
Abstract
Objectives: The aim was to explore adolescents’ beliefs and awareness regarding fertility and preconception health, as well as their views and experiences of information about fertility and preconception health directed at their age group.
Methods: We performed seven semi-structured focus group interviews among upper secondary school students (n = 47) aged 16–18 years in two Swedish counties. Data were analysed by qualitative content analysis.
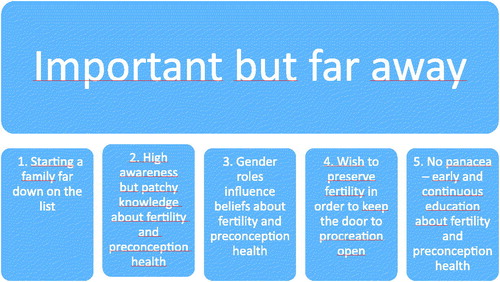
Results: One theme (‘important but far away’) and five categories (‘starting a family far down on the list’; ‘high awareness but patchy knowledge of fertility and preconception health’; ‘gender roles influence beliefs about fertility and preconception health’; ‘wish to preserve fertility and preconception health in order to keep the door to procreation open’; ‘no panacea – early and continuous education about fertility and preconception health’) emerged from the interviews. Participants recognised the importance of preconception health and were highly aware of the overall importance of a healthy lifestyle. Their knowledge, however, was patchy and they had difficulties relating to fertility and preconception health on a personal and behavioural level. Participants wanted more information but had heterogeneous beliefs about when, where and how this information should be given.
Conclusion: The adolescents wanted information on fertility and preconception health to be delivered repeatedly as well as through different sources.
摘要
目的:目的是探讨青少年对生育及孕前健康的信仰及认识, 以及他们针对其年龄组的生育和怀孕前健康信息的观点及经验。
方法:我们对瑞典两个县的16-18岁的高中生(n = 47)进行了7次半结构焦点小组访谈。采用定性内容分析法对数据进行分析。
结果:采访中出现了一个主题(“重要但很遥远”)及五个分类(“组建一个家庭在列表的后面”;“对生育及孕前健康意识很高但认识不全面”;“性别角色影响关于生育和孕前健康的理念”;“希望保持生育能力和孕前健康以确保生育能力的保持”;“没有万能灵药——关于生育和孕前健康的早期持续性的教育”)。参与者认识到孕前健康的重要性, 并高度认识到健康生活方式的整体的重要性。然而, 他们的知识是不全面的, 并且他们的个人和行为方面很难达到生育和孕前健康。参与者们想要更多的信息, 但是何时、何地以及如何提供这些信息有不同的看法。
结论:青少年希望通过不同的渠道来反复提供给他们生育及孕前健康方面的信息。
Introduction
Preconception health refers to health and lifestyle before pregnancy and is an important determinant of a healthy pregnancy and normal fetal development [Citation1,Citation2]. Today, a high proportion of men and women of childbearing age have lifestyle behaviours such as overweight/obesity and alcohol and tobacco use that are associated with increased fertility and childbearing risks [Citation1–4]. There is also a trend towards riskier sexual practices among young people, such as having a greater number of casual sexual partners and using condoms inconsistently [Citation5–7], leading to an increased rate of sexually transmitted infections (STIs) [Citation8,Citation9] constituting a potential threat to fertility and future childbearing [Citation9].
Additionally, there is a trend in many high-resource countries to postpone childbearing until an age when female reproductive capacity in particular has started to decline and obstetric and perinatal risks have begun to increase [Citation10–12]. Although multiple factors contribute to delayed childbearing, research shows that women and men, regardless of age and educational background, often underestimate the impact of female age-related fertility decline and overestimate the success of assisted reproductive technologies [Citation13–17].
Lifestyle and health behaviours are often established at a young age and can have a major impact on adolescents’ preconception health and future fertility. Preconception care interventions have, to a large extent, been designed for women with chronic conditions, or have focused on increasing preconception counselling [Citation18]. Lately, increased attention has been drawn to adolescents, who are now recognised as an important target group for preconception health promotion and fertility awareness interventions [Citation3,Citation19]. Nevertheless, there is limited knowledge about adolescents’ beliefs and their awareness of how age and lifestyle may impact fertility and preconception health, or about adolescents’ own preferences in terms of receiving information on these issues.
The aim of this study was to explore adolescents’ beliefs and awareness of fertility and preconception health. It was also to explore views and experiences of information on fertility and preconception health directed at the adolescent age group.
Methods
Ethical considerations
The study was carried out according to the Declaration of Helsinki and national guidelines [Citation20]. The Regional Ethical Review Board in Uppsala, Sweden (D.nr. 2016/468) approved the study. The adolescents were informed that participation was voluntary, that they could withdraw participation at any time without reason or negative consequence, and that only the researchers would have access to the data. They were also informed that all collected data would be presented at a group level and that no individual could be identified. Participants were provided with contact information for the researchers in case they had further questions. According to Swedish law, children from age 15 who understand what participation means have the right to give informed consent to take part in research studies [Citation20].
Study design
The study had an explorative, qualitative design using focus group interviews among students. The results are reported according to the consolidated criteria for reporting qualitative research (COREQ) [Citation21].
Setting, sample and procedure
We recruited students in two strategically chosen counties in the central regions of Sweden. Students aged 15–19 who attended upper secondary school, both vocational and theoretical programmes, were eligible to take part. Students were invited to participate by a key individual at each school, mainly a teacher in science or health education. Key individuals received information about the project and the study’s aim, before informing students attending their classes about the study. Students interested in sharing their views about fertility and preconception health were asked to take part in a focus group interview. The recruitment process is illustrated in .
Figure 1. Flowchart of recruitment process.
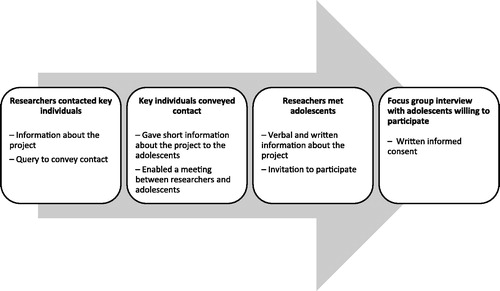
Interviews took place at a convenient location for the students. All interviews except one were carried out in the schools; one interview was undertaken at a researchers’ workplace (university). No one besides the researchers and the students were present during the interview. Every interview started with verbal information about the aim of the study and acknowledgment that participation was voluntary.
Students were asked to provide consent and fill in a short questionnaire providing demographic information and their previous knowledge of and beliefs about fertility and preconception health. In order to explore the adolescents’ beliefs, they were not provided with information about fertility and preconception health before the focus group interviews started or during the interviews. Both the key individuals and the students received a cinema voucher in return for their participation.
Interviews lasted about 60 min and were audio-recorded. The recordings were transcribed verbatim. We continued with data collection until information power, i.e., saturation was reached [Citation22]. The authors conducted interviews during the 2015–2016 school year. Two researchers were present at each interview: one moderator and one observer. The observer took notes, assisted with interviewing and made sure that all questions in the interview guide were discussed. All authors participated in two or more interviews.
Interview guide
A semi-structured interview guide was used. No formal pilot study was conducted. The main areas for questioning were the following: beliefs and awareness about fertility and preconception health; beliefs about the association between fertility and preconception health and lifestyle; and views and experiences about fertility and preconception health-related information. Follow-up questions and probes were also used, such as ‘Can you please explain more about that?’
Analysis
We analysed the interviews using qualitative latent content analysis [Citation23]. The first step was undertaken by all authors to avoid lone researcher bias. The transcripts were read several times to get an overall picture of the findings in relation to the overall aim. Notes, which functioned as the initial codes, were made in the margins of the transcripts. M. G. and J. S. performed the next step. Specifically, the codes were extracted from the transcripts and reduced by removing duplicates; thereafter, categorisation was done by grouping together overlapping or similar codes. The transcripts were then read again for verification, and codes were sorted into suitable categories. M. E. and M. M. validated the categorisation. Excel software was used to manage the data. Examples of the analytical process are presented in .
Table 1. Examples of the analytical process.
The analysis was rigorous and systematic. The researchers went back and forth to the transcripts to make sure that all data were thoroughly analysed and correctly interpreted. All researchers took part in discussing the categories and theme until a consensus was reached. The criteria for assessing the quality and trustworthiness of the conducted studies, as described by Guba and Lincoln [Citation24], were considered: credibility, dependability, confirmability and transferability. Results have been presented as close to the original interviews as possible; quotes are included for trustworthiness of the analysed data. Interviewees did not provide feedback on the transcripts or results, but validations were performed at the end of each interview when the researcher summarised what the adolescent had said to ensure that the information had been correctly understood. As in all qualitative research, the aim was not to generalise but to provide a better understanding of the participants’ perspective [Citation24].
An inductive approach was used since there is limited knowledge about adolescents’ beliefs, awareness and experiences regarding fertility and preconception health. We did not use any predetermined theory in the analysis, although the results are discussed from a public health perspective in light of the Health Belief Model (HBM) [Citation25]. The HBM is useful in understanding factors that influence health behaviour and is widely used in studies on health behaviour and adolescent sexual and reproductive health [Citation26,Citation27]. The HBM includes the following central constructs: perceived susceptibility, perceived severity, perceived benefit and perceived barriers. Furthermore, sociodemographic factors such as age, sex, ethnicity and parental educational level, as well as knowledge, are recognised as factors that can indirectly influence an individual’s behaviour. An important concept in the theory is cues to action, which can motivate individuals to alter their behaviour, and self-efficacy, i.e., the ability of an individual to perform a certain behaviour. The main limitation of the model is that it does not consider emotional or relational aspects involved in decisions about health behaviour [Citation25].
Results
We conducted seven focus group interviews among 47 upper secondary school students aged 17. The participants represented diverse schools, educational programmes, and socioeconomic backgrounds and areas. Their knowledge of fertility and preconception health was generally low ().
Table 2. Characteristics of and background knowledge regarding fertility and preconception health among participating students (n = 47).
Theme: important but far away
Most of the interviewees expressed and acknowledged the importance of receiving timely information about fertility and preconception health in order to preserve and maintain good reproductive health. However, they felt it was difficult to think about long-term health consequences during adolescence. Interviewees felt that there was a risk that information about fertility and preconception health during adolescence could create stress and result in mental distress, negatively affecting mental health. Despite this, gaining knowledge and information about fertility and preconception health would be better at a younger age as the consequences of receiving the information too late were considered more harmful given that lifestyle choices, such as smoking, could affect future fertility ().
Figure 2. Overview of the theme and categories.
Starting a family far down on the list (category 1)
Thinking about pregnancy planning was something that seemed far away and not what the participants felt motivated to think about at this time of life.
The person you are in about 10 years is not at all who you are today, so it feels a bit strange that I’m going to start planning and thinking today that “now you’re going to be fertile in 10 years”. If I start thinking now, it feels almost absurd. (Focus group 7)
Many students had plans and wanted to travel before starting university or work, and they shared a belief in the importance of having a stable financial situation as well as a stable relationship before starting a family.
That’s a bit tough because you … I’ve actually thought about this. You study … first, you go to high school, then maybe you want to have a year before university. I don’t know, to travel and such. Then you study a little longer. I don’t know how long I want to study. If you are going to be a doctor, it will take a really long time. And then you have to get a job. If you are pregnant then too … you have to be home for a year; there is no real end. (Focus group 6)
Another belief about fertility and preconception health was that finding the right partner with whom to start a family is difficult. Some students expressed opinions against starting a family, adding that the world was already overpopulated. The reasons for and possibility of becoming pregnant or having children in other ways had changed. Maybe having children was just a pattern that everybody followed, creating pressure that you had to have children.
Why do you want children? Because it has lost, or not lost [its purpose]; it has changed. Historically, children were needed to help the family; but now, why do you have children? Is it because of a pattern that you feel you need to follow? Maybe that creates pressure that you have to have children. I don’t know. (Focus group 6)
High awareness but patchy knowledge of fertility and preconception health (category 2)
Participants were well aware of the meaning of a healthy lifestyle in general and exemplified this by discussing the importance of good daily routines such as having healthy food, exercise, sleeping habits, and avoiding alcohol and smoking. However, they were not aware of the association between a healthy lifestyle and fertility and preconception health. This was something that they had not thought about before. They also expressed a lack of knowledge about how a healthy lifestyle is associated with fertility and preconception health.
But then, also, we say that if there is a person who smokes in their teens and gets this information, then maybe he or she doesn’t care so much because they think, “I’ll stop in a few years, so it’s OK”. But it may have to do with the fact that you have not developed this consequential thinking so much. (Focus group 6)
There was also a lack of knowledge about the negative impact of an unhealthy lifestyle and the significance of age and its possible effects on future ability to procreate.
I think that [daily] routines are pretty much that you … Like you have good routines and such, so I think it’s easier to have children and be fertile, yes. (Focus group 7)
It’s a bit hard to say, because we don’t know what we don’t know. (Focus group 4)
And age and such too; perhaps that is also important. (Focus group 5)
Gender roles influence beliefs about fertility and preconception health (category 3)
Participants emphasised that information and knowledge about fertility and preconception health were equally important for both sexes. Girls were considered to know more about fertility and preconception health compared with boys, but the general opinion was that girls and boys should receive the same information about fertility and preconception health.
I think girls know more than us [boys] anyway; that’s what I think. (Focus group 1)
It is better to talk to both [boys and girls] to ensure that everybody receives the same information. (Focus group 3)
The adolescents pointed out that gender roles had an impact, based on societal expectations of how men and women should and do relate to fertility and preconception health. They added that men are often excluded from spaces in which fertility and preconception health are discussed. This was considered problematic as both men and women are involved in pregnancy.
It’s hard for girls if they want to get pregnant while they are studying.
Exactly.
But it’s easier for boys: they can just keep on working, watch the child as it grows up; then they are on parental leave for, like, 6 months. It’s not exactly the same thing, right? A woman is gone from the job for almost 2 years. (Focus group 6)
It was also discussed that it is more difficult for boys to talk about fertility and preconception health and that boys often did not take discussions about these kinds of matters seriously, especially if girls were present. Boys felt that it was a little embarrassing to talk about wanting children in the future.
I feel that it is something you don’t want to talk about, that you don’t want to say “I want three children when I become…”. That’s embarrassing. It is not something you discuss at lunchtime. (Focus group 7)
Wish to preserve fertility and preconception health in order to keep the door to procreation open (category 4)
The adolescents believed that it was important to understand how lifestyles may affect future ability to procreate.
I think it’s important to get information, both on how to avoid it and how to make it easier if you really want to have children. (Focus group 3)
It was felt that young people should receive enough information in order to be able to make choices to avoid negative consequences in relation to future procreation. Most agreed that the ability to choose if and when to procreate is important even though those kinds of decisions were considered far into the future.
It‘s like this: the younger you are and the earlier you know that in the future you want children, maybe you start living healthier when you are young. (Focus group 5)
Yes, it’s unnecessary to close a door that you might really want to keep open. (Focus group 7)
No panacea – early and continuous education about fertility and preconception health (category 5)
Various beliefs and suggestions were shared regarding when and where information about fertility and preconception health should be addressed. Some adolescents felt that the earlier young people received information about fertility and preconception health the better, whereas others stated that receiving information too early would be too hard to understand. Some suggested that middle school would be an appropriate time (ages 10–12), while others thought junior high school (ages 13–15) would be better, and a few suggested senior high school (ages 16–18).
But it’s kind of like when you go to middle school, and when you become 15, 16, then maybe it’s good … Maybe it’s good to know about risks, since the older you become … That you split it up, so you don’t get it all at once. It feels like some stuff you don’t need to know when you are 15 years old. It could be better if you knew that later on; otherwise, you would just forget it. (Focus group 2)
Aspects such as gender and maturity were raised as important but difficult topics that should also be considered. Schools and youth health centres were suggested as the best places to obtain information about fertility and preconception health. When discussing who would be the most suitable person to educate young people in fertility and preconception health, it was felt best to have someone competent with a wide knowledge of fertility and preconception health. This type of information was viewed as rather private and personal, and could easily become embarrassing; thus, it was considered important to have someone who was used to talking to young people about fertility and preconception health, regardless of their profession. School nurses, midwives and trained teachers were considered appropriate professions to share information on the subject.
It should be a registered nurse or midwife. Someone who is expert in the field, who really knows and works with these questions all the time. I would like someone like that. Because then you know that this person is oriented in this specific topic and has knowledge about it. (Focus group 3)
Many also expressed the need to get accurate information on the Internet in general but also more specifically on social media and in different applications. In discussing lifestyles associated with risk, such as alcohol, tobacco, drugs and unsafe sex, the adolescents were found to have very heterogeneous experiences. The general opinion was, however, that these factors were not associated with fertility and preconception health. No one had received information about what lifestyle factors to consider when the time came for pregnancy planning. On the contrary, messages about how to avoid pregnancy and parenting at a young age had often been emphasised. This led them to believe that young people were extremely fertile; it was not even considered that pregnancy might not even be possible in the future. Several suggestions were made for improving sexuality education. It was emphasised that someone with experience of talking to young people and having knowledge about fertility and preconception health would be suitable for providing sexuality education.
But they mostly tell you “you should protect yourself”. They don’t tell you that much what you should do to become pregnant. It is more like “this is what you do if you don’t want to get pregnant”. They don’t say how you can become pregnant. (Focus group 5)
Discussion
Findings and interpretation and differences and similarities in relation to other studies
Our most important finding was that adolescents revealed both an interest in and need for information about fertility and preconception health. Participants felt that the notion of starting a family was in the distant future, stating similar prerequisites for parenthood as shown in previous studies [Citation15,Citation28,Citation29]; however, they still acknowledged that their current behaviour and lifestyle might have an impact on their chances of having children in the future. Nonetheless, the extent to which they perceived themselves as being susceptible to infertility and viewed infertility as a potential threat was not clear. Risk-taking behaviour is common during adolescence [Citation6,Citation9]. Because of biological reasons connected to their psychological development, adolescents might have more difficulties reflecting on long-term health-related consequences. Seen from the perspective of life course health development [Citation30], it is paramount that young people receive support in making healthy choices as early as possible. It is, therefore, particularly important to support adolescents in making informed choices about lifestyle with regard to their fertility and reproductive health. This question of public health has long-term consequences for both the individual and society in general. The patchy knowledge about fertility and preconception health among the adolescents in this study is consistent with previous studies carried out among this age group [Citation31,Citation32]. Inadequate knowledge about fertility and preconception health has also been found among young adults and university students [Citation15,Citation16,Citation28,Citation33,Citation34], which implies that knowledge does not necessarily increase with age, making it imperative to provide accurate information as early as possible.
The adolescents were often not aware of their knowledge gaps and showed difficulties applying their knowledge [Citation35]. This possibly creates a false sense of security regarding their fertility and preconception health. Future interventions targeting adolescents should, however, not be limited to increasing knowledge. An immense body of research shows that knowledge is not enough to alter behaviour. According to the HBM, factors such as perception of susceptibility, perception of severity, perceived benefits of lifestyle changes and self-efficacy are paramount to changing individual behaviour [Citation25]. Educational efforts and interventions should therefore aim at those aspects and must be tailored to the specific group or individual.
The health of a future child has been found to be a strong motivator for altering lifestyle habits in connection to pregnancy [Citation36]. By tapping into this motivator, interventions to improve fertility and preconception health might have greater potential to change behaviour. We also believe that interventions must include different perspectives regarding, for example, gender, (dis)ability, sexuality, health literacy, and socioeconomic and cultural background, in order to have a positive effect on supporting informed choices, help finding suitable strategies and possibly effect behavioural change. This is in line with UNICEF’s Convention on the Rights of the Child and is a matter of equality according to national Swedish public health policy. Several ways to apply person-centred care during discussion of this topic in health care encounters have been suggested [Citation17,Citation37].
The adolescents had heterogeneous beliefs about when, where and how education in fertility and preconception care should be given. In line with World Health Organization recommendations for sexuality education [Citation38], a recurrent view was that a single intervention was not enough; instead, continuous age-appropriate education and information from different sources were requested. The adolescents emphasised the importance of providing information without adding to the pressure and creating stress. This echoed previous findings that the sexuality education given in schools mainly focused on preventing STIs and pregnancies, rather than on promoting sexual and reproductive health [Citation39]. To this end, a plethora of interventions to avoid unintended pregnancies among adolescents have been presented [Citation40], but less effort has been placed on sexual and reproductive health promotion. Since it is known that overweight/obesity and alcohol and tobacco use are associated with increased fertility and childbearing risks [Citation1–4], it is important that young women and men receive this information early on in life, in order to be given better opportunities to make healthy choices. We believe that while it is important to prevent unintended and teenage pregnancies, efforts should also be made at preventing postponed parenthood and improving preconception health.
Relevance of the findings: implications for clinicians and policy-makers
Neither peers nor parents were mentioned as common or useful sources of information about fertility and/or preconception health. As adolescence is a time when social norms and peers are most important, it was surprising that peers were not mentioned [Citation23]. Not mentioning parents as a source of information was, however, expected, since many adolescents start to develop autonomy in relation to their parents in general but also regarding information seeking and health consultations. It is, therefore, important that health centres directed towards adolescents are easily accessible, visible and appealing to their target group. The young men in our study felt that youth health centres were not a natural source of information for them. This corresponds well with national surveys reporting that approximately 85% of all visitors to youth health centres in Sweden are female. Clearly other alternatives that appeal to male adolescents should be found.
Unanswered questions and future research
The Internet was mentioned as an important source of information and has been found to be an efficient way of increasing knowledge and changing fertility beliefs, albeit for a short interval [Citation41]. Although searching the Internet for preconception care may still result in poor and inaccurate information [Citation42], preconception health is a rising field of interest. The number of websites addressing preconception health is steadily growing [unpublished data]. It is important that efforts to increase knowledge also include improving online information. This may be particularly important for sexual- and gender-minority adolescents [Citation43]. Providing fertility- and preconception health-related information is a necessity for informed choices and a matter of equality. Thus, to increase equality in line with Swedish public health goals, all children and adolescents should be given the same opportunity to make informed choices in life. Previous research indicates, however, that health literacy, i.e., the ability to access, understand, value and use health information, is lower among vulnerable groups such as immigrants [Citation44]. Nevertheless, providing equal information might contribute to improved awareness, increased knowledge and, in the end, promote fertility and preconception health among youth.
Strengths and limitations of the study
Qualitative methods with an inductive approach were used since there was no previous knowledge about adolescents’ experiences and their views on fertility and preconception health information for their age group in Sweden. A focus group creates a non-judgemental environment and can encourage participants to share their views without the need for consensus. Lifestyle habits, reproduction, fertility and preconception health might be sensitive subjects to discuss. Thus, there were advantages to discussing these topics in a group setting since participants gave one another mutual support and individuals could choose when to speak. We found the adolescents to be open minded, empathetic and tolerant regarding beliefs and statements expressed during the interviews. They supported each other and had mutual respect for differing opinions. The interviewers (the authors) are registered midwives and specialist nurses, as well as researchers in the fields of reproductive health and adolescent health. This might have contributed to a willingness among the participants to share their views on these subjects during the interviews.
The focus group interviews with 47 adolescents were considered sufficient in order to reach information power and to provide a better understanding of the participants’ perspectives, which is considered to be a goal in qualitative research. As in all qualitative research, the aim was not to generalise; however, the results may be transferable to similar settings [Citation22,Citation24].
The study participants were from a wide range of schools in different socioeconomic and geographical areas, and participants attended both university preparatory and vocational programmes. Even though sexuality and relationship education has been mandatory in Swedish schools since 1955, overall knowledge about fertility and preconception health was low among participants; thus, the results are wide but lack depth in some areas. Moreover, compared with individual interviews, focus group interviews might not be as efficient in covering maximum depth on a particular issue. However, the adolescents were engaged in discussing the topic and believed it to be important.
Conclusions
Adolescents recognised the importance of preserving fertility and preconception health and were highly aware of the overall importance of a healthy lifestyle. However, their knowledge was patchy and they had difficulties relating to it on a personal and behavioural level. More information was wanted, but they had heterogeneous beliefs about when, where and how it should be given.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Moos MK, Dunlop AL, Jack BW, et al. Healthier women, healthier reproductive outcomes: recommendations for the routine care of all women of reproductive age. Am J Obstet Gynecol. 2008;199:S280–S289.
- Centers for Disease Control and Prevention. Recommendations to improve preconception health and health care – United States: a report of the CDC/ATSDR Preconception Care Work Group and the Select Panel on Preconception Care. MMWR Recomm Rep. 2006;55:1–23.
- World Health Organization (2013). Meeting to develop a global consensus on preconception care to reduce maternal and childhood mortality and morbidity. Available from: http://apps.who.int/iris/bitstream/10665/78067/1/9789241505000_eng.pdf?ua=1 (accessed 20 November 2017).
- The GBD 2015 Obesity Collaborators, Afshin A, Forouzanfar MH, Reitsma MB, et al. Health effects of overweight and obesity in 195 countries over 25 years. N Engl J Med. 2017;377:13–27.
- Herlitz CA, Forsberg M. Sexual behaviour and risk assessment in different age cohorts in the general population of Sweden (1989–2007). Scand J Public Health. 2010;38:32–39.
- Stenhammar C, Ehrsson YT, Akerud H, et al. Sexual and contraceptive behavior among female university students in Sweden – repeated surveys over a 25-year period. Acta Obstet Gynecol Scand. 2015;94:253–259.
- Horan SM, Cafferty LA. Condom communication: reports of sexually active young adults’ recent messages with new partners. J Health Commun. 2017;22:763–771.
- Public Health Agency of Sweden. Chlamydia infection. Annual report 2014;. Available from: https://www.folkhalsomyndigheten.se/folkhalsorapportering-statistik/statistikdatabaser-och-visualisering/sjukdomsstatistik/klamydiainfektion/kommentarer-och- specialstatistik/2014/ (accessed 25 October 2017).
- Unemo M, Bradshaw CS, Hocking JS, et al. Sexually transmitted infections: challenges ahead. Lancet Infect Dis. 2017;17:e235–e279.
- Luke B, Brown MB. Elevated risks of pregnancy complications and adverse outcomes with increasing maternal age. Hum Reprod. 2007;22:1264–1272.
- Jolly M, Sebire N, Harris J, et al. The risks associated with pregnancy in women aged 35 years or older. Hum Reprod. 2000;15:2433–2437.
- Snijders RJ, Sundberg K, Holzgreve W, et al. Maternal age- and gestation-specific risk for trisomy 21. Ultrasound Obstet Gynecol. 1999;13:167–170.
- D'Onofrio BM, Rickert ME, Frans E, et al. Paternal age at childbearing and offspring psychiatric and academic morbidity. JAMA Psychiatry. 2014;71:432–438.
- Mills M, Rindfuss RR, McDonald P, et al. Why do people postpone parenthood? Reasons and social policy incentives. Hum Reprod Update. 2011;17:848–860.
- Skoog Svanberg A, Lampic C, Karlström P-O, et al. Attitudes towards parenthood and awareness of fertility among postgraduate students in Sweden. Gen Med. 2006;3:187–195.
- Peterson BD, Pirritano M, Tucker L, et al. Fertility awareness and parenting attitudes among American male and female undergraduate university students. Hum Reprod. 2012;27:1375–1382.
- Kudesia R, Talib HJ, Pollack SE. Fertility awareness counseling for adolescent girls. Guiding conception: the right time, right weight, and right way. J Pediatr Adolesc Gynecol. 2017;30:9–17.
- Lassi ZS, Dean SV, Mallick D, et al. Preconception care: delivery strategies and packages for care. Reprod Health. 2014;11:S7.
- Mumford SL, Michels KA, Salaria N, et al. Preconception care: it's never too early. Reprod Health. 2014;11:73.
- CODEX (2015). CODEX rules and guidelines for research. Available from: www.codex.vr.se/en/manniska1.shtml (accessed 25 October 2017).
- Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19:349–357.
- Malterud K, Siersma VD, Guassora AD. Sample size in qualitative interview studies: guided by information power. Qual Health Res. 2016;26:1753–1760.
- Burnard P, Gill P, Stewart K, et al. Analysing and presenting qualitative data. Br Dent J. 2008;204:429–432.
- Lincoln YS, Guba EG, Fourth generation evaluation; 1989. Newbury Park, CA: Sage.
- Champion VL, Sugg Skinner, C, The Health Belief Model. In: Glantz K, Rimer BK, Viswanath K, eds. Health behavior and health education: theory, research, and practice, 4th ed; 2008. San Francisco, CA: Jossey-Bass.
- Underwood NL, Weiss P, Gargano LM, et al. Human papillomavirus vaccination among adolescents in Georgia. Hum. Vaccin Immunother. 2015;11:1703–1708.
- Grandahl M, Rosenblad A, Stenhammar C, et al. School-based intervention for the prevention of HPV among adolescents: a cluster randomised controlled study. BMJ Open. 2016;6:e009875.
- Tydén T, Skoog Svanberg A, Karlström P-O, et al. Female university students’ attitudes to future motherhood and their understanding about fertility. Eur J Contracept Reprod Health Care. 2006;11:181–189.
- Testa MR. Childbearing preferences and family issues in Europe: EU25. Special Eurobarometer no. 253. Vienna: European Commission, Vienna Institute of Demography; Austrian Academy of Sciences 2006.
- Halfon N, Hochstein M. Life course health development: an integrated framework for developing health, policy, and research. Milbank Q. 2002;80:433–479.
- Quach S, Librach C. Infertility knowledge and attitudes in urban high school students. Infertility. Fertil Steril. 2008;90:2099–2106.
- Trent M, Millstein SG, Ellen JM. Gender-based differences in fertility beliefs and knowledge among adolescents from high sexually transmitted disease-prevalence communities. J Adolesc Health. 2006;38:282–287.
- Bretherick K, Fairbrother N, Avila L, et al. Fertility and aging: do reproductive-aged Canadian women know what they need to know? Fertil Steril. 2010; 93:2162–2168.
- Rovei V, Gennarelli G, Lantieri T, et al. Family planning, fertility awareness and knowledge about Italian legislation on assisted reproduction among Italian academic students. Reprod Biomed. 2010;20:873–879.
- Littleton FK. How teen girls think about fertility and the reproductive lifespan. Possible implications for curriculum reform and public health policy. Hum Fertil.2014;17:180–187.
- Atkinson L, Shaw RL, French DP. Is pregnancy a teachable moment for diet and physical activity behaviour change? An interpretative phenomenological analysis of the experiences of women during their first pregnancy. Br J Health Psychol. 2016;21:842–858.
- Stern J, Larsson M, Kristiansson P, et al. Introducing reproductive life plan-based information in contraceptive counselling: an RCT. Hum Reprod. 2013;28:2450–2461.
- World Health Organization Regional Office for Europe and BZgA (2010). Standards for sexuality education in Europe – a framework for policy makers, educational and health authorities and specialists. Available from: www.oif.ac.at/fileadmin/OEIF/andere_Publikationen/WHO_BZgA_Standards.pdf (accessed 25 October 2017).
- Ekstrand M, Engblom C, Larsson M, et al. Sex education in Swedish schools as described by young women. Eur J Contracept Reprod Health Care. 2011;16:210–224.
- Oringanje C, Meremikwu MM, Eko H, et al. Interventions for preventing unintended pregnancies among adolescents. Cochrane Database Syst Rev. 2016;2:CD005215.
- Daniluk JC, Koert E. Fertility awareness online: the efficacy of a fertility education website in increasing knowledge and changing fertility beliefs. Hum Reprod. 2015;30:353–363.
- Agricola E, Gesualdo F, Pandolfi E, et al. Does Googling for preconception care result in information consistent with international guidelines: a comparison of information found by Italian women of childbearing age and health professionals. BMC Med Inform Decis Mak. 2013;13:25–14.
- Steinke J, Root-Bowman M, Estabrook S, et al. Meeting the needs of sexual and gender minority youth: formative research on potential digital health interventions. J Adolesc Health. 2017;60:541–548.
- Wångdahl J, Lytsy P, Mårtensson L, et al. Health literacy among refugees in Sweden - a cross-sectional study. BMC Public Health. 2014;14:1030.