
ABSTRACT
Despite the growing body of literature examining the complex needs of adolescents in residential care populations, few studies have investigated the specific treatment needs and characteristics of adolescents in therapeutic residential care (TRC). This study aimed to describe and compare risk, need and responsivity factors in a national sample of 737 juveniles (63% males, mean age = 16.2) who displayed serious behavioural problems. The study utilised comprehensive assessment data, including demographic information, clinical variables, and risk factors assessed with the Youth Level of Service/Case management Inventory (YLS/CMI). Sample characteristics were explored, and three subgroups were compared: adolescents with serious substance abuse, adolescents with a high risk of continued delinquency and adolescents with low/moderate risk. The sample showed complex needs in multiple criminogenic domains and substantial mental health problems. Subgroups were clearly differentiated by the YLS/CMI risk profile and several demographic attributes; however, most clinical variables concerning mental health overlapped between groups. The findings suggest that TRC interventions should be aimed at reducing the risk of persistent delinquency and structured according to the principles of risk, need and responsivity. The study has important clinical implications for how differentiated services can tailor interventions to group-based needs and characteristics.
ABSTRAKT
Til tross for at nyere forskning tyder på komplekse og sammensatte behov hos ungdom i institusjon, har få studier undersøkt de spesifikke behandlingsbehovene og karakteristikkene til ungdommer plassert i behandlingsinstitusjon grunnet alvorlig og gjentagende lovbrudd eller omfattende rusmiddelbruk. Denne studien hadde som mål å beskrive og sammenligne risiko-, behov- og responsivitetsfaktorer i et nasjonalt utvalg på 737 ungdommer (63% gutter, gjennomsnittsalder = 16.2) med alvorlige atferdsvansker. Studien inkluderte demografiske data, kliniske variabler og risikofaktorer vurdert med Youth Level of Service/Case Management Inventory (YLS/CMI). Hele utvalget ble analysert, og tre målgrupper ble sammenlignet: ungdommer med alvorlige rusproblemer, ungdommer med høy risiko for fremtidig kriminalitet og ungdommer med lav/moderat risiko. Resultatene viste at hele ungdomsgruppen hadde komplekse behov innenfor flere kriminogene områder og høy forekomst av psykiske helseproblemer. Målgruppene ble tydelig differensiert av YLS/CMI-risikoprofil og av flere demografiske variabler, samtidig som de fleste psykiske helsevariablene overlappet mellom gruppene. Resultatene tyder på at tiltak bør rettes mot å redusere risikofaktorer som er opprettholdende for kriminell og antisosial atferd, og struktureres i tråd med prinsippene om risiko, behov og responsivitet. Studien har viktige kliniske implikasjoner for hvordan differensierte tjenester kan tilpasse behandlingstiltak til gruppebaserte behov og karakteristikker.
Introduction
Young individuals who struggle with serious behavioural problems like persistent delinquency and substance abuse are of great concern in most societies. These problems are associated with an increased risk of adverse developmental trajectories and life outcomes (Bhuller & Røgeberg, Citation2022; Moffitt, Citation2018; Rivenbark et al., Citation2018). Hence, providing adequate help could have a large impact on individuals and society. Like many other European countries, Norway does not have juvenile detention centres (Deloitte, Citation2019). Out-of-home placement in therapeutic residential care (TRC) is often chosen as an intervention for severe behavioural difficulties when home-based interventions have failed or are deemed to be ineligible. These TRC provisions offer remedial programmes aimed at reducing delinquency and substance abuse and improving prospects for residents. To meet the needs of young people in TRC, it is necessary to understand the complexity of their problems and the treatment factors that are associated with positive outcomes (Whittaker et al., Citation2015). The growing body of research on residential interventions for delinquency has emphasised the importance of targeting certain treatment factors to improve outcomes (Andreassen, Citation2015; Harder & Knorth, Citation2015).
The most prominent approach for addressing juvenile delinquency and substance abuse with quality intervention is the risk-need-responsivity (RNR) model (Wormith & Zidenberg, Citation2018). The RNR is a rehabilitation framework for offender populations that has gained robust empirical support for its effectiveness (Koehler et al., Citation2013; Lipsey, Citation2009; Lloyd et al., Citation2014; Prendergast et al., Citation2013). The RNR model highlights that interventions should focus on reducing delinquent behaviour through the three main principles of risk, need and responsivity (Andrews et al., Citation1990). The risk principle states that the intensity of intervention should be matched to the level of risk of continued criminal behaviour (i.e. recidivism). The need principle emphasises that intervention should target ΄criminogenic needs΄, which are dynamic factors that are functionally related to sustaining criminal behaviour and malleable to change (e.g. drug use). The responsivity principle states that interventions should be customised to individual characteristics to optimise their response to treatment (e.g. abilities, mental health, maturity, motivation) (Bonta & Andrews, Citation2017).
Although the RNR model is increasingly recognised as a promising framework for nonsecure residential welfare services (Leloux-Opmeer et al., Citation2017), little is known about how these treatment principles apply to the unique characteristics of adolescents in a TRC setting. Research on youths living in European residential care institutions is limited (Johansen et al., Citation2020). Most Norwegian studies have explored the needs of clients in foster care or conventional residential youth care (Lehmann & Kayed, Citation2018) which limits the generalizability to TRC settings. Furthermore, residential studies including subsamples of adolescents from TRC have primarily focused on high levels of psychological strain and mental health needs (Greger et al., Citation2015, Citation2016; Jozefiak et al., Citation2015, Citation2017). While mental health concerns reported in these studies are important to address as responsivity factors, such needs are mainly found to be unrelated to criminal recidivism and persistent delinquency (Guebert & Olver, Citation2014; Jäggi et al., Citation2021; McCormick et al., Citation2017). Consequently, there is a lack of studies incorporating risk factors that are catalysts for criminal behaviour. This leads to concerns; since the main goal of TRC is to reduce prospects of continued delinquency, risk factors therefore represent the specific treatment need, i.e. criminogenic needs (Bonta & Andrews, Citation2017). Hence, there is a need for a better understanding of risk factors among adolescents in TRC and related social services.
While risk factors for persistent delinquency are well known (Assink et al., Citation2015), the population of juvenile delinquents is considered heterogeneous in terms of how these factors transpire (Lanza et al., Citation2014). Research on young offenders has distinguished different profiles based on several criteria, such as the combination of offences, pattern of risk factors and substance abuse (Hillege et al., Citation2017; E. Mulder et al., Citation2019; Onifade et al., Citation2008; van der Put et al., Citation2013). Similarly, there has been an increased awareness within child welfare systems that youths present with different delinquency risks (Bullock & Gaehl, Citation2012; Ryan, Citation2012). In a study by Maneiro et al. (Citation2019), Spanish adolescents placed in residential care could be differentiated by low-, middle-, and high-risk profiles for antisocial behaviour utilising a risk assessment tool. However, actuarial risk assessment and subgroup classification and differentiation of adolescents with serious behavioural problems seem to have received little attention in residential service systems (Aase et al., Citation2020; Berg et al., Citation2020; Deloitte, Citation2019). As such, further exploration of how risk profiles transpire in this population is necessary.
Current study
Given the main goals of TRC and the vast literature supporting the efficacy of treatment principles, it is necessary to explore adolescents’ needs from an RNR perspective. To our knowledge, no study has investigated risk, need and responsivity factors in adolescents with serious behavioural problems in a nonsecure therapeutic residential care setting. Detailed information on these characteristics could help provisions offer appropriate service levels and allocate resources accordingly. Moreover, examining how subgroups are characterised by risk profiles could optimise treatment intensity and guide how interventions could be matched to needs. Such adjustments can have a positive impact on treatment outcomes (Baglivio et al., Citation2018; Luong & Wormith, Citation2011; van der Put et al., Citation2013).
Thus, the primary objective of the current study was to describe and compare risk, need and responsivity characteristics among adolescents in TRC who presented with serious behavioural problems, focusing on three subgroups: Adolescents with low/moderate versus high risk of continued delinquency, and adolescents with serious substance abuse problems.
Methods
Participants
Adolescents referred to national TRC services offered by The Office for Children, Youth and Family Affairs (Bufetat) in the period November 2017 to November 2020 were enrolled in the study. The main exclusion criteria were individuals who had status as unaccompanied asylum seekers in Norway as these adolescents are in extraordinary circumstances, and it is challenging to complete risk ratings. Also, the sample excluded adolescents from Oslo because The Norwegian Office for Children, Youth and Family Affairs (Bufetat) serve as a national service provider except for Oslo municipality. In Oslo, the functions and authority of central government child welfare authorities at regional level are exercised by the municipality itself. The final sample consisted of 737 adolescents.
Setting
TRC placements are regulated by the Norwegian Child Welfare Act and can be pursued with or without the adolescent's consent (‘the Child Welfare Act,’ Citation1992). TRC institutions in Norway are organised by the Norwegian Directorate for Children, Youth and Family. These facilities are not secure, but the staff can regulate the adolescents’ opportunities to leave the institution. All institutions offer therapeutic care and have a multisystemic goal-oriented approach with standardised practices.
Risk factors
As proper exploration of RNR principles in TRC requires adapting structural assessment of risk and needs, (Andrews et al., Citation2011; Andrews & Bonta, Citation2010; Bonta & Andrews, Citation2017) this study used the Youth Level of Service/Case Management Inventory (YLS/CMI) (Hoge & Andrews, Citation2011). The inventory has proven cross- cultural validity in the European context (Basto-Pereira et al., Citation2021; Cuervo et al., Citation2020; Ortega-Campos et al., Citation2020; Vaswani & Merone, Citation2014) and matching services to YLS/CMI informed needs has shown potential in predicting treatment success in young offenders (Vieira et al., Citation2009). The Norwegian version is translated through commonly accepted protocols and approved by the publisher Multi Health Systems Inc. The inventory is designed as a 42-item checklist of criminogenic risk factors relevant to decisions regarding level of service and case management. Each item is coded as either present or absent and then summed for a composite risk score. Based on this total score, four levels of recidivism risk classification are provided in the manual (Hoge & Andrews, Citation2011). These risk levels are low risk (0–8), moderate risk (9–22), high risk (23–34), and very high risk (35–42). The inventory also quantifies risk factors in eight subdomains. The domain Prior and Current offences/Dispositions is concerned with static risk factors related to chronic offending and delinquent behaviour (5 items). The remaining seven domains measure dynamic risk factors considered to be important for effective case management and intervention. These domains are Family Circumstances/Parenting (6 items), Education/Employment (7 items), Peer Relations (5 items), Substance Abuse (4 items), Leisure/Recreation (3 items), Personality/Behaviour (7 items), and Attitudes/Orientation (5 items). All eight domains have a total mean score based on how many items are checked and together these domain scores provide an overall profile of risk factors and criminogenic needs.
Responsivity factors
According to the RNR-model, responsivity factors could be variables which influences how a client responds to efforts made to change their behaviours. Therefore, numerous variables could be considered as responsivity factors. In the present study, we chose to examine demographic factors and mental health-related variables suggested as client-based responsivity factors by Bonta (Citation1995). Demographic data included sex, age, ethnicity (Norwegian vs foreign), and whether the youth had consented to placement. Clinical needs were of main interest to explore as there are considerable mental health needs among adolescents in residential care (Águila-Otero et al., Citation2020; Jozefiak et al., Citation2015; Seker et al., Citation2021) as well as young offenders in juvenile justice systems (Beaudry et al., Citation2021; Burke et al., Citation2015; Penner et al., Citation2011; Seker et al., Citation2021).
Procedure
Data were obtained from the national case journal system used by The Office for Children, Youth and Family Affairs and contained comprehensive information from standardised procedures carried out by a national intake unit. Before institutional placement all cases were assessed and evaluated by a team of psychologists using a comprehensive Risk-Need-Responsivity Analysis (RNR-A). Clinical information was acquired from the local social welfare services, case worker interviews and all other available sources (e.g. psychiatric journals, police reports). Based on this information, the psychologists conducted structural risk assessment, recognised strengths and vulnerabilities and identified the presence or absence of serious substance abuse problems. Based on an overall review of RNR-A as it applied to each individual case, the individuals were designated into three treatment categories: the Substance Abuse group (SA) included adolescents with serious and persistent substance abuse, the High- risk group (HR) included clients estimated to have high risk of continued delinquency, and the Low/Moderate-risk group (LMR) included clients who did not exhibit severe substance abuse and were judged to have either low or moderate risk of persistence of delinquent behaviour. As such, the RNR-A procedure included the professional override principle of classification incorporated in the YLS/CMI (Hoge & Andrews, Citation2011) and did not merely rely on risk scores.
Data on mental health status were registered as part of the RNR-A procedure; any verified ICD-10 diagnosis (WHO, Citation1993) assessed by mental health services (both in- and outpatient clinics) was extracted from individual case files provided by the local child welfare services. Comorbidity was coded if an individual had more than one mental health diagnosis registered. The case-assigned psychologist responsible for the RNR-A also registered reports of significant mental health concerns at intake that were not related to confirmed clinical diagnosis. Additionally, any documented reports of self-harming behaviour and subnormal (below average) cognitive functioning were coded in a binary fashion (yes = 1, no = 0). The level of cognitive functioning was based on information derived from psychiatric case files (most often psychometric tests of ability and intelligence from outpatient clinics).
To make meaningful comparisons as responsivity factors, the specific diagnoses were merged into broader ICD-10 diagnostic categories. ICD-10 does not have a formal ADHD diagnosis; however, the Norwegian Directorate of Health guidelines (Helsedirektoratet, Citation2021) for the diagnosis of hyperkinetic disorder states that criteria from DSM-5 (American Psychiatric Association, Citation2013) should be utilised. Hence, the identification of ADHD and related problems was performed by including diagnoses of category F90 hyperkinetic disorders. This group includes both Disturbance of activity and attention (F90.0), Hyperkinetic conduct disorder (F90.1) and other/unspecified hyperkinetic disorders (F90.8/F90.9). These disorders were combined into a group termed ADHD. The ICD-10 diagnoses of developmental disorders (F80-89) were merged into the category of neurodevelopmental disorders. The ICD-10 diagnoses of mental retardation (F70-79) were placed in the category of intellectual disability. ICD-10 mood disorders (F30-F39) and neurotic disorders (F40.0-F41.9) were combined into a category of depression and anxiety disorders. Disorders of adult personality (F60.0-60.9) were coded in the category personality disorders. All other diagnoses were merged onto a ΄Other psychiatric disorder΄ category.
Statistical analyses
Scores on the YLS/CMI total risk and subdomains were compared using linear regression with groups as categorical covariates, unadjusted, and adjusted for age and sex. We report only the unadjusted results since the adjusted results were substantially the same. For pairwise comparisons between the groups, we applied a closed test procedure to preserve the familywise error rate (Levin et al., Citation1994). This involves that the pairwise comparison p-value was replaced by the overall p value for the three-way group comparison when the latter was higher. The normality of residuals was checked by visual inspection of QQ plots. In some subdomains, there were minor deviations from normality. However, nonparametric tests gave substantially the same p values as parametric tests (data not shown), so we only report results from the parametric tests. Demographic and clinical responsivity variables in the three groups were compared using linear regression with group as a categorical covariate (one-way ANOVA), the Pearson chi-squared test, or the Fisher exact test, as appropriate. All tests were two-tailed, and the level of statistical significance was set at p < .05. The analyses were conducted using SPSS 27.
Ethics
Participants were recruited in accordance with procedures approved by the Norwegian Regional Committee for Medical and Health Research Ethics (REK) (reference number 347377). Archival data were obtained from a national electronic journal system used by The Office for Children, Youth and Family Affairs. Because obtaining consent was impracticable and infringements were minor and outweighed by the expected societal value, the project received permission to bypass common protocols of informed consent and information disclosure requirements. All data were managed on a secure platform and anonymized before analysis.
Results
Sample characteristics
The total sample consisted of 737 adolescents aged 12.1 years to 18.8 years with a mean (SD) age of 16.2 (1.2). There were 463 males with a mean (SD) age of 16.2 (1.2) years and 274 females with a mean age of 16.1 (1.2) years. The geographical distribution was representative of the demographic proportions of the five referring regions in Norway. shows the sample characteristics for all the variables in this study. The mean (SD) YLS/CMI total score was 20.7 (4.6), and the range was 28 (minimum 5, maximum 33). In the sample, 257 (34.9%) had a YLS/CMI total score over 22, which is the guiding cut-off for ΄high risk΄ classification provided by the manual (Hoge & Andrews, Citation2011). No participants scored in the ΄very high΄ risk level category (YLS/CMI total score >34). Only 7 (0.9%) had scores in the low risk level interval (0–8), and the remaining sample (64.2%) scored in the ΄moderate risk level΄ interval (9–22). Descriptive statistics showed that males were overrepresented and that most adolescents did not consent to services and were placed involuntarily. The clinical variables revealed that over half of the sample (56.3%) had one diagnosed mental health disorder prior to referral, and 63% had mental health concerns at intake that were not related to an earlier diagnosed disorder. ADHD was the most common diagnostic category in the sample. The diagnoses of depression and anxiety were relatively infrequent, and there were low rates of neurodevelopmental disorders, intellectual disability, and personality disorders.
Table 1. Total sample characteristics.
Comparing risk factors between subgroups
The Substance Abuse group (SA) accounted for 43.9% (324) of the individuals, while the Low/Moderate-risk group (LMR) accounted for 34.9% (257) of the individuals. The High-Risk group (HR) was the smallest group, accounting for 21.2% (156) of the individuals. The mean and standard deviation of the YLS/CMI domain scores and total scores by subgroup are presented in . YLS/CMI composite risk scores differed significantly between groups. Adolescents in SA had an average total score (20.8), fell between the HR group score (25.0) and LMR group score (18.0). Both the LMR and SA groups displayed mean risk scores in the upper end of the YLS/CMI moderate risk interval (9–22). Comparing group samples on the YLS/CMI subscales revealed significant differences between the groups except for the Family Circumstances/Parenting domain. The HR group scored highest on Offences/Dispositions, and the SA group scored highest on the Substance Abuse domain. On seven of the eight domains, the LMR group scored significantly lower than the HR group. Compared to the SA group, the LMR group scored significantly lower on Peer Relations, Leisure/Recreation, Attitudes/Orientation, and the Substance Abuse domain. However, the SA group had lower scores on the Personality/Behaviour domain. displays mean differences between subgroups on the eight YLS/CMI domains.
Figure 1. Mean differences between subgroups in YLS/CMI subdomains.
Note: Subdomains vary in scale and are not directly comparable.
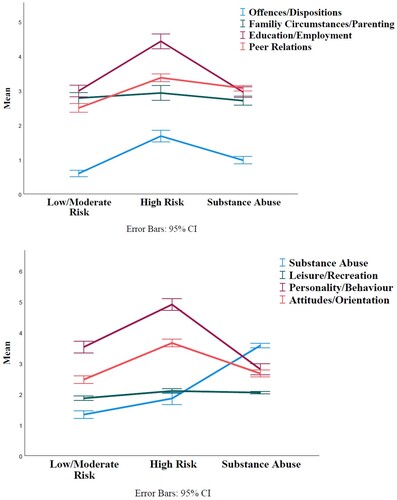
Table 2. Mean scores (SD) on YLS/CMI total risk and subdomains.
Comparing responsivity factors between subgroups
displays the demographic and clinical characteristics in the three groups. The High-Risk group (HR) and the Substance Abuse group (SA) had significantly lower rates of females (17.3% and 38.6%, respectively) than the Low/Moderate-risk group (LMR) (47.5%). The SA group differed significantly from the two other groups in terms of mean age (16.7), higher rates of consenting to placement (22.2%), and lower frequency of individuals with non-Norwegian ethnicity (12.0%). Regarding clinical variables, there were few statistically significant differences. The exception was a significantly lower frequency of depression and anxiety disorders (3.2%) and lower reports of mental health concerns at intake (53.2%) in the HR group.
Table 3. Demographic and clinical responsivity characteristics in the three groups, reported as n (%) unless otherwise noted.
Discussion
The study found that adolescents in TRC present with multiple needs in both criminogenic and clinical domains. The prevalence of risk factors was substantial, as nearly all the adolescents had total risk scores in either the moderate- or high-risk category in the YLS/CMI. Consistent with prior studies, subgroups had distinct risk profiles over and above accumulated risk levels, which demonstrated that adolescents in TRC have heterogeneous treatment needs. Subgroups differed significantly on both static risk (criminal history) and several dynamic risk domains in the YLS/CMI. This has important implications for clinical practice, as disparate risk profiles favour having intervention programmes differentiated by intensity and customised to the specific areas of risk and need that characterise the subgroups. In terms of responsivity factors, mental health-related problems were substantial in the sample, with over half of the sample having a diagnosed condition prior to referral. This is considerably higher than the estimated prevalence rate in the normal population of teens (Mykletun et al., Citation2009) but still lower than suggested rates from other residential studies utilising diagnostic interviews (Jozefiak et al., Citation2015). In contrast to risk factors, however, the clinical variables showed minimal differentiation across the subgroups and mental health should be considered important for responsivity among all adolescents in TRC.
Comparing risk factors in subgroups
YLS/CMI total risk level
The obtained total risk score gives an estimate of the likelihood that continued delinquent behaviour will occur if nothing is done to intervene. From a case management perspective, this cumulated score demonstrates the degree of problem severity in groups and informs how the general intensity level of interventions should be given. Notably, the Low/Moderate-risk group (LMR) and Substance Abuse group (SA) contained adolescents with mean scores that were classified within the moderate risk level according to the YLS/CMI taxonomy. While moderate-risk delinquents tend to have shorter criminal histories and less likelihood of future offending compared to their high-risk peers, they have numerous criminogenic needs in several areas (i.e. school, friends, substance use), which needs attention and systematic targeting to reduce the likelihood of future criminal behaviour (Vincent et al., Citation2012). The obtained frequency of risk factors in both the LMR and SA groups raise concerns about whether adolescents scoring within the lowest YLS/CMI risk category should be placed in TRC. Several treatment studies on risk differentiation show iatrogenic effects of mixing youths with different risk levels, especially on ‘low risk’ individuals (Bonta, Citation2009; Latessa et al., Citation2007; Lowenkamp et al., Citation2006; Lowenkamp & Latessa, Citation2004). In fact, studies have suggested there is up to 18% increase in recidivism for low-risk individuals when placed in residential facilities with higher-risk peers (Latessa et al., Citation2007). The negative effect of mixing residents with different risk levels are attributed to a social learning effect when exposing lower-risk clients to their high-risk counterparts. In our view, Norwegian residential services should only offer congregated TRC placements to adolescents identified with moderate risk levels and higher.
YLS/CMI domains
Beyond the cumulative risk levels, analysis of YLS/CMI subdomains revealed important group differences. These subgroup variations coincide with previous findings (Maneiro et al., Citation2019) and have practical implications in how institutions can target criminogenic needs. As expected, clients in the High-Risk (HR) group had superior scores related to prior offences and dispositions and on most of the dynamic risk domains. Elevated scores across domains signal severe problems and multiple criminogenic intervention needs, which requires intensive and multisystemic effort to reduce the likelihood of recidivism (Sperber et al., Citation2013). As such, the HR group should be offered the most comprehensive approach, including more specialised personnel and higher intensity systematic interventions.
As expected, the Substance Abuse group (SA) displayed a very high mean score in the Substance Abuse domain. Severe substance abuse is a destabilising factor in these adolescents, which adds to the complexity problems and could predict recidivism over and beyond risk level (van der Put et al., Citation2013). Therefore, efforts to reduce risk in this domain should be prioritised in the SA group. Matching needs to the right intensity of services on individuals with substance use disorders (SUD) has shown good outcomes in terms of reduction in use and less problem severity in multiple areas, such as mental health symptoms and family issues, compared to mismatched individuals (Stallvik et al., Citation2015).
Although clients in the Substance Abuse (SA) group and Low/Moderate-risk group (LMR) were classified in the overall same moderate risk level in YLS/CMI, the groups had disparate risk profiles. In addition to the Substance Abuse domain, the SA group had significantly higher scores on Offences/Dispositions, Peer Relations, and Leisure/Recreation. Reviewing the specific risk factors in these domains, this finding indicates that adolescents with substance abuse generally had higher rates of general offending, drug related offences, and more affiliation with delinquent social networks and less engagement in prosocial leisure activities at intake than the LMR group. The latter, however, received a higher score on Personality/Behaviour, which indicates that this group, on average, had more externalising and destructive behaviours than clients in the SA group.
Last and just as importantly, the scores on the Family Circumstances/Parenting domain suggest that adolescents in general have comparable intervention needs in this area (e.g. family problems, inadequate parental management, poor relations). This concurs with the findings that residential youth in general have more unfavourable family characteristics than the general population, such as lower parental education and income, parents’ need for social assistance and higher rates of family members with criminal history (Drange & Hærnes, Citation2020). As family risk factors are also suggested to be highly potent predictors of recidivism in juvenile offender (Mulder et al., Citation2010), there are good reasons for developing standardised procedures and creating professional recommendations for all TRC programmes to target family interventions to improve treatment goals.
Comparing responsivity factors in subgroups
Demographic variables
The results showed that there were relatively fewer females in both the Substance Abuse group (SA) and High-Risk group (HR) than the Low/Moderate-risk group (LMR), with the HR group having an especially low rate (17.3%). This overrepresentation of males in the HR group conforms to population-based statistics showing that young Norwegian males are more prone to criminal acts in general and have the highest prevalence of chronic reoffending in later life (Bhuller & Røgeberg, Citation2022; Drange et al., Citation2022). The SA group included adolescents with the highest age, which was approximately 17 years. This could be an essential responsivity feature, as verging adulthood entails less dependency on parents and family, a more self-reliance way of life, and a shift from youth services to adult-based social support and health care systems. Incorporating this transition into SA interventions could potentially facilitate sustaining the effects of treatment into adulthood.
The general low degree of consent in the sample suggests that an effort to increase motivation and adherence should be an important responsivity issue in all interventions. Implementing approaches like Motivational Interviewing (Miller & Rollnick, Citation2002) can effectively address this important responsivity aspect in all intervention. Nonetheless, SA showed relatively higher rates of consent to treatment than the two other groups, which could reflect that adolescents with severe substance abuse referred to residential care acknowledge their own problems to a higher degree and are motivated for change. A study by Battjes et al. (Citation2003) found that awareness of the negative consequences of substance use was related to motivation, suggesting the importance of interventions to help adolescents recognise the negative effects of their drug and alcohol use. As the SA group consisted of older individuals, this group might have experienced more adverse effects from drug use and more noticeable interference with physical, psychological, and social functioning.
The SA group also differed from the two other groups in having fewer adolescents with non-Norwegian ethnicity. Whether this reflects that referred youths with other cultural backgrounds have fewer problems with drug and alcohol use in general or that such problems are less detected/reported due to potential cultural stigmas should be investigated in future studies.
Mental health variables
Analysis of clinical variables showed a comparable prevalence of mental health-related needs across groups. Regardless of group status, over half of the individuals had a diagnosed mental health disorder, and ADHD was a highly prevalent disorder. While the High-Risk group (HR) had relatively lower rates of reported mental health concerns and fewer diagnosed anxiety and depression disorders, there were no significant group differences in any other clinical variables. This echoes the vast literature from juvenile justice, which recognises that mental disorders (Beaudry et al., Citation2021; Burke et al., Citation2015; Kinner et al., Citation2014; Penner et al., Citation2011), self-harm and suicidal behaviour (Moore et al., Citation2015; Stokes et al., Citation2015) are prevalent in young delinquents in general and that clinical variables do not differentiate in terms of criminogenic needs or recidivism risk (Guebert & Olver, Citation2014; Jäggi et al., Citation2021; McCormick et al., Citation2017).
Since mental health problems seem to be common among individuals in TRC, implementing standardised screening procedures at intake and discharge would enable institutions to identify clinical needs at the start of the treatment period and outcomes on discharge. Early detection of mental health problems could facilitate effective intercollaboration between child welfare and mental health services, which in turn, could make individuals respond better to risk-reducing interventions.
Clinical implications for practice and treatment
In general, the findings support the structuring of TRC interventions in line with the principles of Risk-Need-Responsivity model and that comprehensive and multisystemic treatment approaches spanning educational, social, and familial support are essential. A key clinical implication of the study is that interventions for adolescents in TRC should be targeted towards persistent delinquency (criminogenic needs) while also considering responsivity factors such as mental health needs when designing and implementing interventions. Results support differentiating subgroups of adolescents based on risk and needs, and that high-risk cases should be prioritised for high intensity interventions to reduce the likelihood of future delinquency. To avoid potential iatrogenic effects, it is advised not to offer congregated TRC services to individuals assessed with low risk levels.
Strengths and limitations
A major strength of this study was the use of a national sample from all regions of Norway containing a large set of individuals. This enhances the generalizability of the results, strengthens the findings, and provides a unique opportunity to highlight the complex needs in this population of youths. There were some limitations to this study that must be addressed. Risk assessment was conducted on secondary information from communal caseworkers and all available archival information. Interviewing the individuals could have brought additional nuances pertaining to information on risk, need and responsivity factors. Additionally, diagnostic data were obtained from prior contact with mental health services, and the absence of a diagnosis did not necessarily mean that the person did not have a diagnosable condition. Circumstances such as availability of services, individuals’ own motivation for receiving mental health services, and noncompleted health assessment, among other things, could impact the actual diagnosis reported. The same limitation could be regarded in the reports of cognitive functioning. Thus, the actual prevalence of these characteristics could be higher than the obtained rate. The study had a limitation in that it solely focused on risk factors in the YLS/CMI, without incorporating strength and protective factors assessed in the domains. Lastly, the study did not explore and differentiate delinquency risk in the Substance abuse group (SA). As such, this group consisted of both low/moderate and high-risk delinquency cases, and further exploration within this group could have identified additional in risk and need profiles.
Conclusion
This nationwide study was the first to describe and compare treatment needs in a representative sample of adolescents referred to therapeutic residential care (TRC) in Norway. The findings contribute to expanding the current knowledge about the complexity of needs in adolescents in residential services and adds to the growing body of literature suggesting that effective residential interventions should be aimed at risk factors for future delinquency and structured according to the principles of risk, need and responsivity to maximise the chances of positive outcomes.
Data sharing statement
Due to the sensitivity of the data, they are not publicly available.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Aase, H., Lønnum, K., Sørlie, M. A., Hagen, K. A., Gustavson, K., & Utgarden, I. H. (2020). Barn, unge og kriminalitet. Hvordan forhindre at barn og unge kommer inn i eller fortsetter med en kriminell løpebane? Oppsummering og vurdering av virksomme tiltak, behandling og organisering. https://www.fhi.no/contentassets/9edd82a6bff54e488870e612131bb242/barn-unge-og-kriminalitet-2020.pdf
- Águila-Otero, A., Bravo, A., Santos, I., & Fernández del Valle, J. (2020). Addressing the most damaged adolescents in the child protection system: An analysis of the profiles of young people in therapeutic residential care. Children and Youth Services Review, 112, 104923. https://doi.org/10.1016/j.childyouth.2020.104923
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
- Andreassen, T. (2015). Multifunc. In J. K. Whittaker, J. Fernández del Valle, & L. Holmes (Eds.), Therapeutic residential care for children and youth. Developing evidence-based international practice (pp. 100–110). Jessica Kingsley Publisher.
- Andrews, D. A., & Bonta, J. (2010). Rehabilitating criminal justice policy and practice. Psychology, Public Policy, and Law, 16(1), 39–55. https://doi.org/10.1037/a0018362
- Andrews, D. A., Bonta, J., & Hoge, R. D. (1990). Classification for effective rehabilitation: Rediscovering psychology. Criminal Justice and Behavior, 17(1), 19–52. https://doi.org/10.1177/0093854890017001004
- Andrews, D. A., Bonta, J., & Wormith, J. S. (2011). The risk-need-responsivity (RNR) model: Does adding the good lives model contribute to effective crime prevention? Criminal Justice and Behavior, 38(7), 735–755. https://doi.org/10.1177/0093854811406356
- Assink, M., van der Put, C. E., Hoeve, M., de Vries, S. L. A., Stams, G. J. J. M., & Oort, F. J. (2015). Risk factors for persistent delinquent behavior among juveniles: A meta-analytic review. Clinical Psychology Review, 42, 47–61. https://doi.org/10.1016/j.cpr.2015.08.002
- Baglivio, M. T., Wolff, K. T., Howell, J. C., Jackowski, K., & Greenwald, M. A. (2018). The search for the holy grail: Criminogenic needs matching, intervention dosage, and subsequent recidivism among serious juvenile offenders in residential placement. Journal of Criminal Justice, 55, 46–57. https://doi.org/10.1016/j.jcrimjus.2018.02.001
- Basto-Pereira, M., Villanueva, L., Peterson-Badali, M., Pimentel, A., Quintas, J., Cuervo, K., Hoge, R. D., & Skilling, T. A. (2021). Is a 7-item combination from the YLS/CMI an effective screening strategy for risk to reoffend? Findings from a cross-National study. Criminal Justice and Behavior, 48(5), 655–670. https://doi.org/10.1177/0093854821995866
- Battjes, R. J., Gordon, M. S., O'Grady, K. E., Kinlock, T. W., & Carswell, M. A. (2003). Factors that predict adolescent motivation for substance abuse treatment. Journal of Substance Abuse Treatment, 24(3), 221–232. https://doi.org/10.1016/S0740-5472(03)00022-9
- Beaudry, G., Yu, R., Långström, N., & Fazel, S. (2021). An updated systematic review and meta-regression analysis: Mental disorders among adolescents in juvenile detention and correctional facilities. Journal of the American Academy of Child & Adolescent Psychiatry, 60(1), 46–60. https://doi.org/10.1016/j.jaac.2020.01.015
- Berg, R. C., Johansen, T. B., Jardim, P. S. J., Forsetlund, L., & Ngyen, L. (2020). Interventions for children and youth with behavioral problems or criminal behavior: An overview of reviews. N. I. o. P. Health. https://www.fhi.no/globalassets/dokumenterfiler/rapporter/2020/tiltak-for-barn-og-unge-med-atferdsvansker-eller-som-har-begatt-kriminelle-handlinger-rapport-2020.pdf
- Bhuller, M., & Røgeberg, O. (2022). Kjennetegn ved barn og unge som begår kriminelle handlinger og virkninger av straff. https://www.regjeringen.no/contentassets/e8f0236bb0784a83911537df3d1fb9f2/rapport-ungdomskriminalitet.pdf
- Bonta, J. (1995). The responsivity principle and offender rehabilitation. Forum on Corrections Research, 7(3), 34–37.
- Bonta, J. (2009). Reserarch summary: What to do with low risk offenders. Public Safety Canada. https://www.publicsafety.gc.ca/cnt/rsrcs/pblctns/tdwth-lwrsk/tdwth-lwrsk-eng.pdf
- Bonta, J., & Andrews, D. A. (2017). The psychology of criminal conduct (6th ed.). Routledge.
- Bullock, R., & Gaehl, E. (2012). Children in care: A long-term follow up of criminality and mortality. Children and Youth Services Review, 34(9), 1947–1955. https://doi.org/10.1016/j.childyouth.2012.06.003
- Burke, J. D., Mulvey, E. P., & Schubert, C. A. (2015). Prevalence of mental health problems and service use among first-time juvenile offenders. Journal of Child and Family Studies, 24(12), 3774–3781. https://doi.org/10.1007/s10826-015-0185-8
- the Child Welfare Act. (1992). https://lovdata.no/dokument/NL/lov/1992-07-17-100
- Cuervo, K., Villanueva, L., & Basto-Pereira, M. (2020). Prediction of youth and adult recidivism among spanish juveniles involved in serious offenses. Criminal Justice and Behavior, 47(4), 399–418. https://doi.org/10.1177/0093854819897282
- Deloitte. (2019). Kartlegging av institusjonstilbud i Norge og utvalgte europeiske land. https://bibliotek.bufdir.no/BUF/101/Kartlegging_av_institusjonstilbud_i_Norge_og_utvalgte_europeiske_land%20.pdf
- Drange, N., & Hærnes, Ø. M. (2020). Kvantitativ beskrivelse av institusjonspopulasjonen. (https://www.frisch.uio.no/publikasjoner/pdf/rapp20_03.pdf
- Drange, N., Hernæs, Ø. M., Markussen, S., Oterholm, I., Raaum, O., & Slettebø, T. (2022). Barn, unge og familier i barnevernet - En longitudinell registerstudie. Delprosjekt 2: Hvordan går det med barna? https://www.frisch.uio.no/publikasjoner/pdf/rapp22_02.pdf
- Greger, H. K., Myhre, A. K., Lydersen, S., & Jozefiak, T. (2015). Previous maltreatment and present mental health in a high-risk adolescent population. Child Abuse & Neglect, 45, 122–134. https://doi.org/10.1016/j.chiabu.2015.05.003
- Greger, H. K., Myhre, A. K., Lydersen, S., & Jozefiak, T. (2016). Child maltreatment and quality of life: A study of adolescents in residential care. Health and Quality of Life Outcomes, 14(1), 74–74. https://doi.org/10.1186/s12955-016-0479-6
- Guebert, A. F., & Olver, M. E. (2014). An examination of criminogenic needs, mental health concerns, and recidivism in a sample of violent young offenders: Implications for risk, need, and responsivity. International Journal of Forensic Mental Health, 13(4), 295–310. https://doi.org/10.1080/14999013.2014.955220
- Harder, A. T., & Knorth, E. (2015). Uncovering what is inside the “black box” of effective therapeutic residential youth care. In J. K. Whittaker, J. Fernández del Valle, & L. Holmes (Eds.), Therapeutic residential care for children and youth. Developing evidence-based international practice (pp. 217–228). Jessica Kingsley Publisher.
- Helsedirektoratet. (2021). Kriterier fra DSM-5 bør brukes i diagnostisering av ADHD/hyperkinetisk forstyrrelse, selv om det skal kodes etter ICD-10 (Criteria from DSM-5 should be used in the diagnosis of ADHD/hyperkinetic disorder, even if it should be coded according to ICD-10). Retrieved January 8, 2023, from https://www.helsedirektoratet.no/retningslinjer/adhd/henvisning-utredning-og-tilbakemelding/kriterier-fra-dsm-5-bor-brukes-i-diagnostisering-av-adhd-hyperkinetisk-forstyrrelse-selv-om-det-skal-kodes-etter-icd-10
- Hillege, S. L., Brand, E. F. J. M., Mulder, E. A., Vermeiren, R. R. J. M., & van Domburgh, L. (2017). Serious juvenile offenders: Classification into subgroups based on static and dynamic charateristics. Child and Adolescent Psychiatry and Mental Health, 11(1), 67–67. https://doi.org/10.1186/s13034-017-0201-4
- Hoge, R. D., & Andrews, D. A. (2011). Youth level of service/case management inventory. 2.0 manual. Multi-Health System Inc.
- Jäggi, L., Schmid, M., Bürgin, D., Saladin, N., Grob, A., & Boonmann, C. (2021). Shared residential placement for child welfare and juvenile justice youth: Current treatment needs and risk of adult criminal conviction. Child and Adolescent Psychiatry and Mental Health, 15(1), 2–2. https://doi.org/10.1186/s13034-020-00355-1
- Johansen, T. B., Jardim, P. S. J., Blaasvær, N., Ames, H., Munthe-Kaas, H. M., Tingulstad, A., & Berg, R. C. (2020). Quality care in residential childcare institutions: a systematic scoping review. https://www.fhi.no/en/publ/2020/Quality-care-in-residential-childcare-institutions/
- Jozefiak, T., Kayed, N. S., Ranøyen, I., Greger, H. K., Wallander, J. L., & Wichstrøm, L. (2017). Quality of life among adolescents living in residential youth care: Do domain-specific self-esteem and psychopathology contribute? Quality of Life Research, 26(10), 2619–2631. https://doi.org/10.1007/s11136-017-1603-8
- Jozefiak, T., Kayed, N. S., Rimehaug, T., Wormdal, A. K., Brubakk, A. M., & Wichstrøm, L. (2015). Prevalence and comorbidity of mental disorders among adolescents living in residential youth care. European Child & Adolescent Psychiatry, 25(1), 33–47. https://doi.org/10.1007/s00787-015-0700-x
- Kinner, S. A. P. D., Degenhardt, L. P. D., Coffey, C. P. D., Sawyer, S. M. D., Hearps, S. P. G. D. P., & Patton, G. M. D. (2014). Complex health needs in the youth justice system: A survey of community-based and custodial offenders. Journal of Adolescent Health, 54(5), 521–526. https://doi.org/10.1016/j.jadohealth.2013.10.003
- Koehler, J. A., Lösel, F., Akoensi, T. D., & Humphreys, D. K. (2013). A systematic review and meta-analysis on the effects of young offender treatment programs in Europe. Journal of Experimental Criminology, 9(1), 19–43. https://doi.org/10.1007/s11292-012-9159-7
- Lanza, S. T. P. D., Cooper, B. R. P. D., & Bray, B. C. P. D. (2014). Population heterogeneity in the salience of multiple risk factors for adolescent delinquency. Journal of Adolescent Health, 54(3), 319–325. https://doi.org/10.1016/j.jadohealth.2013.09.007
- Latessa, E., Smith, P., & Bechtel, K. (2007). Reducing the harm: Identifying appropriate programming for low-risk offenders. Corrections Today, 69, 50–52.
- Lehmann, S., & Kayed, N. S. (2018). Children placed in alternate care in Norway: A review of mental health needs and current official measures to meet them. International Journal of Social Welfare, 27(4), 364–371. https://doi.org/10.1111/ijsw.12323
- Leloux-Opmeer, H., Kuiper, C. H. Z., Swaab, H. T., & Scholte, E. M. (2017). Children referred to foster care, family-style group care, and residential care: (How) do they differ? Children and Youth Services Review, 77, 1–9. https://doi.org/10.1016/j.childyouth.2017.03.018
- Levin, J. R., Serlin, R. C., & Seaman, M. A. (1994). A controlled, powerful multiple-comparison strategy for several situations. Psychological Bulletin, 115(1), 153–159. https://doi.org/10.1037/0033-2909.115.1.153
- Lipsey, M. W. (2009). The primary factors that characterize effective interventions with juvenile offenders: A meta-analytic overview. Victims & Offenders, 4(2), 124–147. https://doi.org/10.1080/15564880802612573
- Lloyd, C. D., Hanby, L. J., & Serin, R. C. (2014). Rehabilitation group coparticipants’ risk levels are associated with offenders’ treatment performance, treatment change, and recidivism. Journal of Consulting and Clinical Psychology, 82(2), 298–311. https://doi.org/10.1037/a0035360
- Lowenkamp, C. T., & Latessa, E. (2004). Understanding the risk principle: How and why correctional interventions can harm low risk offenders. Technical Report.
- Lowenkamp, C. T., Latessa, E. J., & Holsinger, A. M. (2006). The risk principle in action: What have We learned from 13,676 offenders and 97 correctional programs? Crime and Delinquency, 52(1), 77–93. https://doi.org/10.1177/0011128705281747
- Luong, D., & Wormith, J. S. (2011). Applying risk/need assessment to probation practice and its impact on the recidivism of young offenders. Criminal Justice and Behavior, 38(12), 1177–1199. https://doi.org/10.1177/0093854811421596
- Maneiro, L., Gómez-Fraguela, J. A., López-Romero, L., Cutrín, O., & Sobral, J. (2019). Risk profiles for antisocial behavior in adolescents placed in residential care. Children and Youth Services Review, 103, 278–286. https://doi.org/10.1016/j.childyouth.2019.06.012
- McCormick, S., Peterson-Badali, M., & Skilling, T. A. (2017). The role of mental health and specific responsivity in juvenile justice rehabilitation. Law and Human Behavior, 41(1), 55–67. https://doi.org/10.1037/lhb0000228
- Miller, W. R., & Rollnick, S. (2002). Motivational interviewing: Preparing people for change (2nd ed.). The Guilford Press.
- Moffitt, T. E. (2018). Male antisocial behaviour in adolescence and beyond. Nature Human Behaviour, 2(3), 177–186. https://doi.org/10.1038/s41562-018-0309-4
- Moore, E., Gaskin, C., & Indig, D. (2015). Attempted suicide, self-harm, and psychological disorder among young offenders in custody. Journal of Correctional Health Care, 21(3), 243–254. https://doi.org/10.1177/1078345815584849
- Mulder, E., Brand, E., Bullens, R., & Marle, H. (2019). Toward a classification of juvenile offenders: Subgroups of serious juvenile offenders and severity of recidivism. International Journal of Offender Therapy and Comparative Criminology, 63(6), 819–836. https://doi.org/10.1177/0306624X10387518
- Mulder, E., Brand, E., Bullens, R., & van Marle, H. (2010). Profiling serious juvenile offenders in juvenile institutions: Change in risk factors in their population. International Journal of Forensic Mental Health, 9(2), 93–100. https://doi.org/10.1080/14999013.2010.499554
- Mykletun, A., Knudsen, A. K., & Mathiesen, K. S. (2009). Psykiske lidelser i norge: Et folkehelseperspektiv. N. folkehelseinstitutt. https://www.fhi.no/globalassets/dokumenterfiler/rapporter/2009-og-eldre/rapport-20098-pdf-.pdf
- Onifade, E., Davidson, W., Livsey, S., Turke, G., Horton, C., Malinowski, J., Atkinson, D., & Wimberly, D. (2008). Risk assessment: Identifying patterns of risk in young offenders with the youth level of service/case management inventory. Journal of Criminal Justice, 36(2), 165–173. https://doi.org/10.1016/j.jcrimjus.2008.02.006
- Ortega-Campos, E., García-García, J., De La Fuente-Sánchez, L., & Zaldívar-Basurto, F. (2020). Predicting risk of recidivism in spanish young offenders: Comparative analysis of the SAVRY and YLS/CMI. Psicothema, 32, 221–228. https://doi.org/10.7334/psicothema2019.275
- Penner, E. K., Roesch, R., & Viljoen, J. L. (2011). Young offenders in custody: An international comparison of mental health services. International Journal of Forensic Mental Health, 10(3), 215–232. https://doi.org/10.1080/14999013.2011.598427
- Prendergast, M. L., Pearson, F. S., Podus, D., Hamilton, Z. K., & Greenwell, L. (2013). The Andrews’ principles of risk, needs, and responsivity as applied in drug treatment programs: Meta-analysis of crime and drug use outcomes. Journal of Experimental Criminology, 9(3), 275–300. https://doi.org/10.1007/s11292-013-9178-z
- Rivenbark, J. G., Odgers, C. L., Caspi, A., Harrington, H., Hogan, S., Houts, R. M., Poulton, R., & Moffitt, T. E. (2018). The high societal costs of childhood conduct problems: Evidence from administrative records up to age 38 in a longitudinal birth cohort. Journal of Child Psychology and Psychiatry, 59(6), 703–710. https://doi.org/10.1111/jcpp.12850
- Ryan, J. P. (2012). Substitute care in child welfare and the risk of arrest: Does the reason for placement matter? Child Maltreatment, 17(2), 164–171. https://doi.org/10.1177/1077559512443125
- Seker, S., Habersaat, S., Boonmann, C., Palix, J., Jenkel, N., Fischer, S., Fegert, J. M., Kölch, M., Schmeck, K., & Schmid, M. (2021). Substance-use disorders among child welfare and juvenile justice adolescents in residential care: The role of childhood adversities and impulsive behavior. Children and Youth Services Review, 121, 105825. https://doi.org/10.1016/j.childyouth.2020.105825
- Sperber, K. G., Latessa, E. J., & Makarios, M. D. (2013). Examining the interaction between level of risk and dosage of treatment. Criminal Justice and Behavior, 40(3), 338–348. https://doi.org/10.1177/0093854812467942
- Stallvik, M., Gastfriend, D. R., & Nordahl, H. M. (2015). Matching patients with substance use disorder to optimal level of care with the ASAM criteria software. Journal of Substance use, 20(6), 389–398. https://doi.org/10.3109/14659891.2014.934305
- Stokes, M. L., McCoy, K. P., Abram, K. M., Byck, G. R., & Teplin, L. A. (2015). Suicidal ideation and behavior in youth in the juvenile justice system: A review of the literature. Journal of Correctional Health Care, 21(3), 222–242. https://doi.org/10.1177/1078345815587001
- van der Put, C. E., Creemers, H. E., & Hoeve, M. (2013). Differences between juvenile offenders with and without substance use problems in the prevalence and impact of risk and protective factors for criminal recidivism. Drug and Alcohol Dependence, 134, 267–274. https://doi.org/10.1016/j.drugalcdep.2013.10.012
- Vaswani, N., & Merone, L. (2014). Are there risk with risk assessement? A study of the predictive accuracy of the youth level of service-case management inventory with young offenders in Scotland. British Journal of Social Work, 44(8), 2163–2181. https://doi.org/10.1093/bjsw/bct059
- Vieira, T. A., Skilling, T. A., & Peterson-Badali, M. (2009). Matching court-ordered services with treatment needs: Predicting treatment success with young offenders. Criminal Justice and Behavior, 36(4), 385–401. https://doi.org/10.1177/0093854808331249
- Vincent, G. M., Guy, L. S., & Grisso, T. (2012). Risk assessment in juvenile justice: A guidebook for implementation. MacArthur Fundation. https://modelsforchange.net/publications/346/
- Whittaker, J. K., Fernandez del Valle, J., Holmes, L., & Gilligan, R. (2015). Therapeutic residential care for children and youth: Developing evidence-based international practice. Jessica Kingsley Publishers.
- World Health Organization (WHO). (1993). The ICD-10 classification of mental and behavioural disorders. World Health Organization.
- Wormith, J. S., & Zidenberg, A. M. (2018). The historical roots, current status, and future applications of the risk-need-responsivity model (RNR). In E. L. Jeglic & C. Calkins (Eds.), New frontiers in offender treatment: The translation of evidence-based practices to correctional settings (pp. 11–41). Springer International Publishing. https://doi.org/10.1007/978-3-030-01030-0_2