Phys Educ Recreat. 1956;27(2):212–341.
- Meyers CR. Effects of two isometric routines on strength, size, and endurance in exercised and nonexercised arms. Res Q Am Assoc Health Phys Educ Recreat. 1967;38(3):430–440.
- Miller LE, Wootten DF, Nickols-Richardson SM, Ramp WK, Steele CR, Cotton JR, Carneal JP, Herbert WG. Isokinetic training increases ulnar bending stiffness and bone mineral in young women. Bone. 2007;41(4):685–689.
- Moritani T, DeVries HA. Neural factors versus hypertrophy in the time course of muscle strength gain. Am J Phys Med Rehabil. 1979;58(3):115–130.
- Munn J, Herbert RD, Hancock MJ, Gandevia SC. Training with unilateral resistance exercise increases contralateral strength. J Appl Physiol. 2005;99(5):1880–1884.
- Narici MV, Roi GS, Landoni L, Minetti AE, Cerretelli P. Changes in force, cross-sectional area and neural activation during strength training and detraining of the human quadriceps. Eur J Appl Physiol. 1989;59(4):310–319.
- Nickols-Richardson SM, Miller LE, Wootten DF, Ramp WK, Herbert WG. Concentric and eccentric isokinetic resistance training similarly increases muscular strength, fat-free soft tissue mass, and specific bone mineral measurements in young women. Osteoporos Int. 2007;18(6):789–796.
- Palmer HS, Haberg AK, Fimland MS, Solstad GM, Moe Iversen V, Hoff J, Helgerud J, Eikenes L. Structural brain changes after 4 wk of unilateral strength training of the lower limb. J Appl Physiol. 2013;115(2):167–175.
- Parker RH. The effects of mild one-legged isometric or dynamic training. Eur J Appl Physiol Occup Physiol . 1985;54(3):262–268.
- Patten C, Kamen G, Rowland DM. Adaptations in maximal motor unit discharge rate to strength training in young and older adults. Muscle Nerve. 2001;24(4):542–550.
- Ploutz LL, Tesch PA, Biro RL, Dudley GA. Effect of resistance training on muscle use during exercise. J Appl Physiol. 1994;76(4):1675–1681.
- Rutherford OM, Jones DA. The role of learning and coordination in strength training. Eur J Appl Physiol Occup Physiol . 1986;55(1):100–105.
- Sariyildiz M, Karacan I, Rezvani A, Ergin O, Cidem M. Cross-education of muscle strength: cross-training effects are not confined to untrained contralateral homologous muscle. Scand J Med Sci Sports. 2011;21(6):e359–e364.
- Shaver LG. Effects of training on relative muscular endurance in ipsilateral and contralateral arms. Med Sci Sports. 1970;2(3):262.
- Shaver LG. Cross transfer effects of conditioning and deconditioning on muscular strength. Ergonomics. 1975;18(1):9–16.
- Shields RK, Leo KC, Messaros AJ, Somers VK. Effects of repetitive handgrip training on endurance, specificity, and cross-education. Phys Ther. 1999;79(5):467.
- Shima N, Ishida K, Katayama K, Morotome Y, Sato Y, Miyamura M. Cross education of muscular strength during unilateral resistance training and detraining. Eur J Appl Physiol. 2002;86(4):287–294.
- Slater-Hammel AT. Bilateral effects of muscle activity. Res Q Am Assoc Health Phys Educ Recreat. 1950;21(3):203–209.
- Smith LE. Facilitatory effects of myotatic stretch training upon leg strength and contralateral transfer. Am J Phys Med Rehabil. 1970;49(2):132–141.
- Souron R, Farabet A, Féasson L, Belli A, Millet GY, Lapole T. Eight weeks of local vibration training increases dorsiflexor muscles cortical voluntary activation. J Appl Physiol. 2017;122:1504–1515.
- Teixeira LA, Caminha LQ. Intermanual transfer of force control is modulated by asymmetry of muscular strength. Exp Brain Res. 2003;149(3):312–319.
- Tillin NA, Pain MT, Folland JP. Short-term training for explosive strength causes neural and mechanical adaptations. Exp Physiol. 2012;97(5):630–641.
- Tillin NA, Pain MTG, Folland JP. Short-term unilateral resistance training affects the agonist-antagonist but not the force-agonist activation relationship. Muscle Nerve. 2011;43(3):375–384.
- Weir JP, Housh DJ, Housh TJ, Weir L. The effect of unilateral concentric weight training and detraining on joint angle specificity, cross-training, and the bilateral deficit. J Orthop Sports Phys Ther. 1997;25(4):264–270.
- Yasuda Y, Miyamura M. Cross transfer effects of muscular training on blood flow in the ipsilateral and contralateral forearms. Eur J Appl Physiol. 1983;51(3):321–329.
- Yue G, Cole KJ. Strength increases from the motor program: comparison of training with maximal voluntary and imagined muscle contractions. J Neurophysiol. 1992;67(5):1114–1123.
- Zhou S, Oakman A, Davie AJ. Effects of unilateral voluntary and electromyostimulation training on muscular strength on the contralateral limb. Hong Kong J Sports Med Sports. 2002;14:1–11.
- Zoeller RF, Angelopoulos TJ, Thompson BC, Wenta MR, Price TB, Thompson PD, Moyna NM, Seip RL, Clarkson PM, Gordon PM, Pescatello LS, Devaney JM, Gordish-Dressman H, Hoffman EP, Visich PS. Vascular remodeling in response to 12 wk of upper arm unilateral resistance training. Med Sci Sports Exerc. 2009;41(11):2003–2008.
- Zult T, Goodall S, Thomas K, Solnik S, Hortobágyi T, Howatson G. Mirror training augments the cross-education of strength and affects inhibitory paths. Med Sci Sports Exerc. 2016;48(6):1001–1013.
- Roth SM, Martel GF, Ivey FM, Lemmer JT, Metter EJ, Hurley BF, Rogers MA. High-volume, heavy-resistance strength training and muscle damage in young and older women. J Appl Physiol. 2000;88(3):1112–1118.
- Roth SM, Martel GF, Ivey FM, Lemmer JT, Tracy BL, Hurlbut DE, Metter EJ, Hurley BF, Rogers MA. Ultrastructural muscle damage in young vs. older men after high-volume, heavy-resistance strength training. J Appl Physiol. 1999;86(6):1833–1840.
- Hendy AM, Teo W-P, Kidgell DJ. Anodal transcranial direct current stimulation prolongs the cross-education of strength and corticomotor plasticity. Med Sci Sports Exerc. 2015;47(9):1788–1797.
- Hortobágyi T, Maffiuletti NA. Neural adaptations to electrical stimulation strength training. Eur J Appl Physiol. 2011;111(10):2439–2449.
- Leung M, Rantalainen T, Teo W-P, Kidgell D. The ipsilateral corticospinal responses to cross-education are dependent upon the motor-training intervention. Exp Brain Res. 2018;236(5):1331–1346.
- Arkov V, Abramova T, Nikitina T, Afanasjeva D, Suprun D, Milenin O, Tonevitsky A. Cross effect of electrostimulation of quadriceps femoris muscle during maximum voluntary contraction under conditions of biofeedback. Bull Exp Biol Med. 2010;149(1):93–95.
- Brown AB, McCartney N, Sale DG. Positive adaptations to weight-lifting training in the elderly. J Appl Physiol. 1990;69(5):1725–1733.
- Tøien T, Unhjem R, Øren TS, Kvellestad ACG, Hoff J, Wang E. Neural plasticity with age: Unilateral maximal strength training augments efferent neural drive to the contralateral limb in older adults. J Gerontol Ser A. 2018;73(5):596–602
- Tracy BL, Ivey FM, Hurlbut D, Martel GF, Lemmer JT, Siegel EL, Metter EJ, Fozard JL, Fleg JL, Hurley BF. Muscle quality. II. Effects of strength training in 65- to 75-yr-old men and women. J Appl Physiol. 1999;86(1):195–201.
- Dragert K, Zehr EP. High-intensity unilateral dorsiflexor resistance training results in bilateral neuromuscular plasticity after stroke. Exp Brain Res. 2013;225(1):93–104.
- Kim C-Y, Lee J-S, Kim H-D, Kim J-S. The effect of progressive task-oriented training on a supplementary tilt table on lower extremity muscle strength and gait recovery in patients with hemiplegic stroke. Gait Posture. 2015;41(2):425–430.
- Manca A, Cabboi MP, Dragone D, Ginatempo F, Ortu E, De Natale ER, Mercante B, Mureddu G, Bua G, Deriu F. Resistance training for muscle weakness in multiple sclerosis: direct versus contralateral approach in individuals with ankle dorsiflexors’ disparity in strength. Arch Phys Med Rehabil. 2017;98(7):1348–1356.e1.
- Mccartney N, Moroz D, Garner SH, McComas AJ. The effects of strength training in patients with selected neuromuscular disorders. Med Sci Sports Exerc. 1988;20(4):362–368.
- Onigbinde AT, Ajiboye RA, Bada AI, Isaac SO. Inter-limb effects of isometric quadriceps strengthening on untrained contra-lateral homologous muscle of patients with knee osteoarthritis. Technol Health Care. 2017;25(1):19–27.
- Urbin MA, Harris-Love ML, Carter AR, Lang CE. High-intensity, unilateral resistance training of a non-paretic muscle group increases active range of motion in a severely paretic upper extremity muscle group after stroke. Front Neurol. 2015;6:119.
- Cohen J. Statistical power analyses for the social sciences. Hillsdale NJ: Lawrence Erlbauni Assoc. 1988;
- Vaz MA, Baroni BM, Geremia JM, Lanferdini FJ, Mayer A, Arampatzis A, Herzog W. Neuromuscular electrical stimulation (NMES) reduces structural and functional losses of quadriceps muscle and improves health status in patients with knee osteoarthritis. J Orthop Res. 2013;31(4):511–516.
- Andrushko JW, Gould LA, Farthing JP. Contralateral effects of unilateral training: sparing of muscle strength and size after immobilization. Appl Physiol Nutr Metab. 2018. doi:10.1139/apnm-2018-0073
- Green LA, Parro JJ, Gabriel DA. Quantifying the familiarization period for maximal resistive exercise. Appl Physiol Nutr Metab. 2014;39(3):275–281.
- Calder KM, Gabriel DA. Adaptations during familiarization to resistive exercise. J Electromyogr Kinesiol. 2007;17(3):328–335.
- McIntosh KCD, Gabriel DA. Reliability of a simple method for determining muscle fiber conduction velocity. Muscle Nerve. 2012;45(2):257–265.
- Kroll W. Reliability variations of strength in test-retest situations. Res Q Am Assoc Health Phys Educ Recreat. 1963;34(1):50–55.