
Abstract
Background: Currently the majority of cancer deaths occur in low- and middle-income countries, where there are appreciable funding concerns. In Kenya, most patients currently pay out of pocket for treatment, and those who are insured are generally not covered for the full costs of treatment. This places a considerable burden on households if family members develop cancer. However, the actual cost of cancer treatment in Kenya is unknown. Such an analysis is essential to better allocate resources as Kenya strives towards universal healthcare.
Objectives: To evaluate the economic burden of treating cancer patients.
Method: Descriptive cross-sectional cost of illness study in the leading teaching and referral hospital in Kenya, with data collected from the hospital files of sampled adult patients for treatment during 2016.
Results: In total, 412 patient files were reviewed, of which 63.4% (n = 261) were female and 36.6% (n = 151) male. The cost of cancer care is highly dependent on the modality. Most reviewed patients had surgery, chemotherapy and palliative care. The cost of cancer therapy varied with the type of cancer. Patients on chemotherapy alone cost an average of KES 138,207 (USD 1364.3); while those treated with surgery cost an average of KES 128,207 (1265.6), and those on radiotherapy KES 119,036 (1175.1). Some patients had a combination of all three, costing, on average, KES 333,462 (3291.8) per patient during the year.
Conclusion: The cost of cancer treatment in Kenya depends on the type of cancer, the modality, cost of medicines and the type of inpatient admission. The greatest contributors are currently the cost of medicines and inpatient admissions. This pilot study can inform future initiatives among the government as well as private and public insurance companies to increase available resources, and better allocate available resources, to more effectively treat patients with cancer in Kenya. The authors will be monitoring developments and conducting further research.
Introduction
Cancer results in high morbidity and mortalityCitation1. In 2012, it was estimated that ∼14 million new cases of cancer worldwide were diagnosed, with 8.2 million deaths due to cancerCitation2,Citation3. There were 8.8 million deaths due to cancer in 2015, with mortality due to cancer projected to rise to 13 million deaths a year by 2030 due to population growth and its ageing, an increase in infection rates, as well as an increase in unhealthy lifestyles known to cause cancerCitation3,Citation4. The majority of cancer deaths are now seen in middle- and low-income countries (LMICs)Citation2,Citation5, with LMICs currently accounting for ∼57% of cancer cases worldwide and ∼65% of cancer deathsCitation3. Other authors have suggested up to 70% or more of the burden of cancer is now among LMICsCitation5,Citation6. Cancer mortality in LMICs is enhanced by late diagnosis, as well as a lack of finances to fund appropriate careCitation2,Citation3. Having said this, in higher income countries there appears to be a limited correlation between resources spent and reduced mortality, with issues such as efficiency, patient centred care and timely treatment more importantCitation7.
In sub-Sahara Africa, the most common cancers affecting women are breast and cervical cancers, with equal incidence, although cervical cancer leads to more deaths aided by infection; whilst, among men, prostate and liver cancer are the most common, and cause more deathsCitation2,Citation3. Prevalence rates are expected to more than double between 2008 and 2030, with the number of new patients developing cancer expected to rise to 1.6 million by 2030Citation5. In Kenya in 2012 there were ∼41,000 new cases of cancer, with 28,453 deathsCitation4,Citation8, making cancer the third highest cause of mortality after infectious and cardiovascular diseases, at ∼7%Citation8. Others, though, have suggested higher incidence rates in Kenya, at ∼82,000 new cancer patients annually, which may be due to improvements in disease detection and characterizationCitation6.
Among women in Kenya, breast cancer (34 cases per 100,000) and cervical cancer (25 per 100,000) are the leading cancers, with prostate cancer (17 cases per 100,000) and esophageal cancer (nine cases per 100,000) the leading cancers in menCitation6. There are, though, appreciable differences in incidence rates among the different ethnic groups in KenyaCitation9. For children, the most common cancers are leukemia, brain and other central nervous system cancer, and lymphomas. Childhood cancers accounted for 15% of cancer admissions at the leading tertiary hospital in Kenya, with currently only one in 10 children surviving cancer in Kenya compared with rates of seven in 10 or higher among developed countriesCitation4,Citation6. However, these disparities in survival are likely to be multifactorial.
The lack of adequate healthcare personnel and diagnostic equipment in Kenya has impacted on survival rates among diagnosed cancer patients. Currently there are only four radiation oncologists, six medical oncologists, and four pediatric oncologists located in the leading hospitals in Kenya, with ongoing concerns when machinery such as radiation equipment breaks downCitation6,Citation10. Some authors, though, have suggested higher figures, with a total of 22 oncologists currently in KenyaCitation4. These numbers will grow, with currently five new cancer centres being planned in Kenya, including those outside NairobiCitation4.
There are also issues of affordability, with high costs of care, including physician visits, medicines, laboratory tests, surgery, and other treatment modalities including radiationCitation11. The cost for one radiotherapy session at US$5–10 in the public hospital can be prohibitively expensive for disadvantaged Kenyans, who typically live on US$1 per day or lessCitation10,Citation12,Citation13. The current estimated average costs of treating patients with cancer in Kenya, at US$1,600–$5,000, is a major concern, as this would be unaffordable for most KenyansCitation10, with only the wealthy able to fully afford treatmentCitation10,Citation14. The type of insurance cover patients have is a major contributor to possible treatment approaches since, even if patients can afford insurance, which is a minority, some insurance policies do not cover all cancer medicines and diagnostic tests, with some limiting the number of chemotherapy courses a yearCitation4,Citation14. Overall, treatment costs depend on many factors including the type of cancer, the type of treatment, the length of therapy and even the location of therapy.
The cost of medicines is a major concern in LMICs countries including Kenya and worldwide, as typically there are high co-payment levels and low incomesCitation5,Citation14–16. Prices of cancer medicines have risen up to 10-fold during the past 10 years in some countries, despite often limited health gainCitation17–23, although this is not universalCitation24. Having said this, some pharmaceutical companies are giving up their patents for biological medicines to ease the patient burden, as seen in India with trastuzumabCitation5. However, this is not universal among LMICs, with, for instance, trastuzumab in Botswana currently only benefiting 3% of its cancer patients, but consuming 43% of its entire cancer budgetCitation4. Having said this, such practices may grow, with estimates suggesting that the cost of production of even some newer cancer medicines may be as low as 1% of the selling priceCitation25. In Kenya, chemotherapy typically costs between KES6,000 (US$60) and KES600,000 (US$600) per treatment course in public hospitals, depending on the cancer being treatedCitation13; however, even these costs may be prohibitive to some patients, affecting their subsequent careCitation26. Costs to patients can be further increased with initial misdiagnosisCitation13.
Since most patients in Kenya are not insured, and hence pay out-of-pocket for their care, this has important implications on timing when they seek treatment and the type of treatment they chooseCitation27. As mentioned, current costs of cancer care impoverish many Kenyans as they struggle to acquire the funds for treatment. Consequently, there is an urgent need to improve the knowledge of treatment costs to help guide patients with cancer and the government on potential ways forward, as exact costs are currently unknownCitation28. Such information can better enable the government and donors to allocate more resources to cancer therapy if needed, and to patients to better understand possible costs. We believe such information will also help hospitals in Kenya to improve their waiver systems for selected cancer patients to ensure more accessible and affordable therapy to enhance equity and improve outcomes. This is important whilst Kenya strives towards universal healthcare.
Consequently, the main objective of this pilot study is to start to quantify the cost of treatment of cancer patients in Kenyatta National Hospital (KNH), the leading referral hospital for cancer patients in Kenya. This includes direct medical costs, including the costs of medicines, laboratory tests, radiation, and surgery.
Methodology
Study design, duration and site
A descriptive cross-sectional study was carried out in the oncology unit at the Kenyatta National Hospital (KNH) between January and March 2017. The cost of illness study involved quantifying the direct medical costs involved in cancer treatment and care. The documented costs were those that the patients incurred during the time they visited the hospital in 2016. The actual time periods for different patients varied, depending on the type and cycle of medication (chemotherapy) that they were on.
Kenya National Guidelines on Cancer Management (2013) exist, and current treatments are typically based on these guidelinesCitation29. These guidelines have been adapted from the World Health Organization (WHO) guidelines on cancer management.
Study site
The study was carried out at KNH, the largest referral and teaching hospital in Kenya. KNH treats various types of cancers affecting Kenyans in both the pediatric and adult settings. Moreover, most cancer patients in Kenya are currently referred to this hospital. The hospital has a specialized oncology unit, with most oncology specialists in Kenya currently working in this hospital.
Study population
The study population were adults above 18 years of age being treated for different cancers at KNH in 2016. The patients’ files were used to collect the data. Pediatric patients were excluded, since patients were consulted in case additional data on resource use were required, and it was believed that it would be unfeasible to collect this information in children as frequently as pediatric patients would not have their parents or guardians present at the hospital at questioning. Consequently, it was predicted that missing cost information would introduce bias and it was best to avoid this in this pilot study. In addition, the vast majority of cancer cases in Kenya currently occur in adultsCitation8.
The sample size could not be easily calculated for the cross-sectional study, as there are no prevalence studies that have been undertaken for Nairobi, since patients treated at KNH are sourced from across Kenya. However, from the KNH cancer registry of 2014–2016Citation30, it was recorded that 4,211 cancer patients were treated in that year. Using this estimate we decided to pick one out of every 10 files from the registry, from which we obtained our pilot sample size of 412 patients, after excluding those that did not meet the inclusion criteria. Sampling has also been undertaken in other LMIC countries to assess the extent of prescribing of chemotherapy agents for patients with cancerCitation31.
According to the KNH Cancer registry, which was established in 2014, KNH attends to an average of over 550,000 outpatients annually, and over 80,000 inpatients per year. The registry estimates the total number of cancer patients between this period (2014–2016) at 10,335, with the majority being women, at 6,279, leaving 4,056 menCitation30. The most common cancer among females at KNH is cervical cancer (n = 1,800), followed by breast cancer (n = 1,500). The most common for men are esophageal and prostate cancer, in equal numbers (n = 480 each). The leading cause of hospitalization in KNH in the years 2015 and 2016 was cancerCitation30.
Data collection
The collection of data was undertaken with the aid of a data collection tool, including the patients’ treatment history (Appendix 1). The data collected included patient demographics, medicines prescribed and their costs, cost of radiologic tests, costs of laboratory tests, any surgery and associated costs, as well as the quantity and costs of any medical devices used.
The information on the costs of medicines used during in-patient care were obtained from the expenditure and revenue collection unit for the oncology department of KNH. The costs of surgery in both the public and private sectors was based on current charges, with typically some subsidization of costs in the public sector. These data were also collated from the revenue collection documents of the oncology department at KNH. Where information could not be obtained from patient records, for example, the costs of medical devices, patients were contacted and asked about these costs. The costs of radiotherapy and medical devices, as well as other pertinent additional costs, were obtained by history taking from the patients. This is because such costs could not be obtained from the KNH Oncology Department expenditure and revenue collection records. Where the services and medical devices could not be obtained from KNH, the patients procured these from other private facilities and paid for them out of pocket. This data was also recorded.
We used a conversion rate of USD 1 = KES 101.3 (Central bank of Kenya - www.centralbank.go.ke/forex/) (correct as of May 2018).
Data management and quality assurance
The data were pre-tested in a pilot study of 10 patients to ensure the feasibility of the study and its methodology, as well as give a trend on the overall cost of therapy. All the data collected were recorded in a questionnaire. The data were cleaned and any errors or omissions corrected. The data was then transferred onto Excel spreadsheets, only accessed by the investigator and analysts. Backup of the data collected was undertaken every day. A qualified statistician was selected for the data analysis and quality assurance.
Descriptive data analysis was undertaken, and the results presented in figures, percentages, and proportions. The data obtained was analyzed using STATA v13.0 (Stata Corporation, TX).
Ethical considerations
The approval to carry out the study was sought from KNH-UON Ethics and Research Committee. Informed consent was sought from the Kenyatta Hospital Records management before conducting the study. In order to ensure confidentiality, serial numbers were used instead of patient names or in-patient numbers or out-patient numbers, so as to ensure the data remains confidential. All data collected was kept secure, and could only be accessed by the investigator.
Results
Of the 412 patients reviewed, 261 (63.4%) were female, and the remaining 151 were male. A small percentage of reviewed patients treated for cancer in 2016 (16%) died of their disease; however, the majority of patients were still undergoing treatment at the time of the study.
Of the reviewed patients, most of them were treated in the public wing (89.8%), with only a small percentage treated in the private wing of KNH. This reflects the fact that the public wing of KNH handles a considerable volume of patients vs the private wing. However, patients in the private wing pay more for their treatment.
Surgery (25.4%) was the most frequently used treatment modality, followed by chemotherapy (24.6%) and palliative care (21.7%), with radiotherapy used in only a few cases (6.3%). A combination of any of the three modalities was seen in only a few cases, i.e. of the 154 patients on chemotherapy:
96 had chemotherapy alone,
36 had chemotherapy and surgery,
14 had chemotherapy plus radiotherapy, and
eight had chemotherapy plus surgery plus radiotherapy
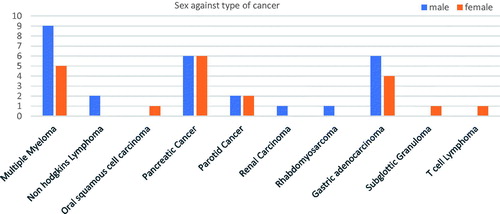
Among the sampled patients, the most prevalent cancers among men were prostate cancer (9.7%, n = 40) and colon cancer (2.9%, n = 12). The most prevalent cancers among women were cervical cancer (23.78%, n = 98) and breast cancer (7.28%, n = 30). There were also cancers that affected both men and women at approximately the same rate. These included esophageal cancer, chronic myeloid lymphoma, colorectal cancer, pancreatic cancer and glioblastoma. This is shown in .
Figure 1. Gender distribution of different types of cancer.
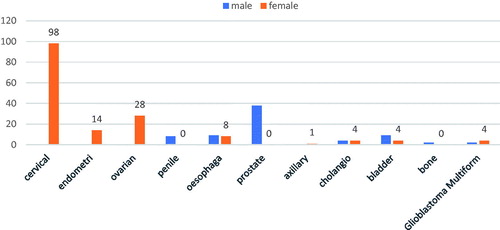
Figure 2. Gender distribution of different types of cancer (cont.).
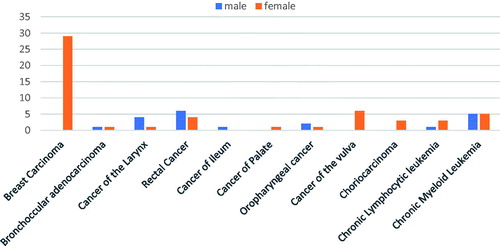
Figure 3. Gender distribution of different types of cancer (cont.).
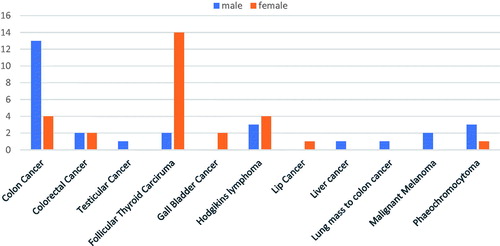
Figure 4. Gender distribution of different types of cancer (cont.).
The average cost of treatment for all the reviewed cases treated was KES 143,132 (USD1412.95) (). The highest contributors to the cost of cancer therapy are the cost of medicines and inpatient admissions (). The cost of medical devices can also be high in view of equipment costs, at a minimum of KES 5,500; however, this applied to only relatively few cases. documents the average costs incurred for the various modalities in treating patients with cancer in KNH in 2016.
Table 1. Average cost of cancer care in KNH (2016).
Table 2. Average cost of cancer therapy in 2016 in KNH.
Surgery is an important mode of treatment of cancer used, with higher costs when combined with other modes of therapy. The only surgical procedures carried out in the selected cohort of patients during the observation period were hysterectomy, radical mastectomy, laparotomy, colectomy and thyroidectomy. For colon cancer patients, a colectomy was performed. No surgery was undertaken for patients with prostate cancer during the observation period. Some cervical cancer patients (n = 10) also underwent a laparotomy for diagnostic purposes. Overall, the most expensive procedures were surgery combined with radiotherapy and chemotherapy (). depicts the current costs (charges) for common surgical procedures in both the public and private sectors in Kenya in 2017.
Table 3. Cost of commonly used surgeries during therapy in KNH in 2017.
The cost for using the theater and consumables during the surgery was charged separately. The theater charge was KES 2,000, while the theater consumables vary with the patient.
Radiological procedures vary from those used for diagnosis and monitoring to the use of radiotherapy as part of treatment. Radiotherapy as part of the treatment regimen is the most expensive, costing an average of KES 31,769 per patient, with the cost of radiotherapy appreciably increasing when used with other treatment modalities (). contains the cost of common laboratory tests undertaken during treatment in 2016.
Table 4. Cost of common laboratory tests offered during therapy in 2016.
The cost of nursing includes the cost of catheterization, nebulization, wound dressing, and drug infusion, among others. The cost of such services depends on the type of admission the patient used (public or private ward admission).
A number of drug regimens are used for various cancers, based principally on current national guidelinesCitation29. The most expensive drug regimen used during the observational period was fluorouracil and actinomycin D, costing KES 2,224,990 per patient (), while the cheapest was fluorouracil alone, which cost KES 30,580.
Table 5. Average cost of chemotherapy regimens in 2016.
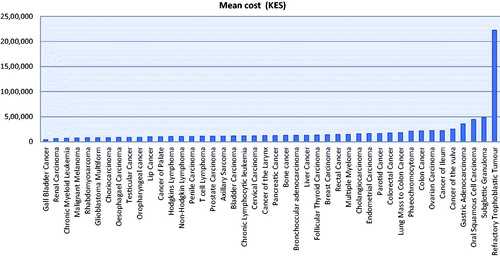
The cost of treating each type of cancer during 2016 depends on the type of cancer, its stage, and treatment approaches. The most expensive cancer treated was a refractory trophoblastic tumor (KES 2,224,990), followed by subglottic granuloma, which costed KES 486,876 per patient, whilst the cheapest included renal carcinoma, which cost KES 68,017 (). Appendix 2 contains more details, including the number of patients with the different cancers and the mean cost in USD.
Figure 5. Average cost of treating different types of cancer (KES).
The cost of treating patients with cancer during 2016 was appreciably higher in the private sector than in the public sector for the same mode of therapy, with variations ranging from KES 15,369 to KES 602,991, depending on the treatment involved ().
Table 6. Cost variations in KES between the private and public sectors (USD in parentheses).
Discussion
Out of the 412 reviewed cancer cases, 63% were female and 37% were male. This corresponds to a study by Korir et al.Citation32, which reported a higher incidence of cancer in females than males in Kenya. The cancer rate for women is 231 per 100,000 people, while the rate for men is 161 per 100,000 people in an age standardized incidence rate studyCitation32. Our findings also corroborate the data on the Kenyatta National Hospital Registry (2014–2016), which reported that there were more females than males currently being treated for cancer in KenyaCitation30. In this period, cancer remained the main cause for hospitalization in KNH. This finding was different from a middle-income country such as Iran, where more men than women were receiving chemotherapyCitation31.
In East Africa, 116,800 men and 170,500 women were diagnosed with cancer in 2012. Of all the cases diagnosed that year, 92,500 men and 116,500 women died as a result of cancer. Statistics, therefore, suggest that cancer morbidity and mortality effects women more than menCitation33. This could be attributed to the health-seeking behaviour of women, who are more likely to seek treatment than men, as well as perhaps greater prevalence of overweight and obesity, as seen for instance in other African countriesCitation34. Women are also more likely to be on hormonal contraceptives, which could be an etiological factor in promoting the growth of hormone-dependent cancers, although studies on their role are conflictingCitation35–38.
The cost of treating cancer in our study depended on the type of cancer, the chemotherapy regimen prescribed, the radiotherapy sessions prescribed, as well as the numerous laboratory and radiologic tests that the patients should undergo during diagnosis and treatment. Regarding the chemotherapy regimens used, whilst cyclophosphamide was being administered in a number of patients (), there appeared to more limited use of capecitabine, cisplatin, docetaxel, doxorubicin, fluorouracil, imatinib, or oxaliplatin compared with other LMIC countriesCitation31,Citation39. Overall, chemotherapy is the key driver of treatment costs, reflected in other studiesCitation5,Citation17,Citation40. Even though laboratory and radiologic investigations are important in the diagnosis and management of various cancers, there are concerns that unnecessary use will increase healthcare costs and expose patients to unnecessary radiationCitation41. This is an area we will be researching further in the future, along with variations in the cost of radiologic and laboratory examinations between sectors to guide future policy. Other authors have also shown that government and teaching hospitals charged less than other hospitals for blood testsCitation42.
Overall, the cost of treatment of cancer patients is prohibitively high for most patients in Kenya. Kenya is a low -income country, where four out of 10 people live below the poverty line, according to the World Bank. Currently, the Kenyan healthcare system relies heavily on out of pocket payments for healthcareCitation14, although there are moves towards universal healthcareCitation4. For this reason, patients may not be able to afford expensive chemotherapy, surgical and radiotherapy procedures, and may default on their treatment, negatively impacting on their outcome. However, the Ministry of Health is currently under-funded, and cannot pay for the costs of all patients with cancer, although there are ongoing moves to improve the availability of facilities and personnelCitation4. The National Health Insurance Fund (NHIF) pays for some costs of patients, but only caters for inpatient hospital stay. Some hospitals, including Kenyatta National Hospital, have adopted a waiver system to cover the costs of care for extremely poor patients. This still has challenges, however, as the hospitals are not able to cover the costs of all patientsCitation43. In addition, there are problems applying the waiver system for cancer patients, since the costs of treating these patients can be very high. This calls for a revision in healthcare financing policies in Kenya to meet the WHO standards for equity in healthcareCitation14, as well as Sustainable Development Goal 3.4Citation4. This also calls for initiatives to obtain low prices for cancer medicines in Kenya, building on current access initiatives in other disease areasCitation44, as many patents for standard cancer medicines are now expired, with increasing availability of biosimilars, although there can be concerns with the quality of generics in LMICsCitation45.
We are aware that we only carried out this pilot study in one hospital (KNH). However, this is the national referral hospital, treating an appreciable number of patients with cancer in Kenya. We also only used patients’ notes for the analysis, with the limitations this imposes on content and accuracy. However, such methods are routinely used to collect costing data in the absence of electronic medical records. In addition, we are aware that there were only a limited number of patients with some cancers, making statistical analysis difficult to interpret, and we only included costs for 1 year. We also could not adequately calculate the sample size due to the absence of cancer prevalence studies. Despite these limitations, we believe our findings are robust and provide a basis for assessing the costs of cancer care in Kenya in the future, which we and others can build upon in future research, including much larger patient samples and durations for the different cancer types.
Conclusion
The cost of cancer treatment in Kenya varies by type of cancer, the modality, cost of medicines, and the type of inpatient admission. However, the cost of medicines and inpatient admissions are currently the greatest cost components in the treatment of patients with cancer in Kenya.
It is anticipated that this study will provide a platform to inform future initiatives from the government, as well as both private and public insurance companies in Kenya, to increase resource availability, and better allocate available resources, to more effectively treat patients with cancer in Kenya given the current high burden for patients. In addition, to provide a basis for future research efforts. Greater availability of generic anti-cancer medicines, as well as biosimilars, should help in the future as Kenya strives towards universal access.
Recommendations
The cost of cancer therapy is currently high in Kenya with respect to average salaries. Consequently, all parties involved should play their role in reducing the prevalence and burden to patients. This includes instigating programs to reduce behaviors that increase the risk of cancer. In view of this, we believe patients should be encouraged to go for regular check-ups to hasten early diagnosis and monitor progression, as well as be given advice and encouragement to alter their lifestyles to reduce their potential for developing cancer. Lifestyle changes include dietary modifications, exercise, and weight loss where pertinent.
We also believe, for those patients with insurance, insurance companies should allocate more resources to cancer therapy to ease the burden for their clients. The National Health Insurance Fund (NHIF), which is public insurance offered by the Kenyan government, should also increase its comprehensive cover for cancer patients in all settings, building on current initiatives. Furthermore, we believe hospitals and donor companies should increase their waiver for cancer patients who are struggling to fund their care to improve future care. Lastly, the Ministry of Health should explore potential access schemes for patients with cancer, building on initiatives in other disease areas. We will be monitoring this development.
Transparency
Declaration of funding
There was no external funding for this project.
Declaration of financial/other relationships
The authors declare they have no relevant conflicts of interest. There was also no writing assistance with this paper. JME peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
Acknowledgements
None reported.
Related Research Data
References
- Ferlay J, Soerjomataram I, Dikshit R. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer 2015;136(5):E359-8
- Stewart BW, Wild CP, editors. World Cancer Report 2014. IARC. WHO. Available from: http://www.searo.who.int/publications/bookstore/documents/9283204298/en/ [Accessed 14 January 2018]
- Torre LA, Bray F, Siegel RL, et al. Global cancer statistics, 2012. Cancer J Clin 2015;65:87-108
- Anderson T. Taking up Africa’s cancer challenge. Botswana, Kenya and Rwanda have started to provide cancer care in their national efforts to achieve universal coverage of health services. Bull WHO 2018;96:229-30
- Chalkidou K, Marquez P, Dhillon PK, et al. Evidence-informed frameworks for cost-effective cancer care and prevention in low, middle, and high-income countries. Lancet Oncol 2014;15:e119-31
- KNCO. Kenya Cancer Statistics & National Strategies. Kenyan Network of Cancer Organizations. Available from: https://kenyacancernetwork.wordpress.com/kenya-cancer-facts/ [Accessed 10 February 2018]
- Uyl-de Groot CA, dVE, Verweij J, Sullivan R. Dispelling the myths around cancer care delivery: It’s not all about costs. J Cancer Policy 2014;2:22-9
- Korir A, Gakunga R, Subramanian S, et al. Economic analysis of the Nairobi Cancer Registry: implications for expanding and enhancing cancer registration in Kenya. Cancer Epidemiol 2016;45(Suppl 1):S20-S9
- Korir A, Yu Wang E, Sasieni P, et al. Cancer risks in Nairobi (2000–2014) by ethnic group. Int J Cancer 2017;140:788-97
- Osman OM. Meet the Kenyans too poor to afford cancer treatment. Available from: http://www.aljazeera.com/indepth/features/2016/02/meet-kenyans-poor-afford-cancer-treatment-16020109563-0008.html [Accessed 10 February 2018]
- KNCO. Cancer facts. Kenyan Network of Cancer Organizations. Available from: https://kenyacancernetwork.wordpress.com/cancer-facts/ [Accessed 10 February 2018]
- Mbui JM, Oluka MN, Guantai EM, et al. Prescription patterns and adequacy of blood pressure control among adult hypertensive patients in Kenya; findings and implications. Expert Rev Clin Pharmacol 2017;10:1263-71
- Situma E. High cost of cancer treatment burdens patients. Business Daily. Available from: https://www.businessdailyafrica.com/High-cost-of-cancer-treatment-burdens-patients/-/539444/1683676/-/rxfm7xz/-/index.html [Accessed 10 January 2018]
- Chuma J, Okungu V. Viewing the Kenyan health system through an equity lens: implications for universal coverage. Int J Equity Health 2011;10:22
- Goldstein DA, Clark J, Tu Y, et al. A global comparison of the cost of patented cancer drugs in relation to global differences in wealth. Oncotarget 2017;8:71548-55
- Cameron A, Ewen M, Ross-Degnan D, et al. Medicine prices, availability, and affordability in 36 developing and middle-income countries: a secondary analysis. Lancet 2009;373:240-9
- Kelly RJ, Smith TJ. Delivering maximum clinical benefit at an affordable price: engaging stakeholders in cancer care. Lancet Oncol 2014;15:e112-18
- WHO. Access to new medicines in Europe: technical review of policy initiatives and opportunities for collaboration and research. WHO. Available from: http://www.euro.who.int/__data/assets/pdf_file/0008/306179/Access-new-medicines-TR-PIO-collaboration-research.pdf?ua =1 [Accessed 10 January 2018]
- Davis C, Naci H, Gurpinar E, et al. Availability of evidence of benefits on overall survival and quality of life of cancer drugs approved by European Medicines Agency: retrospective cohort study of drug approvals 2009–13. BMJ 2017;359:j4530
- Godman B, Wild C, Haycox A. Patent expiry and costs for anti-cancer medicines for clinical use. Generics Biosim Init J 2017;6:1-2
- Bach PB, Saltz LB. Raising the dose and raising the cost: the case of pembrolizumab in lung cancer. J Natl Cancer Inst 2017;109
- Lopes G, Vulto A, Wilking N, et al. Potential solutions for sustaining the costs of cancer drugs. Eur Oncol Haematol 2017;13:102-7
- Howard DH, Bach P, Berndt ER, Conti RM. Pricing in the market for anticancer drugs. J Econ Perspect 2015;29:139-62
- Barron A, Wilsdon T. Challenging perceptions about oncology product pricing in breast and colorectal cancer. Pharm Med 2016;30:321-6
- Hill A, Gotham D, Fortunak J, et al. Target prices for mass production of tyrosine kinase inhibitors for global cancer treatment. BMJ Open 2016;6:e009586
- Sterling L, van Lonkhuijzen L, Nyangena J, et al. Protocol development for ovarian cancer treatment in Kenya: a brief report. Int J Gynecol Cancer 2011;21:424-7
- Ubel PA, Abernethy AP, Zafar SY. Full disclosure—out-of-pocket costs as side effects. N Engl J Med 2013;369:1484-6
- KENCASA. Kenya Cancer Association fact sheet. Kenya Cancer Association. Available from: https://www.uicc.org/membership/kenya-cancer-association [Accessed 11 January 2018]
- Ministry of Health (Kenya). National guidelines for cancer management Kenya. Ministry of Health; 2013. Available from: http://kehpca.org/wp-content/uploads/National-Cancer-Treatment-Guidelines2.pdf [Accessed 20 February 2018]
- Mudenyo M, Mugo M, Muchiri L, et al. Trends of leading cancer cases at KNH cancer registry. KASH. Available from: https://wwwkemriorg/KASH/ojs-248-1/indexphp/KCAB/article/view/19 [Accessed 22 February 2018]
- Taghizadeh-Ghehi M, Amouei A, Mansouri A, et al. Prescribing pattern and prescription-writing quality of antineoplastic agents in the capital city of a middle-income developing country. J Res Pharm Prac 2018;7:46-50
- Korir A, Okerosi N, Ronoh V, et al. Incidence of cancer in Nairobi, Kenya (2004–2008). Int J Cancer 2015;137:2053-9
- de Martel C, Ferlay J, Franceschi S, et al. Global burden of cancers attributable to infections in 2008: a review and synthetic analysis. Lancet Oncol 2012;13:607-15
- Cois A, Day C. Obesity trends and risk factors in the South African adult population. BMC Obesity 2015;2:42
- Kaaks R, Lukanova A, Kurzer MS. Obesity, endogenous hormones, and endometrial cancer risk: a synthetic review. Cancer Epidemiol Biomarkers Prev 2002;11:1531-43
- Becker S, Kaaks R. Exogenous and endogenous hormones, mammographic density and breast cancer risk: can mammographic density be considered an intermediate marker of risk? Recent Results Cancer Res 2009;181:135-57
- Bernstein L, Ross RK. Endogenous hormones and breast cancer risk. Epidemiol Rev 1993;15:48-65
- Henderson BE, Feigelson HS. Hormonal carcinogenesis. Carcinogenesis 2000;21:427-33
- Jakupi A, Godman B, Martin A, et al. Utilization and expenditure of anti-cancer medicines in Kosovo: findings and implications. Pharmacoecon Open 2018
- Barron JJ, Quimbo R, Nikam PT, et al. Assessing the economic burden of breast cancer in a US managed care population. Breast Cancer Res Treat 2008;109:367-77
- Kendall D, Quill E. Reduce unnecessary radiological exams. Third Way. Available from: http://www.thirdway.org/report/reduce-unnecessary-radiological-exams [Accessed 20 February 2018]
- Hsia RY, Akosa Antwi Y, Nath JB. Variation in charges for 10 common blood tests in California hospitals: a cross-sectional analysis. BMJ Open 2014;4:e005482
- Kamanda MI. Determinants of factors affecting adherence to radiotherapy treatment among patients with cervical cancer at the MP Shah Hospital. Available from: file:///C:/Users/mail/Desktop/My%20documents/Ongoing%20papers/Kenya%20publications/Anti%20cancer%20medicines/Kamanda%20.pdf [Accessed 22 February 2018]
- Novartis. Kenya first country to launch ‘Novartis Access’, expanding affordable treatment options against chronic diseases. Novartis; 2015. Available from: https://www.novartis.com/news/media-releases/kenya-first-country-launch-novartis-access-expanding-affor-dable-treatment [Accessed 11 January 2018]
- Yang YT, Nagai S, Chen BK, et al. Generic oncology drugs: are they all safe? Lancet Oncol 2016;17:e493-e501
Appendix:Appendix 1: Data collection tool
Section 1: Patient demographics
Patient Serial Number______________ Age____ Sex_______
Date of Admission________________ Setting: □ Inpatient □ Outpatient
Date of Data Collection___________________
Patient area of Residence__________________
Diagnosis__________________________________________________
Section 2: Direct healthcare costs
(A) Cost of drugs (KES)
(B) Cost of surgical procedures
Done in KNH □ Yes □ No
If no state, where?___________________
(C) Cost of radiology procedures
Done in KNH □ Yes □ No
If no, state where___________________
(D) Cost of laboratory tests
Done in KNH □ Yes □ No
If no, state where___________________
(E) Cost of nursing and drug administration
(F) Consultation fee
(G) Inpatient admission costs
(H) Cost of medical devices