
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Objectives
The impact of grandparenting on depression is mediated by both macro- and micro-level factors, however, their combined examination between different country contexts is relatively rare. This study examined whether country level income and grandparents’ gender influenced the relationship between the transition to grandparenthood and individuals’ depression across England, Europe and China.
Methods
Multi-level linear regression analyses with restricted maximum likelihood estimation were performed covering 15 countries from the ELSA, the SHARE and the CHARLS 2010-15 in order to understand cross-country differences in this area.
Results
This study found significant cross-national variations in the effects of transitioning to grandparenthood on individuals’ depression. Transitioning to grandparenthood reduced the depression score among both men and women in lower income countries, but increased it in higher income countries. Moreover, the gender gap in the effects of becoming a grandparent on one’s depression was wider in lower income countries than higher income countries.
Conclusions
Policymakers should pay attention to the support grandparents need, and systematically integrate childcare provided by grandparents into family policies. Policies supporting older people should take into account the way in which macro-level and micro-level factors combine to affect grandparents’ well-being.
Introduction
The role of grandparents has become increasingly important worldwide, whilst a large number of studies have shown that grandparenthood and grandchild care provision significantly affect individuals’ health in later life (Condon et al., Citation2018; Di Gessa et al., Citation2016; Silverstein & Zuo, Citation2020). Previous research has suggested that the transition to grandparenthood has a complex effect on grandparents’ depressive symptoms, which is influenced by macro-level factors such as the economic, cultural and policy context (Bordone & Arpino, Citation2019; Neuberger & Preisner, Citation2018). In addition, researchers have emphasised the importance of incorporating a gender perspective to examine this topic (Di Gessa et al., Citation2016; Xu, Citation2019). However, although recent evidence has consistently highlighted the need for examining the relationship between grandparenthood and late-life depression across different cultures (Arpino & Gomez-Leon, Citation2020; Chung & Park, Citation2018; Kim et al., Citation2017), there is a lack of research examining macro-level factors to understand the pattern.
This paper seeks to contribute to this relatively under-studied area by investigating the transition to grandparenthood and its impact on people’s depression across different nations, i.e. in the People’s Republic of China which is dominated by the Confucian culture, as well as England and Europe as representative of a Western context. This study is based on multilevel analyses using the Harmonised English Longitudinal Study of Ageing (ELSA), the Harmonised Survey of Health, Ageing, and Retirement in Europe (SHARE) and the Harmonised China Health and Retirement Longitudinal Study (CHARLS) collected between 2010-15.
Grandparenthood and depression
Approximately one billion people in the world population are grandparents, which makes it crucial to examine issues relating to grandparenthood, particularly the complex impact of grandparenthood on people’s health (Moore & Rosenthal, Citation2017). Previous research has shown contradictory findings. On the positive side, becoming a grandparent brings opportunities to interact with the younger generations and to fulfil one’s self-esteem (Condon et al., Citation2018), and is also beneficial for grandparents’ subjective well-being and depressive symptoms (Arpino et al., Citation2018; Bordone & Arpino, Citation2019). However, grandparenting can cause intergenerational conflicts and stress and increase how old the grandparent feels (Condon et al., Citation2018).
Depression is one of the four major diseases influencing human being (World Health Organisation, Citation2008). Previous research has specified non-linear relationship between grandchild care provision and depressive symptoms in Europe and the fact that the financial support received by older people moderates the impact of grandchild care provision on grandparents’ depression in China (Bordone & Arpino, Citation2019; Condon et al., Citation2018; Di Gessa et al., Citation2016; Silverstein & Zuo, Citation2020). However, only two studies have paid attention to examining the initial transition to grandparenthood (Bordone & Arpino, Citation2019; Condon et al., Citation2018). The study by Condon et al. (Citation2018) found that transitioning to grandparenthood was not associated with depression, however this finding was limited as it was based on a relatively small sample of 262 female and 168 male respondents who provided non-custodial grandchild care in Australia. Bordone and Arpino (Citation2019) found that transitioning to grandparenthood in Spain, Israel, Sweden and Denmark reduced the effect of depressive symptoms for the grandmothers, while such associations were not found in the other 12 European countries. Further empirical investigations are needed to understand how becoming a grandparent can affect one’s depression across countries. In order to address this research gap, the current study seeks to critically examine the cross-national differences in the effects of transitioning to grandparenthood on individuals’ depression, and how they are moderated by both macro- and micro- level factors.
Factors affecting depression among grandparents
Micro-level factors
A growing body of literature has investigated micro-level factors influencing depression among grandparents such as grandparents’ ethnicity, age, gender, marital status and educational attainment (Arpino et al., Citation2018; Xu, Citation2019), and the gender of the grandparent has been found to be an important factor (Bordone & Arpino, Citation2019; Hughes et al., Citation2007). For example, it was found in the United States (US) that providing supplementary grandchild care was not significantly associated with the depression among grandmothers, while grandfathers providing such care experienced fewer depressive symptoms compared to those who did not provide grandchild care (Hughes et al., Citation2007). Bordone and Arpino (Citation2019) highlighted that in Europe, becoming a grandmother reduced the number of depressive symptoms one reported, but such relationship was not found among grandfathers. Based on the literature, the gender difference in the relationship between transitioning to grandparenthood and reporting depression is examined in the current study.
Marco-level factors
Little research has investigated the role of macro-level factors in determining the relationship between grandparenthood and one’s depression across countries (Bordone & Arpino, Citation2019; Di Gessa et al., Citation2016; Neuberger & Preisner, 2018). One reason is the lack of available high-quality international data with relevant information (Kim et al., Citation2017). A few studies have shown that culture (i.e. family norms) and policies (i.e. public childcare services, parental leave regulation and women labour force participation) can moderate the association between grandparenting and late-life depression (Di Gessa et al., Citation2016; Jappens & Van Bavel, Citation2012; Schwarz et al., Citation2010). For example, Jappens and Van Bavel (Citation2012) found that mothers in European contexts characterised by more conservative family norms tend to rely on grandparents as the main source of childcare. Di Gessa et al. (Citation2016) found that variations in grandparental childcare across Europe were mostly explained by differences in female labour market structure and formal childcare provision. Bordone and Arpino (Citation2019) examined cross-country differences in the relationship between grandparenthood and people’s depression by categorising European countries into three groups based on different levels of public childcare availability and parental leave policy: countries close to familialism, countries characterised by defamilialisation, and intermediate countries. However, the policy factors were used as criteria to classify European countries, and the effects of specific policy or cultural factors were not directly examined in this study (Bordone & Arpino, Citation2019).
Overall, the research on the cross-national variations in the relationship between transitioning to grandparenthood and one’s depressive symptoms remains at a preliminary stage. Existing studies provide important insights into the need of examining the relationship across contexts and investigate how macro-level and micro-level factors can moderate the relationship.
Conceptual framework
The structured ambivalence theory and the role theory help to understand how a country’s income can modify the relationship between becoming a grandparent and one’s depression.
The structured ambivalence theory
The structured ambivalence theory elaborates the conflict between individual behaviours and the individuals’ social context (Connidis & McMullin, Citation2002), which has been used to understand the cross-national differences in the effects of grandparenthood on individuals’ depression. For example, previous research has suggested that social or cultural expectations for grandparenthood can influence the psychological health among grandparents (Bordone & Arpino, Citation2019; Neuberger & Haberkern, Citation2014). The modernisation theory argues that familism is strongly associated with a country’s economic development, therefore norms of filial piety are less embedded in high income countries (Cowgill, Citation1972). The conflict between the expectation of becoming grandparents and the relatively weak norms of filial responsibility in higher income countries may lead to depressive symptoms among grandparents (Neuberger & Haberkern, Citation2014).
The role theory
The role strain theory focuses on the perceived strain and decreased health resulting from multiple roles (Goode, Citation1960). By contrast, the role enhancement theory proposes that role accumulation leads to positive feelings such as self-esteem and personality enhancement, therefore occupying multiple role responsibilities contributes to better health outcomes (Sieber, Citation1974). As suggested by previous research, the two role theories complement each other, and one may outweigh the other depending on the context (Chen & Liu, Citation2012). Most people retire at an older age in higher income countries compared to lower income countries, therefore grandparents in higher income countries may be more likely to experience depression resulting from a role overload, such as combining paid work and grandparenting. By contrast, the transition to grandparenthood may provide a sense of purpose and pride for new grandparents in lower income countries taking into account both stronger family ties and a lower retirement age compared to higher income countries, which consequently lessens grandparents’ depression symptoms based on the role enhancement theory.
No previous study has investigated how a country’s economy can moderate the effect of grandparenthood on older persons’ depression. An interesting study by Neuberger and Preisner (Citation2018) investigated the cross-national difference in the impact of having children on the parent’s quality of life, and how such relationship depends on the country’s economy and welfare state. Based on the longitudinal SHARE and ELSA data, the researchers found that older people living in countries with lower gross domestic product per capita benefited more from parenthood than those living in other countries (Neuberger & Preisner, Citation2018). Although this study focused on parenthood rather than grandparenthood, it has shone a light on examining the role of a country’s economy to moderate the relationship between grandparenthood and one’s depression.
Importantly, women in many countries, particularly lower income countries, are expected to take on more family responsibilities than men due to their different positions in the social structure, and they are also more likely than men to experience strain from transitioning to grandparenthood especially taking account of the increasing grandmothers’ participation in the labour force, hence the grandmothers’ and grandfathers’ experience of ambivalence also varies across countries (Arpino et al., Citation2018; Connidis & McMullin, Citation2002). Specifically, it is hypothesised that the gender gap of the effect of grandparenthood on depression is wider in lower income countries than higher income countries.
Research questions and hypotheses
Based on the above literature review, this study addresses the following research questions and proposes the following hypotheses:
How does the impact of transitioning to grandparenthood on the change of people’s depression vary across England, Europe and China?
Does the national economy (measured by country level income) modify the relationship between grandparenthood and depression in England, Europe and China?
Are there gender differences in the effects of transitioning to grandparenthood on people’s depression in Europe, England and China?
Hypothesis 1: Cross-national variations exist in the relationship between transitioning to grandparenthood and one’s depression.
Hypothesis 2: In less wealthy countries, transitioning to grandparenthood has a protective effect against depression among grandparents.
Hypothesis 3: In wealthier countries, transitioning to grandparenthood increases depression among grandparents.
Hypothesis 4: The gender gap of the effects of transitioning to grandparenthood on depression is wider in less wealthy countries than in wealthier countries.
Methods
Data
The Health and Retirement Studies and their harmonised versions are designed to facilitate cross-national and longitudinal research on demographic, health, family structure and social network of middle-aged and older people (Program on Global Aging, Citation2018). In order to compare information in the same periods, the Harmonised ELSA Waves 5-7, the Harmonised SHARE Waves 4-6 and the CHARLS Waves 1, 2 and 4 collected in 2010/1, 2012/3 and 2014/5 are used for the analyses (Beaumaster et al., Citation2018; Munich Center for the Economics of Aging (MEA), 2020; Phillips et al., Citation2017).
The data has a hierarchical structure of three levels: country- individual- observations. Observations are nested within individuals (i.e. an individual has three observations if participated in all three waves of the survey), which are nested within countries. The hierarchical structure of the data determines the use of multilevel modelling methods in this study (Hox, 2002).
Measures
Depression
The depressive symptoms of respondents are measured by the 8-item Centre for Epidemiologic Studies Depression Scale (CES-D) in the ELSA, 10-item CES-D in the CHARLS and 12-item EURO-D depression scale in the SHARE in each wave (Radloff, Citation1977; Prince et al., Citation1999). Each item in the ELSA and SHARE is measured with a binary answer (1 = yes, 0 = no), and the total depression score ranges between 0–8 in the ELSA and 0–12 in the SHARE (MEA, 2020; Phillips et al., Citation2017). The CHARLS provides a four-score scale for each depression-related item (0 = rarely or none of the time, 1 = some or a little of the time, 2 = occasionally or a moderate amount of time, 3 = all of the time). Consequently, for the CHARLS, the total score calculated using the sum of the 10 items ranges between 0–30 (Beaumaster et al., Citation2018). The differences in measuring depression in these countries should not be a concern as previous research has validated them in different settings and showed that they are valid comparable measures (Chin et al., Citation2015; Crimmins et al., Citation2011; Jadhav & Weir, Citation2018).
Three forms of the depression variables are used and compared as a robustness check: the original depression score (the higher the score, the more depressed the respondent is), the normalised depression score (calculated for each survey, ranging between 0–10) and a binary variable reflecting depression status (1 = yes, 0 = no). As has been done in existing studies, the cut-off point for the category of being depressed is 4 for the ELSA and SHARE (Arpino & Gomez-Leon, Citation2020; Dewey & Prince, Citation2005; Hamer et al., Citation2009), and 12 for the CHARLS (Ni et al., Citation2017; Xu et al., Citation2016).
Transitioning to grandparenthood
Transitioning to grandparenthood (1 = yes, 0 = no) is captured when respondents had no grandchild at baseline and had at least one grandchild in 2013 or 2015; or respondents had no grandchild in 2013 and had at least one grandchild in 2015. The same measures have been validated in previous research (Arpino et al., Citation2018; Bordone & Arpino, Citation2019).
Factors and covariates
The macro-level factor, a country’s mean income, was calculated using the mean income of individuals in a country. The logarithms of the country-level income were used in the analyses (ranging between 5–10) (Ermini & Hendry, Citation2008).
A number of covariates related to depression were controlled in the analyses based on existing literature (e.g. Bordone & Arpino, Citation2019; Silverstein & Zuo, Citation2020; Wang & Mutchler, Citation2020). Gender was used as a control variable in the models based on the full sample (Models 1, 2 & 5), and other analysis was stratified by gender (0 = male, 1 = female). Two health indicators, namely Activities of Daily Living (ADL) functional score (ranging from 0–6, measuring the number of ADL items the respondent has difficulties with) and self-reported health (a scale ranging from 1–5: Excellent to Poor) were included in the models. Socio-demographic variables including age (centered at 60 years old), marital status (1 = married or partnered, 0 = others), educational attainment (1 = less than lower secondary, 2 = upper secondary & vocational training, and 3 = tertiary) and the natural log of the individual income of respondents (the sum of individual total income and take-home pay after tax and any other deductions) were controlled in the models (Bordone & Arpino, Citation2019; Di Gessa et al., Citation2016). The annual individual income for the Chinese and European sample was transformed to its equivalent value in GBP based on the exchange rates in 2011, 2013 and 2015 accordingly.
Sample
Only countries with valid information about the depressive symptoms of respondents and the number of grandchildren in at least two waves are included in the analysis. In total, 15 countries are analysed, including England, Austria, Belgium, Czech Republic, Denmark, Estonia, France, Germany, Italy, Netherlands, Slovenia, Spain, Sweden and Switzerland and China. Respondents who were aged between 50 and 90, and who had at least two valid answers in terms of their grandparenthood status and depressive symptoms were kept in order to estimate the changes in the variables between waves. In order to focus on estimating the effect of transitioning to grandparenthood on the individuals’ depression, respondents who were grandchildless at baseline were kept as the analytical sample. The data structure and sample information are provided in and .
Table 1. Descriptive sample statistics in the longitudinal dataset.
Table 2. Multilevel estimates of transitioning to grandparenthood on the depression score of respondents.
shows the descriptive analysis of the characteristics of respondents by gender. Most statistics showed significant differences in the characteristics between men and women. Nearly one fifth of men and one third of women reported depression between 2010 and 2015. Almost one quarter and one fifth of respondents became grandparents between 2010-3 and 2012-5 respectively. Women had significantly poorer self-rated health and ADL functional status than men at baseline. On average, female respondents had significantly lower income than their male counterparts at baseline.
Analysis
Using Stata V.16 (StataCorp, Citation2019), multilevel linear regression models with Restricted Maximum Likelihood (REML) estimation was conducted in order to produce unbiased estimates taking into account the small level 2 sample size (Elff et al., Citation2016; McNeish & Stapleton, Citation2016). Analyses were stratified by sex where appropriate (Bordone & Arpino, Citation2019). Three steps of analyses were conducted. First, a three-level intercept-only model (Model 1) was compared with the null-model to examine whether there were cross-country differences in the depression score (Sascha et al., Citation2020). The three-level variance-components model is written as followed:
(1)
In this equation, is the depression score for observation
in respondent
in country
, where
is the fixed effects estimate,
is the between-country variance,
is the between-individual variance and
is the within-individual variance.
measures the extent to which depression scores vary between countries,
measures the extent to which depression scores vary within-countries-between-individuals, and
measures the extent to which depression scores vary within-individuals-between-observations. The intraclass correlation coefficient (ICC) was calculated to estimate the total variance that can be attributed to differences between countries and individuals (Rabe-Hesketh & Skrondal, Citation2012).
The country-level ICC is
The individual-level ICC is
Secondly, whether transitioning to grandparenthood as the explanatory variable, as well as a number of covariates were added to Model 1. Notably, with the use of REML estimates, the model fit indices are only comparable if the fixed effects are identical between models (Boedeker, Citation2017; Faraway, Citation2016, p. 156). As recommended by the literature, Log-likelihood deviance, Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC) were compared using Maximum Likelihood (ML) estimation in order to fit a best model (Boedeker, Citation2017). Afterwards, REML was used to estimate the final model in order to reduce bias. Model 2 provides the REML estimates based on the full sample, while Models 3 and 4 provide the estimates by gender. Independent residuals are assumed in order to avoid over-complication as the average respondent has only 2.7 measurement occasions (Rabe-Hesketh & Skrondal, Citation2012).
Finally, cross-level interactions between transitioning to grandparenthood and the country-level income was added to investigate whether a country’s income modifies the impact of transitioning to grandparenthood on depression (Model 5). Models 6 and 7 provide the estimates by gender. The multilevel model with cross-level interactions (Mode 5) can be written as below:
(2)
(2)
Where -
are the fixed effects regression parameters,
,
and
represent the between-country variance, the between-individual variance and the within-individual variance respectively.
Results
Cross-national differences in depression
demonstrates the significant country differences in the respondents’ depression score based on the three-level intercept-only model. Specifically, respondents in Denmark, Netherlands, Sweden, Switzerland, Austria and England reported significantly lower depression scores compared to China, Italy, Spain, Estonia and France. No significant country effects on reporting depression were found in Belgium, Slovenia, Czech Republic and Germany.
Figure 1. Predicted country effect on depression in the 15 countries, 2010-15.
Source: Author’s analysis of the Harmonised ELSA, SHARE, CHARLS 2010-15.
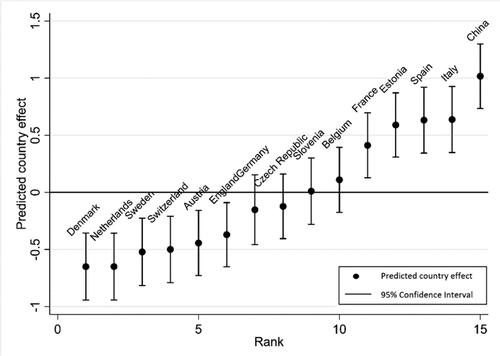
Model 1 in further shows the substantial country-level and individual-level clustering in the data. The country-level ICC is 21.9% and individual level ICC is 39.6%, which means that almost 22% of the total variance in reporting depressive symptoms were attributed to differences between countries and 40% of the total variance in reporting depressive symptoms were attributed to differences between individuals within countries.
Cross-national differences in the effects of grandparenthood on depression
shows the REML estimates of the random intercept model after adding whether transitioning to grandparenthood as the explanatory variable and individual and country level factors as explained in the Methods section. Transitioning to grandparenthood was associated with an increase in the depression score for both men and women, holding all other covariates constant (β1 = 0.08–0.09, p < 0.05, Models 3-4). Being married, being male, having higher education attainment, having a good self-rated health, having a good ADL functional status, having a higher individual income, and living in a higher income country were associated with a lower depression score (Model 2).
Cross-level interactions between the country-level income and transitioning to grandparenthood were further included, and results are reported in Models 5-7. Interestingly, the negative effect of transitioning to grandparenthood on one’s depression score weakens by 0.07 as the mean income in a country increases by one unit (Model 5). The mediation effect of country level income depends on grandparent’s gender. Specifically, the negative effect of becoming a grandfather on one’s depression score weakens by 0.09 as the mean income in a country increases by one unit (Model 6), and the effect of becoming a grandmother on one’s depression was not statistically related to a country’s income (Model 7). Robustness check using the other two depression variables (the normalised depression score and the binary depression variable) not presented in this paper showed similar results.
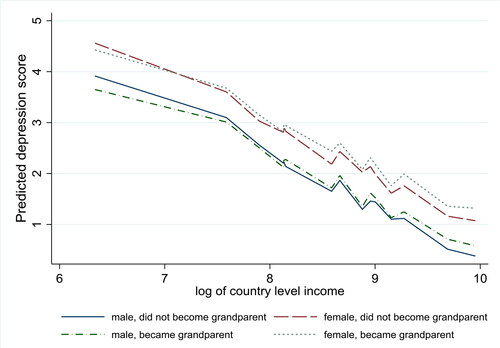
shows how the relationship between transitioning to grandparenthood and one’s depression depends on a country’s mean income by gender. In all countries, women had higher depression scores than men. In countries with relatively lower income including China, Czech Republic, Estonia, Italy, Spain and Slovenia, transitioning to grandparenthood reduced the depression score among both men and women. By contrast, for countries with relatively higher income such as Denmark, Netherlands, Sweden, Belgium, France and England, transitioning to grandparenthood increased the depression score among both men and women. The gender difference in the effect of transitioning to grandparenthood on depression also relates to a country’s income. Specifically, there is a larger difference between the predicted depression score for men and women in lower income countries. The gap between male and female depression scores is smaller in higher income countries ().
Figure 2. Predicted depression score on transitioning to grandparenthood for men and women by country mean income.
Note: The depression scores are predicted based on Model 4.
Source: Author’s analysis of the Harmonised ELSA, SHARE, CHARLS 2010-15
Discussion
In times of increasing longevity, research on the role of grandparenthood and its impact on people’s psychological health has become crucial. Little is known about whether and how such impact varies across country (Bordone & Arpino, Citation2019; Kim et al., Citation2017). This study set out to longitudinally examine cross-country differences in the relationship between grandparenthood and depression in England, Europe and China, and how the grandparent’s gender and the country level income can moderate the relationship.
The findings show significant cross-national differences in reporting depressive symptoms among people aged 50-90. Respondents in Denmark, Netherlands, Sweden, Switzerland, Austria and England were significantly less likely to report depressive symptoms than those in in China, Italy, Spain, Estonia and France. A previous study using multi-group confirmatory factor analysis concluded that among 11 European countries, the depression scores were lowest in Denmark, Switzerland, Sweden, and highest in southern European countries such as Italy and Spain (Missinne et al., Citation2014). The current study showed consistent findings and added that Chinese people aged 50-90 reported high depression scores, whilst English inhabitants were among the less depressed groups. The significant country variations in reporting depression need to be taken into account in future comparative research on grandparents’ health.
Significant cross-country differences were found in the effect of transitioning to grandparenthood on people’s depression, which support H1. This study confirms previous findings which showed that the impact of transitioning to grandparenthood on depressive symptoms varied between countries in Europe (Bordone & Arpino, Citation2019), but shows divergence in other ways. Specifically, previous research failed to find a clear pattern of the country differences, which may be due to the study’s restricted ability to compare across countries with the use of country fixed effects models (Bordone & Arpino, Citation2019). By contrast, this study highlights that transitioning to grandparenthood reduced the depression scores among both men and women in lower income countries, but increased the depression scores in higher income countries. The research finding provides evidence for H2 and H3. Neuberger and Haberkern (Citation2014) suggested that in countries where grandparents were normatively expected to provide grandchild care such as Spain and Italy, not looking after grandchildren favoured negative feelings and therefore, contributed to grandparents’ lower quality of life. Conversely, in countries with low social expectations towards grandparenting such as Denmark and Sweden, grandparents who provided grandchild care experienced a lower quality of life (ibid). Our findings used a broader concept of grandparenthood and a different measure of psychological health, contributing to a deeper understanding of the beneficial effect of grandparenthood on one’s depression in less wealthy countries. As explained by the Structural Ambivalence Theory and the Modernisation Theory, a country’s economic development influences familism which consequently affects the societal expectation for the role of grandparents, and moderates the relationship between grandparenthood and individuals’ depression (Neuberger & Haberkern, Citation2014; Silverstein & Zuo, Citation2020). The findings imply that becoming a grandparent lessens the effect of depressive symptoms in lower income countries, which supports the role enhancement theory. Conversely, the disadvantageous effect of grandparenthood on depression outweighs its beneficial effect in higher income countries. Existing research has not compared the application of role enhancement and role strain theory across countries of different income levels, which is an avenue for future studies on grandparenthood.
It is interesting to note the significant gender difference in the impact of transitioning to grandparenthood on reporting depression, which also relates to a country’s income. Specifically, the findings support H4 by showing that the gender difference in the effect of transitioning to grandparenthood on one’s depression was even larger in less wealthy countries. Previous studies on the cross-national differences of depression in Europe consistently found that depression was more prevalent among women than men, and such gender difference was smaller in Nordic countries compared to Eastern and Southern European countries (Van de Velde et al., Citation2010; Zunzunegui et al., Citation2007). This research expands the small existing body of literature by showing that the difference in the prevalence of depression in women and men varies depending on a country’s income.
The current study contributes to existing knowledge of the relationship between grandparenthood and depression by providing the comparisons across England, Europe and China. First, this study has confirmed cross-national variations in the impact of transitioning to grandparenthood on individuals’ depression based on comparable data. In addition, the empirical findings provide a new understanding of how a country’s income and the grandparent’s gender affect the relationship between grandparenthood and one’s depression with the use of multilevel models.
However, a number of limitations need to be considered. First, this study has only examined the effects of transitioning to grandparenthood, rather than the provision of grandchild care across countries. This is because this variable was measured differently in the ELSA (i.e. in a different module, information not directly collected) compared to the SHARE and the CHARLS. Consequently, the prevalence of grandchild care provision is very low based on the ELSA, and including such information would have biased the results (Phillips et al., Citation2017). This suggests the need to make available more comparable measures of grandchild care provision in international surveys (Hank et al., Citation2018). Second, the current study was unable to analyse more macro-level factors due to the availability of such information. Future research could investigate how other contextual-structural factors influence the relationship between grandparenthood and late-life depression, such as filial norms and welfare policies (Di Gessa et al., Citation2016; Igel & Szydlik, Citation2011).
Nevertheless, the current study makes an important contribution to the field of cross-national comparisons of the relationship between grandparenthood and depression. This is the first time that the topics have been compared across England, Europe and China, adding to a growing body of literature by showing that the complex relationship is related to macro-level factor such as a country’s income, as well as micro-level factors such as grandparents’ gender. This study has effectively used the Structural Ambivalence Theory and the Role Theory to explain the potential mechanisms of the different relationship between grandparenthood and depression across countries. Both researchers and policymakers should take into account the heterogeneous nature of grandparenthood, macro-level and micro-level factors when planning policies in order to improve the health and well-being of older people worldwide. Family and other policies involving older people need to be aware of the increasing importance of grandparents in providing childcare for their grandchildren, and take into account the impact of grandparenting on grandparents’ health. With policy reforms aimed at increasing the pension age being implemented worldwide, the stress resulting from becoming a grandparent and caring for grandchildren whilst working could increase if people retire at an older age. Higher income countries in particular should investigate policy instruments that might buffer the negative health impact of transitioning to grandparenthood. Particular attention should be devoted to grandmothers, who are more likely than grandfathers to experience depression when transitioning to grandparenthood.
Acknowledgements
This study used Gateway to Global Aging Data, produced by the Program on Global Aging, Health & Policy, University of Southern California. This study was approved by the University of Southampton’s Ethics Committee (ERGO II 61545). The author thanks Maria Evandrou and Athina Vlachantoni for their helpful comments that improved the manuscript.
Disclosure statement
The authors report no conflict of interest.
Additional information
Funding
References
- Arpino, B., Bordone, V., & Balbo, N. (2018). Grandparenting, education and subjective well-being of older Europeans. European Journal of Ageing, 15(3), 251–263. https://doi.org/10.1007/s10433-018-0467-2
- Arpino, B., & Gomez-Leon, M. (2020). Consequences on depression of combining grandparental childcare with other caregiving roles. Aging & Mental Health, 24(8), 1263–1270. https://doi.org/10.1080/13607863.2019.1584788
- Beaumaster, S., Chien, S., Lau, S., Lin, A., Phillps, D., Wilkens, J., Lee, J. (2018). Harmonised CHARLS documentation. http://charls.pku.edu.cn/uploads/document/harmonized_charls/application/Harmonized_CHARLS_C.pdf
- Boedeker, P. (2017). Hierarchical linear modeling with maximum likelihood, restricted maximum likelihood, and fully Bayesian estimation. Practical Assessment. Research, and Evaluation, 22(1), 2. https://doi.org/10.7275/5vvy-8613
- Bordone, V., & Arpino, B. (2019). Grandparenthood, grandchild care and depression among older people in 18 countries. Journal of Family Research, 31(2), 216–239. https://doi.org/10.3224/zff.v31i2.06
- Chen, F., & Liu, G. (2012). The health implications of grandparents caring for grandchildren in China. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 67(1), 99–112. https://doi.org/10.1093/geronb/gbr132
- Chin, W. Y., Choi, E. P. H., Chan, K. T. Y., & Wong, C. K. H. (2015). The psychometric properties of the Center for Epidemiologic Studies Depression Scale in Chinese primary care patients: Factor structure, construct validity, reliability, sensitivity and responsiveness. PLoS One, 10(8), e0135131. https://doi.org/10.1371/journal.pone.0135131
- Chung, S., & Park, A. (2018). The longitudinal effects of grandchild care on depressive symptoms and physical health of grandmothers in South Korea: A latent growth approach. Aging & Mental Health, 22(12), 1556–1563. https://doi.org/10.1080/13607863.2017.1376312
- Condon, J., Luszcz, M., & McKee, I. (2018). The transition to grandparenthood: A prospective study of mental health implications. Aging & Mental Health, 22(3), 336–343. https://doi.org/10.1080/13607863.2016.1248897
- Connidis, I. A., & McMullin, J. A. (2002). Sociological ambivalence and family ties: A critical perspective. Journal of Marriage and Family, 64(3), 558–567. https://doi.org/10.1111/j.1741-3737.2002.00558.x
- Cowgill, D. O. (1972). A theory of aging in cross-cultural perspective. In D. O. Cowgill & L. D. Holmes (Eds.), Aging and modernization. (pp. 1–14). Appleton-Century-Crofts.
- Crimmins, E. M., Kim, J. K., & Solé-Auró, A. (2011). Gender differences in health: Results from SHARE, ELSA and HRS. European Journal of Public Health, 21(1), 81–91. https://doi.org/10.1093/eurpub/ckq022
- Dewey, M. E., & Prince, M. J. (2005). Mental health. In A. Borsch-Supan (Ed.), Health, ageing and retirement in Europe. First results from the survey of health, ageing and retirement in Europe. (pp. 108–117). Mannheim Research Institute for the Economics of Ageing.
- Di Gessa, G., Glaser, K., & Tinker, A. (2016). The impact of caring for grandchildren on the health of grandparents in Europe: A lifecourse approach. Social Science & Medicine (1982), 152, 166–175. https://doi.org/10.1016/j.socscimed.2016.01.041
- Elff, M., Heisig, J. P., Schaeffer, M., Shikano, S. (2016). No need to turn Bayesian in multilevel analysis with few clusters: How frequentist methods provide unbiased estimates and accurate inference. In Annual Meeting of the European Political Science Association (pp. 1–50). European Political Science Association.
- Ermini, L., & Hendry, D. F. (2008). Log income vs. linear income: An application of the encompassing principle. Oxford Bulletin of Economics and Statistics, 70(supplement), 807–827. https://doi.org/10.1111/j.1468-0084.2008.00531.x
- Faraway, J. J. (2016). Extending the linear model with R: Generalized linear, mixed effects and nonparametric regression models. CRC press.
- Goode, W. J. (1960). A theory of role strain. American Sociological Review, 25(4), 483–496. https://doi.org/10.2307/2092933
- Hamer, M., Molloy, G. J., de Oliveira, C., & Demakakos, P. (2009). Leisure time physical activity, risk of depressive symptoms, and inflammatory mediators: The English Longitudinal Study of Ageing. Psychoneuroendocrinology, 34(7), 1050–1055. https://doi.org/10.1016/j.psyneuen.2009.02.004
- Hank, K., Cavrini, G., Di Gessa, G., & Tomassini, C. (2018). What do we know about grandparents? Insights from current quantitative data and identification of future data needs. European Journal of Ageing, 15(3), 225–235. https://doi.org/10.1007/s10433-018-0468-1
- Hox, J. (2002). Multilevel analysis: Techniques and applications. Psychology Press.
- Hughes, M. E., Waite, L. J., LaPierre, T. A., & Luo, Y. (2007). All in the family: The impact of caring for grandchildren on grandparents’ health. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 62(2), S108–S119. https://doi.org/10.1093/geronb/62.2.s108
- Igel, C., & Szydlik, M. (2011). Grandchild care and welfare state arrangements in Europe. Journal of European Social Policy, 21(3), 210–224. https://doi.org/10.1177/0958928711401766
- Jadhav, A., & Weir, D. (2018). Widowhood and depression in a cross-national perspective: Evidence from the United States, Europe, Korea, and China. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 73(8), e143–e153. https://doi.org/10.1093/geronb/gbx021
- Jappens, M., & Van Bavel, J. (2012). Regional family norms and child care by grandparents in Europe. Demographic Research, 27(4), 85–120. https://doi.org/10.4054/DemRes.2012.27.4
- Kim, H.-J., Kang, H., & Johnson-Motoyama, M. (2017). The psychological well-being of grandparents who provide supplementary grandchild care: A systematic review. Journal of Family Studies, 23(1), 118–141. https://doi.org/10.1080/13229400.2016.1194306
- McNeish, D. M., & Stapleton, L. M. (2016). The effect of small sample size on two-level model estimates: A review and illustration. Educational Psychology Review, 28(2), 295–314. https://doi.org/10.1080/00273171.2016.1167008
- Missinne, S., Vandeviver, C., Van de Velde, S., & Bracke, P. (2014). Measurement equivalence of the CES-D 8 depression-scale among the ageing population in eleven European countries. Social Science Research, 46(1), 38–47. https://doi.org/10.1016/j.ssresearch.2014.02.006
- Moore, S., & Rosenthal, D. (2017). Grandparenting: Contemporary perspectives. Routledge/Taylor & Francis Group.
- Munich Center for the Economics of Aging. (2020). SHARE release guide. http://www.share-project.org/fileadmin/pdf_documentation/SHARE_release_guide_7-1-1.pdf
- Neuberger, F. S., & Haberkern, K. (2014). Structured ambivalence in grandchild care and the quality of life among European grandparents. European Journal of Ageing, 11(2), 171–181. https://doi.org/10.1007/s10433-013-0294-4
- Neuberger, F. S., & Preisner, K. (2018). Parenthood and quality of life in old age: The role of individual resources, the welfare state and the economy. Social Indicators Research, 138(1), 353–372. https://doi.org/10.1007/s11205-017-1665-6
- Ni, Y., Tein, J.-Y., Zhang, M., Yang, Y., & Wu, G. (2017). Changes in depression among older adults in China: A latent transition analysis. Journal of Affective Disorders, 209, 3–9. https://doi.org/10.1016/j.jad.2016.11.004
- Phillips, D., Lin, Y.-C., Wight, J., Chien, S., Lee, J. (2017). Harmonized ELSA documentation. http://doc.ukdataservice.ac.uk/doc/5050/mrdoc/pdf/5050_harmonized_elsa_e.pdf
- Prince, M. J., Beekman, A. T., Deeg, D. J., Fuhrer, R., Kivela, S. L., Lawlor, B. A., Lobo, A., Magnusson, H., Meller, I., van Oyen, H., Reischies, F., Roelands, M., Skoog, I., Turrina, C., & Copeland, J. R. (1999). Depression symptoms in late life assessed using the EURO-D scale. Effect of age, gender and marital status in 14 European centres. The British Journal of Psychiatry : The Journal of Mental Science, 174(4), 339–345. https://doi.org/10.1192/bjp.174.4.339
- Program on Global Aging. (2018). The gateway to global ageing data. University of Southern California. https://g2aging.org/
- Rabe-Hesketh, S., & Skrondal, A. (2012). Multilevel and longitudinal modeling using Stata. STATA Press.
- Radloff, L. S. (1977). The CES-D Scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1(3), 385–401. https://doi.org/10.1177/014662167700100306
- Sascha, d B., Martijn, H., & Deeg, D. J. H. (2020). Macro-level determinants of post-retirement health and health inequalities: A multilevel analysis of 18 European countries. Social Science & Medicine (1982), 245, 112669https://doi.org/10.1016/j.socscimed.2019.112669
- Schwarz, B., Trommsdorff, G., Zheng, G., & Shi, S. (2010). Reciprocity in intergenerational support: A comparison of Chinese and German adult daughters. Journal of Family Issues, 31(2), 234–256. https://doi.org/10.1177/0192513X09347991
- Sieber, S. D. (1974). Toward a theory of role accumulation. American Sociological Review, 39(4), 567–578. https://doi.org/10.2307/2094422
- Silverstein, M., & Zuo, D. (2020). Grandparents caring for grandchildren in rural China: Consequences for emotional and cognitive health in later life. Aging & Mental Health. Advance online publication. https://doi.org/10.1080/13607863.2020.1852175
- StataCorp (2019). Stata statistical software: Release 16. StataCorp LLC.
- Van de Velde, S., Bracke, P., & Levecque, K. (2010). Gender differences in depression in 23 European countries. Cross-national variation in the gender gap in depression. Soc Sci Med), 71(2), 305–313. https://doi.org/10.1016/j.socscimed.2010.03.035
- Wang, S., & Mutchler, J. E. (2020). The implications of providing grandchild care for grandparents’ marital quality. Journal of Family Issues, 41(12), 2476–2501. https://doi.org/10.1177/0192513X20934845
- World Health Organisation. (2008). Integrating mental health into primary care: A global perspective. http://apps.who.int/iris/bitstream/10665/43935/1/9789241563680_eng.pdf
- Xu, H. (2019). Physical and mental health of Chinese grandparents caring for grandchildren and great-grandparents. Social Science & Medicine (1982), 229, 106–116. https://doi.org/10.1016/j.socscimed.2018.05.047
- Xu, Y., Yang, J., Gao, J., Zhou, Z., Zhang, T., Ren, J., Li, Y., Qian, Y., Lai, S., & Chen, G. (2016). Decomposing socioeconomic inequalities in depressive symptoms among the elderly in China. BMC Public Health, 16(1), 1214–1219. https://doi.org/10.1186/s12889-016-3876-1
- Zunzunegui, M. V., Minicuci, N., Blumstein, T., Noale, M., Deeg, D., Jylhä, M., & Pedersen, N. L., CLESA Working Group (2007). Gender differences in depressive symptoms among older adults: A cross-national comparison: The CLESA project. Social Psychiatry and Psychiatric Epidemiology, 42(3), 198–207. https://doi.org/10.1007/s00127-007-0158-3