
ABSTRACT
The concept of a safety culture is crucial to improving organisational risk management in several sectors, including health and aviation. However, social and welfare services are also sectors where organisations should be aware of the risk in their daily practice. The aim of the present article is to confirm the usability of a modified Safety Attitudes Questionnaire (SAQ) in the Norwegian child protection services CPS by checking a number of its psychometric properties. The SAQ is an instrument that has been widely applied and understood as valid and trustworthy for mapping employees’ views of their organisation’s safety culture. A confirmative factor analysis of data from a national survey of Norwegian CPSs demonstrated that the modified questionnaire has a factor structure which is internally consistent and matches the structure of the widely used SAQ health care questionnaire. The results indicate that the CPS-modified SAQ questionnaire could help understanding and mapping safety culture in the child protection services.
ABSTRAKT
Sikkerhetskultur har vist seg å kunne være avgjørende for å forbedre organisasjoners evne til å håndtere risiko i flere sektorer, som blant annet helsetjenester og luftfart. Sosial- og velferdstjenester er også sektorer der organisasjoner bør være oppmerksomme på risiko i daglige praksis. Målet med denne artikkelen er å vurdere psykometriske egenskaper i spørreskjemaet Safety Attitudes Questionnaire (SAQ) modifisert for norske barneverntjenester. SAQ er et instrument som har blitt mye brukt og som er vurdert som gyldig og pålitelig for å kartlegge ansattes syn på organisasjoners sikkerhetskultur. Konformativ faktoranalyse av data fra en nasjonal undersøkelse fra Norske barneverntjenester viste at det modifiserte spørreskjemaet har en faktor struktur som er internt konsistent og samsvarer med strukturen til det mye brukt SAQ spørreskjemaet for helsevesenet. Resultatene indikerer at det modifisert SAQ spørreskjema kan hjelpe forståelse og kartlegging av sikkerhetskultur i barnevernet.
Background
Daily, child protection services’ (CPS) employees find themselves in situations where they make decisions about children’s, youth’s and family’s lives. These decisions are always connected to the risk of making incorrect decisions that could lead to the complication of family relations, serious maltreatment, and even death. Unfortunately, there have been some cases in Norway where CPS decisions had fatal outcomes (Kirkengen & Thornquist, Citation2013).
Insufficient decisions can be misunderstood as reflecting individual social workers’ incompetence or being unfortunate single incidents (Munro, Citation2019a). According to Sicora (Citation2018), problems in CPS practice are nearly always related to organisational culture and system issues (Munro, Citation2019b). This understanding is also supported by various reports from the Norwegian Board of Health Supervision, which has documented that mistakes in the CPS are often no single incidents but practices being repeated time and again (Slettebø et al., Citation2019). Consequently, improvements to make the actors perform better may turn the focus from individual performance in specific cases to an organisational culture of preventing and handling inefficacy and mistakes (Reason et al., Citation2001). The lack of attention to safety culture in practice and decision making may have negative consequences, such as an increased culture of blame, in which individual persons or single services are blamed (Lachman & Bernard, Citation2006). This undermines psychological safety, which is required to learn from adverse events and organisational failures (Edmondson, Citation2018). The relevance for focusing on CPS organisations and a safety culture is also supported by research from several other countries. Studies have described a lack of culture to learn from mistakes and accountability as an issue in CPS (Munro, Citation2019a; Sicora, Citation2018; Sicora et al., Citation2020; Vogus et al., Citation2016). In the development of CPS, internal control systems and capacity building have been discussed, but the development of supportive learning cultures is also key (Sicora, Citation2018), here with a focus on the safety and working conditions of employees (Munro, Citation2005). Drawing on the organisational safety culture literature from other high-risk sectors, Munro (Citation2019a) calls for a positive and proactive culture to improve services in child protection, including proactive learning from mistakes.
Senge (Citation2010) defines learning organisations as those that are adaptive and develop a culture of innovative learning that facilitates continuous reflection and growth. A learning culture in CPS implies that the services create, transfer, and use knowledge and experiences to achieve positive changes and realise their goals from practise and decisions that went wrong. We can find important support for the value of safety culture in a study from the US showing that young people who receive services from CPS with a well-functioning organisational culture increase the chances for better outcomes for youths (Glisson & Green, Citation2011).
In other sectors such as the military, aviation and hospitals, this perspective has been well established. It has been proven that organisations that systematically work to improve their safety culture have reduced risk for errors (Braithwaite et al., Citation2017). Many organisations apply surveys to map the safety culture as a part of their organisational development. However, CPS lacks the tools for evaluating safety cultures. There are several established instruments for mapping safety culture in services; one of the most well-known is the Safety Attitude Questionnaire (SAQ) (Sexton et al., Citation2006), which has been widely applied for building safety culture in hospitals and healthcare services (Deilkås & Hofoss, Citation2008; Nordén-Hägg et al., Citation2010). Internal validation of the SAQ has been performed in several studies. Some have also reported that the questionnaire is correlated with patient outcome (Colla et al., Citation2005; Deilkås & Hofoss, Citation2008). Therefore, questionnaires can be an important tool in health services to map safety concerns and improve safety culture. In the present article, we examine the validity and reliability (psychometric properties) of the SAQ adapted to CPS. The paper also discusses the possibilities of implementing the SAQ in CPS to strengthen the organisational learning culture and user quality of their services.
It seems that CPS services both in Norway and elsewhere lack knowledge of how to map safety concerns in services that can provide knowledge of how the organisation can facilitate systematic work and prevent recurring mistakes (Lachman & Bernard, Citation2006; Zuchowski et al., Citation2019).
Safety culture, knowledge from aviation and hospitals that can have relevance for CPS
Helmreich and Merritt’s (Citation2001) book Culture at Work exemplifies how safety and error management can improve by working with different aspects of organisational culture and professional attitudes and values. Deilkås et al. (Citation2019, p. 2) state that the safety culture as a culture ‘involves leader and staff interactions, attitudes, routines, awareness, and practices that influence risks of adverse events’ in a health service setting. Deilkås et al. (Citation2019, p. 2) further describe, ‘A cultural trait may, for example, be how leaders facilitate dialogue with staff to uncover negative relationships and behaviour, promote mutual understanding of the causes of adverse events, and establish consensus regarding safety priorities’. This is also a relevant situation for CPS.
The report, To Err is Human: Building a Safer Health System (Kohn et al., Citation1999), explicitly describes how failures and mistakes in American health services lead to patient injuries. These failures are often connected to employees’ work situations and the factors connected to internal organisational services, such as lack of routines, work stress or conflicts, or lack of collaboration between professionals. The report has contributed to an intensified focus on patient safety in hospitals.
Aviation and surgery are probably more standardised globally than CPS. CPS has major differences in its mandate and structure, both within national communities and worldwide. However, the question of how to help organisations and professionals learn from unsuccessful interventions and build and maintain a safety culture is relevant across sectors and national borders. Health services have several instruments to measure employees’ safety concerns and attitudes (Singla et al., Citation2006) that might be useful for CPS. The measurements of perceptions of safety culture shared among staff in an organisational unit are referred to as safety climates (Zohar, Citation2014). Valid safety climate measurements can identify levels of staff perceptions, the extent to which they are shared and how they vary across organisational units (Alsalem et al., Citation2018). Variations in such assessments may predict variability in risk related to tasks, work environment, staff behaviour and the outcome for users (Braithwaite et al., Citation2017).
Safety Attitude Questionnaire (SAQ)
Sexton et al. (Citation2006) work on organisational culture has been transformed into the SAQ (Sexton et al., Citation2006), a questionnaire for mapping employees’ and leaders’ views of organisational safety culture and concerns. The short version of the SAQ has been modified and applied globally in many services, but it is most commonly used to measure and facilitate safety culture within hospitals (Deilkås & Hofoss, Citation2008). The SAQ has also been applied and found to have acceptable validity in other health care services, for instance, in nursing homes (Bondevik et al., Citation2019; Deilkas et al., Citation2019), pharmacies (Nordén-Hägg et al., Citation2010) and general practitioner practices and emergency rooms (Deilkås et al., Citation2019).
The questionnaire focuses on six defined factors in organisational culture that have an impact on how employees manage situations in which there is a risk of defective or erroneous action: safety climate, teamwork climate, working conditions, job satisfaction, stress recognition and perceptions of safety management. Research has confirmed the relevance of the factor structure of the SAQ short version in Norwegian hospitals (Deilkås & Hofoss, Citation2008).
Parts of the SAQ questionnaire have also been applied earlier in CPS (Munro, Citation2019b; Vogus et al., Citation2016). However, to the best of our knowledge, there is no study in which the questionnaire has been systematically modified and tested in a CPS setting. Hence, the aim of the present study was to modify and adapt SAQ for CPS settings and to test its psychometric properties.
Materials and methods
Participants and setting
The present study was based on a study of system accountability in CPS, in which all Norwegian child protection workers working frontline were invited to participate. The SAQ items were added at the end of the questionnaire. This article focuses on confirmatory factor analysis and include only the SAQ-items included in the survey.
The Norwegian CPS is organised into municipalities, and no central registry of employees exists. Therefore, an inquiry was sent to all Norwegian chief municipal executives asking for permission to invite their CPS employees to participate. The municipality administrators sent our research team a list of the e-mail addresses of relevant employees. We received 2844 valid e-mail addresses of staff employed in professional positions in municipal CPS. All received invitations at their work e-mail address to participate in a Questback questionnaire. Reminders were sent to those who did not respond. Individual invitations to the questionnaire ensured that the appropriate individuals replied, that no one replied more than once and that participation was anonymous for CPS leaders and colleagues.
Measures
The SAQ short version
The items in the latest nongeneric short version of the SAQ consist of 36 items grouped into six factors (Sexton et al., Citation2006): teamwork climate (6 items), safety climate (7 items), job satisfaction (5 items), stress recognition (4 items), perceptions of management (5 items, measured at levels: unit and hospital) and working conditions (4 items). Five of the items in the questionnaire were not included in any factors and, therefore, were irrelevant to the confirmatory factor analysis. The complete questionnaire with factors is presented in the first column of .
Table 1. Original SAQ questionnaire and Norwegian CPS version (translated to English by the authors).
Modification of SAQ and hypothesised factor structure
Transforming a questionnaire from one sector to another includes changes in the terms and context-related items. Changes in factor structure could also be considered. Such changes should be theoretically based on arguments, previous research or advice from people with advanced knowledge of the field.
The first and second authors developed drafts for the questionnaire based on the English short version of the SAQ for hospitals. We consulted an expert panel comprising practitioners, bureaucrats, researchers, and service users from CPS to benefit from their experience. To modify the SAQ for use in a CPS context, particular emphasis was placed on adapting the wording. For example, we had to develop appropriate concepts for CPS and replace words from the health context, such as nurses, doctors, hospitals and patients. Some items were edited to fit the context.
In total, four items in the short version for hospitals of the SAQ were not found applicable for conversion to the CPS context and, therefore, were excluded. Those four items were all part of the ‘stress recognition’ factor, which neither the researchers nor the expert panel considered appropriate in the CPS context.
The questionnaire was also piloted in a child welfare service in which the employees had the opportunity to comment on content and structure. They also suggested removing the ‘stress recognition’ factor. In addition, their feedback was related to some minor language changes, and they stated that the questions were relevant and easy to answer for CPS workers.
Like the original short SAQ version for hospitals, our questionnaire applies a 5-point Likert-type scale that ranges from 1 = disagree strongly to 5 = agree strongly for all items. The participants were informed that they could leave the items blank.
The questionnaire presented in the present article was translated from Norwegian to English. The translation was done by the first author and verified by the other authors.
In the workshop groups, the practitioner was given the modified items and asked to place them in the right factor (teamwork climate, safety climate, job satisfaction, perceptions of management and working conditions). Most of the factor structure from health was confirmed to be relevant for CPS. The researchers discussed and negotiated where an item was scored as belonging to another factor than in the generic version. Item 19, which focuses on morale, was moved from the job satisfaction factor to teamwork climate. The researchers’ conclusion was to include items that refer to everyday collaboration in the teamwork climate factor and those that relate more specifically to managing or avoiding risk in the safety climate factor. This led to three items (2, 3 and 5) being moved from teamwork climate to safety climate because these were found to be more closely related to concerns about communication and risks in practice than to general team collaboration. In practice, our hypothesis is based on the idea that teamwork is not so much related to direct risk in CPS because there is probably less direct collaboration than in cockpits, hospital wards and operating rooms. Teamwork is still highly relevant for ensuring safety in CPS by involving colleagues as discussion partners or co-workers in difficult or risky cases. There was no need for any changes in the items related to the factors of working conditions and perceptions of management. The modified questionnaire with a hypothesised factor structure is presented in , second column.
Sociodemographic variables
The questionnaire includes several sociodemographic variables, such as gender, age, profession, education, position, CPS work experience and size and geographical spread of CPS. These items are applied in the analysis for knowledge about the dataset’s representativity.
We also asked questions about sick leave and future ambitions, which are relevant for a wider understanding of the respondents’ views and work situations. These items are not included in the current article but can be relevant data for further understanding the work and safety culture.
Data processing – confirmatory factor analysis: internal construct validity
The confirmatory analysis of the SAQ was performed using the software AMOS, which is an SPSS extension. SPSS was applied to estimate Cronbach’s alpha, item-to-own correlations, intercorrelations of factors, test–retest correlations and all item-descriptive statistics. An indicator of an item not belonging where it was hypothesised to be included is whether its removal would markedly improve that variable set’s Cronbach’s alpha. Cronbach’s alpha scores between 0.70 and 0.90 were considered good and above 0.60 as acceptable (Tavakol & Dennick, Citation2011).
The hypothesised five-factor model was tested by confirmatory factor analysis (CFA) in AMOS. Because factors reflect the correlation structure in the item responses, valid factors should reflect a thematic logic that is coherent with the purpose of the questionnaire. CFA provides goodness-of-fit indices that measure how well the factor pattern of the survey responses conformed to the prehypothesised factor model.
The following goodness-of-fit indices were calculated: the ratio of the Chi-square to the model’s degrees of freedom (χ2/d.f.), the model’s p-value, the root mean squared error of approximation (RMSEA), the comparative fit index (CFI), the Tucker–Lewis Index (TLI) and the Hoelter 0.05. The χ2/d.f. should be below 5 (Wheaton et al., Citation1977); the p-value should exceed 0.05 (Joreskog, Citation1969); the RMSEA should not exceed 0.08 (Browne & Cudeck, Citation1993); and the CFI and TLI should exceed 0.90 (Jackson et al., Citation2009). The Hoelter 0.05 – an estimate of the largest sample for which the model in question would fit the data – should exceed 200 (Joreskog, Citation1969).
Ethical considerations
The present study was approved by the Norwegian Social Science Data Services, which is the government agency responsible for protecting the privacy of respondents participating in survey research, here according to the Norwegian Personal Data Act (Ref. No. 2015/42892). Informed consent was obtained, and the participants could withdraw from the study at any time.
Results
Response rates and demographic variables
An invitation to participate was sent to 2844 individuals, and 1429 returned the web-based survey. A total of 149 responses were rejected because of incomplete questionnaires. The final nationwide sample comprised 1280 participants, which constituted 45% of the original number invited to participate.
The sample’s sociodemographic variables were compared with register data about CPS from Statistics Norway (Statistikkbanken - barnevern, Citation2017). Distribution of important parameters such as gender, education, number of employees at the offices and national geographic spread in the survey were found to be close to representative for the population.
lists the respondents’ education data and a comparison with the data from Statistics Norway. From the table, it can be seen that the educational backgrounds of the sample and the population were almost identical.
Table 2. All CPS workers in Norway compared with the respondents.
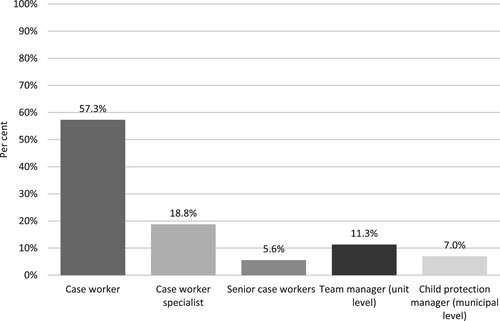
Understanding organisation mapping views from those individuals with different positions in the organisation is important. illustrates the respondents across positions in CPS. We have not been able to find data that give a fair comparison of responses compared with the general population of CP employees. However, analysis of the invited versus sample indicates that leaders have higher response rates than caseworkers.
Figure 1. Participants’ positions in CPS.
Data quality
The number of participants is considered acceptable for exploring the psychometric properties of the questionnaire. A commonly used rule of thumb is that adequately sized samples have cases-to-indicator ratios of at least 10 or 20 (Kyriazos, Citation2018) – our ratio was 1280/27 ≈ 47.
Missing answer was for all items, from 2.3% to 4.7%. The highest percentage of missing items was related to perceptions of management. This is not necessarily an indication that the question was unclear or that the informants would not score their management. It could also be a natural consequence that some employees probably never met their top leader and, therefore, did not answer this. It is known that turnover is high in CPS (Statistikkbanken - barnevern, Citation2017) and that many respondents (11.6%) have worked in the respective CPS for less than one year.
Cronbach’s alphas – internal consistency
The Cronbach’s alphas of our five factors are as follows: perception of management (5 items, alpha = .878), safety climate (10 items, alpha = .867), teamwork climate (4 items, alpha = .756), job satisfaction (4 items, alpha = .869) and work conditions (4 items, alpha = .733).
For no factor, the exclusion of any variable would noticeably increase the α-value.
Construct validity – confirmatory factor analysis (CFA)
We tested the factor structure using CFA. Our factor structure model is presented in .
Figure 2. Factor structure of generic re-hypnotised version of SAQ for CPS (variable number in original SAQ questionnaire (see )).
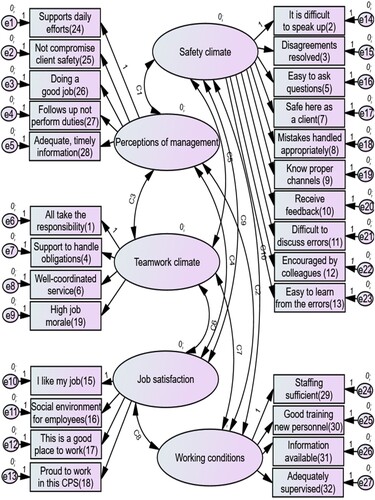
CFA showed that the hypothesised total model, which grouped the 27 indicators under five factors, that is, teamwork climate, safety climate, job satisfaction, perceptions of management and working conditions, fit the data adequately. The goodness-of-fit indices for the model are presented in .
Table 3. Goodness-of-fit indices for generic re-hypnotised version of SAQ for CPS.
Discussion
The current article has presented a psychometric analysis of the SAQ instrument, modified and translated to the Norwegian CPS context. The Cronbach’s alpha values from .733 to .869 are good. In general, the current paper shows acceptable Goodness-of-Fit values for the hypothesised five-factor model (perception of management, safety climate, teamwork climate, job satisfaction and work conditions). The sample, despite its low response rate of 1280/2844 = 45%, is probably close to being representative of important parameters, such as gender, education, number of employed and national geographic spread.
The results indicate that the questionnaire provides an opportunity to measure CPS employees’ views of organisational safety culture and concerns that are well-known in other sectors.
Today, hospitals and health services have established a common understanding of that patient safety (Halligan & Zecevic, Citation2011); this processes to build organisations that are aware of risks and avoid patient injuries are crucial for daily practice. Pronounced and active safety cultures probably also influence users’ trust in organisations services. In CPS, lack of clarity of risk could make it hard to identify and build learning organisations that handle risks and errors. In the modifying process of the questionnaire, with input from both an expert panel and a pilot test, we have seen that CPS also need concepts that differ from health services, although most of the items from the health service questionnaire were possible to modify. The questionnaire presented in this article could be relevant for providing knowledge for the ongoing discussions to obtain a more common understanding of how to define errors in CPS and the crucial elements for building a safety culture.
A main strength of the SAQ is the possibility of comparing different workplaces and institutions. This has been done across national borders and sectors. For instance, in Norwegian hospitals, the same questionnaire is used annually to map and compare different hospital and hospital wards (Deilkås & Hofoss, Citation2010). This annual comparison has aimed to understand which services are successfully building a safety culture and which are at a high risk. This has provided knowledge on how to learn from others and reduce the chance of risk in all national hospitals. Today, there is no instrument to conduct such a comparison in Norwegian CPS. The modified questionnaire presented in the present article could be a starting point to map and compare safety culture in CPS too.
The questionnaire could probably be improved by conducting further surveys and modifications. However, we have found it likely that the questionnaire in its current form could be applied in the organisational development process for understanding how CPS operates concerning the conditions for safeguarding quality and avoiding repetitive mistakes in client work.
An important lesson to be learned from safety culture management is that risk should be understood as an organisational issue (Helmreich & Merritt, Citation2001). Instead of blaming individuals for failures and mistakes, one should use the incidents and adverse events for organisational learning. From the dialogue with the expert panel in the modification process of the questionnaire, we were left with the impression that the responsibility for mistakes in CPS is unclear. In the evaluation of British CPS, Munro (Citation2005) identifies a potential blame culture where case workers and services are at risk of being characterised by lack of competence, assessment ability or skills in following manuals, routines or the legal system when mistakes happened. These cultures do not stimulate organisational learning. Sicora (Citation2018) also describes blame culture as an obstacle to building responsible services in Italy. Theory from safety culture and SAQ could be relevant in exploring how responsibility is placed in CPS and how this supports safety culture.
SAQ supports the improvement of organisational culture in an evidence-based way, as in other sectors. In CPS, a debate of the evidence has had a different orientation from country to country (Gilbert et al., Citation2011) and has often been focusing on measures to clients and less on organisation building. Research strongly indicates that organisation culture can impact client’s outcome from services (Glisson & Green, Citation2011; Williams & Glisson, Citation2013a, Citation2013b). To support more evidence of how to build well-functioning CPS, we need studies that openly share the questionnaire and give readers knowledge of how the questionnaire is organised, including its strengths and weaknesses. Regarding the fact that CPS can be seen as very different depending on the location, the country-to-country application of this questionnaire should be done with a critical stance. Evidence is context dependent, but we believe that more awareness of safety culture, including applying questionnaires like SAQ, has universal relevance for improving services. For leaders and employees in CPS, the present article and the validated questionnaire also give an evidence base for understanding and discussing organisation and safety concerns.
Limitations
The analysis confirmed the internal validity of the modified questionnaire. The external validity of the CPS instrument was not explored. Further research should explore external validity by acquiring knowledge about connections between cultural elements in the workplace and quality of services provided to users, hereby documenting the important key elements for facilitating a safety culture in CPS and by exploring the eventual correlation between these elements.
Conclusions
The current study has presented a modification of the SAQ for CPS. The analysis shows an acceptable factor structure. From a wider perspective, the presented paper discusses how knowledge from the safety culture in healthcare may improve CPS. The discussion illustrates that both the questionnaire and transformation of the framework are relevant to understanding and developing CPS.
Acknowledgements
We want to thank research studentassistant Simon Molvær and his team for distributing the questionnaire. Many thanks to the expert panel who participated in the quality assurance of the questionnaire and the employees who participated in the pilot survey.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data that support the findings are available from the authors and VID Specialised University, subject to the restrictions laid down by the Norwegian Social Science Data Services.
Additional information
Funding
Notes on contributors
Erik Skjeggestad
Erik Skjeggestad, is an Associate Professor(PhD) and Programme Coordinator at the Faculty of Social Studies at VID scientific university. He has work in child protection services as social worker in several years. His field of research are child welfare and professional collaboration. He has a special interest in service and quality development in child protection services.
Torgeir Sørensen
Torgeir Sørensen is an Associate Professor at the at the Faculty of Health at VID Specialized University. He holds a PhD in the field of psychology of religion, and he has performed studies investigating relationships between religion and health, as well as qualitative studies on the significance of meaning-making for people in demanding life situations. Additionally, he has worked with translation and validation of standardized instruments for the Norwegian context.
Dag Hofoss
Dag Hofoss, PhD, Professor (University of Oslo (ret)). Health services research, sociology of professionalization, inequalities in health, quality of life, patient satisfaction and experiences with health care, standardization of care, safety culture in health care, psychometric properties of patient and employee questionnaires, service monitoring methods, quality improvement methods.
Tor Slettebø
Tor Slettebø is a professor in social work at the Faculty of Social Studies at VID scientific university with a long-lasting research background. His field of research is user participation in health and welfare services, and in particular in child protection. He has a special interest in service and quality development in child protection services and how they can develop into learning organisations. He was the leader of the project out of which this article stem from.
Ellen Tveter Deilkås
Ellen Tveter Deilkås, is a specialist in internal medicine with 30 years of clinical practice, and a PhD in patient safety culture. She works as a senior researcher on patient safety and part time as a clinical consultant in an ambulatory multidisciplinary rehabilitation clinic at Akershus University hospital. She has worked both full time and part time as an advisor for the Norwegian government since 2010, designing, establishing and developing national measurements for adverse events and patient safety culture.
References
- Alsalem, G., Bowie, P., & Morrison, J. (2018). Assessing safety climate in acute hospital settings: A systematic review of the adequacy of the psychometric properties of survey measurement tools. BMC Health Services Research, 18(1), 353–353. https://doi.org/10.1186/s12913-018-3167-x
- Bondevik, G. T., Hofoss, D., Husebo, B. S., & Deilkas, E. C. T. (2019). The safety attitudes questionnaire - ambulatory version: Psychometric properties of the Norwegian version for nursing homes. BMC Health Services Research, 19(1), 423. https://doi.org/10.1186/s12913-019-4244-5
- Braithwaite, J., Herkes, J., Ludlow, K., Testa, L., & Lamprell, G. (2017). Association between organisational and workplace cultures, and patient outcomes: Systematic review. BMJ Open, 7(11), e017708. https://doi.org/10.1136/bmjopen-2017-017708
- Browne, M., & Cudeck, R. (1993). Alternative ways of assessing model fit. In K. A. Bollen & J. S. Long (Eds.), Testing structural equation models (pp. 136–162). Sage.
- Colla, J. B., Bracken, A. C., Kinney, L. M., & Weeks, W. B. (2005). Measuring patient safety climate: A review of surveys. Quality & Safety in Health Care, 14(5), 364–366. https://doi.org/10.1136/qshc.2005.014217
- Deilkas, E. C. T., Hofoss, D., Hansen, E. H., & Bondevik, G. T. (2019). Variation in staff perceptions of patient safety climate across work sites in Norwegian general practitioner practices and out-of-hour clinics. PLoS One, 14(4), e0214914. https://doi.org/10.1371/journal.pone.0214914
- Deilkås, E. C. T., Hofoss, D., Husebo, B. S., & Bondevik, G. T. (2019). Opportunities for improvement in nursing homes: Variance of six patient safety climate factor scores across nursing homes and wards—assessed by the safety attitudes questionnaire. PLoS One, 14(6), e0218244–e0218244. https://doi.org/10.1371/journal.pone.0218244
- Deilkås, E., & Hofoss, D. (2010). Patient safety culture lives in departments and wards: Multilevel partitioning of variance in patient safety culture. BMC Health Services Research, 10(1), 1–5. https://doi.org/10.1186/1472-6963-10-85
- Deilkås, E. T., & Hofoss, D. (2008). Psychometric properties of the Norwegian version of the Safety Attitudes Questionnaire (SAQ), generic version (short form 2006). BMC Health Services Research, 8(1), 191. https://doi.org/10.1186/1472-6963-8-191
- Edmondson, A. C. (2018). The fearless organization. Creating psychological safety in the workplace for learning, innovation and growth. Wiley.
- Gilbert, N., Parton, N., & Skivenes, M. (2011). Child protection systems: International trends and orientations. Oxford University Press. https://doi.org/10.1093/acprof:oso/9780199793358.001.0001
- Glisson, C., & Green, P. (2011). Organizational climate, services, and outcomes in child welfare systems. Child Abuse & Neglect, 35(8), 582–591. https://doi.org/10.1016/j.chiabu.2011.04.009
- Halligan, M., & Zecevic, A. (2011). Safety culture in healthcare: A review of concepts, dimensions, measures and progress. BMJ Quality & Safety, 20(4), 338–343. https://doi.org/10.1136/bmjqs.2010.040964
- Helmreich, R. L., & Merritt, A. C. (2001). Culture at work in aviation and medicine: National, organizational and professional influences. Avebury Technical.
- Jackson, D. L., Gillaspy, J. A., & Purc-Stephenson, R. (2009). Reporting practices in confirmatory factor analysis: An overview and some recommendations. Psychological Methods, 14(1), 6–23. https://doi.org/10.1037/a0014694
- Joreskog, K. (1969). A general approach to confirmatory maximum likelihood factor analysis. Psykometrika, 34(2), 183–202. https://doi.org/10.1007/BF02289343
- Kirkengen, A. L., & Thornquist, E. (2013). When diagnosis makes us blind. Tidsskr Nor Laegefo, 133(14), 1466–1468. https://doi.org/10.4045/tidsskr.13.0519
- Kohn, C., & Donaldson, J., & S, M. (1999). To Err is human: Building a safer health system. National Academy Press.
- Kyriazos, T. A. (2018). Applied psychometrics: Sample size and sample power considerations in factor analysis (EFA, CFA) and SEM in general. Psychology (Irvine, Calif.), 9(8), 2207–2230. https://doi.org/10.4236/psych.2018.98126
- Lachman, P., & Bernard, C. (2006). Moving from blame to quality: How to respond to failures in child protective services. Child Abuse & Neglect, 30(9), 963–968. https://doi.org/10.1016/j.chiabu.2006.07.002
- Munro, E. (2005). Improving practice: Child protection as a systems problem. Children and Youth Services Review, 27(4), 375–391. https://doi.org/10.1016/j.childyouth.2004.11.006
- Munro, E. (2019a). Decision-making under uncertainty in child protection: Creating a just and learning culture. Child & Family Social Work, 24(1), 123–130. https://doi.org/10.1111/cfs.12589
- Munro, E. (2019b). Effective child protection. SAGE Publications Ltd.
- Nordén-Hägg, A., Sexton, J. B., Kälvemark-Sporrong, S., Ring, L., & Kettis-Lindblad, Å. (2010). Assessing safety culture in pharmacies: The psychometric validation of the Safety Attitudes Questionnaire (SAQ) in a national sample of community pharmacies in Sweden. BMC Clinical Pharmacology, 10(1), 8. https://doi.org/10.1186/1472-6904-10-8
- Reason, J. T., Carthey, J., & de Leval, M. R. (2001). Diagnosing ‘vulnerable system syndrome’: An essential prerequisite to effective risk management. Quality in Health Care, 10(Suppl 2), ii21–ii25. https://doi.org/10.1136/qhc.0100021
- Senge, P. M. (2010). The fifth discipline: The art & practice of the learning organization (Rev. And updated ed.). Crown/Archetype.
- Sexton, J. B., Helmreich, R. L., Neilands, T. B., Rowan, K., Vella, K., Boyden, J., Roberts, P. R., & Thomas, E. J. (2006). The Safety Attitudes Questionnaire: Psychometric properties, benchmarking data, and emerging research. BMC Health Services Research, 6(1), 44. https://doi.org/10.1186/1472-6963-6-44
- Sicora, A. (2018). Learning from mistakes in social work. European Journal of Social Work, 21(5), 684–696. https://doi.org/10.1080/13691457.2017.1320980
- Sicora, A., Lu, W., & Lei, J. (2020). Exploring mistakes and errors of professional judgement in social work in China and Italy: The impact of culture, organization and education. Journal of Social Work, 21(5), 1065–1083. https://doi.org/10.1177/1468017320919879
- Singla, A. K., Kitch, B. T., Weissman, J. S., & Campbell, E. G. (2006). Assessing patient safety culture: A review and synthesis of the measurement tools. Journal of Patient Safety, 2(3), 105–115. https://doi.org/10.1097/01.jps.0000235388.39149.5a
- Slettebø, T., Briseid, K. M., Brodtkorb, E., Skjeggestad, E., Sverdrup, S. M., & Sørensen, T. (2019). Godt nok barnevern? Forståelser av forsvarlighet og internkontroll i den kommunale barneverntjenesten. VID vitenskapelige høgskole.
- Statistikkbanken - barnevern. (2017). Statistikkbanken [Statisti]. https://www.ssb.no/statbank/list/barneverng.
- Tavakol, M., & Dennick, R. (2011). Making sense of Cronbach's alpha. International Journal of Medical Education, 2, 53–55. https://doi.org/10.5116/ijme.4dfb.8dfd
- Vogus, T. J., Cull, M. J., Hengelbrok, N. E., Modell, S. J., & Epstein, R. A. (2016). Assessing safety culture in child welfare: Evidence from Tennessee. Children and Youth Services Review, 65, 94–103. https://doi.org/10.1016/j.childyouth.2016.03.020
- Wheaton, B., Muthen, B., Alwin, D. F., & Summers, G. F. (1977). Assessing Reliability and Stability in Panel Models. Sociological Methodology, 8, 84–136. https://doi.org/10.2307/270754
- Williams, N. J., & Glisson, C. (2013a). Reducing turnover is not enough: The need for proficient organizational cultures to support positive youth outcomes in child welfare. Children and Youth Services Review, 35(11), 1871–1877. https://doi.org/10.1016/j.childyouth.2013.09.002
- Williams, N. J., & Glisson, C. (2013b). Testing a theory of organizational culture, climate and youth outcomes in child welfare systems: A United States national study. Child Abuse & Neglect, 38(4), 757–767. https://doi.org/10.1016/j.chiabu.2013.09.003
- Zohar, D. (2014). Safety climate: Conceptualization, measurement, and improvement. In B. Schneider & K. M. Barbera (Eds.), The Oxford handbook of organizational climate and culture (pp. 317–334). Oxford University Press. https://doi.org/10.1093/oxfordhb/9780199860715.013.0017
- Zuchowski, I., Miles, D., Woods, C., & Tsey, K. (2019). Continuous quality improvement processes in child protection: A systematic literature review. Research on Social Work Practice, 29(4), 389–400. https://doi.org/10.1177/1049731517743337