
Abstract
Introduction: Perceived loneliness and depression are risk factors threatening mental well-being of older people. Yet, hardiness, a modifiable internal resource that supports functional resilience, may enhance the capacity of adjusting to challenges arising from age-related physical and psychosocial changes. Hence, hardiness can be a protective factor of mental health. This study examined the role of hardiness in the relationship between perceived loneliness and depressive symptoms among older people in Hong Kong.
Methods: 424 Cantonese-speaking Chinese participants, aged 60 years or above, completed a self-reported questionnaire set related to perceived loneliness, hardiness, and depressive symptoms. Structural equation modeling was used to test the proposed model.
Results: Results revealed that hardiness partially mediated the positive association between perceived loneliness and depressive symptoms [β = .18, p < .001, BC 95% CI (.10, .27)] with good data-model fit [χ2(32) = 36.34, p = .27; CFI = .998; TLI = .997; RMSEA = .018; SRMR = .022].
Conclusion: Older people with higher level of perceived loneliness reported less hardiness. Lower levels of hardiness, in turn, correlated with increased self-reported depressive symptoms. The potential benefits of hardiness for promoting mental health of older people was discussed.
Introduction
Advanced age is associated with various life challenges that include issues stemming from retirement, health concerns, and the loss of loved ones. Such changes inevitably have an impact on older people’s social lives in a way that can lead to perceived loneliness (Cacioppo, Hawkley, & Thisted, Citation2010) and psychological feelings of depression. Even if such individuals do not technically meet the diagnostic criteria for clinical depression, many older people are, in fact, suffering from depressive symptoms (Braam et al., Citation2014; Jeuring, Huisman, Comijs, Stek, & Beekman, Citation2016). Both perceived loneliness and depressive symptoms significantly impact the well-being of older people (Braam et al., Citation2014; Jeuring et al., Citation2016) and may increase the predisposed risk of suicide among older people (Rurup, Deeg, Poppelaars, Kerkhof, & Onwuteaka-Philipsen, Citation2011). As such, understanding the relationship between these two variables would furnish valuable insight into suitable modes of intervention for promoting quality-of-life improvements during natural aging.
Perceived loneliness refers to one’s subjective experience of dissatisfaction and distress in social relationships, regardless of the reality of engagement in activities and actual amount of time spent alone (Andersson, Citation1998; Peplau & Perlman, Citation1982). Perceptions of one’s internal and external worlds interact with each other to produce a self-reinforcing cycle; this cycle works to maintain a given level of perceived loneliness via subconscious hypervigilance to social threats in the environment (loneliness model; Hawkley & Cacioppo, Citation2010). Cognitive biases are formed during this cycle and such biases play a role in shaping a person’s cognitions, behaviors, and emotions (Hawkley & Cacioppo, Citation2010).
The research has repeatedly shown positive association between loneliness and depressive symptoms (Barg et al., Citation2006; Cacioppo, Hughes, Waite, Hawkley, & Thisted, Citation2006; Luo, Hawkley, Waite, & Cacioppo, Citation2012). Loneliness is also associated with activations of areas in the brain that are related to affective processing and as such, plays a meaningful role in late-life depression (Wong et al., Citation2016). There is a scarcity of studies on the mechanisms underlying the perceived loneliness-depressive symptoms relationship that address issues other than related risks and protective factors. It would be worthwhile to attain a more robust understanding of the potential mechanisms to get a firmer grasp of individual differences among older individuals.
One factor that may contribute to variations in the capacity for adaptive adjustment to late-life changes is hardiness, a modifiable essential component of resilience (Bonanno, Citation2004; Maddi, Citation2007, Citation2013; Ong, Bergeman, & Boker, Citation2009). Hardiness motivates people to persevere in the face of challenges (Maddi, Citation2002). It consists of a pattern of attitudes and behaviors that facilitate adaptive adjustment under stressful conditions (Kobasa, Maddi, & Courington, Citation1981). According to the hardiness model (Maddi, Citation2002), people characterized by hardy attitudes tend to engage with activities and people (Commitment), believe that efforts can achieve desirable outcomes (Control), and regard difficulties as surmountable challenges and learning opportunities (Challenge). Such individuals exhibit hardy forms of behaviors that include effective coping strategies, supportive social interactions, and beneficial self-care aimed at averting the development of strain and onset of physical, mental, and behavioral breakdowns (Maddi, Citation2013).
The contribution of hardiness to well-being has been demonstrated by studies that involved different population samples, such as military personnel (Bartone, Citation1999), undergraduates (Beasley, Thompson, & Davidson, Citation2003), and older people (Magnani, Citation1990). Hardiness appears to be inversely correlated with depressive symptoms (Eschleman, Bowling, & Alarcon, Citation2010). This inverse relationship can also be found among older people in both community (Sharpley & Yardley, Citation1999) and care centers (Engel et al., Citation2011). Further, research has also found hardiness to be associated with brain activations of the right amygdala and left orbitofrontal areas that are related to affective processing, integration, and regulation (Reynaud et al., Citation2013). Older people with higher level of hardiness were found to experience more positive emotions daily, regardless of life challenges and stress (Ong, Bergeman, Bisconti, & Wallace, Citation2006). Taken together, the results of these studies indicate that hardiness potentially has the capacity to protect older people from the negative emotions stemming from the positive association identified between perceived loneliness and depressive symptoms.
The relationship between loneliness and depressive symptoms and that between hardiness and depressive symptoms have been consistently reported. Hardiness is likely a mediator rather than a moderator to influence the strength or direction of the relationship between loneliness and depressive symptoms because moderation usually applies to explain inconsistent relationship between variables (Baron & Kenny, Citation1986). In this study, the objective was to determine if hardiness, as a modifiable component of resilience, plays a significant role in mediating the relationship between perceived loneliness and depressive symptoms in older individuals. We hypothesized that hardiness (1) would be inversely correlated with perceived loneliness and depressive symptoms and (2) would mediate the relationship between perceived loneliness and depressive symptoms.
Methods
Participants
The current study was part of a larger study of older people with the aim to examine effectiveness of cognitive training on cognitive functioning (Lee & Yu, Citation2018) and approved by the Human Research Ethics Committee of The University of Hong Kong. Four hundred and twenty-four older Cantonese-speaking Chinese participants were recruited from the community via notices posted at the university, elderly centers within non-governmental organization, and a monthly newsletter targeted at older people. Inclusion criteria were the following: age of 60 years or above, vision and hearing at normal or corrected-to-normal levels, and a literacy level of Grade 3 or higher. Exclusion criteria included a history of psychiatric or neurological disorder(s) impacting cognitive and affective functioning and a score below 22 on the Hong Kong version of the Montreal Cognitive Assessment (HK-MoCA; Wong et al., Citation2009).
Measures and procedures
Upon receiving written consent from the participants after full explanation of the study, well-trained research staff administered the HK-MoCA (Wong et al., Citation2009) and helped the participants complete the self-reported questionnaires. At the end of the session, the research staff provided participants with a verbal report about their general cognitive status and depressive tendencies, according to their scores.
Loneliness
The Chinese version of the University of California, Los Angeles (UCLA) Loneliness Scale (Version 3; Chou, Jun, & Chi, Citation2005; Russell, Citation1996) measured level of perceived loneliness. The scale included 20 statements inquiring about how people feel and participants scored the frequency of their own such feelings on a 4-point scale (1 = never, 2 = rarely, 3 = sometimes, 4 = always). Example of items included “How often do you feel that people are around you but not with you?”. 9 out of the 20 statements were reverse-scored. Higher scores reflected higher levels of perceived loneliness. Past studies indicated that the scale correlated negatively with social support, self-reported quality of health, and life satisfaction, while correlating positively with burnout and depression (Russell, Citation1996). The test-retest reliability of the scale over one year was .73 (Russell, Citation1996). The scale has been found to be reliable among samples in western culture (Cronbach’s α = .89–.94; Russell, Citation1996) and for sample located in Hong Kong (Cronbach’s α = .90; Chou et al., Citation2005). Cronbach’s alpha in the current study was .91.
Hardiness
The Chinese version of the Dispositional Resilience Scale (DRS-15; Bartone, Citation1999; Wong et al., Citation2014) assessed hardiness in terms of the concepts of commitment, control, and challenge (3Cs). The participants completed the scale by evaluating the relative truth of 15 statements (as applied to themselves) on a 4-point scale (0 = not at all true, 1 = slightly true, 2 = quite true, 3 = completely true). Example item included: “Most of my life gets spent doing things that are meaningful”. 6 out of the 15 statements were reverse-scored. Higher scores reflected higher levels of hardiness. The total score of the scale responses correlated negatively with depression; the scores of non-depressed participants were higher than those of the depressed participants (Wong et al., Citation2014). The scale has been found to be reliable in a sample in the West (Cronbach’s α = .82; Bartone, Citation1999). The Chinese version has been found to be reliable for sample located in Hong Kong (Cronbach’s α = .78; Wong et al., Citation2014). Cronbach’s alpha in the current study was .70.
Depressive symptoms
The Chinese version of the Geriatric Depression Scale (GDS; Chiu et al., Citation1994; Yesavage & Sheikh, Citation1986) was used to assess depressive symptoms over the previous week based on a “yes/no” response. Example item included: “Do you feel pretty worthless the way you are now?”. 10 out of the 15 symptoms were reverse-scored. Higher scores indicated more depressive symptoms. The mean scores on the scale among the depressed older people were higher than those of the non-depressed group (Chiu et al., Citation1994). The test-retest reliability of the scale over one week was .84 (Chiu et al., Citation1994). The Chinese version of the scale has been demonstrated to be reliable among the samples of Chinese older people (Cronbach’s α = .92; Chiu et al., Citation1994). Cronbach’s alpha in the current study was .75.
Data analyses
Analysis of correlations was conducted by SPSS software (Version 22; SPSS INC., Chicago, IL, USA) which identified demographic characteristics such as age, gender, years of education, and employed status that correlated with the study variables.
Structural equation modeling (SEM) with maximum likelihood was conducted to test the proposed mediation model by Mplus (Muthén & Muthén, Citation2012). There were no missing data in the analysis. SEM offers simultaneously examination of measured and latent variables, with consideration of measurement error, to avoid bias of the parameter estimations (Kline, Citation2011). Loneliness and depressive symptoms were independent and dependent variables respectively; whereas hardiness was a mediator. All study variables were constructed as latent variables to prevent biased estimation. Parcels of items (summing several items together) served as indicators under each latent variable instead of using individual items or total scale scores to obtain less biased estimates (Bandalos & Finney, Citation2001; Coffman & MacCallum, Citation2005). The advantages of this approach include: increased reliability of the indicators, a more parsimonious model with higher power of tests of model fit, and working on non-normally distributed data and dichotomous variables (Coffman & MacCallum, Citation2005; Kishton & Widaman, Citation1994). In the item-parceling (Coffman & MacCallum, Citation2005), exploratory factor analysis (EFA) with oblique rotation was conducted on the items by SPSS software (Version 22; SPSS INC., Chicago, IL, USA). Three parcels under each latent variable were used by following model identification in SEM and less estimation bias (Coffman & MacCallum, Citation2005; Kline, Citation2011; Matsunaga, Citation2008). The items were assigned to one of the three parcels one-by-one in descending order of their factor loadings.
Bootstrapping technique was used to test the indirect effect of the mediation model (Shrout & Bolger, Citation2002). A total bootstrap sample of 5000 was derived from the original data to generate bias-corrected 95% confidence intervals (BC 95% CI) aimed at conducting an accurate assessment of the mediating effect (MacKinnon, Lockwood, Hoffman, West, & Sheets, Citation2002). If the indirect effect was significant at p < .05 and the BC 95% CI did not include zero, the mediating effect was supported (Shrout & Bolger, Citation2002). The chi-square statistics (χ2), Comparative Fit Index (CFI), Tucker-Lewis Index (TLI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR) were used to evaluate data-model fit (Hu & Bentler, Citation1999). The mediation model was accepted if CFI and TLI > .90 while SRMR and RMSEA < .08 (Browne & Cudeck, Citation1993; Hu & Bentler, Citation1999).
Results
Descriptive statistics
The characteristics of the sample are presented in . Means, standard deviations, and correlations of the study variables are summarized in . Gender (r = −.12, p = .02) was correlated with depressive symptoms and thus was included as exogenous variable in the model. There were no significant differences in loneliness [t(422) = −0.51, p = .61] and hardiness scores [t(422) = −0.14, p = .89] between the male and female participants. However, there was a significant gender-related effect on depressive symptoms [t(422) = 2.41, p = .02]. Female participants (M = 3.73, SD = 2.60) had more depressive symptoms than males (M = 3.05, SD = 2.67).
Table 1. Characteristics of the study sample (N = 424).
Table 2. Descriptive statistics and correlations of the study variables.
Mediation model
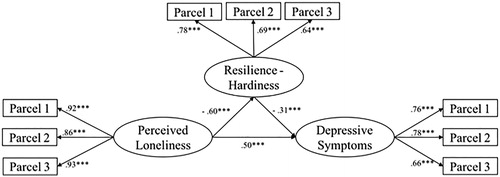
Factor loadings of all item parcels to the latent variables were significant (). The data suggests good data-model fit: χ2(32) = 36.34, p = .27; CFI = .998; TLI = .997; RMSEA = .018; SRMR = .022. The paths from loneliness to hardiness (β = −.60, p < .001) and to depressive symptoms (β = .50, p < .001) were significant. Also, the path from hardiness to depressive symptoms was significant (β = −.31, p < .001). Total effect of loneliness on depressive symptoms was significant (β = .69, p < .001). Indirect effect of hardiness on the positive relationship between loneliness and depressive symptoms was significant (β = .18, p < .001). The bootstrap BC 95% CI (.10, .27) did not include zero. Hardiness partially mediated the positive association of perceived loneliness and depressive symptoms.
Figure 1. Standardized estimates of the mediation model showing that hardiness partially mediated the positive relationship between perceived loneliness and depressive symptoms. The items under each parcel, standardized regression coefficients of the error terms, and covariate are not shown. ***p < .001.
Discussion
Findings of the structural equation modeling implemented in this study supported the two a priori hypotheses. To wit, there were negative correlations between hardiness and perceived loneliness as well as hardiness and depressive symptoms. Furthermore, hardiness partially mediated the direct relationship between perceived loneliness and depressive symptoms.
The role of hardiness in the relationship between perceived loneliness and depressive symptoms
Findings of this study are consistent with that of previous studies (Barg et al., Citation2006; Cacioppo et al., Citation2006; Cacioppo et al., Citation2010) showing a positive relationship between perceived loneliness and depressive symptoms. We observed that hardiness partially mediated the positive relationship between perceived loneliness and depressive symptoms among the older people in the current study. The distorted beliefs and emotions borne of the experience of perceived loneliness might facilitate the development of depressive symptoms (Beck, Citation2008).
It has been found that people with higher level of perceived loneliness reported lower level of perceived social support (Cacioppo et al., Citation2006), a perspective association with maladaptive coping (Vanhalst, Luyckx, Teppers, & Goossens, Citation2012), and were likelier to engage in unhealthy behaviors (Lauder, Mummery, Jones, & Caperchione, Citation2006). According to the loneliness model proposed by Hawkley and Cacioppo (Citation2010), perceived loneliness could be maintained by social cognitive processes such as interpretation biases in the self-reinforcing loneliness loop. Furthermore, perceived loneliness may influence an individual’s cognitions, behaviors, and emotions. Following these lines of thoughts, older people with high level of perceived loneliness may be reluctant to engage in activities that promote hardiness, adversely affecting the cultivation of hardiness (i.e. hardy attitudes and behaviors). As such, older people with high level of perceived loneliness do not usually engage in social activities or behavioral practices that help alleviate depressive symptoms (low commitment). They tend to see the suffering that they perceived as unaltered reality (from perceived loneliness). Yet, they are unwilling to commit much effort to enact healthy behavioral practices to improve the situation (low control). Also, it is common that they perceive the experience of loneliness as adversity rather than an opportunity of growth (low challenge). As a result, substantial depressive symptoms may be accumulated.
Hardiness has been found to be positively correlated with activations of brain areas related to affective processing, integration, and regulation (Reynaud et al., Citation2013). It played a role in weakening the inverse correlation between negative and positive emotions in confronting daily stress (Ong et al., Citation2006). Older people with higher level of hardiness engaged and savored more in positive events in daily life (Ong et al., Citation2009). Hardiness was also related to adaptive coping (Soderstrom, Dolbier, Leiferman, & Steinhardt, Citation2000). In this study, we observed that older people with higher level of hardiness were associated with fewer depressive symptoms. This finding is consistent with that reported in previous studies (Engel et al., Citation2011; Sharpley & Yardley, Citation1999). It seems that hardiness can be a protective factor of affective dysregulation causing depressive symptoms. Hardiness could be one of the mechanisms underlying the relationship between perceived loneliness and depressive symptoms.
Implications for future study
The present study, as the very first empirical evidence, highlights the mediating role of hardiness in the relationship between perceived loneliness and depressive symptoms. Hardiness, as a potentially modifiable internal component of resilience, can be cultivated via coaching and training (Maddi, Citation2007). To reduce the depressive symptoms that may derive from perceived loneliness among older people due to late-life changes, providing them with hardiness training could be helpful. Studies related to hardiness training have been conducted among different samples, including university students (Hasel, Abdolhoseini, & Ganji, Citation2011), nurse managers (Judkins, Reid, & Furlow, Citation2006), and clinically depressed patients (Bahamin, Taheri, Moghaddas, Sohrabi, & Dortaj, Citation2012). The sustained increase in hardiness from the hardiness training may be over 6 to 24 months (Maddi, Citation2013). Future studies should consider replicating this study to a larger and representative sample to understand the potential benefit of hardiness training for older people.
Limitations
The conclusion about causal relationships among the variables studied was limited by the cross-sectional design of this study. A longitudinal study design is required to address the causal directionality of these variables. Findings based on questionnaires could be vulnerable to subjective bias. To minimize this threat to the validity of our findings, we used only reliable and validated questionnaires with good psychometric properties. The scores of GDS were treated as continuous variables in this study. However, the scores could also be divided into categories according to cut-off. People could be categorized as normal even with few depressive symptoms if the scores are within the cut-off. Future studies may use GDS as categorical variable to understand the relationships of the variables from another perspective. A convenient sample (Female participants: 71.2%) was used in this study. Although gender was included as an exogenous variable in the model, to control for its effect on depressive symptoms, the generally homogeneous sociodemographic backgrounds of our participants might have compromised the representativeness and generalizability of the findings in the current study. The use of a convenient sample in this study limits the degree of representativeness and generalizability of the findings. Future studies should consider using a stratified and ecologically valid sample.
Conclusion
Hardiness plays a role in mediating the positive relationship between perceived loneliness and depressive symptoms in the older people, suggesting that hardiness training may help alleviate depressive symptoms in older people. Future studies may consider exploring and verifying the application of hardiness training to promote mental well-being and quality of life in older people.
Disclosure statement
No potential conflict of interest was reported by the authors.
Funding
This work was supported by funding from The University of Hong Kong May Endowed Professorship and the KKHo International Charitable Foundation.
References
- Andersson, L. (1998). Loneliness research and interventions: A review of the literature. Aging and Mental Health, 2, 264–274.
- Bahamin, G., Taheri, F., Moghaddas, A., Sohrabi, F., & Dortaj, F. (2012). The effects of hardiness training on suicide ideation, quality of life and plasma levels of lipoprotein (a) in patients with depressive disorder. Procedia – Social and Behavioral Sciences, 46, 4236–4234.
- Bandalos, D. L., & Finney, S. J. (2001). Item parceling issues in structural equation modeling. In G. A. Marcoulides & R. E. Schumacker (Eds.), New developments and techniques in structural equation modeling (pp. 269–296). Mahwah, NJ: Lawrence Erlbaum Associates.
- Barg, F. K., Huss-Ashmore, R., Wittink, M. N., Murray, G. F., Bogner, H. R., & Gallo, J. J. (2006). A mixed-methods approach to understanding loneliness and depression in older adults. The Journals of Gerontology Series B: Social Sciences, 61(6), S329–S339.
- Baron, R. M., & Kenny, D. A. (1986). The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51(6), 1173–1182.
- Bartone, P. T. (1999). Hardiness protects against war-related stress in Army Reserve forces. Consulting Psychology Journal: Practice and Research, 51(2), 72–82.
- Beasley, M., Thompson, T., & Davidson, J. (2003). Resilience in response to life stress: The effects of coping style and cognitive hardiness. Personality and Individual Differences, 34(1), 77–95.
- Beck, A. T. (2008). The evolution of the cognitive model of depression and its neurobiological correlates. The American Journal of Psychiatry, 165(8), 969–977.
- Bonanno, G. A. (2004). Loss, trauma, and human resilience: Have we underestimated the human capacity to thrive after extremely aversive events? American Psychologist, 59(1), 20–28.
- Braam, A. W., Copeland, J. R. M., Delespaul, P. A. E. G., Beekman, A. T. F., Como, A., Dewey, M., … Skoog, I. (2014). Depression, subthreshold depression and comorbid anxiety symptoms in older Europeans: Results from the EURODEP concerted action. Journal of Affective Disorders, 155, 266–272.
- Browne, M. W., & Cudeck, R. (1993). Alternative ways of assessing model fit. In Bollen, K. A. & Long, J. S. (Eds.), Testing structural equation models (pp. 136–162). Newbury Park, CT: Sage.
- Cacioppo, J. T., Hawkley, L. C., & Thisted, R. A. (2010). Perceived social isolation makes me sad: 5-year cross-lagged analyses of loneliness and depressive symptomatology in the Chicago Health, Aging, and Social Relations Study. Psychology and Aging, 25(2), 453–463.
- Cacioppo, J. T., Hughes, M. E., Waite, L. J., Hawkley, L. C., & Thisted, R. A. (2006). Loneliness as a specific risk factor for depressive symptoms: Cross-sectional and longitudinal analyses. Psychology and Aging, 21(1), 140–151.
- Chiu, H. F., Lee, H. C., Wing, Y. K., Kwong, P. K., Leung, C. M., & Chung, D. W. (1994). Reliability, validity and structure of the Chinese Geriatric Depression Scale in a Hong Kong context: A preliminary report. Singapore Medical Journal, 35, 477–480.
- Chou, K. L., Jun, L. W., & Chi, I. (2005). Assessing Chinese older adults’ suicidal ideation: Chinese version of the Geriatric Suicide Ideation Scale. Aging and Mental Health, 9(2), 167–171.
- Coffman, D. L., & MacCallum, R. C. (2005). Using parcels to convert path analysis models into latent variable models. Multivariate Behavioral Research, 40(2), 235–259.
- Engel, J. H., Siewerdt, F., Jackson, R., Akobundu, U., Wait, C., & Sahyoun, N. (2011). Hardiness, depression, and emotional well‐being and their association with appetite in older adults. Journal of the American Geriatrics Society, 59(3), 482–487.
- Eschleman, K. J., Bowling, N. A., & Alarcon, G. M. (2010). A meta-analytic examination of hardiness. International Journal of Stress Management, 17(4), 277–307.
- Hasel, K. M., Abdolhoseini, A., & Ganji, P. (2011). Hardiness training and perceived stress among college students. Procedia – Social and Behavioral Sciences, 30, 1354–1358.
- Hawkley, L. C., & Cacioppo, J. T. (2010). Loneliness matters: A theoretical and empirical review of consequences and mechanisms. Annals of Behavioral Medicine, 40(2), 218–227.
- Hu, L. T., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6(1), 1–55.
- Jeuring, H. W., Huisman, M., Comijs, H. C., Stek, M. L., & Beekman, A. T. F. (2016). The long-term outcome of subthreshold depression in later life. Psychological Medicine, 46(13), 2855–2865.
- Judkins, S., Reid, B., & Furlow, L. (2006). Hardiness training among nurse managers: Building a healthy workplace. The Journal of Continuing Education in Nursing, 37(5), 202–207.
- Kishton, J. M., & Widaman, K. F. (1994). Unidimensional verses domain representative parceling of questionnaire items: An empirical example. Educational and Psychological Measurement, 54(3), 757–765.
- Kline, R. B. (2011). Principles and practice of structural equation modeling (3rd ed.). New York, NY: Guilford Press.
- Kobasa, S. C., Maddi, S. R., & Courington, S. (1981). Personality and constitution as mediators in the stress-illness relationship. Journal of Health and Social Behavior, 22(4), 368–378.
- Lauder, W., Mummery, K., Jones, M., & Caperchione, C. (2006). A comparison of health behaviours in lonely and non-lovely populations. Psychology, Health, and Medicine, 11(2), 233–245.
- Lee, T. M. C., & Yu, J. (2018). Neural and behavioural effects of cognitive training during prefrontal modulation with tDCS in healthy elderly. Unpublished Raw Data.
- Luo, Y., Hawkley, L. C., Waite, L. J., & Cacioppo, J. T. (2012). Loneliness, health, and mortality in old age: A national longitudinal study. Social Science and Medicine, 74(6), 907–914.
- MacKinnon, D. P., Lockwood, C. M., Hoffman, J. M., West, S. G., & Sheets, V. (2002). A comparison of methods to test mediation and other intervening variable effects. Psychological Methods, 7(1), 83–104.
- Maddi, S. R. (2002). The story of hardiness: Twenty years of theorizing, research, and practice. Consulting Psychology Journal: Practice and Research, 54(3), 173–185.
- Maddi, S. R. (2007). Relevance of hardiness assessment and training to the military context. Military Psychology, 19(1), 61–70.
- Maddi, S. R. (2013). Hardiness: Turning stressful circumstances into resilient growth. Dordrecht: Springer.
- Magnani, L. E. (1990). Hardiness, self-perceived health, and activity among independently functioning older adults. Scholarly Inquiry for Nursing Practice, 4, 171–184.
- Matsunaga, M. (2008). Item parceling in structural equation modeling: A primer. Communication Methods and Measures, 2(4), 260–293.
- Muthén, L. K., & Muthén, B. O. (2012). Mplus user’s guide (7th Ed). Los Angeles, CA: Muthén & Muthén.
- Ong, A. D., Bergeman, C. S., Bisconti, T. L., & Wallace, K. A. (2006). Psychological resilience, positive emotions, and successful adaptation to stress in later life. Journal of Personality and Social Psychology, 91(4), 730–749.
- Ong, A. D., Bergeman, C. S., & Boker, S. M. (2009). Resilience comes of age: Defining features in later adulthood. Journal of Personality, 77(6), 1777–1804.
- Peplau, L. A., & Perlman, D. (1982). Perspectives on loneliness. In Peplau, L. A., & Perlman, D. (Eds.), Loneliness: A sourcebook of current theory, research and therapy (pp. 1–18). New York, NY: Wiley.
- Reynaud, E., Guedj, E., Souville, M., Trousselard, M., Zendjidjian, X., El Khoury-Malhame, M., … Khalfa, S. (2013). Relationship between emotional experience and resilience: An fMRI study in fire-fighters. Neuropsychologia, 51(5), 845–849.
- Rurup, M. L., Deeg, D. J. H., Poppelaars, J. L., Kerkhof, A. J. F. M., & Onwuteaka-Philipsen, B. D. (2011). Wishes to die in older people: A quantitative study of prevalence and associated factors. Crisis, 32(4), 194–203.
- Russell, D. (1996). UCLA Loneliness Scale (Version 3): Reliability, validity, and factor structure. Journal of Personality Assessment, 66(1), 20–40.
- Sharpley, C. F., & Yardley, P. (1999). The relationship between cognitive hardiness, explanatory style, and depression-happiness in post-retirement men and women. Australian Psychologist, 34(3), 198–203.
- Shrout, P. E., & Bolger, N. (2002). Mediation in experimental and nonexperimental studies: New procedures and recommendations. Psychological Methods, 7(4), 422–445.
- Soderstrom, M., Dolbier, C., Leiferman, J., & Steinhardt, M. (2000). The relationship of hardiness, coping strategies, and perceived stress to symptoms of illness. Journal of Behavioral Medicine, 23(3), 311–328.
- Vanhalst, J., Luyckx, K., Teppers, E., & Goossens, L. (2012). Disentangling the longitudinal relation between loneliness and depressive symptoms: Prospective effects and the intervening role of coping. Journal of Social and Clinical Psychology, 31(8), 810–834.
- Wong, J. Y.-H., Fong, D. Y.-T., Choi, A. W.-M., Chan, C. K.-Y., Tiwari, A., Chan, K. L., … Bartone, P. (2014). Transcultural and psychometric validation of the Dispositional Resilience Scale (DRS-15) in Chinese adult women. Quality of Life Research, 23(9), 2489–2494.
- Wong, N. M. L., Liu, H.-L., Lin, C., Huang, C.-M., Wai, Y.-Y., Lee, S.-H., & Lee, T. M. C. (2016). Loneliness in late-life depression: Structural and functional connectivity during affective processing. Psychological Medicine, 46(12), 2485–2499.
- Wong, A., Xiong, Y. Y., Kwan, P. W. L., Chan, A. Y. Y., Lam, W. W. M., Wang, K., … Mok, V. C. T. (2009). The validity, reliability and clinical utility of the Hong Kong Montreal Cognitive Assessment (HK-MoCA) in patients with cerebral small vessel disease. Dementia and Geriatric Cognitive Disorders, 28(1), 81–87.
- Yesavage, J. A., & Sheikh, J. I. (1986). Geriatric Depression Scale (GDS) recent evidence and development of a shorter version. Clinical Gerontologist, 5(1-2), 165–173.