
Abstract
This prospective study aimed to investigate the relationship between metabolic syndrome (Met S) and premature ejaculation (PE) among men. The study included 300 consecutive male patients (53.6 y ± 8.7) who attended the urology clinic (December 2013–September 2014), mostly complaining of renal/ureteric calculi. A diagnostic approach was undertaken to include demographics, clinical features and laboratory investigations of the study subjects. Both erectile function and PE were evaluated using the International Index of Erectile Function (abridged form, IIEF-5) and Premature Ejaculation Diagnostic Tool (PEDT) questionnaires, respectively. Results identified 182 (60.7%) men had Met S. Prevalence of PE was significantly higher in the subjects with Met S than the controls (35.2% vs 7.6%, p < 0.001). Patients with Met S and PE had significantly higher PEDT scores (15.4 vs 6.7), smaller waist circumference (108.3 cm vs 111.5 cm) and higher fasting blood sugar (187 mg% vs 161 mg%) than those with no PE (p < 0.001, 0.047 and 0.019, respectively). The other variables including IIEF-5 score, body mass index, serum triglycerides and high-density lipoprotein (14.98 vs 16.8, 30.6 vs 31.5, 192.9 mg% vs 178.1 mg% and 37.4 mg% vs 36.2 mg%, respectively) did not reveal significant differences. Both systolic hypertension and erectile dysfunction (ED) had significant associations (p = 0.047 and <0.001, respectively) with PE in Met S. In conclusion, PE has a high prevalence in Met S. Patients with Met S should be questioned about PE. Both ED and systolic hypertension may be associated with PE. Prevention of Met S should be considered, and this may be of help to decrease the prevalence of PE.
Introduction
According to The Diagnostic and Statistical Manual of Mental Disorders [Citation1], premature ejaculation (PE) is defined as “a persistent or recurrent pattern of ejaculation occurring during partnered sexual activity within approximately 1 minute following vaginal penetration and before the individual wishes it”. PE has recently received considerable attention on both clinical and research levels as it can adversely affect the quality of life of both partners [Citation2]. It is considered recently as the most common sexual dysfunction in sexually active men [Citation3]. Studies have proposed association of PE with a number of risk factors, including diabetes [Citation4,Citation5], anxiety, depression [Citation6], prostatitis [Citation7] and erectile dysfunction (ED) [Citation8,Citation9].
To date, metabolic syndrome (Met S) is getting increased attention [Citation10]. It is a collection of health disorders which include insulin resistance, central obesity, systemic inflammation, endothelial dysfunction and atherogenic dyslipidemia [Citation11]. These maladies increase the risk of heart disease, diabetes and stroke [Citation12]. A man is considered to have the Met S when three or more of these listed medical states are existent: blood pressure ≥130/85 mmHg, waist circumference (WC) >102 cm, triglyceride (TG) level ≥150 mg%, high-density lipoprotein (HDL) <40 mg% and fasting blood sugar (FBS) >110 mg% [Citation13].
Recent studies identified a higher prevalence of ED among patients with Met S [Citation14,Citation15]. Several components of Met S were also found to represent risk factors for ED [Citation14,Citation16]. Although a big body of evidence has clearly identified the interrelationship of ED and PE [Citation8,Citation9], PE did not receive the same attention like ED during the study of the patients with Met S. Knowledge is still lacking about the real prevalence of PE in such patients, and the impact of different components of Met S on this ejaculatory disorder.
Therefore, the goal of the current study was to determine the prevalence of PE among men with Met S, ascertain the associated medical conditions to PE and describe the patients’ sociodemographic characteristics.
Materials and methods
Study design
The present study is a prospective controlled study. A total of 300 consecutive male patients (53.6 y ± 8.7) who attended the urology outpatient clinic at the Alexandria Faculty of Medicine, Alexandria, Egypt from December 2013 to September 2014 were included. All patients were adults and engaged in heterosexual relationships. Their initial complaints were discomfort/pain in loin. This was mostly related to renal/ureteric calculi. Other less frequent causes were diagnosed as either urologic (hydronephrosis due to congenital pelvi-ureteric junction obstruction) or non-urologic (muscle/skeletal or colonic) pathology. Exclusion criteria included patients with lower urinary tract disorders and those with severe physical (e.g. renal failure) or mental illness which may affect the sexual function. Exclusion criteria also included any intake of medications for ED or PE. Before launching this research work, an informed consent was signed by every patient. The protocol of the study was approved by the institutional review board.
Study work-up
All patients underwent full history taking, which covered personal, medical, lifestyle aspects and sociodemographics which entailed data about the socioeconomic condition, smoking, alcohol intake and body mass index (BMI). Socioeconomic condition (SEC) could be indicated by education and income [Citation17]. According to their SEC, the studied subjects were categorized into three classes (low, middle or high). Body mass index (BMI) was estimated by dividing the weight (kg) by the square of height (m). The presence of Met S was determined according to the National Cholesterol Education Program-Adult Treatment Panel III (NCEP-ATP-III) guidelines [Citation13]. The syndrome would be existent when a patient has three or more of the following criteria: blood pressure ≥ 130/85 mmHg, WC > 102 cm (man), TG level ≥ 150 mg%, HDL < 40 mg% and FBS > 110 mg%.
Erectile function was evaluated using the Arabic version [Citation18] of the abridged form of International Index of Erectile Function (IIEF-5) [Citation19]. IIEF-5 is a simplified brief validated questionnaire which has been recently introduced to diagnose ED. It has proved to be specific and sensitive scale for use in the clinical setting [Citation19]. According to the score of the IIEF-5, ED could be severe (1–7), moderate (8–11), mild to moderate (12–16), mild (17–21) or absent (22–25). PE was assessed by means of Premature Ejaculation Diagnostic Tool (PEDT) [Citation20]. PEDT consists of five questions connected to PE control, PE frequency, ejaculation with minimal stimulation, distress and difficulty with the sexual partner. Questions in PEDT are scored between 0 and 4, yielding a minimum score of 0 and maximum of 20. Based on this PEDT scoring, the patients could have no PE (score ≤ 8), probable PE (score 9–10) or definite PE (score ≥ 11). To avoid inflating the prevalence rate of PE in this study, we did not include the subjects who were ascribed as “probable” premature ejaculators into the subgroups containing the definite PE. These subjects’ scores are not “clear-cut”, and the subjects should be directed for further assessment before a final diagnosis is made. This was recommended by the workers who invented the PEDT for the first time [Citation20]. In this study, we estimated only the prevalence rate of probable PE for the reader’s interest.
All participants in the study, then, underwent a physical examination with special emphasis on genital checkup and estimation of WC and blood pressure. WC was estimated in supine position at the level of umbilicus with the person breathing silently while blood pressure was measured after 30 minutes rest during which smoking and drinking caffeinated beverages were not allowed. Laboratory assessment of overnight FBS, serum TG and HDL was done.
Statistical analyses
The SPSS program for Windows Release 16 (SPSS Inc., Chicago, IL) was used to analyze the data. Descriptive statistics (mean and standard deviation) for numerical study variables were recorded. Distribution of quantitative variables was tested using Levene’s test. As data distribution was not uniform, Mann–Whitney test was used to compare between means of each variable in the different subgroups of the study. Prevalence and scoring of PE as related to the number of Met S elements were studied using chi-square test and one-way ANOVA, respectively. The associations of PE with each of the independent variables in the study were assessed using a chi-square test for univariate analysis after putting these variables as categorical data. Any resulting significant association was included as continuous data in binary logistic regression to guess if it could represent a possible predictor for PE in men with Met S. A p values was significant when it was <0.05.
Results
Prevalence of definite PE in the study groups
The patients in the current study (n = 300) were divided into two groups according to presence/absence of Met S. Group I contained 182 patients with Met S and group II had 118 patients without Met S (controls). In the Met S group, the number (%) of the subjects with definite PE, probable PE and no PE were 64 (35.2), 42 (23.1) and 76 (41.7), respectively while in the control group, these categories were 9 (7.6), 18 (15.3) and 91 (77.1), respectively. The prevalence of definite PE was significantly higher among the patients with Met S than the controls (35.2% vs 7.6%, respectively, p < 0.001). Then, exclusion of men with probable PE was done. This made the group I and group II consisting of 140 and 100 subjects, respectively for subsequent data analysis (vide infra).
Demographics of the study subjects
The comparison between the participants’ ages with and without PE in the two study groups (with Met S/controls) indicated no significant difference (p = 0.75, p = 0.28, respectively). Within either group, the age was also matched among the patients with and without PE with no significant difference (p = 0.12, the Met S group and 0.77, the control group, ). The number of smokers was higher in the subjects with PE than with no PE in the two study groups, although the difference was not significant (p = 0.48, the Met S group and p = 0.11, the control group, ). All the subjects of this study were non-drinkers. SEC, in general, seemed similar (p = 0.62, ) in men with/without PE. According to the class of SEC, most cases with or without PE belonged to the middle class () with nearly similar dissemination (p = 0.9). Patients of the low class came next with no difference between those with and without PE (p = 0.99). The high class contained the fewest number of cases with nearly comparable distribution (p = 0.63). We could not analyze the SEC in the control group due to the missing data of a substantial number of its participants. BMI was significantly higher (p < 0.001) in the Met S patients than in the controls. Within the same study group, BMI, however, was nearly similar in the 2 categories, with and without PE, with no significant difference (p = 0.31, the Met S group, p = 0.33, the controls, ).
Table 1. Clinical features of men in the two study groups in relation to the presence/absence of premature ejaculationTable Footnote*.
Table 2. Univariate analysis of the study variables based on the presence/absence of the Met S and PETable Footnote*.
Clinical features of the study subject
In the Met S group, the patients with PE had significantly smaller WC (p = 0.047), higher FBS (p = 0.019) and elevated PEDT score (p < 0.001) compared with the patients without PE (). Other features of the Met S in addition to IIEF-5 scores did not reveal any significant difference between the two categories, as presented in the same table. In the control group, the WC was lower and FBS was higher in men with PE compared with those without PE, but the difference was not significant (). The PEDT scoring was significantly high (p < 0.001) in men with PE compared with those without PE. Other features of the controls, in the presence or absence of PE, did not reveal any significant difference, except the SBP (p = 0.043). Comparing the data of any studied clinical feature of each subgroup in the Met S cohort with its comparable one in the control population, as itemized in , identified significant differences (p < 0.001).
Prevalence and scoring of PE as related to the number of Met S elements
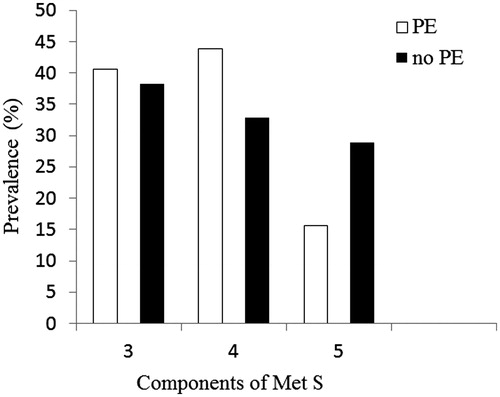
The prevalence of PE according to the number of Met S elements was demonstrated in . The prevalence increased among the patients with 4 components compared with those with 3 components but this increase was insignificant (p = 0.56). Then the prevalence dropped when the components were 5, and the drop was also insignificant (p = 0.053). The patients with PE and 3, 4 and 5 elements of the syndrome had PEDT scores (mean ± SD): 15.3 ± 2.9, 15.1 ± 2.8 and 16.6 ± 2.9, respectively. There were no significant differences (p = 0.37) among these scores.
Figure 1. Prevalence of PE according to the number of Met S elements.
Univariate analysis of the study variables based on the presence/absence of the Met S and PE
A significant association between PE and both ED (p < 0.001) and systolic hypertension (p = 0.047) has been noticed among the patients with Met S as shown in . Other study variables did not show significant associations with PE (). In the control group, no associations were identified, except for the WC (p = 0.0002) and FBS (p = 0.003) as demonstrated in the same table.
Binary logistic regression analysis of SBP and ED for PE
Checking the regression model revealed that both variables did not make a significant contribution to the prediction of PE in the studied men with Met S (). However, the model indicated the inverse relationship between the probability to have PE and both variables.
Table 3. Results from the logistic regression analysis using the PE as the dependent variable in the patients with Met S.
Discussion
The present work is the first study to investigate directly and focus exclusively on the relationship between PE and Met S. The study identified that the prevalence of PE among patients with Met S is significantly higher (p < 0.001) than that reported in the controls (35.2% vs 7.6%, respectively). This agrees with other studies [Citation21,Citation22] which examined the same topic indirectly and claimed the higher prevalence of PE among patients with Met S. Lotti et al. examined 27 and 342 men with and without Met S and reported a prevalence of PE of 22.2% versus 14.4% in each group, respectively [Citation21]. Corona et al. [Citation22] studied 236 patients who fulfilled criteria for Met S and their 567 controls. Their study revealed the higher prevalence of PE among the patients with Met S as compared with those with no Met S (22.7% versus 3% respectively). The difference between the prevalence of PE in our patients and that given by these two studies may be related to several factors. These may include the different methodology to check for the existence of PE, as claimed previously [Citation23], the varying sources where the patients were recruited, the great discrepancy in the prevalence of hyperglycemia in the different studies, which is associated with a higher prevalence of PE [Citation4,Citation5], and the obviously low number of subjects who participated in the Lotti et al. study [Citation21].
The present study also showed the prevalence of PE among men without Met S (controls). This represents, therefore, the first report to show this prevalence in the Egyptian community depending on PEDT. The reported prevalence in the current study (7.6%) seems close to that identified by a recent investigation [Citation24] which devised a large global study in which the prevalence of PE was estimated in men from different geographical zones across the globe, and depended on one simple question to diagnose PE “did you reach climax too early”. In that study, the prevalence in the Middle East as “one notable exception” was estimated to be 12.4%, which was lower than in other geographical zones.
According to the present study, both WC and FBS were significantly related to the existence of PE. WC got significantly smaller (p = 0.047) when compared with that in the Met S men without PE and the difference got more significant (p < 0.001) when the comparison was made with that in the controls without PE. These data coincide with other investigators who identified a leaner body constitution of their patients with PE as compared with the healthy controls [Citation25]. Those investigators attributed this to increased desensitization of serotonin 1A receptors in obese men due to the direct effect of estradiol, present in high amounts in these men, on these receptors. Serotonin is well-known as the most potent central monoamine neurotransmitter that is involved in delaying ejaculation [Citation26]. In regard to FBS, it was significantly higher in Met S-associated PE (p = 0.019). This agrees with other authors who addressed the increase in the prevalence of PE with DM [Citation4,Citation5]. The pathophysiology of PE in DM is not well understood. However, El-Sakka [Citation4] suggested a dis-integrity of the autonomic nervous system with improper actions of its central and peripheral neurotransmitters as evidenced by the existence of diabetic neuropathy.
In this study, the demographic variables did not identify significant association with PE. Ageing was comparable in subjects with/without PE whether in the study or control groups. Several researchers have not reported a rising risk of PE as age advances [Citation27,Citation28]. Similarly, smoking, socioeconomic status and BMI did not reveal significant differences among the different study subgroups. This agrees with other investigators who reported the same observation [Citation29,Citation30].
The present investigation revealed that there was a significant association between PE and both systolic hypertension and ED in Met S (p = 0.047 and < 0.001, respectively). In the literature, there is no peer-reviewed study demonstrating the relationship between hypertension and PE. However, browsing the Internet showed many websites which claim the link between both conditions anecdotally [Citation31]. This subject is, therefore, open for future research with scientific merits which can elucidate it giving a solid conclusion. In regard to ED, its highly significant association with PE was replicable with and thus confirming other studies [Citation8,Citation9,Citation30]. This strong interrelationship between these two conditions was suggested by some investigators to be due to their mutual pathophysiological mechanisms [Citation9]. Others postulated that in an effort to sustain an erection, a man will shift to direct stimulation (touch) to raise his degree of excitement. Although this may be useful in one aspect (keeping an erection), it may not be so in another aspect where PE will happen [Citation8]. Although we could not indicate in this study that ED may be a predictor of PE, in spite of this strong association between both conditions, several investigators have already considered ED as the grandest predictor of PE, although not the only factor [Citation28,Citation32]. The inability to indicate ED as a predictor in this study may be related to the extremely diverse nature of PE related to its definition, natural history and taxonomy and also the relatively limited number of the studied patients. The present study, therefore, may help to find factors associated with PE. However, additional studies on the prevalence and associated factors of PE are required to corroborate and extend the current results. We also think that in order to manage PE, it is essential to recognize and treat its etiology first, which is possible to improve its severity [Citation33], before shifting to the classical therapeutic options of the disorder like pharmacotherapy.
The current study did not report that any of the different components Met S would represent a risk factor to have PE. This agrees with the very limited number of studies which touched this subject just in passing [Citation21,Citation22]. However, we think that the net impact of the different components of Met S, particularly high FBS and low WC, working side by side through different pathophysiological mechanisms could be a reason to facilitate the occurrence of PE. Meanwhile, the study did not also reveal a significant association between the number of Met S components and the prevalence of PE, which is in contrast to the significant association between ED prevalence and the number of components [Citation34]. Interestingly, there was a decline in the prevalence of PE with the existence of 5 components compared with that prevalence in the presence of 3 or 4 components. The reason for this drop may be related to the strong association between increasing number of Met S components and drop in serum testosterone [Citation21,Citation22]. Low testosterone level is often linked to delayed than to premature ejaculation [Citation35]
The current study has some limitations. First, the use of PEDT, not intravaginal ejaculatory latency time (IELT) to diagnose PE may represent an important drawback and could be criticized by some. The PEDT questionnaire has been developed according to the outdated DSM-IV definition [Citation20] which has been slammed for being vague and lack operational criteria [Citation36]. However, PEDT is obviously an easy tool to diagnose PE, and has been validated meticulously [Citation20]. In contrast to IELT, which is an objective and operational marker for criteria applied in the assessment of PE [Citation2,Citation37], PEDT lacks individual inconvenience and subsequent bias during stopwatch-estimated IELT [Citation37]. Second, this study was an office-based study, and the investigated patients did not represent the general population. Therefore, the results of the study may not be applicable to the general population. In fact, it may be difficult to have a representative sample from the general population given the taboo, present in this community for talking about sexual matter [Citation38]. Third, the inability to use an Arabic validation of PEDT during evaluation of PE because it is not available so far. Fourth, the exclusion criteria in this study included intake of any medications for ED or PE, but it was extremely difficult to exclude patients receiving medications against chronic medical conditions e.g. DM or hypertension. These medications may affect indirectly the degree of PE after ameliorating Met S components. Fifth, the lack of testosterone assessment in this study could not explain and hence support our finding that the increase in the number of Met S components is associated with a drop, although not significant, in the prevalence of PE.
Conclusions
PE has a high prevalence in Met S patients. Patients with Met S should be questioned about PE, and physicians should be aware of that. Both ED and systolic hypertension may be associated with PE under Met S, which mandates an inclusive scheme for clinical management of Met S-associated PE. A better definition of the relationship between Met S and PE is supposed to improve this management. Prevention of Met S should also be expedited, and this may be of help to decrease the prevalence of PE.
Declaration of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research and/or publication of this article.
References
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Washington (DC): American Psychiatric Association; 2013
- Lee SW, Lee JH, Sung HH, et al. The prevalence of premature ejaculation and its clinical characteristics in Korean men according to different definitions. Int J Impot Res 2013;25:12–17
- Rosen RC. Prevalence and risk factors of sexual dysfunction in men and women. Curr Psychiatry Rep 2000;2:189–95
- El-Sakka AI. Premature ejaculation in non-insulin-dependent diabetic patients. Int J Androl 2003;26:329–34
- Owiredu WK, Amidu N, Alidu H, et al. Determinants of sexual dysfunction among clinically diagnosed diabetic patients. Reprod Biol Endocrinol 2011;9:70
- Mourikis I, Antoniou M, Matsouka E, et al. Anxiety and depression among Greek men with primary erectile dysfunction and premature ejaculation. Ann Gen Psychiatry 2015;14:34
- Liang CZ, Hao ZY, Li HJ, et al. Prevalence of premature ejaculation and its correlation with chronic prostatitis in Chinese men. Urology 2010;76:962–6
- Jannini EA, Lombardo F, Lenzi A. Correlation between ejaculatory and erectile dysfunction. Int J Androl 2005;28:40–5
- Brody S, Weiss P. Erectile dysfunction and premature ejaculation: interrelationships and psychosexual factors. J Sex Med 2015;12:398–404
- Reynolds K, He J. Epidemiology of the metabolic syndrome. Am J Med Sci 2005;330:273–9
- Huang PL. A comprehensive definition for metabolic syndrome. Dis Model Mech 2009;2:231–7
- Khang YH, Cho SI, Kim HR. Risks for cardiovascular disease, stroke, ischaemic heart disease, and diabetes mellitus associated with the metabolic syndrome using the new harmonised definition: findings from nationally representative longitudinal data from an Asian population. Atherosclerosis 2010;213:579–85
- Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) Final Report. Circulation 2002;106:3143–421
- Chaudhary RK, Shamsi BH, Tan T, et al. Study of the relationship between male erectile dysfunction and type 2 diabetes mellitus/metabolic syndrome and its components. J Int Med Res 2016;44:735–41
- Chen K, Mi H, Gao Y, et al. Metabolic syndrome: a potential and independent risk factor for erectile dysfunction in the Chinese male population. Urology 2012;80:1287–92
- Besiroglu H, Otunctemur A, Ozbek E. The relationship between metabolic syndrome, its components, and erectile dysfunction: a systematic review and a meta-analysis of observational studies. J Sex Med 2015;12:1309–18
- Williams DR, Collins C. U.S. socioeconomic and racial differences in health: patterns and explanations. Ann Rev Sociol 1995;21:349–86
- Shamloul R, Ghanem H, Abou-zeid A. Validity of the Arabic version of the sexual health inventory for men among Egyptians. Int J Impot Res 2004;16:452–5
- Rosen RC, Cappelleri JC, Smith MD, et al. Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int J Impot Res 1999;11:319–26
- Symonds T, Perelman MA, Althof S, et al. Development and validation of a premature ejaculation diagnostic tool. Eur Urol 2007;52:565–73
- Lotti F, Corona G, Degli Innocenti S, et al. Seminal, ultrasound and psychobiological parameters correlate with metabolic syndrome in male members of infertile couples. Andrology 2013;1:229–39
- Corona G, Mannucci E, Schulman C, et al. Psychobiologic correlates of the metabolic syndrome and associated sexual dysfunction. Eur Urol 2006;50:595–604
- Carson C, Gunn K. Premature ejaculation: definition and prevalence. Int J Impot Res 2006;18:S5–13
- Laumann EO, Nicolosi A, Glasser DB, GSSAB Investigators’ Group, et al. Sexual problems among women and men aged 40–80 y: prevalence and correlates identified in the global study of sexual attitudes and behaviors. Int J Impot Res 2005;17:39–57
- Gökçe A, Ekmekcioglu O. Insight on pathogenesis of lifelong premature ejaculation: inverse relationship between lifelong premature ejaculation and obesity. Int J Impot Res 2010;22:251–4
- Mas M, Rodriguez del Castillo A, Guerra M, et al. Neurochemical correlates of male sexual behavior. Physiol Behav 1987;41:341–5
- Dunn KM, Jordan K, Croft PR, Assendelft WJ. Systematic review of sexual problems: epidemiology and methodology. J Sex Marital Ther 2002;28:399–422
- Tang WS, Khoo EM. Prevalence and correlates of premature ejaculation in a primary care setting: a preliminary cross-sectional study. J Sex Med 2011;8:2071–8
- Basile Fasolo C, Mirone V, Gentile V, Andrology Prevention Week Centers, Italian Society of Andrology (SIA), et al. Premature ejaculation: prevalence and associated conditions in a sample of 12,558 men attending the andrology prevention week 2001 – a study of the Italian Society of Andrology (SIA). J Sex Med 2005;2:376–82
- Son H, Song SH, Kim SW, Paick JS. Self-reported premature ejaculation prevalence and characteristics in Korean young males: community-based data from an internet survey. J Androl 2010;31:540–6
- Would you have premature ejaculation when you have high blood pressure? [Internet]. NY (NY): eHealthMe; 2016. Available from: http://www.ehealthme.com/cs/high+-blood+pressure/premature+ejaculation [last accessed 29 Aug 2016]
- Lewis RW, Fugl-Meyer KS, Definitions, classification, and epidemiology of sexual dysfunction. In: Lue TF, Basson R, Rosen R, Giuliano F, Khoury S, Montorsi F, eds. Sexual medicine: sexual dysfunctions in men and women. Paris (France): Health Publications; 2004:37–72
- Magri V, Montanari E, Škerk V, et al. Fluoroquinolone-macrolide combination therapy for chronic bacterial prostatitis: retrospective analysis of pathogen eradication rates, inflammatory findings and sexual dysfunction. Asian J Androl 2011;13:819–27
- Demir T, Demir O, Kefi A, et al. Prevalence of erectile dysfunction in patients with metabolic syndrome. Int J Urol 2006;13:385–8
- Corona G, Jannini EA, Lotti F, et al. Premature and delayed ejaculation: two ends of a single continuum influenced by hormonal milieu. Int J Androl 2011;34:41–8
- Waldinger MD, Schweitzer DH. Changing paradigms from a historical DSM-III and DSM-IV view toward an evidence-based definition of premature ejaculation. Part 1. Validity of DSM-IV-TR. J Sex Med 2006;3:682–92
- Patrick DL, Althof SE, Pryor JL, et al. Premature ejaculation: an observational study of men and their partners. J Sex Med 2005;2:358–67
- Salama N. Consultation for small-sized penis in the Egyptian males: a case-control study. Am J Mens Health 2016;10:220–7