
Abstract
The latest guidelines for cardiopulmonary resuscitation recommend that in case of suspected cardiac arrest first responders, who are close to the emergency location, should be notified by a smartphone app or text message. Smartphone Alerting Systems (SAS) aim to reduce the resuscitation-free interval. Thus, there is a need for uniform reporting of process times. Objective: To compare the response times in a SAS either by using global positioning system (GPS) data or by manual confirmation of first responders arriving at the scene. Methods: In the region of Freiburg (Southern Germany, 1,531 km2, 493,000 inhabitants), a SAS is activated when the emergency dispatch center receives a call regarding suspected cardiac arrest. First responders who accept a mission are tracked using GPS. GPS-based times are logged for each responder when their position is within a radius of 100, 50, or 10 meters around the geographical position of the reported emergency. When arriving at the patient location, the first responders manually confirm “arrived” via their app. GPS-based and manually confirmed response arrival times were compared for all cases between 1 October and 31 March. Results: 192 missions with correct manual logging of the arrival time were included. GPS-based times were available in 175 (91%), 100 (52%), and 30 (16%) cases within radii of 100, 50, and 10 meters, respectively. GPS arrival times were approximately 1.5 minutes shorter when using a 100-meter radius and significantly longer when using a 10-meter radius. No difference was found for a 50-meter radius, but this would result in a lack of data in nearly half of the cases. Conclusion: GPS-based logging of arrival times leads to missing data. A 100-meter circle is associated with a low number of missing values, but 1.5 minutes must be added for the last 100 meters the first responder has to move. A wide range of the difference in response times (GPS vs. manual confirmation) must be regarded as a disadvantage. Manual confirmation reveals precise response times, but first responders may forget to confirm when they arrive. Trial registration: DRKS00016625 (14 April 2019).
Introduction
Out-of-hospital cardiac arrest (OHCA) has low survival rates and a high risk for irreversible neurological damage and disability in survivors. 275,000 people in Europe experience OHCA annually, with only 10% surviving to hospital discharge (Citation1). An important factor contributing to the survival rate is early basic life support (BLS).
The concept of a smartphone alerting system (SAS) aims to alert first responders who are located near the emergency location (Citation2). Due to mobile technology and the common use of smartphones, the implementation of these systems is feasible and becoming widespread in numerous countries (Citation3, Citation4). The latest international resuscitation guidelines recommend that these technologies be implemented to reduce the time to first compression and shock delivery (Citation5).
SASs are developed using different technological approaches. Text message systems usually do not include a solution for logging the arrival time of the first responder. App-based systems offer the possibility of tracking first responders using global positioning system (GPS) technology. In principle, it is possible to determine the arrival time of the first responders using the GPS-tracking features of smartphone systems. The RDL system in Freiburg logs “arrived” times of first responders when they enter a 100-meter radius around the emergency location. In evaluating the process times, we realized that occasionally the time at which a first responder arrived differed from the time that was logged when entering the 100-meter radius. Furthermore, we realized that in some cases, the “arrived” times were not logged at all. This led to the idea of the present study.
The objective of this study was to investigate whether it is possible to determine first responders’ arrival times using GPS technology and to compare these times with the effective arrival times, which are determined by the first responder’s manual confirmation.
Methods
Study Design
This observational study evaluates the response times of first responders in a smartphone-based alerting process using two different methods: GPS-based logging and manual confirmation of the time at which the first responder arrives at the patient location. Data were collected during a six-month period from 1 October 2020 to 31 March 2021. Due to the COVID-19 pandemic, the SAS had been paused in March 2020. We restarted the system with a special pandemic concept after 7 weeks and from June 2020 the alarm acceptance rates were at the same level as before the pandemic (Citation6). First responder activations in the Freiburg dispatch center were included in the analysis (total area: 1,531 km2; total population: 493,036).
Ethics
Ethical approval for this study was provided by the University of Freiburg Ethics Committee (No. 482/18), University of Freiburg, Freiburg, Germany (Chair: Prof. Dr. R. Korinthenberg) on December 4th, 2018.
The study was registered in the German Clinical Trials Register (DRKS00016625, 15 April 2019).
System
The SAS in Freiburg has been operated since July 2018 and is based on the FirstAED software system (FirstAED, Denmark) (Citation7). The charitable organization Region of Lifesavers (Region der Lebensretter (RDL)) is responsible for operating the SAS in Freiburg. According to a ministerial directive for first responder systems, participation requires a medical qualification as a nurse, paramedic, physician, emergency medical technician or certified first responder with 48 hours of medical training. During the observation period, the number of registered first responders increased from 950 to 1,058 volunteers.
When the dispatch center receives emergency calls with the indication “suspected cardiac arrest” or “unconscious person,” the SAS is activated automatically. The SAS system receives the geographical position, which represents the address of the emergency, and the estimated time enroute (ETE) of the closest EMS vehicle. The alerting radius for first responders is set by the SAS with the aim of activating first responders who have a chance of arriving prior to the ambulance. Registered first responders who are located within the alerting radius are activated via the SAS and are asked if they can accept the alarm. A maximum of four volunteers are selected by the system and receive details about the emergency (address and name of the patient). One of them receives the task of bringing a publicly available automated external defibrillator (AED) to the emergency location by navigating to the closest AED when there is one nearby. After the completion of a first responder alarm, the app asks every involved volunteer to fill out a questionnaire.
In the Freiburg area 5 G mobile network technology is already implemented by several providers, but the area covered by the SAS also includes the black forest. In this rural area there are many places with only 3 G or even EDGE network available.
Logging by GPS Tracking
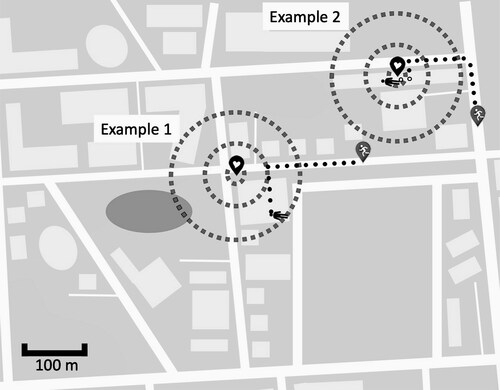
When a first responder receives an alarm and accepts it, that person’s smartphone is added as a resource (similar to the ambulances) by the operations control computer in the dispatch center. For a period of 20 minutes, the system sends repetitive push messages every 10 seconds to each smartphone, which is part of the mission, requesting the current geographical position by using the location services of the smartphones. Poor or lost network connection may make the transmission of the position data impossible. However, the requests are repeated every 10 seconds to allow for the most accurate tracking of first responders. Three circles with radii of 100, 50, and 10 meters around the geographical position of the medical emergency are defined by the SAS. When the position of a first responder is within one of those circles (100, 50, or 10 meters), the first responder is logged as having arrived (). For every first responder, up to three GPS-based arrival times can be retrieved, as the time for each radius is registered separately.
Figure 1. Heart icon represents the geographical position of the reported emergency. Gray icons with white stickman represent first responders in a mission. Black stickman represents the patient. Three circles are drawn with radii of 100, 50, and 10 meters around the emergency location. A GPS position within the respective circle results in logging the first responder as “arrived.”
Logging by Manual Confirmation
Arrival times are also detected by using an arrived button in the smartphone app. This feature allows first responders to press a dedicated button when they arrive at the emergency location. When a first responder presses the button and confirms having arrived, the respective time is saved in the app and transmitted to the dispatch center. Poor or lost network coverage of the first responder´s smartphone will not lead to transmission of incorrect data. The arrival time is transmitted to the backend system as soon as the connection is restored. The first responders are instructed to confirm their arrival at the time that they reach the patient. This includes the time spent walking upstairs to the specific floor or waiting until a flat door is opened. Sometimes a first responder might forget to press the button or might start first aid measures and confirm arrival later. To identify these cases, we included one question in the first responder questionnaire evaluating whether the arrival time was confirmed correctly.
Data Collection
Every alert of the SAS is registered in the FirstAED backend system in the dispatch center. The process times were extracted from the backend database and used for the analysis. If a first responder reported that a manually confirmed arrival time was incorrect, those data were excluded from the analysis. The clocks of the FirstAED server and the dispatch center system are synchronized.
Patient and Public Involvement
Patients and the public were not involved in the design, conduct, reporting, and dissemination plans of this research.
Statistical Analysis
All statistical analyses and visualizations were conducted using R statistic software version 4.0.3, the R package ggplot2 and BlandAltmanLeh (Citation8, Citation9). To test the assumption of normally distributed data, a Shapiro-Wilk test was performed. Response times were compared using a Wilcoxon signed rank test. Data were expressed as medians with interquartile ranges, and p < .05 was considered significant.
Results
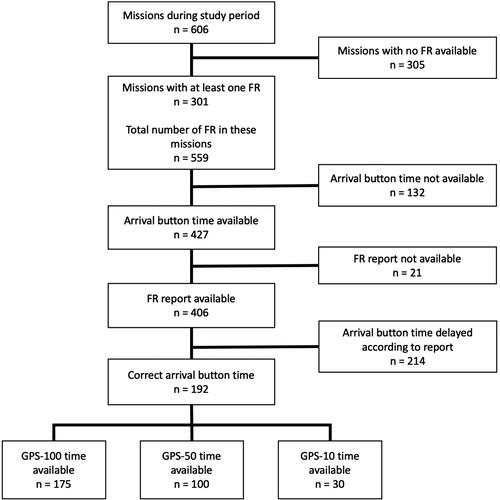
Between 1 October 2020 and 31 March 2021, in 301 of 606 missions, at least one first responder accepted the alarm. In total, 559 first responders were active in these 301 missions. The number of first responder alarms for which the arrival times for manual confirmation and GPS could be retrieved is shown in .
Figure 2. Flow diagram of the cases included in the study.
The mean distance between the first responders’ position and the emergency site was 404 meters IQR [258 to 625 meters].
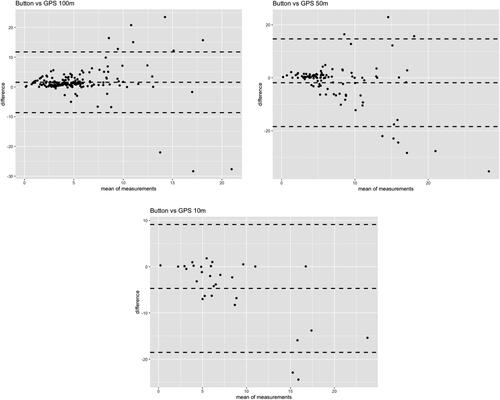
The manually confirmed response times and corresponding GPS-based times are depicted for each radius in .
Figure 3. Bland-Altmann plots for the response times of first responders. Each value represents the real arrival time (manual confirmation) and the time at which the first responder’s position was logged within the circle with a radius of 100 (a), 50 (b), or 10 (c) meters around the geographical position of the reported emergency. The outer dashed lines represent the 95% confidence interval of the mean of all measurements, which is marked by the middle-dashed line.
shows the number of first responder missions with successful GPS-based logging of arrival among all first responder missions with manually confirmed arrival.
Table 1. GPS-based logging versus manual confirmation of arrival times.
The number of successful GPS-based logs of arrival decreased for arrival radii of 100, 50, and 10 meters (). The mean response times measured by manual confirmation and by GPS are given in . Measuring the response times using the GPS-100 meter circle reveals too short response times and using the GPS-10 meters results in measuring too long response times (). The median of manually confirmed response times and the median of GPS-50 response times are nearly identical, but the difference has a wide range. In 37% of the cases with successful logging of GPS-50 time, the difference between manual confirmation and GPS-based time was less than one minute.
Discussion
This study included 192 cases in which a first responder accepted an alarm, arrived at the patient site, and confirmed that he or she had arrived via the app. When a GPS-based system was used to log arrival times, time stamps were successfully obtained in 91%, 52%, and 16% of cases for radii of 100, 50, and 10 meters, respectively. There might be multiple reasons for these findings. First, the emergency location is represented as a geographical position on a map. This position does not necessarily match the exact position of the patient. One example is shown in (example 1): The emergency location in the SAS is a geographical position representing the address of a patient’s house. If the current position of the patient is in the bottom-right corner of the house or even in the garden, this position might be outside the 10-meter, 50-meter, or even 100-meter radius, resulting in the system not being able to log the first responder as having arrived. The chance that the exact position of the patient is within the circle around the position of the emergency address to which the first responders are directed decreases with smaller radii. Other factors leading to missing values might comprise poor network coverage or lack of a GPS signal. The backend system sends push messages to the smartphones of the first responders who are involved in an alarm every 10 seconds requesting the exact GPS position. Poor network coverage might result in delayed transmission of the position or even no answer. When the connection is restored, the next push request will be answered and tracking of the first responder is possible again. However, if the GPS coverage is poor in the whole circle, in which the first responders are logged as arrived, it might be impossible to log the arriving time using GPS tracking (see , example 2). Using larger circles increases the probability that the first responder is logged as having arrived before he or she enters an area with poor GPS coverage (e.g., building, in which the patient is located). This might be an explanation for the lower proportion of missing data when using the 100-meter circle.
If the GPS signal is compromised the smartphone might not be able to retrieve a precise position and might send a wrong position to the SAS backend system. This might happen when the first responder enters the circle, in which the arrival is logged. As a result, the first responder´s real position might be within the 100-meter (50-meter; 10-meter) circle, but the position sent to the backend is outside the respective circle. The probability of the first responder being logged successfully as having entered the respective circle decreases with smaller radii.
Regarding the 50-meter and 100-meter radii a higher variability was observed in longer response times. Since longer response times usually occur in rather rural areas, this observation might be due to differences in network coverage, which can lead to over- as well as underestimation of the arrival time.
When we compared the GPS-based arrival times and the manually confirmed times, we found that first responders were logged as arrived too early when using a 100-meter radius and they were logged too late when using a 10-meter radius. When a 50-meter radius is used, there is no significant difference, but this would result in a lack of data in nearly half of the cases. The median GPS based arrival times using a 100-meter circle are approximately 1.5 minutes earlier than the median arrival times using manual confirmation. This can be explained by a speed of the first responder of 1 meter/second. One could assume that the median arrival time can probably best be approximated by using the median GPS 100-meter arrival times and adding 1.5 minutes to it. However, the difference between manual confirmation and GPS-100 response times has a wide range, and in some cases the difference is much longer than 1.5 minutes.
Furthermore, when considering a single mission, the arrival time using GPS and manual confirmation are not identical in most cases. In the Freiburg system (and probably in other SAS systems, too), the dispatcher can see the positions of the first responders on the EMS dispatch system map and receive a notification when a first responder arrives. The feature enabling the first responders to manually confirm his or her arrival is rated as an added value in our system.
We specified an “I arrived with the patient” button feature in the alerting app. This feature was previously described by Stroop and colleagues (Citation10), but in a current manuscript, the same authors state that a smartphone-based recording of response times is not reliably available (Citation11). The authors might have experienced the problem that first responders forget to confirm having arrived due to the need to immediately start BLS or other tasks or confirm late, which might result in less accurate data. We anticipated these problems and included a question in the questionnaire that had to be filled out after each mission. In one-quarter of the cases, the first responders forgot to confirm their arrival, and in approximately half of the missions, the first responders reported that they had confirmed their arrival after a delay. We assume that it is very important to take measures to improve the accuracy of manual confirmation of arrival, including the request to confirm via the button in the app when approaching the patient but directly before treatment starts. Furthermore, this important issue has since been included in the training tutorial for new first responders.
The objective of SAS is to shorten the resuscitation-free interval of OHCA. Recent studies have revealed promising results: Alerting nearby first responders can result in response times of approximately four minutes (Citation3). The latest resuscitation guidelines include a new chapter, “Systems saving lives,” and recommend that “first responders […] who are near a suspected OHCA should be notified […] through an alerting system implemented with a smartphone app or a text message” (Citation5). However, these systems have not yet been established in every European country, and a wide variety of different systems exist (Citation12). Due to recent hardware and software developments, smartphone apps can be used instead of text messages to alert first responders. The possibility of locating first responders and sending the alarm to those whose current position is close to the emergency location leads to reduced response times (Citation13). There is a need for more research about how to achieve high response rates and short response times, especially in sparsely populated regions, where it might be difficult to achieve a high density of first responders. Furthermore, it is not yet known which distance from the emergency location is optimal for the activation of first responders, especially when aiming to achieve response times below 5 minutes. Using a small distance results in short response times but a lower response rate due to fewer first responders being available (Citation14). Research on the optimal distance, first responder density, and even intelligent algorithms for urban and rural areas requires exact documentation of the process times. Some research groups have worked with estimated response times (Citation11, Citation15), others have used GPS-based tracking to evaluate response times (Citation16, Citation17), and some manuscripts have not explained how response times were measured (Citation18).
Further research on SAS should be based on valid process times and not on estimated data. Recommendations for standardized documentation of OHCA were proposed as early as 1991 (Citation19). The 2015 update of the Utstein Resuscitation Registry template for out-of-hospital cardiac arrest includes the measurement of the process times (Citation20). However, this includes only the bystander (who is not part of an organized emergency response system) and the response time of the first emergency response vehicle. With the increasing spread of SAS there is a need for uniform reporting regarding the key parameters (probably availability of first responders in case of an alarm, response times, and perhaps some more).
In the future, the accuracy of the incident location might be improved by using GPS data of the caller´s smartphone instead of the geographical position of the emergency address. Advanced mobile location service (AML) is already established in many countries (Citation21). This technology enables the dispatch center to retrieve the GPS position of the caller. Simulation research to compare GPS and manual confirmation times could be helpful to test for different confounders such as GPS accuracy in buildings and differences in hard- and software.
Limitations
GPS accuracy varies between different hardware, operating systems and versions of the operating system. However, when GPS is turned on, the accuracy goes up to about one meter within short time with a current modern smartphone.
First responders in a SAS use many different smartphones, and it is not possible to control the used hardware and operating system. However, when setting up a SAS, the responsible persons should carefully plan how to measure process times. Once a reliable set up is done, further development and improvements can be monitored.
Conclusion
Our data comprised two different methods to reveal response times. Manual confirmation can probably be the most precise way to document the arrival time. However, it must be ensured that first responders confirm when they arrive. Automatically measuring arrival times using GPS tracking offers advantages by allowing first responders to focus on their mission. In this case, a 100-meter circle around the emergency scene is associated with a low number of missing values, but 1.5 minutes must be added for the last 100 meters the first responder has to move. A wide range of the difference in response times measured by GPS and manually confirmed response times must be regarded as a disadvantage.
References
- Atwood C, Eisenberg MS, Herlitz J, Rea TD. Incidence of EMS-treated out-of-hospital cardiac arrest in Europe. Resuscitation. 2005;67(1):75–80. doi:10.1016/j.resuscitation.2005.03.021.
- Ringh M, Rosenqvist M, Hollenberg J, Jonsson M, Fredman D, Nordberg P, Järnbert-Pettersson H, Hasselqvist-Ax I, Riva G, Svensson L, et al. Mobile-phone dispatch of laypersons for CPR in out-of-hospital cardiac arrest. N Engl J Med. 2015;372(24):2316–25. doi:10.1056/NEJMoa1406038.
- Scquizzato T, Pallanch O, Belletti A, Frontera A, Cabrini L, Zangrillo A, Landoni G. Enhancing citizens response to out-of-hospital cardiac arrest: a systematic review of mobile-phone systems to alert citizens as first responders. Resuscitation. 2020;152:16–25. doi:10.1016/j.resuscitation.2020.05.006.
- Valeriano A, Van Heer S, de Champlain F, Brooks S. Crowdsourcing to save lives: a scoping review of bystander alert technologies for out-of-hospital cardiac arrest. Resuscitation. 2021;158:94–121. doi:10.1016/j.resuscitation.2020.10.035.
- Semeraro F, Greif R, Böttiger BW, Burkart R, Cimpoesu D, Georgiou M, Yeung J, Lippert F, S Lockey A, Olasveengen TM, et al. European resuscitation council guidelines 2021: systems saving lives. Resuscitation. 2021;161:80–97. doi:10.1016/j.resuscitation.2021.02.008.
- Ganter J, Damjanovic D, Trummer G, Busch H-J, Baldas K, Hänsel M, Müller MP. Smartphone based alerting of first responders during the corona virus disease-19 pandemic: an observational study. Medicine (Baltimore). 2021;100(27):e26526 doi:10.1097/MD.0000000000026526.
- Ganter J, Trummer G, Damjanovic D, Baldas K, Busch H-J, Müller M. APP-based alarm system “FirstAED” for cardiopulmonary resuscitation in Freiburg Breisgau-Hochschwarzwald. Resuscitation. 2019;142:e106–7. doi:10.1016/j.resuscitation.2019.06.257.
- R Core Team. R: A language and environment for statistical computing. Vienna (Austria): R Foundation for Statistical Computing; 2021. https://www.R-project.org/
- Wickham H. ggplot2: Elegant graphics for data analysis. 2nd ed. Basel: Springer International Publishing 2016. doi:10.1007/978-3-319-24277-4.
- Stroop R, Strickmann B, Horstkötter H, Kuhlbusch T, Hartweg H-R, Kerner T. Smartphone-basierte first-responder-Alarmierung „Mobile Retter. Notarzt. 2015;31(5):239–45. doi:10.1055/s-0035-1552700.
- Stroop R, Hensel M, Kerner T. Smartphone-basierte Ersthelferalarmierung – Auswertung der Alarmierungsdaten aus 7 Mobile-Retter-Regionen. Der Notarzt. 2020;36(06):324–32. doi:10.1055/a-1224-4103.
- Oving I, Masterson S, Tjelmeland IBM, Jonsson M, Semeraro F, Ringh M, Truhlar A, Cimpoesu D, Folke F, Beesems SG, ESCAPE-NET Investigators, et al. First-response treatment after out-of-hospital cardiac arrest: a survey of current practices across 29 countries in Europe. Scandinavian Journal of Trauma. Scand J Trauma Resusc Emerg Med. 2019;27(1):112 doi:10.1186/s13049-019-0689-0.
- Caputo ML, Muschietti S, Burkart R, Benvenuti C, Conte G, Regoli F, Mauri R, Klersy C, Moccetti T, Auricchio A, et al. Lay persons alerted by mobile application system initiate earlier cardio-pulmonary resuscitation: a comparison with SMS-based system notification. Resuscitation. 2017;114:73–8. doi:10.1016/j.resuscitation.2017.03.003.
- Blackwood J, Mancera M, Bavery S, Carbon C, Daya M, VanKeulen B, Alteneder DN, Helm J, Robertson J, Charbonneau J, et al. Improving response to out-of-hospital cardiac arrest: the verified responder program pilot. Resuscitation. 2020;154:1–6. doi:10.1016/j.resuscitation.2020.06.015.
- Berglund E, Claesson A, Nordberg P, Djärv T, Lundgren P, Folke F, Forsberg S, Riva G, Ringh M. A smartphone application for dispatch of lay responders to out-of-hospital cardiac arrests. Resuscitation. 2018;126:160–5. doi:10.1016/j.resuscitation.2018.01.039.
- Henriksen FL, Schorling P, Hansen B, Schakow H, Larsen ML. FirstAED emergency dispatch, global positioning of community first responders with distinct roles – a solution to reduce the response times and ensuring an AED to early defibrillation in the rural area Langeland. IJNVO. 2016;16(1):86. doi:10.1504/IJNVO.2016.075131.
- Auricchio A, Gianquintieri L, Burkart R, Benvenuti C, Muschietti S, Peluso S, Mira A, Moccetti T, Caputo ML. Real-life time and distance covered by lay first responders alerted by means of smartphone-application: implications for early initiation of cardiopulmonary resuscitation and access to automatic external defibrillators. Resuscitation. 2019;141:182–7. doi:10.1016/j.resuscitation.2019.05.023.
- Stroop R, Kerner T, Strickmann B, Hensel M. Mobile phone-based alerting of CPR-trained volunteers simultaneously with the ambulance can reduce the resuscitation-free interval and improve outcome after out-of-hospital cardiac arrest: A German, population-based cohort study. Resuscitation. 2020;147:57–64. doi:10.1016/j.resuscitation.2019.12.012.
- Cummins RO, Chamberlain DA, Abramson NS, Allen M, Baskett PJ, Becker L, Bossaert L, Delooz HH, Dick WF, Eisenberg MS, et al. Recommended guidelines for uniform reporting of data from out-of-hospital cardiac arrest: the Utstein Style. A statement for health professionals from a task force of the American Heart Association, the European Resuscitation Council, the Heart and Stroke Foundation of Canada, and the Australian Resuscitation Council. Circulation. 1991;84(2):960–75. doi:10.1161/01.CIR.84.2.960.
- Perkins GD, Jacobs IG, Nadkarni VM, Berg RA, Bhanji F, Biarent D, Bossaert LL, Brett SJ, Chamberlain D, de Caen AR, et al. Cardiac arrest and cardiopulmonary resuscitation outcome reports: update of the Utstein resuscitation registry templates for out-of-hospital cardiac arrest: a statement for healthcare professionals from a task force of the International Liaison Committee on Resuscitation (American Heart Association, European Resuscitation Council, Australian and New Zealand Council on Resuscitation, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Southern Africa, Resuscitation Council of Asia); and the American Heart Association Emergency Cardiovascular Care Committee and the Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation. Circulation. 2015;132(13):1286–300. doi:10.1161/CIR.0000000000000144.
- Silva MA. Advanced mobile location. EENA. [cited 2021 Sept 14]. Available from:https://eena.org/our-work/eena-special-focus/advanced-mobile-location/.