
ABSTRACT
Early caries detection is essential for minimal intervention dentistry, since it could give the opportunity to reverse the process and eliminate or at least postpone the surgical treatment. The aim of the present study was to evaluate the effectiveness of near-infrared transillumination in early caries diagnosis for both occlusal and proximal lesions. Thirty-eight adult patients were included in the study. The results from the visual, radiological and near-infrared transillumination examination for proximal caries lesions were compared. The diagnostic abilities of these methods for occlusal lesions were assayed on 60 teeth. The three methods showed a very high level of correlation when there were caries lesions involving the enamel and dentin. Concerning proximal caries involving only the enamel, the visual--tactile diagnosis proved to be insufficiently sensitive even with the use of magnification. Radiographic examination and near-infrared transillumination correlated significantly, but the latter was more sensitive. Radiographic examination proved to be insufficiently sensitive for occlusal lesions. The results obtained with the near-infrared fluorescence correlated most with the visual–tactile examination. These results suggest that near-infrared transillumination is an effective method for diagnosis of lesions both involving only the enamel and involving the enamel and dentin. It could be used for both occlusal and proximal caries lesions and it could eventually substitute radiographic bitewings, especially in children and pregnant women, due to its efficiency as a diagnostic tool and the absence of radiation.
Introduction
The concept of dental caries has changed significantly over the last decade. While the only way of managing caries used to be the complete removal of the demineralized tissues, today, caries is considered a dynamic process which, if diagnosed in time, could be reversed [Citation1]. This became the basis of the minimal intervention concept in dentistry. It comprises five main concepts: (1) early detection of caries, if possible, at the stage when the lesion is still non-cavitated; (2) remineralization of these early lesions and reduction of the cariogenic bacteria present in the mouth; (3) minimal surgical intervention if a cavitated lesion is present (including the use of hand instruments, air abrasion, sonic devices, ozone, chemomechanical and fluorescence-aided caries excavation use of specially designed burs, and modifications of cavity preparations); (4) use of adhesive restorative materials; and (5) preference of repairing instead of replacing restorations if needed [Citation2,Citation3]
Early caries detection is essential for minimal intervention dentistry because it could give the opportunity to reverse the process and eliminate or at least postpone the surgical treatment. The ideal caries detection device should be able to detect the caries from the earliest stages, when the organic matrix is still not damaged, to the latest stages of cavitated lesion [Citation1]. There are a number of different methods for caries detection. The oldest method is the visual–tactile one (using a probe and a dental mirror). It remains the first step in detecting the presence or absence of caries [Citation4]. However, this method is not sensitive enough, especially for early lesions and those affecting the proximal tooth surfaces. Bitewing radiographs have also been used for a long time for the detection of proximal lesions, but they are not reliable for occlusal defects, especially when only the enamel is involved [Citation5].
Another widely used method for caries diagnosis is fibre-optic transillumination (FOTI) [Citation6,Citation7]. The device could be applied for both occlusal and proximal lesions and is non-invasive and cost-effective, but there is controversial data concerning its sensitivity compared with radiography and probing [Citation8].
Digital imaging fibre-optic transillumination (DIFOTI) is the digitized version of FOTI. It could be applied for the detection of advanced and incipient lesions, fractures, cracks and secondary caries lesions, but it is not useful for determination of the depth of penetration of the caries process [Citation6]. For example, the new DIAGNOcam (KaVo, Biberah, Germany) DIFOTI device uses wavelength in the invisible near-infrared light (780 nm) for the transillumination. The light here is transmitted through the alveolar process, which makes the diagnostic image considerably better [Citation9].
Quantitative light-induced fluorescence is a technology that was introduced long ago. It uses the autofluorescence of dental tissues, which diminishes with demineralization. Quite a lot of studies have used this method for the diagnosis of occlusal and smooth surfaces caries, demineralization and remineralization monitoring [Citation10–13]. This method has high sensitivity but it cannot distinguish between caries, development anomalies, and stain and calculus [Citation8]. A new device that uses this principle is Sopro-Life [Citation14].
Laser-induced fluorescence is used for detection of demineralization and remineralization and occlusal caries lesions [Citation15]. The latest version of the diagnostic device DIAGNOdent (KaVo) could be used for proximal surfaces, too. This method shows higher sensitivity compared to conventional ones, but its specificity is lower [Citation10,Citation16].
Other devices used for early caries diagnosis are electrical caries monitor, Midwest Caries I.D.™, polarization-sensitive optical coherence tomograph, CarieScan, frequency-domain infrared photothermal radiometer, and devices based on modulated luminescence, cone-beam computed tomography, etc. [Citation8].
The aim of the present study was to evaluate the effectiveness of near-infrared transillumination in early caries diagnosis for both occlusal and proximal lesions.
Subjects and methods
Thirty-eight adult patients were included in the study. Examination was performed with a mirror and a dental explorer, under 6.4-fold magnification using a Leica M320 dental microscope (Leica Microsystems GmbH, Wetzlar, Germany). Then DIAGNOcam (KaVo) was used as a diagnostic tool. All patients were administered bitewings. When a lesion involving the enamel and dentin was diagnosed, the caries was excavated. This was used as a way to confirm the validity of the diagnosis based on the visual, radiological and near-infrared transillumination. Enamel lesions were not confirmed operatively, because, according to the minimal intervention concept, these lesions should be treated non-operatively.
Three independent authors performed the study for the effectiveness of the near-infrared transillumination in early diagnosis of occlusal caries lesions on 60 teeth. The presence/absence of lesions was also diagnosed with the visual–tactile method under 6.4-fold magnification for this group as well. The teeth were photographed with DIAGNOcam and the authors evaluated them. X-rays were administered and the examiners viewed them separately, without magnification. As an additional diagnostic method, a laser-induced fluorescence device, DIAGNOdent (KaVo), was used. This device emits red laser light (λ = 655 nm), which reacts with protoporphyrin IX and other products of the metabolism of bacteria with similar chemical structure.
Pearson's correlation coefficients were determined using SPSS 16.0 package for Windows (SPSS Inc., Chicago, USA)
Results and discussion
Early and accurate diagnosis is of significant importance for the choice of the most appropriate treatment strategy. In respect of the new paradigm of minimally invasive dentistry, this will allow caries lesions to be treated at an early stage non-operatively, thus preserving tooth tissues. Accurate diagnosis of occlusal caries lesions is still regarded as difficult. The most largely applied methods, visual (even under magnification) and tactile, are not sensitive enough. Visual examination relies on the changes in the opacity and discolouration of the fissures. It is a highly subjective method. This needs a significant experience and, even so, the sensitivity of the method varies from 0.30 to 0.80 and its specificity from 0.70 to 0.90 [Citation13,Citation17,Citation18]. The combination of a visual and a tactile examination leads to more accurate diagnosis, but again the practitioner could be misled: on the one hand, the ‘sticking’ of the dental explorer could be due to anatomic structures and, on the other hand, the probe might not ‘stick’ when the so-called ‘hidden caries’ or fluoride syndrome is present.
In our study, we diagnosed 125 non-cavitated proximal lesions in the examined patients. The results obtained by the three methods used in this study (visual–tactile, radiographic and near-infrared transillumination) were similar for lesions involving both the enamel and the dentin. Our results showed that the visual–tactile method failed to determine the presence of occlusal caries lesion in 3.4% of the cases, so the condition of the patient was underestimated. Concerning the application of the visual–tactile method for proximal lesions, it is generally accepted that it could lead to false negative results, especially when the process involves only the enamel [Citation19,Citation20]. In the diagnosis of non-cavitated proximal lesions, our results correspond to other reports: the radiographic method is accurate when the dentin is involved, but often leads to underestimation when only the enamel is affected, although it gives better results than the visual–tactile method [Citation21,Citation22].
The results from the diagnosis of occlusal lesions with near-infrared fluorescence in our study correlated most with those from the visual–tactile examination (r = 0.508). Laser-induced fluorescence gave close results, but the radiographic examination failed to diagnose 17.2% of the occlusal caries lesions. Other studies confirm that, when applied to occlusal lesions, the X-ray examination could lead to underestimation of both the number and the size of the affected areas [Citation18,Citation23], due to the superimposition of the enamel. It has been found that occlusal surface tissues are demineralized beyond the middle third of the dentin when the lesion could be diagnosed radiographically [Citation5,Citation24]. Radiography was reliable only for the large ones with significant dentinal involvement. We also studied the effectiveness of laser fluorescence for occlusal caries diagnosis and compared it with DIAGNOcam. The data obtained with the laser-induced fluorescence correlated with that obtained with both visual–tactile and near-infrared transillumination.
The three methods used in this study showed very high level of correlation when caries lesions involving the enamel and the dentin were present. Only 6.4% of the cases with such lesions were not diagnosed with the visual–tactile examination. The operative treatment confirmed the reliability of both radiographic and near-infrared transillumination as diagnostic tools for proximal caries lesions involving both the enamel and the dentin: no overestimation was found.
Significant discrepancies were observed when carries affected only the enamel (). In the present study, 38% (n = 47) of the diagnosed proximal caries were only in the enamel. Concerning that type of caries lesions, the visual–tactile diagnosis proved to be insufficiently sensitive even with the use of magnification: only 11 caries lesions (23.4%) were diagnosed. Forty-one caries lesions were diagnosed in the same patients when bitewings were checked. Forty-seven caries lesions were diagnosed with DIAGNOcam ( and ). Thus, the results obtained using near-infrared transillumination were close to those in the X-ray examination (r = 0.910), but differed significantly from those diagnosed visually (r = 0.446). For this type of lesions, validation of the results with operative excavation was not performed because it is accepted that they could eventually be treated conservatively [Citation25]. Three of the six more lesions observed with the near-infrared transillumination were confirmed during the operative treatment of neighbouring caries. This supports the preliminary hypothesis of higher sensitivity of this new method for early caries diagnosis. The first studies on near-infrared transillumination were performed with devices emitting light with wavelength of λ = 1310 nm [Citation26,Citation27]. There are just a few studies on the effectiveness of DIAGNOcam as a diagnostic tool [Citation9,Citation28–30]. Our results support the evidence shown in all these reports that near-infrared transillumination could be used for early diagnosis of both occlusal and proximal lesions.
Table 1. Statistical correlation between the results obtained with different diagnostic methods.
Figure 1. Caries lesion involving the enamel on teeth 24 and 25 visualized using near-infrared transillumination and X-rays.
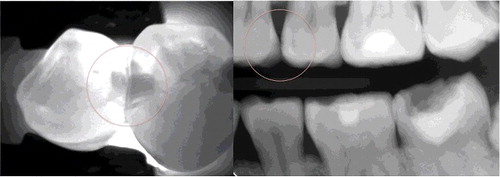
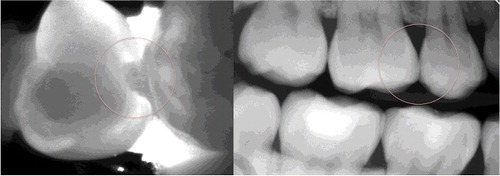
Figure 2. Caries lesion involving the enamel on tooth 15 visualized using near-infrared transillumination and X-rays.
In a review of the data presented in the literature, Rickets [Citation31] noted that DIAGNOdent demonstrated greater sensitivity but poorer specificity compared with visual caries diagnosis. False positive results were measured. Other authors obtained similar results, too [Citation16,Citation17,Citation19,Citation20]. Based on these and our study, we could recommend the device to be used as an adjunct method. Only the radiographic examination did not correlate with DIAGNOdent results. It could be speculated that this is due to the fact that X-rays could give false negative results if the lesion is not advanced enough, while DIAGNOdent is more likely to give false positive readings.
Conclusions
Based on the data obtained from our study, we suggest that near-infrared transillumination is an effective method for the diagnosis of lesions both involving only the enamel and involving the enamel and dentin. When proximal lesions involving only the enamel are concerned, its sensitivity is as high as that of a radiographic examination and better than that of visual--tactile examination. It is as effective for occlusal lesions as laser fluorescence and visual examination under magnification, and is more sensitive than an X-ray examination. It could eventually substitute radiographic bitewings, especially in children and pregnant women, due to its efficiency as a diagnostic tool and the absence of radiation.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Dalli M , Çolac H , Hamidi MM . Minimal intervention concept: a new paradigm for operative dentistry. J Invest Clin Dent. 2012;3(3):167–175.
- Frencken JE , Peters MS , Manton DJ , et al. Minimal intervention dentistry (MID) for managing dental caries – a review. Int Dent J. 2012;62:223–243.
- Dwivedi S , Dwivedi CD , Baranwal HC . Minimal intervention dentistry – current concept and future strategies. Guident. 2013;6(6):26–30.
- Neuhaus KW , Ellwood R , Lussi A , et al. Traditional lesion detection aids. Monogr Oral Sci. 2009;21:42–51.
- Angnes V , Angnes B , Batisttella M , et al. Clinical effectiveness of laser fluorescence, visual inspection and radiography in the detection of occlusal caries. Caries Res. 2005;39:490–495.
- Young DA , Featherstone JD . Digital imaging fiber-optic trans-illumination, F-speed radiographic film and depth of approximal lesions. J Am Dent Assoc. 2005;136(12):1682–1687.
- Young DA . New caries detection technologies and modern caries management: merging the strategies. Gen Dent. 2002;50(4):320–331.
- Amaechi BT . Emerging technologies for diagnosis of dental caries: the road so far. J Appl Phys. [ Internet]. 2009 [ cited 2016 Jul 31];105(10):102047. Available from: http://scitation.aip.org/content/aip/journal/jap/105/10/10.1063/1.3116632
- Sochtig F , Hichel R , Kuchnich K . Caries detection and diagnostics with near-infrared transillumination: clinical experiences. Quint Int. 2014;45:531–538.
- Pretty IA , Ellwood RP . The caries continuum: opportunities to detect, treat and monitor the re-mineralization of early caries lesions. J Dent. 2013;41(Suppl. 2):S12–21.
- Ando M , van der Veen MH , Shemehorn BR , et al. Comparative study to quantify demineralized enamel in deciduous and permanent teeth using laser- and light-induced fluorescence techniques. Caries Res. 2001;35:464–470.
- Pretty IA , Ingram GS , Agalamanyi EA , et al. The use of fluorescein-enhanced quantitative light-induced fluorescence to monitor de- and re-mineralization of in vitro root caries. J Oral Rehabil. 2003;30:1151–1157.
- Pereira AC , Eggertsson H , Gonzalez-Cabezas C , et al. Quantitative light-induced fluorescence (QLF) in relation to other technologies and conventional methods for detecting occlusal caries in permanent teeth. Braz J Oral Sci. 2011;10:27–32.
- Rehmann P , Rechman BMT , Featherstone JDD . Caries detection using light-based diagnostic tools. Compendium. 2012;33:582–593.
- Tam LE , McComb D . Diagnosis of occlusal caries: part II. Recent diagnostic technologies. J Can Dent Assoc. 2001;67(8):459–463.
- Karlsson L . Caries detection methods based on changes in optical properties between healthy and carious tissue. Int J Dent. [ Internet]. 2010 [ cited 2016 Jul 31];2010:270729. Available from: http://www.hindawi.com/journals/ijd/2010/270729/
- Mestriner SF , Vinha D , Mestriner W Jr. Comparison of different methods for the occlusal dentine caries diagnosis. J Appl Oral Sci. 2005;13(1):28–34.
- Mc Comb D , Tam LE . Diagnosis of occlusal caries: part I. Conventional methods. J Can Dent Assoc. 2001;67(8):454–457.
- Bader JD , Shugars DA , Bonito AJ . Systematic reviews of selected dental caries diagnostic and management methods. J Dent Edu. 2001;65(10):960–968.
- Gomez J , Tellez M , Pretty IA , et al. Non-cavitated carious lesions detection methods: a systematic review. Commun Dent Oral Epidemiol. 2013;41:55–73.
- Astvaldsdottir A , Ahlund K , Holbrook WP , et al. Approximal caries detection by DIFOTI: in vitro comparison of diagnostic accuracy/efficacy with film and digital radiography. Int J Dent. [ Internet]. 2012 [ cited 2016 Jul 31]; 2012:326401. Available from: http://www.hindawi.com/journals/ijd/2012/326401/
- Vaarkamp J , ten Bosch JJ , Verdonschot EH , et al. The real performance of bitewing radiography and fiber-optic transillumination in approximal caries diagnosis. J Dent Res. 2000;79:1747–1751.
- Kudiyirickal MG , R Ivančaková . Early enamel lesion. Part I. Classification and detection. Acta Medica. 2008;51(3):145–149.
- Rickets DN , Whaites EJ , Kidd EA , et al. Clinical and radiographic diagnosis of occlusal caries: a study in vitro . J Oral Rehabil. 1995;22:15–20.
- Pitts NB . Are we ready to move from operative to non-operative/preventive treatment of dental caries in clinical practice? Caries Res. 2004;38(3):294–304.
- Maia AMA , Karlson L , Margulis W , et al. Evaluation of two imaging techniques: near-infrared transillumination and dental radiographs for the detection of early approximal enamel caries. Dent Maxill Radiol. 2011;40:429–433.
- Simon JC , Lucas SA , Lee RC , et al. Near-infrared imaging of secondary caries lesions around composite restorations at wavelengths from 1300–1700 nm. Dent Mater. 2016;32:587–595.
- Kachilia P . Caries detection using near-infrared transillumination. Adding objectivity to diagnosis to save tooth structure. Dent Today. 2015;34(5):86–88.
- Abdelaziz M , Krejci J . DIAGNOcam – a near-infrared digital imaging transillumination (NIDIT) technology. Int J Esthet Dent. 2015;10(1):158–165.
- Kühnisch J , Söchtig F , Pitchika V , et al. In vivo validation of near-infrared transillumination for interproximal dentin caries detection. Clin Oral Invest. 2016;20:821–829.
- Ricketts D . The eyes have it. How good is DIAGNOdent at detecting caries? Evid Based Dent. 2005;6(3):64–65.