
Abstract
Introduction: The COVID pandemic has significantly impacted educational development and delivery, yet there is little quantitative research on this topic. The primary objective of this study was to compare the total number of Emergency Medical Service (EMS) Refresher (ER) course completions during 2020 versus prior years. Secondary outcomes examined in person versus on-line/distributive learning during the study period. Methods: The Commission on Accreditation for Prehospital Continuing Education (CAPCE) is the only national organization that accredits continuing education (CE) for paramedics and EMTs and currently has a database with over 14 million CE records. The total number of ER course completions each month in 2020 were compared to 2019 and 2018. We also compared the different educational format types: live in-person (LIP), asynchronous on-line distributive learning (DL), and virtual instructor lead training (VILT) synchronous DL courses. Data was analyzed using descriptive and two-way ANOVA statistics. Results: There were 1,922,783 ER course completions in 2020 versus 1,166,335 in 2019 and 1,074,636 in 2018, representing a 179% increase during the study period. Asynchronous DL course completions in 2020 were 1,830,513 EMS versus 1,078,580 in 2019 and 987,749 in 2018 a 185% increase over the three-year study period. Asynchronous DL monthly means by year was statistically significant, F(2, 99) = 95.632, p < .001. Mean monthly LIP and VLIT educational deliveries by year were not significantly different, p = .802, p = .754, respectively. Total LIP course completions in 2020 were 20,045 versus 51,552 in 2019 and 63,058 in 2018. In 2020 LIP courses made up only 1.0% (20,045/1,922,783) of all ER completions. This study was limited to only EMS professionals taking ER course completions in the CAPCE database. However EMS is not unique, since previous research has suggested that DL has flourished in other health care disciplines while LIP courses have continued to decrease. Conclusion: This large nationwide study of EMS profession has shown the trend toward DL education and a trend away from LIP courses. Future studies should examine the advantages and disadvantages of DL education.
Introduction
The COVID-19 pandemic has significantly impacted educational development and delivery for health care professionals. Yet, there is little quantitative research data on the effects of COVID-19 on education within healthcare. Prior research has been limited, focusing on a single EMS system, an individual institution, or subspecialties within a single institution (Citation1–4). Knowing our ability to develop and deliver ongoing education during a prolonged event is important for the management and mitigation of education during future disasters. Unfortunately, there are very few national databases to assess the educational impact of COVID-19.
The Commission on Accreditation for Prehospital Continuing Education (CAPCE) has a database with over 14 million continuing education (CE) records and is the only national organization that accredits CE for Emergency Medical Service (EMS) professionals. CAPCE accredits different educational formats which include: F1 – classic live in-person (LIP) course, F3 – classic asynchronous on-line/distributive learning (DL) course, and an F5 – virtual instructor lead training (VILT) synchronous DL course, see (Citation5).
Table 1. CAPCE course formats
The primary objective of this study was to compare the total number of EMS Refresher (ER) course completions during 2018, 2019, 2020. Secondary outcomes also compared LIP, DL and VILT courses completions during the study period.
Methods
The large CAPCE database was used to examine the types of educational format delivery over time. This secure database allows only certain CAPCE staff access to the CAPCE CE records. In order to uphold the Family Educational Rights and Privacy Act our database query did not include any individual identifiers and thus all data collected for this study was deidentified (Citation6). This study was administratively approved and determined to be exempt by the Institutional Review Board at East Carolina University Brody School of Medicine.
This study examined the total number of EMS Refresher course completions each year, see . During the three year study period we also examined the total number of different format types including: F1 – classic in person (LIP) course, F3 – classic on-line/distributive learning (DL) course, and F5 – virtual instructor lead training (VILT), see (Citation5). We also compared mean monthly course completions for LIP, DL, VILT during the study period. All data were analyzed using descriptive and two-way ANOVA statistics, using univariate testing with Bonferroni adjusted pairwise comparison by means each year and by education method. Outliers were assessed by inspection of a boxplot, and normality was assessed using QQ-plots. Data analysis was performed using IBM SPSS version 24.
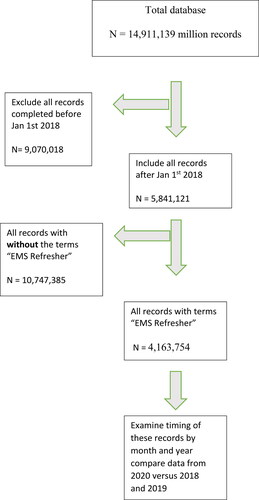
Figure 1. Records Selection Protocol.
Results
During the three-year study period there were a total of 4,163,754 ER course completions, see and . In 2020 there were 1,922,783 total ER course completions versus 1,166,335 in 2019 and 1,074,636 in 2018, representing a 179% increase during the study period.
Table 2. Monthly means by year and delivery methods
Table 3. Totals by year and delivery methods
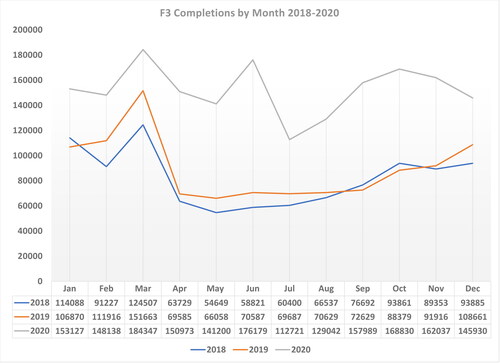
Asynchronous DL course completions for 2020 were 1,830,513 versus 1,078,580 in 2019 and 987,749 in 2018, see and . This large increase of on-line asynchronous DL represents a 70% increase from 2019 to 2020, and a 185% increase from 2018 to 2020, see and .
Figure 2. Monthly mean of delivery method and by year.
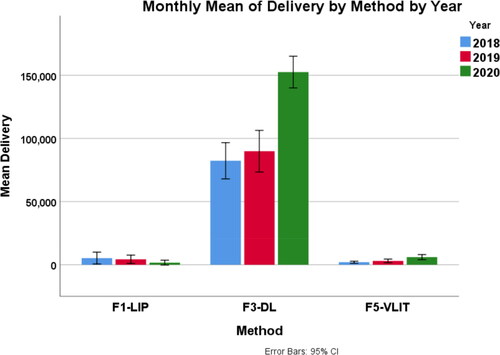
Figure 3. F3 completions by month 2018–2020.
Monthly means for asynchronous DL in 2020 noted a statistically significant difference, F(2, 99) = 95.632, p < .001, partial η2 = .659.
Changes in monthly means by year for LIP and VLIT were not significant, p = .802, p = .754, respectively, see . LIP course completions in 2020 were 20,045 versus 51,552 in 2019 and 63,058 in 2018, see and and . LIP course completions decreased 68% during the study period. In 2020 LIP courses made up only 1.0% (20,045/1,922,783) of all ER course completions. VILT course completions in 2020 were 72,225 versus 36,203 in 2019 and 23,829 in 2018, a 303% increase during the study period. Yet in 2020 VILT courses made up only 3.8% (72,225/1,922,783) of all course completions, see and and .
Figure 4. F1 completions by month 2018–2020.
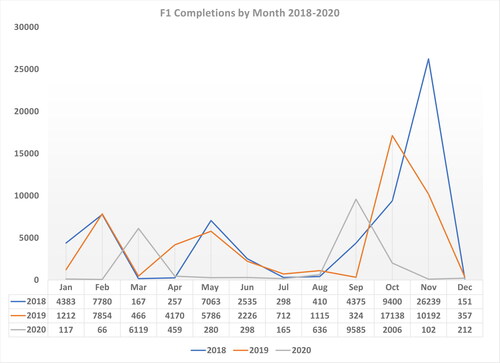
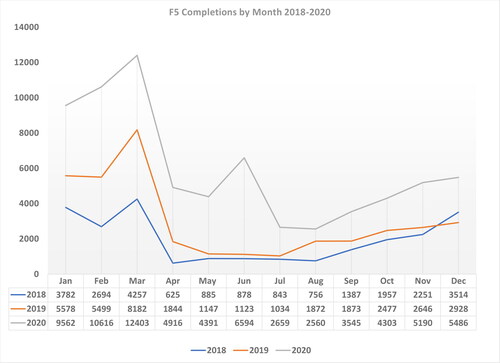
Figure 5. F5 completions by month 2018–2020.
Discussion
This is the first study to examine the trend of DL on a nationwide level in any profession. Previous studies have often been limited in scope or simply descriptive in nature. This study noted that prior to 2020 there had already been a large increase in DL education and a decrease in LIP ER course completions. Additionally, our data showed an even larger increase of DL and VILT course completions during the 2020 COVID pandemic. Although there was an association for an increasing trend in DL and VILT course completions during the pandemic, it did not prove causation.
Overall, for 2020 there was a 70% increase in DL courses completions compared to 2019, and an 185% increase compared to 2018. One possible explanation for the unusual peaks seen in the months of May and June may have been a result of NREMT extending the 2020 recertification deadline from March 31 to June 30 (Citation7). Yet this June 30 deadline extension does not explain a second unusual and prolonged peaks in the months of September, October, and November.
There were no statistically significant differences regarding LIP course completions during the study period. However, in 2018 LIP ER courses made up only 5.8% (63,058/1,074,636) of all ER course completions. This study suggests that there is clearly a trend away from LIP course completions, since in 2020 LIP made up only 1% of all ER course completions nationwide. Although there was no statistically significant difference in LIP course completions, clearly during the pandemic there was a large shift toward DL education and away from LIP course. Although not substantiated, we believe this trend away for LIP courses during the COVID pandemic was done purposefully in order to maximize social distancing.
While DL has flourished due to social distancing there are some associated drawbacks and weakness with DL (Citation8). Indeed, asynchronous DL lacks instant immediate interactions and feedback with the instructor, as well as a lack of hands-on skills training. Although one study suggests that VILT (synchronous) is preferred by students over asynchronous DL, very little research has been published on this topic (Citation9). Prior to COVID-19, several research studies had shown that improving access to initial education and CE impacts recruitment and retention of EMS professionals (Citation10–12). Even before the COVID-19 pandemic access to DL has been identified as a way to improve access to EMS education (Citation13,Citation14).
Limitations
Our study results were limited to only EMS professionals and ER course completions, and not other healthcare professionals nor other EMS courses. Some readers may also argue that this study was limited to only CAPCE accredited courses, and not locally accredited courses. However our study results were not unique, since several smaller and single institution studies have suggested that COVID has helped DL flourish, while making LIP courses extinct (Citation1–4). Anecdotally, we anticipate this is representative of the current educational climate in other healthcare and non-health care professions as well as other EMS educational offerings.
Conclusion
In summary, our data have shown that during the COVID-19 pandemic there was a statistically significant increase in ER course completions for DL on a nationwide scale. Our study also showed that even prior to the COVID-19 pandemic there was decreasing trend in LIP, which now make up only a very small portion of ER courses completions. As DL continues to grow, future studies should examine the advantages and disadvantages of DL education.
References
- Balanchivadze N, Donthireddy V. Hematology/oncology fellowship emergency restructuring in response to the COVID-19 pandemic-Henry Ford Hospital, Michigan. JCO Oncol Pract. 2020;16(9):e943–7. doi:10.1200/op.20.00261.
- Singhi EK, Dupuis MM, Ross JA, Rieber AG, Bhadkamkar NA. Medical hematology/oncology fellows' perceptions of online medical education during the COVID-19 pandemic. J Cancer Educ. 2020;23(4S):S367-S380. doi:10.1007/s13187-020-01863-6.
- Shah S, Diwan S, Kohan L, Rosenblum D, Gharibo C, Soin A, Sulindro A, Nguyen Q, Provenzano DA. The technological impact of COVID-19 on the future of education and health care delivery. Pain Physician. 2020;23(4S):S367–S80.
- Choi B, Jegatheeswaran L, Minocha A, Alhilani M, Nakhoul M, Mutengesa E. The impact of the COVID-19 pandemic on final year medical students in the United Kingdom: A national survey. BMC Med Educ. 2020;20:206. doi:10.1186/s12909-020-02117-1.
- Bailey SC. 2020. Accreditation Manual. Accessed February 27, 2021. https://www.cecbems.org/docs/Accred.Guidebook.pdf
- Diab J, Riley S, Downes A, Gaeta T, Hern HG, Hwang E, Kass L, Kelly M, Luber SD, Martel M, et al. A multicenter study of the family educational rights and privacy act and the standardized letter of recommendation: impact on emergency medicine residency applicant and faculty behaviors. J Grad Med Educ. 2014;6(2):292–5. doi:10.4300/jgme-d-13-00179.1.
- NREMT Extends 2020 Recertification Deadline, Modifies Requirements due to COVID-19. Accessed April 29, 2021. https://www.ems1.com/ems-products/online-training/articles/nremt-extends-2020-recertification-deadline-modifies-requirements-due-to-covid-19-7XRPZGafKUacym6H/.
- Dhawan S. Online learning: A panacea in the time of COVID-19 crisis. J Educ Technol Syst. 2020;49(1):5–22. doi:10.1177/0047239520934018.
- Kunin M, Julliard KN, Rodriguez TE. Comparing face-to-face, synchronous, and asynchronous learning: postgraduate dental resident preferences. J Dent Educ. 2014;78(6):856–66. doi:10.1002/j.0022-0337.2014.78.6.tb05739.x
- Cash RE, Clay CE, Leggio WJ, Camargo CA Jr. Geographic distribution of accredited paramedic education programs in the United States. Prehosp Emerg Care. 2021. doi:10.1080/10903127.2020.1856984.
- Blau G, Chapman SA. Why Do Emergency Medical Services (EMS) Professionals Leave EMS? Prehosp Disaster Med. 2016;31(S1):S105-S111. doi:10.1017/S1049023X16001114.
- Chapman SA, Bentley MA, Crowe RP. Recruitment and retention of new Emergency Medical Technician (EMT)-basics and paramedics. Prehosp Disaster Med. 2016;31(S1):S70–S86. doi:10.1017/S1049023X16001084.
- Education NC-19 TFFI. Approaches for Initial EMS Education at All Levels Following COVID-19 Pandemic National Association of EMS Educators (NAEMSE) Committee on Accreditation of Educational Programs for the Emergency Medical Services Professions (CoAEMSP) National Association. July 2020. Accessed March 16, 2021. https://cdn.ymaws.com/naemse.org/resource/resmgr/coronavirus_resources/naemse_covid19_educationaldo.pdf.
- Boyer CT, Zielewicz J, Frailey GT. Investigating the efficacy of a hybrid EMT course - PubMed. J Allied Health. 2019;48(4):298–301.
