
Abstract
Objectives: This study addresses the gendered risks of loneliness and depression in later life from a social exclusion perspective. Exclusion from social relations (ESR) in older age is an unwanted situation associated with increased loneliness and depressive symptoms, with gender differences in the perception of solitude, and the evaluation of existing social networks, potentially accounting for the increased susceptibility of older women.
Method: Secondary analyses was conducted in a sample of 60,918 participants in the Survey on Health, Aging and Retirement in Europe (SHARE). Older persons’ subjective perception of solitude (i.e. solitude satisfaction), and their satisfaction with established relations (i.e. network satisfaction), were examined in gender-stratified regression models, predicting loneliness and depressive symptomatology, controlling for network size, demographics, and health.
Results: There was no convincing evidence for significant associations between solitude satisfaction (SoS) and loneliness among older men, nor between network satisfaction (NeS) and loneliness for both genders. Low SoS and low NeS were independently associated with more depressive symptoms and an increased probability of depression, especially among older women. This vulnerability could not be attributed to increased loneliness, as only among older women, low SoS was associated with lower levels of loneliness, and lower levels of loneliness was anaemically associated with more depressive symptoms.
Conclusions: The perception of solitude, and the evaluation of social relations, are associated with gendered risks of depression among older persons who are challenged by objective and subjective ESR states.
Introduction
Older persons are a population at risk of exclusion from social relations (ESR), with demographic changes raising concerns that a greater number will be ‘socially and emotionally disconnected from adequate levels of intimate relationships, social networks, social support, and/or social opportunities’ (Aartsen et al., Citation2021). ESR in older age is associated with increased loneliness and more depressive symptoms (Berkman & Glass, Citation2000; Courtin & Knapp, Citation2017; Smith & Victor, Citation2019), emerging often as co-occurring and potentially overlapping aspects that affect older persons’ mental wellbeing (Cacioppo et al., Citation2010; Prince et al., Citation1999). Therefore, loneliness and the prevalence of depressive symptoms in older age are typically discoursed as collateral issues associated with the unmet social needs of older persons who are challenged by ESR states (Walsh et al., Citation2017).
Social networks are often quantified and typified based on objective (e.g. network size) and subjective (e.g. network quality) characteristics, with the literature providing inconsistent findings on their relative importance for the mental wellbeing of older persons (Courtin & Knapp, Citation2017; Litwin, Citation2011; Pinquart & Sörensen, Citation2000). For example, Litwin et al. (Citation2015) found that older persons who are subjectively satisfied with their established social relations (i.e. network satisfaction), as well as older persons who objectively have larger networks, experience fewer depressive symptoms. However, Cacioppo et al. (Citation2010) could not find evidence that older persons’ network size is longitudinally associated with depression, although, they argued that higher loneliness may predict adverse changes in depressive symptomatology.
Menec et al. (Citation2020) found that loneliness moderates the effects of objective ESR states (i.e. having few or no social ties) on the mental wellbeing of older persons. Using data from the Canadian Longitudinal Study of Aging (CLSA), they found that older persons who are excluded and lonely are more depressed than those who are excluded but not lonely. In addition, they found that older persons who are lonely but not excluded (i.e. challenged by subjective ESR states) are more depressed than those who are excluded but not lonely. Among all groups, those who were neither excluded nor lonely had the lowest levels of depressive symptomatology
Often coined as a paradox, loneliness is commonly observed among older persons who are embedded in a social network, even more so within cultures epitomized for the intimacy of social relations and for the density of older persons’ social networks. For example, older persons in Southern European have on average larger social networks than their counterparts in the Nordic countries, yet loneliness is more prevalent among older southern Europeans (Hansen & Slagsvold, Citation2016; Sundstrom et al., Citation2009; Tomini et al., Citation2016). Sundstrom et al. (Citation2009) argued that the compositions of older persons’ social networks are culturally bound, and therefore, their interpretation of loneliness is determined by culturally shaped expectations for social interaction, leading to the experience of subjective ESR states. Accordingly, Beridze et al. (Citation2020) examined the associations of loneliness and social isolation with the quality of life (QoL) of older persons in Spain and Sweden. In their study, social isolation was negatively associated with QoL in both countries, but loneliness was negatively associated with QoL only among the Swedish persons with higher levels of loneliness, but more uniformly so (i.e. across levels of loneliness) in Spain.
The intra-individual processes that modify feelings of loneliness among objectively excluded older persons have been rarely discussed, even though the subjective interpretation of solitude may lead to differential affective outcomes (Newall & Menec, Citation2019). Lay et al. (Citation2019) argued that there are two types of everyday solitude among older persons, one characterized by negative affect (negative affect solitude), and one characterized by calmness and near absence of negative affect (positive affect solitude). In their study of 100 older adults, Lay et al. (Citation2019) observed that almost 25% of the participants experienced solitude only positively, while the desire to spend time alone (but not their social network size) was associated with positive affect. Similar studies have shown that older persons who prefer their solitude over socializing, or those who cherish their low standards of sociability, may not feel lonely (Burger, Citation1995; Dykstra, Citation1995). However, other studies have shown that some objectively excluded older persons feel lonely, with no further emotional affliction observable (Burger, Citation1995; Toyoshima & Sato, Citation2017, Citation2019).
Previous studies on the gender-sensitive associations between ESR, loneliness, and depressive symptoms suggest critical accumulations of risks for the mental wellbeing of excluded older women. More precisely, the prevalence of both loneliness and depression is reported more frequently among older women than among older men (Castro-Costa et al., Citation2007; Courtin & Knapp, Citation2017; Dykstra, Citation1995; Prince et al., Citation1999). Older women have on average fewer financial and social resources, as well as more mobility limitations than older men, all factors that potentially affect their socialization and mental health (Goodman et al., Citation2015). Because women live longer than men, older women are more likely to experience widowhood, a condition that potentially leads to ESR in older age (Antonucci et al., Citation2001). Among widowed older women, good quality of existing relations has been associated with better mental health (Guma & Fernandez-Carro, Citation2021), but supporting a better social integration has been associated with improvements in depressive symptoms among older men but not among older women (Santini et al., Citation2016). Older women are more likely than older men to report network expansion over time (Schwartz & Litwin, Citation2018), yet older women assume more often than men caregiving roles with significant implications for their socialization and mental wellbeing (Bien et al., Citation2013).
Umberson and Karas Montez (Citation2010) argued that the risks of loneliness and depression are pronounced among older persons that are challenged by extreme objective ESR states. Similarly, Litwin and Levinsky (Citation2021) found that 8.5% of older persons who are ‘network-less’ were chronically isolated, and along with those moving from a close-family interpersonal environment to being ‘network-less’ (i.e. 19.1% of the ‘network-less’) have the highest levels of depressive symptoms. Pavlidis et al. (Citation2022) found that among older ‘network-less’ persons, lower solitude satisfaction (SoS) is associated with lower QoL, comparatively more so among older women. Although the ‘non-existence’ of loneliness within a proportion of older ‘network-less’ persons has been explained as the result of a sympathetic stance towards solitude (Menec et al., Citation2020; Newall & Menec, Citation2019), this assumption remains hitherto with limited empirical support, overlooking potential gender differences in this respect. Therefore, we examined the gendered associations of SoS with feelings of loneliness and depression among older ‘network-less’ persons.
Pavlidis et al. (Citation2022) found that most older persons in Europe (95%) are very satisfied with their social relations, but the minority with low network satisfaction (NeS) has significantly lower QoL. To our knowledge, research on the associations of NeS with the prevalence of depressive symptoms among older persons with small or larger networks is missing from the literature. Barger et al. (Citation2014) found that a perceived lack of support and contact frequency with network members are associated with depressive outcomes. In their study, subjective ESR states were examined in conventional terms, namely via normative and predefined assumptions about what relational aspects may bring fulfilment in older age (e.g. emotional closeness, perceived support). Yet, perceptual gaps between gerontology professionals and older persons themselves on what aspects of social relations bring fulfilment, as well as the potentially gendered proclivities in socialization needs, may pose a threat of homogenizing and delegitimatizing older persons’ preferences (Bailey & Marsden, Citation1999; Ost-Mor et al., Citation2021). In our study, we deviated from normative accounts of social relations, examining the gendered associations of loneliness and depressive symptoms with older persons’ subjective satisfaction with their established relations (i.e. with NeS).
The research questions leading to our examination were (i) whether the associations of SoS with loneliness and depressive symptoms among older ‘network-less’ persons are gendered, over and above other indicators of ESR in older age (i.e. retirement, living alone, widowhood, divorce), and (ii) whether the associations of NeS with loneliness and depressive symptoms are gendered among older persons embedded in a social network. The prevalence of depressive symptoms is qualitatively different from the prevalence of depression, as enduring a small number of depressive symptoms is common, whereas only a fraction of the population suffers from depression (Prince et al., Citation1999). Since older women are overrepresented among the depression affected, we examined whether the gendered risks of depression are associated with loneliness, SoS and NeS. We hypothesized that (i) lower SoS will predict independently higher levels of loneliness and more depressive symptoms among ‘network-less’ older persons, especially among older women, (ii) lower NeS will be associated with higher levels of loneliness and more depressive symptoms among older persons with a social network, especially among older women, and (iii) older ‘network-less’ persons with low SoS, as well as older persons with small networks and low NeS, are more likely to have depression than those with larger networks and high NeS, with an increased susceptibility among older women.
Method
Participants
Given the difficulties observed in the sampling capacity of large surveys to include socially excluded persons (Litwin et al., Citation2020; Newall & Menec, Citation2019), the current cross-sectional study opted to pool data from two waves of the Survey on Health, Aging and Retirement in Europe (SHARE), according to previous research (Pavlidis et al., Citation2022). The sample included unique respondents participating in the fourth or the sixth wave of SHARE (Börsch-Supan, Citation2019) collected in 2011 and 2015, respectively. The eight wave of the SHARE study was not included in the analyses, since data collection in this wave was interrupted due to the restrictions posed during the COVID-19 pandemic. The pandemic period has had significant implications for older persons’ sociability and mental health, and therefore this wave was excluded from the analyses. Other waves from the SHARE study were not included, as only the fourth, sixth, and eight wave had a dedicated module on social networks.
The sample was restricted to participants who completed information about depressive symptoms and loneliness and responded to the social network module themselves (N = 60,918). Approximately 61% of the sample came from the fourth wave, and 39% came from the sixth wave. For those who participated in both waves, we used data only from the fourth wave, so that no participant was represented in the sample twice. The respondents originated from 20 European countries, namely Austria, Germany, Sweden, the Netherlands, Spain, Italy, France, Denmark, Greece, Switzerland, Belgium, Israel, the Czech Republic, Poland, Luxemburg, Hungary, Portugal, Slovenia, Estonia, and Croatia. Information about the SHARE’ survey procedures (e.g. sampling methods, data collection methods, response rates) and its ethics approval can be found in Bergmann et al. (Citation2019) and on the official website of the survey (www.share-project.org/faqs/3-methodology.html). In the study sample, 43.9% were male and 56.1% were female. The pooled sample’s age distribution (Mage = 66.01, SD = 9.68, Range = 50–105) did not deviate significantly from that of the fourth wave (Mage = 65.97, SD = 9.84) and the sixth wave (Mage = 66.67, SD = 9.66). The demographics of the pooled sample disaggregated by gender are presented in .
Table 1. Frequency analyses for demographic, social, and health variables.
Measures
Social network
The size of older persons’ social network was assessed in SHARE by using a name generating inventory. Participants were asked to name up to six persons with whom they talked about important issues during the last year, using the probe question ‘Over the last 12 months, who are the people with whom you most often discussed important things? These people may include your family members, friends, neighbours, or other acquaintances’. Respondents were given the opportunity to list an additional person that was important for them for any other reason (Börsch-Supan, Citation2019). According to previous research (Litwin & Levinsky, Citation2021), participants who did not report any person in this inventory were considered as ‘network-less’. Given the distribution of the network size in the sample (see ), we created two additional categories representing older persons who had one or two members in their network (small networks), and those with three or more members in their social network (large networks).
Network satisfaction
For those reporting at least one person in their social network, NeS was assessed in SHARE using a single question ‘Overall, on a scale from 0 to 10, where 0 means completely dissatisfied and 10 means completely satisfied, how satisfied are you with the [relationship that you have with the person/relationships that you have with persons] we have just talked about?’ (Börsch-Supan, Citation2019). As observed in previous studies using SHARE data (Litwin et al., Citation2015), NeS is highly skewed in the sample, with 43% reporting to be completely satisfied with their network. Therefore, a dummy variable was created to represent low (0–6), medium (7–8), and high satisfaction (9–10).
Solitude satisfaction
For those who did not report even one person in their network (i.e. the ‘network-less’), SHARE used the probe ‘You indicated that there is no one with whom you discuss important matters, and no one who is important to you for some other reason. On a scale from 0 to 10, where 0 means completely dissatisfied and 10 means completely satisfied, how satisfied are you with this (situation)?’ The SoS scale has the same scoring principles as the NeS scale, allowing to compare the two groups in equal terms (Börsch-Supan, Citation2019). A dummy variable was created to represent low (0–6), medium (7–8), and high SoS (9–10).
Loneliness
Loneliness was measured using the short version of the Revised University of California at Los Angeles Loneliness scale (R-UCLA) (Hughes et al., Citation2004). The scale consists of three items asking about the frequency of feelings of lack of companionship, being left out, and isolation from others, with three available responses: hardly ever or never, some of the time, and often. The final score is a summation of the three items and has possible values between 3 and 9 (Börsch-Supan, Citation2019).
Depressive symptoms
The EURO-D 12-item scale was used to assess the existence of depressive symptoms. The scale uses 12 binary yes/no response items to yield a total score between 0 and 12. The items cover depression, pessimism, suicidality, guilt, sleep, interest, irritability, appetite, fatigue, concentration, enjoyment, and tearfulness during the last month. Higher scores in this scale indicate more depressive symptoms, with scores of four or higher considered consistent with the clinical manifestation of depression (Börsch-Supan, Citation2019; Prince et al., Citation1999). The Cronbach’s α for the EURO-D scale was reported in the range of 0.61–0.75 in previous studies using data from SHARE (Prince et al., Citation1999).
Demographics
Participants in the SHARE study were asked whether any other person was living in their household and the number of the household members. Household income was an imputed variable in euros, available in the ‘gv_imputation’ module of the SHARE database. Education represents the years of attending full-time education. Participants were also asked about their marital and employment status (Börsch-Supan, Citation2019).
Health
Participants in the SHARE study were asked about the chronic health conditions they have, about the limitations they experience with six activities of daily living (ADL), with seven instrumental activities of daily living (IADL), and whether they have any mobility limitations in ten activities (Börsch-Supan, Citation2019).
Data analysis plan
The data were analysed using SPSS v.27. A preliminary analysis on gender differences and associations in demographics, health, network size, SoS, NeS, and depressive symptoms, was conducted through t-tests and Pearson correlation analyses.
Separate linear regression models were constructed for ‘network-less’ men and women to examine (i) the independent predictive value of SoS on loneliness, and (ii) the independent predictive values of SoS and loneliness on depressive symptoms. Similarly, linear regression models were constructed separately for men and women who have a network, to examine (i) the independent predictive values of NeS and network size on loneliness, (ii) the independent predictive values of NeS, network size, and loneliness on depressive symptoms, and (iii) the potential moderation effect of NeS in the associations of network size with both loneliness and depressive symptoms. Following the recommendations of Frazier et al. (Citation2004), the moderation effect of NeS on the associations of network size with loneliness and depression was examined by including the interaction term of network size and NeS in an additional step in the respective regression models. In all regression models, demographic variables (i.e. age, education, living alone, income, marital status, employment status) and health variables (number of chronic conditions and mobility limitations, number of ADL and IADL difficulties), were added to the models in separate steps, preceding the social network variables in two separate, sequential steps.
Binary logistic regression analyses were conducted separately for men and women to examine the predicted probability of having four or more depressive symptoms on the EURO-D scale. The independent predictors in the models were loneliness and group membership in one of the network categories formed by network size, SoS, and NeS. These groups were (i) three groups of ‘network-less’ persons with either low, medium, or high SoS, (ii) three groups of older persons with small networks and either low, medium, or high NeS, and (iii) three groups and older persons having large networks with either low, medium, or high NeS. The probabilities of depression in the models were adjusted for the effects of demographic variables (i.e. age, education, living alone, income, marital status, employment status) and health variables (number of chronic conditions and mobility limitations, number of ADL and IADL difficulties).
Results
Preliminary analysis
The gender stratified mean scores in the EURO-D scale disaggregated by network category are presented in . Mean scores and standard deviations for all variables disaggregated by gender are presented in . Independent sample t-test revealed statistically significant gender differences in most demographic and health variables (see ). Compared to older men, older women reported larger social networks (t(60916) = −29.959, p = .000), higher NeS (t(60916) = −11.925, p = .000), more loneliness (t(60916) = −3.128, p < .050), and more depressive symptoms (t(60916) = −48.473, p =.000). There were no statistically significant gender differences in the mean scores of SoS (t(60916) = −.179, p > .050). Pearson correlation analysis revealed statistically significant associations between demographics and health variables with loneliness and EURO-D scores for both genders (see ). Loneliness was statistically significant associated with SoS for both men and women (rmen = .086, p < .050; rwomen = .167, p = .000), but NeS was statistically significant associated with loneliness only among men (rmen = −.014, p < .050; rwomen = −.007, p > .050). For both genders, SoS (rmen = −.181, p = .000; rwomen = −.269, p = .000) and NeS (rmen = −.126, p = .000; rwomen = −.117, p = .000) were statistically significant associated with EURO-D scores.
Figure 1. Mean unadjusted EURO-D scores, disaggregated by gender, network size, and levels of solitude satisfaction or network satisfaction. Note. SoS: solitude satisfaction; NeS: network satisfaction.
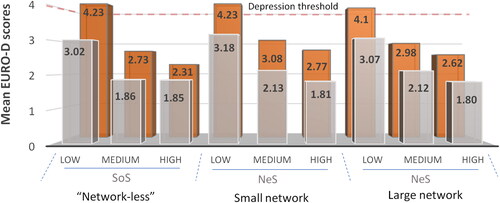
Table 2. Gender differences (t-test) and Pearson correlation coefficient for demographics, health, social relations, and outcome variables.
Gender-stratified associations of SoS and NeS with loneliness
Among ‘network-less’ older persons, gender-stratified multiple linear regression analyses on loneliness scores yielded models that were statistically significant for men (F(19, 973) = 3.687, p = .000, AR2 = 4.9%) and women (F(19, 921) = 4.009, p = .000, AR2 = 5.7%). For both men and women, the demographic variables explained most of the variation in loneliness scores (). Higher SoS emerged as a statistically significant independent predictor of higher loneliness for both men (β = .066, p < .050) and women (β = .139, p = .000). The variance explained from SoS on loneliness scores was higher among older women (R2change = 1.8%, p = .000) than among older men (R2change = .4%, p = .000).
Table 3. Regression analyses and standardized beta coefficients on loneliness scores among older persons with and without a network, with demographics, health variables, network size, and network or solitude satisfaction as predictors.
Among older persons who have a network, the gender-stratified multiple linear regression on loneliness scores yielded models that were statistically significant for men (F(21, 25721) = 34.245, p = .000, AR2= 2.6%) and women (F(21, 33239) = 40.623, AR2 = 2.4%, p = .000). The demographic variables explained the most variance in loneliness scores for both men and women (). Lower NeS emerged as an independent but weak predictor of higher loneliness for women (β = −.018, p < .050) but not for men (β = −.007, p > .050). A larger network size emerged as an independent but weak predictor of higher loneliness levels for both men (β = .014, p < .050) and women (β = .018, p < .050). The interaction term of network size and NeS did not emerge as an independent predictor of loneliness scores. Given the sample size and the small variance explained from NeS and network size on loneliness scores (i.e. for both genders R2change = .01%, p < .050), the results indicate trivial or no direct associations, nor a moderation effect of NeS in the association of network size with loneliness.
Gender-stratified associations of SoS and NeS with EURO-D scores
Among older ‘network-less’ persons, gender-stratified multiple linear regression on EURO-D scores yielded models that were statistically significant for men (F(20, 972) = 11.439, p = .000, AR2 = 17.4%) and women (F(20, 920) = 20.513, p = .000, AR2 = 29.3%). The health variables explained most of the variance in EURO-D scores (). Lower SoS emerged as an independent predictor of higher EURO-D scores for both men (β = −.137, p = .000) and women (β = −.150, p = .000), explaining additional variance in depressive symptoms among men (R2change = 1.8%, p = .000) and women (R2change = 2.4%, p = .000). A lower loneliness score emerged as an independent predictor of higher EURO-D scores only among older women (β = −.087, p < 0.50), explaining an additional variance of R2change = 0.7%.
Table 4. Regression analyses and standardized beta coefficients on EURO-D scores among older persons with and without a network, with demographics, health variables, loneliness, network size and network or solitude satisfaction as predictors.
Table 5. Binary logistic regression on the probability of having four or more depressive symptoms, adjusted for age, living alone, marital status, employment status, and health.
Among older persons who have a network, gender-stratified multiple linear regression analyses on EURO-D scores yielded models that were statistically significant for men (F(22, 25700) = 308.662, p < .001, AR2 = 20.8%) and women (F(22, 33238) = 443.683, p < .001, AR2 = 22.6%). Health variables explained most of the variance in EURO-D scores (). Lower NeS emerged as an independent predictor of higher EURO-D scores for both men (β = −.130, p = .000) and women (β = −.110, p = .000). Network size did not emerge as a statistically significant independent predictor of EURO-D scores for either gender. The network size*NeS interaction term was a weak but statistically significant independent predictor of EURO-D scores explaining almost no variance for older men (β = −.042, p =. 000, R2change = .00%, p = .000) or older women (β = −.020, p < 0.50, R2change = .00%, p < .050). Less loneliness emerged as an independent but weak predictor of higher EURO-D scores only among women (β = −.014, p < .050), explaining almost no additional variance (R2change = 0.0%, p < .050).
Gender-stratified probability of having depression
The binary logistic regression analyses separately for men and women examining the predicted probability of having depression among nine network categories yielded models that were statistically significant for men (χ2(28) = 3387.821, p = .000, Nagelkerke R2 = .196) and women (χ2(28) = 5474.595, p = .000, Nagelkerke R2 = .207). For both genders and compared to those with large networks and high NeS (), the models favoured the occurrence of depression among (i) older ‘network-less’ persons with low SoS (ORmen = 105%, ORwomen = 138%), (ii) older persons with small networks and low NeS (ORmen = 154%, ORwomen = 133%), and (iii) older persons with large networks and low NeS (ORmen = 146%, ORwomen = 173%). The models favoured the occurrence of depression to a (comparatively) lesser extend among older persons with moderate NeS within small networks (ORmen = 35%, ORwomen = 41%) and those with moderate NeS and large networks (ORmen = 53%, ORwomen = 44%). There was no evidence that the probability of depression was greater among older ‘network-less’ persons with moderate or high levels of SoS. Lower levels of loneliness emerged as an independent predictor of depression only among older women (B = −.024, p = .000).
Discussion
In this study, we examined the gendered associations of SoS and NeS with loneliness and depressive symptoms among older persons with none, small, or larger social networks. Similarly, the probability of depression (i.e. having four or more depressive symptoms) was compared among older persons with and without a social network, accounting for SoS and NeS as potential modifiers of these probabilities.
Supporting partly our study’s first hypothesis, lower satisfaction with being ‘network-less’ was associated with more depressive symptoms in older age. This association remained robust over and above the potential ‘depressive’ effects of retirement, solitary living, widowhood, divorce, and illness. Older women who regarded their solitude negatively had on average more than four depressive symptoms (), a threshold consistent with the clinical manifestation of depression (Prince et al., Citation1999). These results indicate a double jeopardy for the mental health of older ‘network-less’ women who are dissatisfied with their objective ESR state. Older women’s increased vulnerability was hardly attributable to loneliness, as opposingly to widely held assumptions (Menec et al, Citation2020; Newall & Menec, Citation2019), lower SoS among older women was an independent predictor of lower loneliness. This association was anaemically visible among older ‘network-less’ men, indicating gender differences in the co-occurrence of two seemingly antithetical experiences (i.e. low SoS and low loneliness).
A positive association between favourable evaluations of solitude with higher levels of loneliness, yet, less negative affect, is not an unprecedented finding in the literature (e.g. see Burger, Citation1995; Toyoshima & Sato, Citation2017, Citation2019). Although only substantiated as a plausible explanation for our empirical results, a positive association between SoS and loneliness may reflect an emotion-regulation strategy that embraces loneliness. Partial support for this assumption can be found in qualitative studies showing that embracing loneliness is a preferred strategy among older persons who cope with the emotional burden of objective ESR states (Kharicha et al., Citation2018, Citation2021; Wijesiri et al., Citation2019). Adding to the literature, the evidence of our study may indicate that such emotion-regulation strategy is predominately exercised among older ‘network-less’ women.
The second hypothesis of our study was partly supported, as independently from an older person’s gender and network size, higher NeS was associated with fewer depressive symptoms. This is consistent with the findings of Pavlidis et al. (Citation2022), who found that the QoL of older persons with low NeS is significantly lower than the QoL among those with high NeS. However, we did not find convincing evidence that older person’s lack of satisfaction with their social relations is associated with loneliness, nor an association between loneliness and depression. This may suggest that subjective ESR states (i.e. having low NeS) is interpreted differently than loneliness, probably reflecting a perceived lack of support, or conflict-generating ties within a social network (Barger et al., Citation2014; Litwin, Citation2011; Menec et al., Citation2020; Tucker, Citation2002, for a discussion see Rook, Citation2018).
Menec et al. (Citation2020) argued that older persons who are socially embedded but lonely, tend to report fewer positive interactions with their social network, less tangible and emotional support, and more desire for additional social activities. Theoretical perspectives on loneliness also describe the unmet social needs of older persons, based on discrepancies between the desired and achieved levels of social relations (social loneliness), or of intimacy levels (emotional loneliness) (Gierveld & Tesch-Römer, Citation2012). The lack of any association between NeS and loneliness in our study may suggest that the unifactorial structure of the R-UCLA loneliness scale in SHARE fails to bring forth these discrepancies at the aggregated level (Hughes et al., Citation2004; Trucharte et al., Citation2021). The culture-bound prevalence of loneliness within the European region (Sundstrom et al., Citation2009) may also suggest that the association of loneliness with NeS may emerge in some, but not in most of national contexts. Notwithstanding cultural differences however, the evidence of our study indicates that subjective ESR states in older age are as much ‘depressive’ as objective ESR states can be among those with low SoS, consistent with the findings of Menec et al. (Citation2020).
Supporting our third hypothesis, low SoS among ‘network-less’ older persons, as well as low NeS among the socially embedded sample of this study, predicted independently the probability of depression. Adding to the conclusions of Litwin and Levinsky (Citation2021), we found that objective ESR states does not constitute a stand-alone risk factor for depression in older age. Accounting for the potentially ‘depressive’ effects of retirement, solitary living, widowhood, divorce, and illness, the probability of depression is relatively high among older ‘network-less’ persons with low SoS but remains rather low among satisfied ‘network-less’ persons. In addition, on par with the increased probability of depression among ‘network-less’ persons with low SoS, the probability of depression is relatively high among socially embedded persons with low NeS and large social networks, especially among older women. Due to the cross-sectional design of this study, we cannot argue for any causational link between SoS, NeS, and the clinical manifestation of depression. However, the findings of our study suggests that simple measures of SoS and NeS are useful for the identification of vulnerable groups at-risk of depression in older age.
The findings of our study have practical implication, as they suggest that older ‘network-less’ women who are satisfied with their solitude may benefit from interventions that mitigate loneliness. However, efforts to expand social opportunities with the view of reducing their levels of loneliness remains a debatable course of action. Interventions targeting the expansion of existing networking opportunities may have more promising outcomes among older persons who endure their objective ESR states less readily, especially among older women with low SoS. However, relying solely to accounts of loneliness as to identify older women at-risk of depression may be less promising than commonly expected. Among older persons who are challenged by their subjective ESR states, exploring functional deficiencies in their social networks may lead to tailored interventions that address individualized and relational shortcomings. Given the complexities of social relations, it is rather unlikely that a general-purpose intervention would benefit older persons that are challenged by subjective ESR states.
The findings of this study should be considered according to the strengths and limitations of cross-sectional studies, including the inability to interpret a causational link. Being ‘network-less’ in this study did not signify isolation from any form of human contact. As the social network inventory used in SHARE asks about older adults’ confidants plus one person who is important for any other reason, this referred most probably to meaningful relations (Bailey & Marsden, Citation1999). The social relations established in the wider community (e.g. participation in clubs) may not be reflected here, although those relations may be equally important for the mental wellbeing of older persons. It is recommended that qualitative studies should seek for explanatory content to our study’s results, in regards with the unusual associations observed between SoS, NeS, loneliness, and depressive symptomatology. In addition, future studies on ageing using longitudinal designs could examine the disruptive effect of retirement on older persons’ social networks, and to that extend, the relevance of retirement to objective and subjective ESR states.
In conclusion, the subjective evaluation of solitude seems to modify the probability of depression among older persons who are challenged by objective ESR states. The probability of depression is high among older persons who are dissatisfied with objective ESR states, as well as among older persons who are challenged by subjective ESR states. These disadvantages are gendered and considerable, with the risk of depression summiting alarmingly high among older women who are either dissatisfied with their solitude, or with their social relations.
Ethics approval
Wave 4 of SHARE and the continuation of the SHARE project were reviewed and approved by the Ethics Council of the Max Planck Society. For more details on consent to participate and consent for publication, please see SHARE’s official website (www.share-project.org/faqs/3-methodology.html).
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Aartsen, M., Walsh, K., Villar, F., Lowenstein, A., Katz, R., Naim, S. P., Motel-Klingebiel, A., Wanka, A., Urbaniak, A., Hansen, T., & Vidovićová, L. (2021). Exclusion from social relations in later life and the role of gender: A heuristic model. Gender a Výzkum / Gender and Research, 22(1), 16–35. http://doi.org/10.13060/gav.2021.005
- Antonucci, T. C., Lansford, J. E., Schaberg, L., Baltes, M., Takahashi, K., Dartigues, J. F., Smith, J., Akiyama, H., & Fuhrer, R. (2001). Widowhood and illness: A comparison of social network characteristics in France, Germany, Japan, and the United States. Psychology and Aging, 16(4), 655–665. 10.1037/0882-7974.16.4.655
- Bailey, S., & Marsden, P. V. (1999). Interpretation and interview context: Examining the General Social Survey name generator using cognitive methods. Social Networks, 21(3), 287–309. https://doi.org/10.1016/S0378-8733(99)00013-1
- Barger, S. D., Messerli-Bürgy, N., & Barth, J. (2014). Social relationship correlates of major depressive disorder and depressive symptoms in Switzerland: Nationally representative cross sectional study. BMC Public Health, 14(1), 273. https://doi.org/10.1186/1471-2458-14-273
- Bergmann, M., Kneip, T., De Luca, G., & Scherpenzeel, A. (2019). Survey participation in the Survey of Health, Ageing and Retirement in Europe (SHARE), Wave 1-7. Based on Release 7.0.0. SHARE Working Paper Series 41-2019. SHARE-ERIC.
- Beridze, G., Ayala, A., Ribeiro, O., Fernández-Mayoralas, G., Rodríguez-Blázquez, C., Rodríguez-Rodríguez, V., Rojo-Pérez, F., Forjaz, M. J., & Calderón-Larrañaga, A. (2020). Are loneliness and social isolation associated with quality of life in older adults? Insights from Northern and Southern Europe. International Journal of Environmental Research and Public Health, 17(22), 8637–8614. https://doi.org/10.3390/ijerph17228637
- Berkman, L. F., & Glass, T. (2000). Social integration, social networks, social support, and health. Social epidemiology (Vol. 1, pp. 137–173). Oxford University Press.
- Bien, B., McKee, K. J., Döhner, H., Triantafillou, J., Lamura, G., Doroszkiewicz, H., Krevers, B., & Kofahl, C. (2013). Disabled older people’s use of health and social care services and their unmet care needs in six European countries. European Journal of Public Health, 23(6), 1032–1038. https://doi.org/10.1093/eurpub/cks190
- Börsch-Supan, A. (2019). Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 6. Release version: 7.1.0. SHARE-ERIC. Data set. 10.6103/SHARE.w6.710
- Burger, J. M. (1995). Individual differences in preference for solitude. Journal of Research in Personality, 29(1), 85–108. https://doi.org/10.1006/jrpe.1995.1005
- Cacioppo, J. T., Hawkley, L. C., & Thisted, R. A. (2010). Perceived social isolation makes me sad: 5-year cross-lagged analyses of loneliness and depressive symptomatology in the Chicago Health, Aging, and Social Relations Study. Psychology and Aging, 25(2), 453–463. https://doi.org/10.1037/a0017216
- Castro-Costa, E., Dewey, M., Stewart, R., Banerjee, S., Huppert, F., Mendonca-Lima, C., Bula, C., Reisches, F., Wancata, J., Ritchie, K., Tsolaki, M., Mateos, R., & Prince, M. (2007). Prevalence of depressive symptoms and syndromes in later life in ten European countries: The SHARE study. The British Journal of Psychiatry, 191(5), 393–401. https://doi.org/10.1192/bjp.bp.107.036772
- Courtin, E., & Knapp, M. (2017). Social isolation, loneliness and health in old age: A scoping review. Health & Social Care in the Community, 25(3), 799–812. https://doi.org/10.1111/hsc.12311
- Dykstra, P. A. (1995). Loneliness among the never and formerly married: The importance of supportive friendships and a desire for independence. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 50B(5), S321–S329.
- Frazier, P. A., Tix, A. P., & Barron, K. E. (2004). Testing moderator and mediator effects in counseling psychology research. Journal of Counseling Psychology, 51(1), 115–134. https://doi.org/10.1037/0022-0167.51.1.115
- Gierveld, D. J., & Tesch-Römer, C. (2012). Loneliness in old age in Eastern and Western European societies: Theoretical perspectives. European Journal of Ageing, 9(4), 285–295. https://doi.org/10.1007/s10433-012-0248-2
- Goodman, A., Adams, A., Swift, H. J. (2015). Hidden citizens: How can we identify loneliness in our communities? Technical report. The Campaign to End Loneliness, Kent, UK. https://kar.kent.ac.uk/57835/1/Hidden%20Citizens%20Research%20Report.pdf
- Guma, J., & Fernandez-Carro, C. (2021). Life goes on: The influence of the perceived quality of social relations on older women’s mental health after the loss of a partner in Europe. Aging & Mental Health, 25(1), 53–60. https://doi.org/10.1080/13607863.2019.1675141
- Hansen, T., & Slagsvold, B. (2016). Late-life loneliness in 11 European countries: Results from the generations and gender survey. Social Indicators Research, 129(1), 445–464. https://doi.org/10.1007/s11205-015-1111-6
- Hughes, M. E., Waite, L. J., Hawkley, L. C., & Cacioppo, J. T. (2004). A short scale for measuring loneliness in large surveys: Results from two population-based studies. Research on Aging, 26(6), 655–672. https://doi.org/10.1177/0164027504268574
- Kharicha, K., Manthorpe, J., Iliffe, S., Chew-Graham, C. A., Cattan, M., Goodman, C., Kirby-Barr, M., Whitehouse, J. H., & Walters, K. (2021). Managing loneliness: A qualitative study of older people’s views. Aging & Mental Health, 25(7), 1206–1208. https://doi.org/10.1080/13607863.2020.1729337
- Kharicha, K., Manthorpe, J., Iliffe, S., Davies, N., & Walters, K. (2018). Strategies employed by older people to manage loneliness: Systematic review of qualitative studies and model development. International Psychogeriatrics, 30(12), 1767–1781. https://doi.org/10.1017/S1041610218000339
- Lay, J. C., Pauly, T., Graf, P., Biesanz, J. C., & Hoppmann, C. A. (2019). By myself and liking it? Predictors of distinct types of solitude experiences in daily life. Journal of Personality, 87(3), 633–647. https://doi.org/10.1111/jopy.12421
- Litwin, H. (2011). The association between social network relationships and depressive symptoms among older Americans: What matters most? International Psychogeriatrics, 23(6), 930–940. https://doi.org/10.1017/S1041610211000251
- Litwin, H., & Levinsky, M. (2021). Always alone? Network transitions among detached older Europeans and their effects. Ageing and Society, 41(10), 2299–2215. https://doi.org/10.1017/S0144686X20000240
- Litwin, H., Levinsky, M., & Schwartz, E. (2020). Network type, transition patterns and well-being among older Europeans. European Journal of Ageing, 17(2), 241–250. https://doi.org/10.1007/s10433-019-00545-7
- Litwin, H., Stoeckel, K. J., & Schwartz, E. (2015). Social networks and mental health among older Europeans: Are there age effects? European Journal of Ageing, 12(4), 299–309. https://doi.org/10.1007/s10433-015-0347-y
- Menec, V. H., Newall, N. E., Mackenzie, C. S., Shooshtari, S., & Nowicki, S. (2020). Examining social isolation and loneliness in combination in relation to social support and psychological distress using Canadian Longitudinal Study of Aging (CLSA) data. PLos One, 15(3), e0230673–20. https://doi.org/10.1371/journal.pone.0230673
- Newall, N. E., & Menec, V. H. (2019). Loneliness and social isolation of older adults: Why it is important to examine these social aspects together. Journal of Social and Personal Relationships, 36(3), 925–939. https://doi.org/10.1177/0265407517749045
- Ost-Mor, S., Palgi, Y., & Segel-Karpas, D. (2021). Exploring gaps in positive solitude perceptions: Older adults vs. gerontology professionals. International Psychogeriatrics, 33(12), 1253–1211. 10.1017/S1041610220003555
- Pavlidis, G., Hansen, T., Motel-Klingebiel, A., & Aartsen, M. (2022). Network and solitude satisfaction as modifiers of disadvantages in the quality of life of older persons who are challenged by exclusion from social relations: A gender stratified analysis. Applied Research in Quality of Life, 1–17. https://doi.org/10.1007/s11482-022-10045-z
- Pinquart, M., & Sörensen, S. (2000). Influences of socioeconomic status, social network, and competence on subjective well-being in later life: A meta-analysis. Psychology and Aging, 15(2), 187–224. https://doi.org/10.1037/0882-7974.15.2.187
- Prince, M. J., Beekman, A. T., Deeg, D. J., Fuhrer, R., Kivela, S. L., Lawlor, B. A., Lobo, A., Magnusson, H., Meller, I., van Oyen, H., Reischies, F., Roelands, M., Skoog, I., Turrina, C., & Copeland, J. R. (1999). Depression symptoms in late life assessed using the EURO–D scale. The British Journal of Psychiatry, 174(4), 339–345. https://doi.org/10.1192/bjp.174.4.339
- Rook, K. S. (2018). Stressful aspects of older adults’ social relationships: Current theory and research. In Stress and coping in later-life families (pp. 173–192). Taylor & Francis.
- Santini, Z. I., Fiori, K. L., Feeney, J., Tyrovolas, S., Haro, J. M., & Koyanagi, A. (2016). Social relationships, loneliness, and mental health among older men and women in Ireland: A prospective community-based study. Journal of Affective Disorders, 204, 59–69. https://doi.org/10.1016/j.jad.2016.06.032
- Schwartz, E., & Litwin, H. (2018). Social network changes among older Europeans: The role of gender. European Journal of Ageing, 15(4), 359–367. 10.1007/s10433-017-0454-z
- Smith, K. J., & Victor, C. (2019). Typologies of loneliness, living alone and social isolation, and their associations with physical and mental health. Ageing and Society, 39(8), 1709–1730. https://doi.org/10.1017/S0144686X18000132
- Sundstrom, G., Fransson, E., Malmberg, B., & Davey, A. (2009). Loneliness among older Europeans. European Journal of Ageing, 6(4), 267. https://doi.org/10.1007/s10433-009-0134-8
- Tomini, F., Tomini, S. M., & Groot, W. (2016). Understanding the value of social networks in life satisfaction of elderly people: A comparative study of 16 European countries using SHARE data. BMC Geriatrics, 16(1), 203. https://doi.org/10.1186/s12877-016-0362-7
- Toyoshima, A., & Sato, S. (2017). Examination of the relationship between preference for solitude and emotional well-being after controlling for the effect of loneliness. Osaka Human Sciences, 3, 171–183.https://doi.org/10.4992/jjpsy.86.13234
- Toyoshima, A., & Sato, S. (2019). Examination of the effect of preference for solitude on subjective well-being and developmental change. Journal of Adult Development, 26(2), 139–148. https://doi.org/10.1007/s10804-018-9307-z
- Trucharte, A., Calderón, L., Cerezo, E., Contreras, A., Peinado, V., & Valiente, C. (2021). Three-item loneliness scale: Psychometric properties and normative data of the Spanish version. Current Psychology, 1–9. https://doi.org/10.1007/s12144-021-02110-x
- Tucker, J. S. (2002). Health-related social control within older adults’ relationships. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 57(5), P387–P395. https://doi.org/10.1093/geronb/57.5.P387
- Umberson, D., & Karas Montez, J. (2010). Social relationships and health: A flashpoint for health policy. Journal of Health and Social Behavior, 51(1_suppl), S54–S66. https://doi.org/10.1177/0022146510383501
- Walsh, K., Scharf, T., & Keating, N. (2017). Social exclusion of older persons: A scoping review and conceptual framework. European Journal of Ageing, 14(1), 81–98. https://doi.org/10.1007/s10433-016-0398-8
- Wijesiri, H. M. S., Samarasinghe, K., & Edberg, A. K. (2019). Loneliness among older people living in care homes in Sri Lanka. International Journal of Older People Nursing, 14(4), 1–11. https://doi.org/10.1111/opn.12253