
Abstract
Objective: This paper seeks to document changes in the effect of educational attainment on cognitive function of older adults in Mexico, and measure gender differences using data from two time periods.
Methods: The data come from the Mexican Health and Aging Study (MHAS), taking the cross-sections of adults aged 60 years or older interviewed in 2001 and 2012. We perform an OLS regression using standardized z-scores for five individual cognitive domains and for total cognition.
Results: Total cognitive scores and educational attainment were higher for men than women in both years. When cognitive components were analyzed separately, women had higher verbal memory and verbal recall scores than men. The gender gap in overall cognition score was smaller in 2012 compared to 2001, while the gender gap in educational attainment was larger in 2012 than in 2001. Even though men had higher educational attainment than women, the effect of educational attainment on cognition was higher for women. Similarly, the difference between total scores for each task for men compared to women decreased between 2012 and 2001, except for verbal learning and verbal recall where the gender difference widened.
Conclusions: If younger cohorts of women continue to progressively achieve higher levels of education, the gender gap in old-age cognition should close. Additional work should determine the mechanisms through which added formal education seems to translate into higher cognitive gains for women compared to men.
Introduction
Cognitive function represents an important health dimension for researchers on aging because it significantly affects independence and quality of life among older adults (Langa et al., Citation2009) and has a significant impact on their caregivers and families. Studies have shown that old age and socioeconomic variables account for more than 20.0% of the variance in cognitive test scores (Zelinski, Gilewski, & Schaie, Citation1993). Education is a major factor in cognitive function (Lee, Kawachi, Berkman, & Grodstein, Citation2003; Matallana et al., Citation2011) with profound gender differences (Lei, Hu, McArdle, Smith, & Zhao, Citation2012; Maurer, Citation2011). More years of formal education have also been shown to protect against cognitive decline (Amieva et al., Citation2014).
However, those with more education may have a more rapid decline in cognitive function (Scarmeas, Albert, Manly, & Stern, Citation2006; Wilson et al., Citation2004) but the relationship between education and rates of cognitive decline among cognitively intact older adults remains unclear (Alley, Suthers, & Crimmins, Citation2007). Therefore, we need additional studies to better understand the relationship between educational attainment and cognitive function (Kalaria et al., Citation2008).
In developing countries like Mexico, older adults have experienced poor institutional support and weak economic conditions over the life course. These conditions result in low overall educational attainment and bad health conditions, increasing the risk of diminished cognitive function in old age (Comijs, Dik, Deeg, & Jonker, Citation2004; Maurer, Citation2011). In addition, Mexico is a country with significant regional differences that include different rates of economic development spanning from the wealthier northern region where the manufacturing industry is dominant, to the service-based central region benefitting from Mexico City’s economic reach, to the modest north-central region that provides a small contribution to Mexico’s economy thanks to an agriculture-based system, and the energy-producing southern region mired by poverty (Cañas & Gutierrez, Citation2015).
Economic development is occurring along with urbanization, shifting the population concentration into urban areas (Smith & Goldman, Citation2007). Nevertheless, low levels of economic development, weak infrastructure, and lack of resources to support the needs of a fast-growing older adult population affect a large number of people. Mexico is currently in a mixed regime in which infectious diseases are still prevalent in some groups of the population alongside chronic and degenerative diseases (Samper-Ternent, Michaels-Obregón, Wong, & Palloni, Citation2012; Wong & Palloni, Citation2009). Current care for older adults with health problems remains inadequate in many regions. Around 30 percent of those aged 60 or older are not covered by any type of health insurance and 35 percent of the elderly population live in poverty (Instituto Nacional de Estadística y Geografía, Citation2010).
Mexico, like other Latin American countries, has seen major gains in educational achievement. An increase in investment in public education began around 1920 but it was interrupted by the Great Depression in the 1930s. The investment growth resumed later that decade when expenditures on education reached its peak (Kehoe & Meza, Citation2011). Finally, in the 1950s, the increase in urbanization led to more investments in public education, increasing the literacy levels among the population aged 5 or older to nearly 70% (Solís-Manjarrez, Citation2000). Between 1970 and 2010, the percentage of the population with no education decreased from 32% to 7%. Among women, the decrease went from 35% in 1970 to 8% in 2010 (Instituto Nacional de Estadística y Geografía, Citation2011). This remarkable change raises questions about the effect these gains in educational attainment will bring to future generations of older adults and their rates of cognitive decline.
There are two major theories about the relationship between education and cognition. First, the cognitive reserve theory states that more educational attainment increases cognitive reserve and therefore reduces or slows down cognitive decline with advanced age. And second, the compensation theory states that more educational attainment allows more cognitive domains to fully develop and, once diseases affect cognitive function, the domains not affected compensate for declines in the compromised domains (Zahodne et al., Citation2011). Previous studies in Mexico have analyzed the effect of educational attainment on cognition. Ardila, Ostrosky-Solis, Rosselli, and Gómez (Citation2000) examined a sample of 806 individuals aged 16-85 between 1993-1996 who were administered a neuropsychological evaluation. Test scores were strongly associated to educational attainment and an interaction between educational attainment and age was reported. Authors propose that there are different patterns of cognitive decline and that the percentage of variance explained by educational attainment varies by cognitive test.
Recent data has shown that education is more than simply the number of years of schooling. Research has found that the quality of education during childhood can affect cognitive function during late life, especially among those with less than 12 years of schooling (Crowe et al., Citation2013). However, research also questions whether we can accurately measure cognitive function in low-income, low-literacy societies with the tools currently available (Langa et al., Citation2009). Despite this discussion, other studies in Latin America and the Caribbean provide additional support to the direct relationship between educational attainment and cognitive function. Some studies use models that include a life-course approach and suggest education is a pathway linking early-life educational attainment to cognitive function at older ages (Maurer, Citation2010; Nitrini et al., Citation2009). Other studies address gender inequality and suggest gender differences in cognitive function in the region are explained by differences in educational attainment (Maurer, Citation2011).
Recent studies suggest that the prevalence rates of dementia around the world are remaining stable and in some countries declining, despite epidemiological evidence and projections that suggest otherwise (Wu et al., Citation2017). These studies only include developed countries and no Latin American countries are represented. However, one of the potential explanations for this decline in those countries are better living conditions, more education and health care, which are identified as potential factors behind this change in prevalence. Our study contributes to these gaps in the literature by analyzing the relationship between educational attainment and cognitive function in Mexico, a country in the midst of an epidemiological transition, using two national samples of adults separated by slightly over a decade (Wong & Palloni, Citation2009).
Thus, given the close relationship between education and cognition, and the rapid changes in educational attainment that have occurred in developing countries, we seek to narrow the knowledge gap in this area by answering the following questions: Given the significant increase in years of educational attainment in Mexico, are there differences in cognitive function between cohorts of older adults with significantly different education levels? Have the fast gains in educational achievement, in particular among women, resulted in higher cognitive scores such that the gender gap in cognition closed appreciably?
We postulate the hypothesis that, given the important increase in educational attainment among older adults over time, cognitive scores have increased for both genders. We also hypothesize that, as successive generations of Mexican older adults have achieved higher levels of education, the gender gap in cognitive function will close due to the observed higher gains in education for women. To test these hypotheses, we use two national cross-sections of data on older adults (aged 50 and older) in Mexico with the following goals: a) to document the gender differences in education and in cognitive status among older adults in 2001 and 2012 and b) to examine the gender differences in the association between education and cognition and how these differ between 2001 and 2012. Because there are well-established gender differences across cognitive domains (Lei et al., Citation2012), and since educational achievement may affect each component of our cognitive assessment differently for men and women, we will examine cognition assessments using total scores as well as by cognitive domains.
Data and methods
Sample
Data come from the Mexican Health and Aging Study (MHAS), a nationally representative panel investigation of health and aging in Mexicans aged 50 years or older (Wong, Michaels-Obregón, & Palloni, Citation2017). The 2001 survey completed 15,186 in-person interviews with individuals aged 50 and older, with a 92% response rate (Mexican Health & Aging Study, Citation2001) conducted by the Instituto Nacional de Estadística y Geografía (INEGI, or the National Institute of Statistics and Geography). Follow-ups were made in 2003 and in 2012, with an 88% response rate,(Mexican Health & Aging Study, Citation2012). The sample in 2012 was refreshed with the inclusion of new respondents (n = 6,259) to once again conform a nationally representative sample of older adults aged 50 an older (Instituto Nacional de Estadística y Geografía, Citation2013).
For the purpose of this paper, we use data from the two waves, 2001 and 2012 of the MHAS. These two waves are considered representative cross-sections of the population aged 50 and older in each of the two years. For descriptive analyses, we further divided the samples by age (60-69 years and 70 years or older) to capture the pattern of cognitive decline with old age.
For the 2001 cross-section, we begin with 7,171 respondents aged 60 or older. For descriptive analyses, we exclude 1,850 respondents who had incomplete cognitive battery (1,257) or answered through a proxy (593). For the main statistical analysis, we further exclude 284 respondents who had missing covariates, leaving a sample of 5,037 respondents. Compared to this sample, the excluded respondents in 2001 are older individuals, are predominantly men, have low-educational attainment, and have a higher prevalence of stroke. For the 2012 cross-section, we begin with a pool of 10,170 respondents aged 60 or older. For descriptive analyses, we exclude 2,392 respondents who had incomplete cognition battery (1,372) or answered through a proxy (1,020). For the main statistical analysis, we further exclude 128 respondents with missing covariates, leaving a sample of 7,650 respondents. Compared to this sample, the excluded respondents are slightly older, predominantly men, low-educated, and have a higher prevalence of diabetes.
Statistical analysis
We aim to analyze the effect of educational attainment on cognitive scores for respondents aged 60 years or older in both cross-sections and compare the gender differences. We use Ordinary Least Squares (OLS) to measure the effect of educational attainment and other sociodemographic and health variables on the total cognition score. Our samples are not independent as respondents from 2001 could be present in the 2012 cross-section if they survived. We include bootstrapped standard errors as a way of reducing the risk of violating any statistical assumption. Respondents were included in the regression if they were aged 60 or older in 2001 and 2012 respectively, and if they answered a complete cognitive battery without any assistance. We present the results for the total cognition score and the five cognitive domains that make up the total score expressed as standardized z-scores, since the conversion to a common metric facilitates the comparison across measures, the translation of raw scores, and the interpretation of results (Mejía-Arango, Wong, & Michaels-Obregón, Citation2015). The analyses were conducted using Stata/SE version 14.2 (StataCorp, Citation2015).
Measures
Cognitive function was assessed using the screening portion of the Cross-Cultural Cognitive Examination (CCCE) (Glosser et al., Citation1993). The CCCE was developed as a short and sensitive tool for dementia diagnosis in the community. It consists of two portions: an initial screening portion and a more complex diagnosis portion. All tasks included in the CCCE are accepted as cognitive function indicators and the effect of education and literacy is supposed to be small (Glosser et al., Citation1993). The MHAS has used the screening portion of the CCCE since the first wave in 2001. The scale has been previously used to study congnitive function in Mexico by other researchers (Al Hazzouri, Haan, Galea, & Aiello, Citation2011; Downer, Veeranki, & Wong, Citation2016; Mejía-Arango et al., Citation2015).
We use five tasks measuring four cognitive domains in 2001 and in 2012: visuospatial ability, visuospatial recall, verbal learning, verbal recall, and visual scanning. In 2001, visuospatial ability was measured by presenting two geometrical figures and asking respondents to copy the figures within 90 seconds. In 2012, the task was changed by presenting only one figure and the scoring system was modified to make scores comparable across waves. Visuospatial recall was measured by asking respondents to remember the figure(s) they copied and draw them on a blank piece of paper; three minutes were allocated to complete this task. Verbal learning was measured by asking respondents to listen to a list of eight words and then repeat them. This task was performed three times and the average score of these trials was calculated. For verbal recall, performed after the visuospatial memory task, respondents were asked to repeat all the words they could remember from the previous list of words. Finally, visual scanning was measured by asking respondents to circle all figures identical to a given model in a disorganized display in a given amount of time.
Scores for visuospatial ability and visuospatial memory ranged from 0-2 for each task, the score for verbal learning and verbal recall ranged 0-8 each, and the score for visual scanning ranged 0-60. The total cognitive score ranged 0-80 but, in the 2012 survey, the scores of two tasks were modified. For visuospatial ability and visuospatial memory, the range changed to 0-6 each with the remaining dimensions being unchanged. Hence, the total score increased from a maximum of 80 points to a maximum of 88 points. Following methodology by Michaels-Obregón, Mejía-Arango, and Wong (Citation2014), the visuospatial ability and visuospatial memory scores were adjusted so that scores for both years ranged from 0 to 80.
Independent variables
Age: continuous variable measuring the respondent’s age. For descriptive analyses, we grouped respondents in two age categories (60-69 years and 70 years or older). Educational attainment: continuous variable measuring the number of years of formal schooling. For descriptive analyses, we included educational attainment in four categories (no years of education, one to five years, six years, and seven or more years) given the data distribution and characteristics of the educational system in Mexico. In the regression analysis, we include continuous years of education and years of education squared to allow for a non-linear relationship between education and cognition (Mendel, Murphy, Miller, Martin, & Karnik, Citation1999). We expect that higher levels of education will result in higher levels of cognition but, at some point, the marginal benefit in the cognition score of adding one more year of education will decline. Gender: dichotomous variable (women =1). Area of Residence: dichotomous variable measuring residence in communities under 100,000 inhabitants (reference category) and those of 100,000 inhabitants or more. We included this variable to take into account the marked socioeconomic differences between urban and rural areas in the country. Health conditions: a discrete variable measuring the total number of self-reported chronic health conditions ranging from zero to five and including hypertension, diabetes, stroke, heart problems, and respiratory problems. We included these five conditions because of their high prevalence and their association with loss of functionality among older adults. Additionally, they have all been shown to be independet risk factors for cognitive decline and dementia. Depressive symptoms: respondents answered an abbreviated version of the Center for Epidemiologic Studies – Depression (CES-D) battery (Radloff, Citation1977) with nine symptoms included in the MHAS. Each symptom was dichotomized and the results added to generate a score (0-9) with three positive items being reverse coded. The MHAS depression battery has been validated in the past (Aguilar-Navarro, Fuentes-Cantú, Ávila-Funes, & García-Mayo, Citation2007) and depression and cognition have been previously linked (Van Den Kommer et al., Citation2013).
Results
shows the sample distribution of years of education by age group and gender for the two cross-sections. Average educational attainment in the 2012 cross-section was higher than the mean educational attainment in the 2001 cross-section. The increases in educational attainment were larger for women compared to men. In 2001, the percentange of women with no education was higher compared to men, with a 5.2% gender difference. By 2012, the gender difference was only 1.0%. Also, the percentage of men with seven or more years of education in 2001 was 22.7% and increased to 38.6% in 2012. For women, the relative increase was larger, with 18.8% having seven or more years of education in 2001 compared to 36.4% in 2012, an 15.9% increase for men versus a 17.6% increase for women. Independent of the year of observation and gender, the younger group of adults (aged 60-69) had a higher level of education compared to the older group (70+).
Table 1. Education Characteristics of Older Mexicans Stratified by Age, Gender, and Cross-Section.
shows the z scores for the total cognitive score and the five cognitive domains, stratified by age group and gender in both cross-sections. The average total raw cognition score was 4.8 points higher in the 2012 cross-section than the average total raw cognition score in the 2001 cross-section. The difference in mean total cognition score between men and women in 2012 was smaller and statistically significant than the difference in mean total cognition score between men and women in 2001.
Table 2. Z-Scores of Total and Task-Specific Cognitive Assessments of Older Mexicans Stratified by Age, Gender, and Cross-Section.
In the 2001 cross-section, cognition scores in adult men aged 60-69 years were 0.5 standard deviations higher than those for adult men aged 70 years or older. This difference was 0.6 standard deviations in the 2012 cross-section. For women, the comparable difference between age groups was 0.6 standard deviations in 2001 and nearly 0.7 standard deviations in 2012. With the exception of verbal learning and verbal recall, z-scores for the other domains were higher among men in both years.
Other results (not shown) indicare that, in terms of the gap between urban and rural areas, both cross-sections showed gender differences. In 2001, urban men had on average 5.1 years of schooling while rural men had only 2.4 years. Similarly, women in urban areas had on average 4.1 years of schooling while women in rural areas had 2.1 years. By 2012, urban men had an average of 6.5 years of schooling while rural men had 3.3 years. For women, these increases were smaller, with urban women having an average of 5.2 years of schooling compared to 2.8 years for rural women.
Similar differences were observed in cognition (results not shown). The average total raw score for urban men increased from 36.8 points in 2001 to 42.1 points in 2012 while scores for rural men were 30.0 and 33.2 points in the same periods. The scores for urban women were also higher in the later cross-section (34.2 in 2001 and 39.9 in 2012) while scores for rural women were 27.6 and 31.7 points, respectively.
Overall, women living in rural areas in 2012 had an average of 0.7 more years of schooling than the average of years of schooling that women living in rural areas had in 2001. However, this increase was associated with a total raw cognition score of 4.1 points higher than the total raw cognition score for the 2001 sample. Similarly for men, in 2012 those living in rural areas had an average of 0.9 more years of schooling than men in the 2001 sample and this increase was associated with an average total cognition score 3.2 points higher than men living in rural areas in 2001.
presents results for OLS regressions of z-scores for the five domains and the total score in each cross-section, controlling for gender, years of education, years of education squared, and an interaction term of gender by educational attainment. The regression models also control (not shown) for age, urban/rural residence, number of chronic conditions, and number of depressive symptoms and we present results for covariates with the largest effects on the z-scores. For both cross-sections, years of education was associated with a significant higher z-score in all domains and in the total cognition score. The regression model also showed significantly higher z-scores for verbal learning and verbal recall among women compared to men in both cross-sections. Looking at the interaction of gender and educational attainment, the results show higher effects of educational attainment for women than men in the total score, visuospatial ability and visual scanning in 2001; a similar result is evident for total score and for all domains except the verbal in 2012.
Table 3. OLS Regression of Z-Scores in Total Cognitive Scores and in the Five Domains of Cognition, 2001 and 2012.
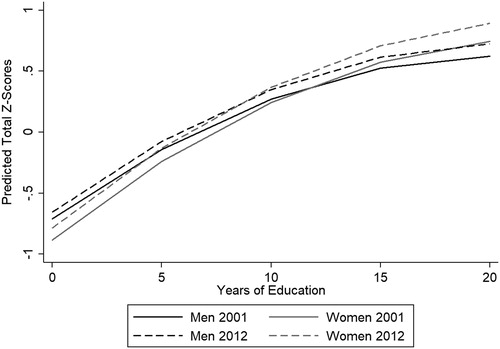
Based on the OLS regression results, shows predicted total cognition scores by years of education, gender, and cross-section. As years of educational attainment increased, the total cognition score increased for both men and women in both 2001 and 2012. A significant difference was observed between the two years. Further, the benefits of educational attainment (i.e., the marginal effect of higher educational achievement) were significantly higher for women compared to men. Women in the 2012 cross-section needed about 9.5 years of educational attainment to reach a similar total cognition score than men. In contrast, women in the 2001 cross-section required about 12.5 years of educational attainment to match male total cognition scores.
Figure 1. Predicted Total Cognition Z-Scores for Older Mexicans by Years of Education, Gender, and Cross-Section. Note: Solid lines correspond to 2001 and dashed lines to 2012. Black corresponds to men and gray to women. Source: Authors’ own elaboration with data for older adults aged 60 years or older from the Mexican Health and Aging Study, Wave 1 (2001) and Wave 3 (Citation2012).
In summary, the cohorts of men and women aged 60 and older exhibited important gains in educational attainment in Mexico between 2001 and 2012. These advances were associated with higher cognitive scores overall. Furthermore, the relative cognitive advantages resulting from more educational attainment were larger for women compared to men, although an advantage for men still remained. When differences by cognitive domains were analyzed, men had advantages in visuospatial ability, visuospatial recall, and visual scanning, while women presented advantages in verbal learning and verbal recall.
Discussion
This paper aimed to contribute to the body of knowledge on cognition in older adults by examining the association of educational attainment and cognition in a rapidly changing developing country, paying particular attention to gender differences across a decade. We used data from a nationally representative sample of older Mexicans to examine gender differences among adults aged 60 years and older in 2001 and 2012. Significant rises in educational achievement of the overall population are evident, especially for women. Nevertheless, gender differences in educational attainment and cognitive scores continue to favor men.
Analysis of the separate cognitive domains showed that women scored higher than men in the verbal domains. These results are consistent with previous literature showing that women have a concrete advantage over men in verbal memory tasks, which might be due to women having a better ability to associate an image with a corresponding word (Kimura & Clarke, Citation2002; Sundermann et al., Citation2016). However, gender differences in cognitive function remain under further scrutiny as many disciplines are beginning to question the reach of these claims. Some establish that there are differences in the way the male and female brain can process several verbal or spatial tasks (Andreano & Cahill, Citation2009), while others find that the way men and women are viewed in society affects several socioeconomic variables (e.g., educational attainment) which in turn, affect cognitive functioning (Linn & Kessel, Citation2003). It is clear that gender differences in cognition are the result of biopsychosocial interactions through the lifecourse (Bonsang, Skirbekk, & Staudinger, Citation2017).
Results from our study support previous literature suggesting that differences in cognitive function between men and women are, at least in part, explained by lower educational attainment among women compared to men.
Data from Mexico and other developing countries in Latin America have confirmed that women are usually at a disadvantage that impacts their health in older adult life (Wong & Palloni, Citation2009). Our results build on this notion and highlight the effect of socioeconomic differences observed between men and women in Mexico. There is data that suggests that improving these socioeconomic disadvantages can impact health in older ages and benefit society as a whole (Al Hazzouri, Sibai, Chaaya, Mahfoud, & Yount, Citation2011). Our findings support these data in the sense that the cognitive benefits of more educational attainment is higher for older Mexican women compared to men, even though both benefit from significant increases in educational attainment.
Our study also supports findings from clinical literature that shows distinctive cognitive profiles for men and women. The idea of “a male and a female brain” has been long debated (Joel et al., Citation2015), and imaging studies and neurocognitive profiles show that older women have advantages in verbal memory compared to men (Sundermann et al., Citation2016). These findings suggest that future studies should analyze cognitive decline by domains and build on this literature so that interventions for men and women with cognitive decline can be tailored with these differences in mind.
Our study has several limitations. First, we used a cognitive tool with only five cognitive tasks to assess cognitive function. These five tasks are important for adequate cognitive function, but they are not the only important cognitive tasks. In fact, after the baseline interview, the MHAS added three new cognition tasks measuring orientation (in 2003), numeracy (in 2012), and semantic verbal fluency (in 2012). These tasks provide additional and important information for the study of cognitive function but also modify the structure of the survey questionnaire. Further, learning certain trades or crafts might change the overall cognitive function of a person. Studies in developing countries could not be found but previous research in the US states that those who have a clerical work and those who only learn a craft have 2.25 times greater risk of developing dementia than those with a professional, managerial or technical occupation (Stern, Citation2012).
Second, verbal recall scores in 2012 were indeed lower than those in 2001; this might be partly because respondents in 2012 had a longer time-lag in which to get to the verbal recall task compared to 2001. Longer delays in-between recalling tasks could produce a serial position effect where respondents who have the task of remembering a list of random words are more capable of identifying the words at the beginning (primacy) and at the end (recency) of the list as short-term memory begins to deteriorate. However, we believe that the impact of these effects do not significantly change the overall cognitive performance of our sample.
Third, the changes to the cognition section of the MHAS in 2012 also included a different design in the visuospatial ability and visuospatial recall tests. In 2001, respondents needed to draw and remember two figures and were graded in a scale of 0-2 depending on completion of the figures. In 2012, the test was re-designed and respondents had to draw and remember just one figure but the score went to a scale of 0-6, measuring whether or not the figure was completed or correctly drawn. Despite adjustments to the 2012 scores to match those in 2001, the modification in the test might have altered the results in 2012 because respondents had to draw only one figure instead of two. Nevertheless, we are confident that, by focusing on gender differences within each cross-section separately, we ameliorated the possible effects of these changes in the cognition instrument.
Finally, this research has been conducted using two separate observations in time of a nationally representative longitudinal study. The use of this data as cross-sections allows us to get distinct ideas of how the relationship between cognitive functioning and educational attainment is observed in 2001 and then in 2012. We did not exploit the longitudinal nature of the data to examine trajectories of cognitive change among older adults, which can be examined in future research.
Also, future research needs to identify factors other than educational attainment that determine cognitive score. In the existing literature on education and cognition, several authors have stated that a significant share of cognitive function is not explained by educational attainment. Life experiences, social factors, overall health status, and nutrition have all been proposed as additional factors that affect cognitive function (see for example, Piccinin et al., Citation2012).
In our current study, we controlled for relevant socioeconomic and health-related variables but further analyses could be conducted incorporating social factors of relevance given the recent socioeconomic changes in Mexico. Aspects such as the individual’s social network (Fratiglioni, Wang, Ericcson, Maytan, & Winblad, Citation2000), the role both men and women play in the workforce and in society in general (Kryspin-Exner, Lamplmayr, & Felnhofer, Citation2011), and life events (Van Den Berg, Deeg, Lindeboom, & Portrait, Citation2010), among others, affect cognitive function and are likely to explain part of the differences observed by gender.
In addition, cross-national comparisons could provide useful information for understanding how education affects cognition in societies at different stages of the socioeconomic and epidemiologic transitions, as well as across cohorts that grow old with vastly different life-cycle experiences.
Finally, our results revealed a significant narrowing of the gender disparity in cognition among older adults over a decade in Mexico. We would expect that, as young cohorts of women have continued to achieve increasingly higher educational attainment, the gender gap in cognition among future cohorts of older adults will continue to close. Future work will be important to determine the mechanisms through which additional formal education translated into larger cognitive gains for women than for men. This knowledge will provide a better understanding of the factors that impact negatively on cognitive function as well as those that promote it, addressing a critical need of the rapidly growing population of older adults in Latin America.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Aguilar-Navarro, S. G., Fuentes-Cantú, A., Ávila-Funes, J. A., & García-Mayo, E. J. (2007). Validez y Confiabilidad del Cuestionario del ENASEM para la Depresión en Adultos Mayores. Salud Pública de México, 49(4), 256–262. doi: http://dx.doi.org/10.1590/S0036-36342007000400005
- Al Hazzouri, A. Z., Haan, M. N., Galea, S., & Aiello, A. E. (2011). Life-course exposure to early socioeconomic environment, education in relation to late-life cognitive function among Older Mexicans and Mexican Americans. Journal of Aging and Health, 23(7), 1027–1049. doi: http://dx.doi.org/10.1177/0898264311421524
- Al Hazzouri, A. Z., Sibai, A. M., Chaaya, M., Mahfoud, Z., & Yount, K. M. (2011). Gender differences in physical disability among older adults in underprivileged communities in Lebanon. Journal of Aging and Health, 23(2), 367–382. doi: http://dx.doi.org/10.1177/0898264310385454
- Alley, D., Suthers, K., & Crimmins, E. (2007). Education and cognitive decline in older Americans: Results from the AHEAD Sample. Research on Aging, 29(1), 73–94. doi: http://dx.doi.org/10.1177/0164027506294245
- Amieva, H., Mokri, H., Goff, M. L., Meillon, C., Jacqim-Gadda, H., Foubert-Samier, A., … Dartigues, J. F. (2014). Compensatory mechanisms in higher-educated subjects with Alzheimer’s Disease: A study of 20 years of cognitive decline. Brain, 137(4), 1167–1175. doi: https://doi.org/10.1093/brain/awu035
- Andreano, J. M., & Cahill, L. (2009). Sex Influences on the neurobiology of learning and memory. Learning & Memory, 16(4), 248–266. doi: http://dx.doi.org/10.1101/lm.918309
- Ardila, A., Ostrosky-Solis, F., Rosselli, M., & Gómez, C. (2000). Age-related cognitive decline during normal aging: The complex effect of education. Archives of Clinical Neuropsychology, 15(6), 495–513. doi: http://dx.doi.org/10.1016/S0887-6177(99)00040-2
- Bonsang, E., Skirbekk, V., & Staudinger, U. M. (2017). As you sow, so shall you reap: Gender-role attitudes and late-life cognition. Psychological Science, 28(9), 1201–1213. doi: http://dx.doi.org/10.1177/0956797617708634
- Cañas, J., & Gutierrez, E. (2015). Mexico's four economies reflect regional differences. Challenges Southwest Economy, (Q3), 10–13.
- Comijs, H. C., Dik, M. G., Deeg, D. J., & Jonker, C. (2004). The course of cognitive decline in older persons: Results from the longitudinal aging study Amsterdam. Dementia and Geriatric Cognitive Disorders, 17(3), 136–142. doi: http://dx.doi.org/10.1159/000076346
- Crowe, M., Clay, O. J., Martin, R. C., Howard, V. J., Wadley, V. G., Sawyer, P., & Allman, R. M. (2013). Indicators of childhood quality of education in relation to cognitive function in older adulthood. The Journals of Gerontology, Series A: Biological Sciences and Medical Sciences, 68(2), 198–204. doi: http://dx.doi.org/10.1093/gerona/gls122
- Downer, B., Veeranki, S. P., & Wong, R. (2016). A late life risk index for severe cognitive impairment in Mexico. Journal of Alzheimer's Disease, 52(1), 191–203. doi: http://doi.org/10.3233/JAD-150702
- Fratiglioni, L., Wang, H. X., Ericcson, K., Maytan, M., & Winblad, B. (2000). Influence of social network on occurrence of dementia: A community-based longitudinal study. Lancet, 355(9212), 1315–1319. doi: http://dx.doi.org/10.1016/S0140-6736(00)02113-9
- Glosser, G., Wolfe, N., Albert, M. L., Lavine, L., Steele, J. C., Calne, D. B., & Schoenberg, B. S. (1993). Cross-cultural cognitive examination: Validation of a dementia screening instrument for neuroepidemiological research. Journal of the American Geriatrics Society, 41(9), 931–939. doi: http://dx.doi.org/10.1111/j.1532-5415.1993.tb06758.x
- Instituto Nacional de Estadística y Geografía. (2010). Censo de Población y Vivienda. Retrieved from http://www.inegi.org.mx/sistemas/olap/Proyectos/bd/censos/cpv2010/PT.asp?s=est&c=27770&proy=cpv10_pt
- Instituto Nacional de Estadística y Geografía. (2011). Características Educativas de la Población: Distribución Porcentual de la Población de 15 y Más Años por Nivel Educativo, Para Cada Sexo, 1960 a 2010. Retrieved from http://www3.inegi.org.mx/sistemas/sisept/Default.aspx?t=medu09&s=est&c=35006
- Instituto Nacional de Estadística y Geografía. (2013). Mexican Health and Aging Study 2012: Sample Design. Aguascalientes, Mex.: INEGI. Available at: http://mhasweb.org/Resources/DOCUMENTS/2012/Methodological_Document_2012-SEC.pdf.
- Joel, D., Berman, Z., Tavor, I., Wexler, N., Gaber, O., Stein, Y., … Assaf, Y. (2015). Sex beyond the genitalia: The human brain mosaic. Proceedings of the National Academy of Sciences of the United States of America, 112(50), 15468–15473. doi: http://dx.doi.org/10.1073/pnas.1509654112
- Kalaria, R. N., Maestre, G. E., Arizaga, R., Friedland, R. P., Galasko, D., Hall, K., … Antuono, P. (2008). Alzheimer's disease and vascular dementia in developing countries: Prevalence, management, and risk factors. The Lancet Neurology, 7(9), 812–826. doi: http://dx.doi.org/10.1016/S1474-4422(08)70169-8
- Kehoe, T. J., & Meza, F. (2011). Catch-up growth followed by stagnation: Mexico, 1950-2010. Latin American Journal of Economics, 48(2), 227–268. doi: http://dx.doi.org/10.4067/S0719-043320110002000006
- Kimura, D., & Clarke, P. G. (2002). Women's advantage on verbal memory is not restricted to concrete words. Psychological Reports, 91, 1137–1142. doi: http://dx.doi.org/10.2466/pr0.2002.91.3f.1137
- Kryspin-Exner, I., Lamplmayr, E., & Felnhofer, A. (2011). Geropsychology: The gender gap in human aging – A mini-review. Gerontology, 57(6), 539–548. doi: http://dx.doi.org/10.1159/000323154
- Langa, K. M., Llewellyn, D. J., Lang, I. A., Weir, D. R., Wallace, R. B., Kabeto, M. U., & Huppert, F. A. (2009). Cognitive health among older adults in the United States and in England. BMC Geriatrics, 9, 23. doi: http://dx.doi.org/10.1186/1471-2318-9-23
- Lee, S., Kawachi, I., Berkman, L. F., & Grodstein, F. (2003). Education, other socioeconomic indicators, and cognitive function. American Journal of Epidemiology, 157(8), 712–720. doi: http://dx.doi.org/10.1093/aje/kwg042
- Lei, X., Hu, Y., McArdle, J. J., Smith, J. P., & Zhao, Y. (2012). Gender differences in cognition among older adults in China. Journal of Human Resources, 47(4), 951–971. doi: http://dx.doi.org/10.1353/jhr.2012.0033
- Linn, M. C., & Kessel, C. (2003). Gender differences in cognition and educational performance. In L. Nadel (Ed.), Encyclopedia of cognitive science (pp. 261–267). New York: MacMillian.
- Matallana, D., de Santacruz, C., Cano, C., Reyes, P., Samper-Ternent, R., Markides, K. S., … Reyes-Ortiz, C. A. (2011). The relationship between education level and mini-mental state examination domains among older Mexican Americans. Journal of Geriatric Psychiatry and Neurology, 24(1), 9–18. doi: http://dx.doi.org/10.1177/0891988710373597
- Maurer, J. (2010). Height, education and later-life cognition in Latin America and the Caribbean. Economics and Human Biology, 8(2), 168–176. doi: http://dx.doi.org/10.1016/j.ehb.2010.05.013
- Maurer, J. (2011). Education and male-female differences in later-life cognition: International Evidence from Latin America and the Caribbean. Demography, 48(3), 915–930. doi: http://dx.doi.org/10.1007/s13524-011-0048-x
- Mejía-Arango, S., Wong, R., & Michaels-Obregón, A. (2015). Normative and standardized data for cognitive measures in the Mexican Health and Aging Study. Salud Pública de México, 57(1), S90–S96.
- Mendel, J., Murphy, S., Miller, L., Martin, M., & Karnik, N. (1999). The Fuzzy logic advisor for social judgments: A first attempt. In L. Zadeh & J. Kacprzyk (Eds.), Computing with words in information/intelligent systems 2 (Vol. 34, pp. 459–483). Heidelberg: Physica-Verlag.
- Mexican Health and Aging Study. (2001). Data Files and Documentation (Public Use): Wave 1. Retrieved from http://www.mhasweb.org
- Mexican Health and Aging Study. (2012). Data Files and Documentation (Public Use): Wave 3. Retrieved from http://www.mhasweb.org
- Michaels-Obregón, A., Mejía-Arango, S., & Wong, R. (2014). The Mexican Health and Aging Study: Cognitive Functioning Measures, Version 3. Retrieved from http://www.mhasweb.org/DiscussionForum/File%20Upload/Documents/Mexican%20Health%20and%20Aging%20Study%20(MHAS)%20-%20Cognition%20Battery%20(version%203).pdf
- Nitrini, R., Bottino, C. M., Albala, C., Custodio-Capuñay, N. S., Ketzoian, C., Llibre-Rodríguez, J. J., … Caramelli, P. (2009). Prevalence of dementia in Latin America: A collaborative study of population-based cohorts. International Psychogeriatrics, 21(4), 622–630. doi: http://dx.doi.org/10.1017/S1041610209009430
- Piccinin, A. M., Muniz-Terrera, G., Clouston, S., Reynolds, C. A., Thorvaldsson, V., Deary, I. J., … Hofer, S. M. (2012). Coordinated analysis of age, sex, and education effects on change in MMSE Scores. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 68(3), 374–390. doi: http://dx.doi.org/10.1093/geronb/gbs077
- Radloff, L. S. (1977). The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Applied Psychological Measurement, 1(3), 385–401. doi: http://dx.doi.org/10.1177/014662167700100306
- Samper-Ternent, R., Michaels-Obregón, A., Wong, R., & Palloni, A. (2012). Older adults under a mixed regime of infectious and chronic diseases. Salud Pública de México, 54(5), 487–495. doi: http://dx.doi.org/10.1590/S0036-36342012000500005
- Scarmeas, N., Albert, S. M., Manly, J. J., & Stern, Y. (2006). Education and rates of cognitive decline in incident Alzheimer's disease. Journal of Neurology, Neurosurgery, and Psychiatry, 77(3), 308–316. doi: http://dx.doi.org/10.1136/jnnp.2005.072306
- Smith, K. V., & Goldman, N. (2007). Socioeconomic differences in health among older adults in Mexico. Social Science & Medicine, 65(7), 1372–1385. doi: http://dx.doi.org/10.1016/j.socscimed.2007.05.023
- Solís-Manjarrez, L. (2000). La Realidad Económica Mexicana: Retrovisión y Perspectivas (3rd ed.). Mexico, D.F.: Fondo de Cultura Económica.
- StataCorp. (2015). Stata Statistical Software: Release 14. College Station, TX: StataCorp LP.
- Stern, Y. (2012). Cognitive reserve in ageing and Alzheimer's Disease. The Lancet Neurology, 11(11), 1006–1012. doi: http://dx.doi.org/10.1016/S1474-4422(12)70191-6
- Sundermann, E. E., Maki, P. M., Rubin, L. H., Lipton, R. B., Landau, S., & Biegon, A. (2016). Female advantage in verbal memory: Evidence of sex-specific cognitive reserve. Neurology, 87(18), 1916–1924. doi: http://dx.doi.org/10.1212/WNL.0000000000003288
- Van Den Berg, G. J., Deeg, D. J. H., Lindeboom, M., & Portrait, F. (2010). The role of early-life conditions in the cognitive decline due to adverse events later in life. The Economic Journal, 120(548), F411–F428. doi: http://dx.doi.org/10.1111/j.1468-0297.2010.02396.x
- Van Den Kommer, T. N., Comijs, H. C., Aartsen, M. J., Huisman, M., Deeg, D. J. H., & Beekman, A. T. F. (2013). Depression and cognition: How do they interrelate in old age? The American Journal of Geriatric Psychiatry, 21(4), 398–410. doi: http:/dx.doi.org/10.1016/j.jagp.2012.12.015
- Wilson, R. S., Li, Y., Aggarwal, N. T., Barnes, L. L., McCann, J. J., Gilley, D. W., & Evans, D. A. (2004). Education and the course of cognitive decline in Alzheimer Disease. Neurology, 63(7), 1198–1202. doi: http://dx.doi.org/10.1212/01.WNL.0000140488.65299.53
- Wong, R., Michaels-Obregón, A., & Palloni, A. (2017). Cohort profile: The Mexican Health and Aging Study (MHAS). International Journal of Epidemiology, 46(2), e2. doi: http://doi.org/10.1093/ije/dyu263
- Wong, R., & Palloni, A. (2009). Aging in Mexico and Latin America. In P. Uhlenberg (Ed.), International handbook of population aging (pp. 231–252). Dordrecht: Springer.
- Wu, Y.-T., Beiser, A. S., Breteler, M. M. B., Fratiglioni, L., Helmer, C., Hendrie, H. C., … Brayne, C. (2017). The changing prevalence and incidence of dementia over time: Current evidence. Nature Reviews Neurology, 13(6), 327–339. doi: http://dx.doi.org/10.1038/nrneurol.2017.63
- Zahodne, L. B., Glymour, M. M., Sparks, C., Bontempo, D., Dixon, R. A., MacDonald, S. W. S., & Manly, J. J. (2011). Education does not slow cognitive decline with aging: 12-year evidence from the Victoria Longitudinal Study. Journal of the International Neuropsychological Society, 17, 1–8. doi: http://dx.doi.org/10.1017/S1355617711001044
- Zelinski, E. M., Gilewski, M. J., & Schaie, K. W. (1993). Individual differences in cross-sectional and 3-year longitudinal memory performance across the adult life span. Psychology and Aging, 8(2), 176–186. doi: http://dx.doi.org/10.1037/0882-7974.8.2.176