
Abstract
Purpose: To explore possible effects of tongue piercing on perceived speech quality.
Methods: Using a quasi-experimental design, we analyzed the effect of tongue piercing on speech in a perception experiment. Samples of spontaneous speech and read speech were recorded from 20 long-term pierced and 20 non-pierced individuals (10 males, 10 females each). The individuals having a tongue piercing were recorded with attached and removed piercing. The audio samples were blindly rated by 26 female and 20 male laypersons and by 5 female speech-language pathologists with regard to perceived speech quality along 5 dimensions: speech clarity, speech rate, prosody, rhythm and fluency.
Results: We found no statistically significant differences for any of the speech quality dimensions between the pierced and non-pierced individuals, neither for the read nor for the spontaneous speech. In addition, neither length nor position of piercing had a significant effect on speech quality. The removal of tongue piercings had no effects on speech performance either. Rating differences between laypersons and speech-language pathologists were not dependent on the presence of a tongue piercing.
Conclusions: People are able to perfectly adapt their articulation to long-term tongue piercings such that their speech quality is not perceptually affected.
Introduction
Body piercing, i.e. the application of body decoration and jewelry on different parts of the body by perforation and permanent penetration of skin, adipose tissue, or cartilage is much more than just a fashionable trend and shows a strong increase since the 1990s. Body piercing prevalence (not considering earlobes) was found to be as high as 8% in Australia (Citation1), 9% in Germany (Citation2), 10% in England (Citation3), and 14% in the USA (Citation4). The preferred body area for piercing depends on the person’s nationality, age and sex. While the British prefer the navel with 33% of the piercings (Citation3), Germans tend to wear piercings in the ear (44.8%, earlobes excluded) (Citation2). The highest numbers of pierced individuals were reported for young adults, showing a prevalence of 27% in the British and German population (Citation2,Citation3). While in general more women than men are pierced, navel piercings are found more often among women, whereas piercings of the eyebrows, nipples and genitals are more common for men (Citation2,Citation3). Compared to other types of piercings, oral piercings are a rather recent fashion (Citation3). The preferred intraoral piercing is a tongue piercing (Citation5). Besides "hoops" and "labrets", barbell-shaped devices are among the most widely used tongue piercings (Citation6). They consist of a bar with spherical ends, which is made of titanium, stainless steel, silver or gold. In most cases this barbell is inserted vertically through the midline of the tongue muscle, directly in front of the lingual frenum in the anterior third () or in the region from the anterior to the middle third of the tongue (Citation7).
Figure 1. Barbell-type tongue piercing close to the tongue tip.

Depending on form and position of the tongue piercings, different kinds of local and systemic complications have been reported. A common immediate consequence of the application of the piercing bar is bleeding and swelling, and in the absence of complications, the healing period lasts 4 to 6 weeks (Citation5). Complications that may arise from wearing a tongue piercing over longer periods of time include alveolar bone abnormalities, breaks, lesions, or chipping of the teeth, recession or trauma of the gingiva, and increased salivary flow (Citation5,Citation8–10). Although more severe complications are rare, they are potentially life-threatening. They range from lesions of the lingual artery with bleeding (Citation5,Citation11), to hematoma and suffocation (Citation12). Further complications may arise from different types of local infections such as molar abscess, glossitis, submandibular lymphadenitis and sialadenitis, Ludwig’s angina, or be systemic like hepatitis, HIV, cerebellar abscess, endocarditis and others (Citation11,Citation13).
Besides the problems mentioned above, the possible influence of tongue piercings on speech received only little attention. The position of the piercings at the most important articulatory organ raises the question to what extent they affect the speech quality of their carriers after healing of the puncture. So far, a few studies reported speech difficulties during the first days or weeks after piercing. For example, Farah and Harmon (1998) reported difficulties with the pronunciation of [s], [∫], [θ], [p], [f], [v], and [j] within the first week after piercing in a single-case study. Stead et al. (Citation14) undertook a survey of 123 individuals with tongue piercings, 24% of which complained about speech problems (that were not further defined) within the first 24 h following tongue piercing, 19% up to one week later, and 9% more than one week later. Altogether, 51% of the participants complained about speech problems in this study. To our knowledge, the only study dealing with the impact of long-term tongue piercing on speech was performed by Van Borsel and Cornelis (Citation15). In their study, three speech-language pathologists perceptually scored the speech quality of eight participants with a barbell-type piercing. The speech material consisted of a text that was read by each subject both with the piercing in place and with the piercing removed. The scores assigned by the raters did not significantly differ for these two conditions.
In the present study, we performed a more rigorous examination of possible effects of tongue piercings on speech quality. We compared the speech quality of 20 long-term pierced subjects (both with the piercings in place versus removed) with 20 non-pierced subjects for both read and spontaneous speech in a perception experiment. The read speech items consisted of a reading text and additionally selected word sequences to detect possible differences in speech quality for different places of articulation. Instead of using a single rating scale, speech quality was judged in terms of five quality dimensions, namely, speech clarity, speech rate, prosody, rhythm and fluency. Finally, we had two groups of raters: one group of 46 laypersons and one group of 5 speech language pathologists (SLPs).
Our research questions were as follows:
Are there perceptible differences in the speech quality of pierced speakers, unpierced speakers, and speakers who have removed their piercings, in any of the five quality dimensions?
Do the possible rating differences depend on the kind of stimulus material (coherent sentences versus single words versus spontaneous speech)?
Is there a correlation between the position or the length of the piercing barbell and the perceptual ratings?
Is the perceptual rating influenced by the participants’ or raters’ sex?
Do the perceptual ratings differ between laypersons and SLPs?
Material and methods
Preparation of the audio samples
To obtain the speech samples, we recruited 40 volunteers: ten women (mean age: 24;0 years, range: 19;7–26;8 years) and ten men (mean age: 25;4 years, range: 19;3–32;0 years), who were not pierced, and ten women (mean age: 25;10 years, range: 21;6–29;8 years) and ten men (mean age: 28;6 years, range: 21;4–43;0 years), who were pierced with a barbell-type tongue piercing. All the participants were native speakers of German with no reported complaints of their orofacial organs (inflammations, lesions, hypersalivation, etc.) at the time of the study. Professional speakers, non-native speakers of German, and persons with recorded hearing impairments, speech or voice disorders were not included. Twenty-four of the 40 volunteers were employees, 3 trainees, 11 students, and 2 pupils. Their professions belonged to the fields of technology (n = 11), medicine (n = 9), pedagogics (n = 8), economy (n = 5), and others (n = 7). All pierced individuals had been wearing their tongue piercings for at least two and a half years. On average, male subjects were pierced 6.9 years ago (range: 2.5–10.0) and females 5.9 years ago (range: 2.5–9.5). All tongue piercings were barbells attached along the midline of the tongue, as shown in . The mean position of the piercing (distance of tongue tip to barbell) was 13 mm (range: 6–22 mm) for men and 15.5 mm (range: 8–25 mm) for women, and the mean length of the piercing barbell was 23 mm (range: 19–27 mm) for men and 22 mm (range: 19–28 mm) for women.
For the recordings and the subsequent analyses, we defined 3 groups of speakers: Group 1 were the non-pierced subjects, group 2 were the pierced subjects (with piercings in place), and group 3 were the same pierced subjects with temporarily removed piercings. For each group, three types of samples were recorded. For sample 1, the participants read the German standard text "The north wind and the sun" (German: “Der Nordwind und die Sonne”). The phoneme distribution in this text is roughly representative for the German language. For sample 2, six two-word and eight three-word sequences were recorded, which contained different consonants or consonant combinations as initial, medial, and final sounds. These word sequences included labiodental and alveolar as well as palatoalveolar phonemes to test the different places of articulation. The word sequences and the phonetic sound or structure they represented are listed in . For sample 3, all the participants had to answer two open questions: (1) Where did you stay for your last holiday and when was it? (German: Wo und wann waren Sie zuletzt in Urlaub?). (2) What did you like best? (German: Was hat Ihnen besonders gut gefallen?). The duration of their spontaneous answers was 2–20 s (mean: 6.34 ± 4.26 s). The length of utterances differed mainly interindividually. The shortest responses were two-word expressions while most of the answers included one or more sentences. In all cases, the time interval was sufficient to perform the demanded rating. In conclusion, the three samples contained a read text, specific words for individual phonemes and spontaneous speech.
Table 1. Test word sequences for speech quality ratings categorized for their places of articulation and consonants tested.
The recordings were made with a studio large diaphragm condenser microphone (Fame SKE C010) and a USB audio interface (TASCAM) at a sampling rate of 44 kHz with 24 bit quantization. The volume of the audio files was normalized by performing a sound level adjustment with WavGain V 1.0.3. To reduce the data for the subsequent perception experiment to a practical amount, not all recordings were used. From the read text, only one sentence was selected. In addition, only the word sequences of the speaker groups 1 and 2 were selected. Of the spontaneous speech, all audio samples were used.
Procedure of the perception study
For the perception study, 51 raters were recruited, consisting of 20 male and 26 female laypersons as well as five female SLPs experienced in speech diagnostics and therapy. The mean age of the raters was 36;10 years (range: 23;7–49;3 years) for the male laypersons, 35;4 years (range: 18;2–49;2 years) for the female laypersons, and 30;4 years (range 24;3–48;10 years) for the female SLPs. Raters older than 50 years or persons with hearing impairment, speech or voice disorders were not included. The raters were not informed about the purpose of the study or the fact that some of the audio samples were recorded from pierced individuals.
The task of the raters was to perceptually judge the speech quality of the samples with respect to five selected quality dimensions, namely, speech clarity, speech rate, prosody, rhythm and fluency. For each dimension, the quality had to be marked on a five-point scale as either "very good (1)", "good (2)", "neither good nor bad (3)", "bad (4)", or "very bad (5)". These quality dimensions were chosen because they are important for speech intelligibility. In addition, the parameter setting should mask the purpose of the study and guarantee blind rating. The samples were presented to the raters in groups of 3–10 over studio loudspeakers (JBL Control 1 Pro) in a quiet room. To each group, the samples were played in one of two pseudo-randomized orders.
To reduce the number of evaluations to a practicable amount, not all of the five quality dimensions were considered equally for rating each of the three sample types. The read phrase was evaluated by all raters considering the parameters speech clarity, prosody, and speech fluency. The 14 word sequences were evaluated by all raters just considering the parameter speech clarity. The open-set answers were judged considering all five parameters, but only by the SLPs. In total, the laypersons rated 620 audiofiles each in a rating time of about 1.25 h, the experts rated 740 files.
Statistical procedures
The influence of the speaker group (non-pierced speakers versus pierced speakers versus speakers with removed piercing) on the speech quality ratings was evaluated using a repeated measures analysis of variance (ANOVA) because the same raters evaluated all stimuli. For the read sentence, the ANOVAs were performed separately for the dimensions clarity, prosody and fluency. For the word sequences, only speech clarity was measured, and for the spontaneous speech samples, the ratings of all five speech quality characteristics were pooled. In order to assess the interrater reliability of rating data, the following coefficients were calculated: ICC (both for absolute identity of ratings and for consistency only), Cronbach’s alpha, Krippendorff’s alpha (for further details cf. (Citation16), pp. 142–164). The absolute level of interrater agreement as assessed with the Krippendorff alpha coefficient with weights for ordinal ratings was only moderate for the different rating tasks although significantly above chance level (cf. Supplementary Tables S1–S3). Since the analyses looking for a potential influence of rater gender, gender of the voice samples to be rated, and the presence of a tongue piercing were all based on the average ratings computed for the whole groups of raters, biases influencing the relation of mean rating levels for these factor level combinations are not to be expected. Additional intrarater reliability has not been estimated since otherwise the auditory sample load of the participants would have overrun their limits of attention.
Results
As shown in , no overall significant difference could be found between pierced speakers, non-pierced speakers, and speakers who removed their piercing.
Table 2. Influence of the speaker group, i.e. pierced subjects versus non-pierced subjects versus subjects that removed their piercing on the speech quality ratings for the different sample types based on a repeated measures one-factorial ANOVA.
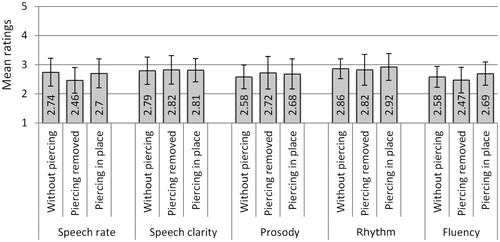
illustrate the ratings separately for the three sample types, namely the sentences read, the word lists with the focus on different places of articulation, and the spontaneous speech samples. In general, there were only very minor differences between the mean ratings for the speaker groups for all three sample types. For the word sequences (), there are six sequences (for the target consonants [d], [s], [z], [l], [n], [ks]), for which the mean rating for the pierced group is more than 0.1 scale points above the rating for the non-pierced group. This indicates a tendency that for these consonants (all of them involve the alveolar place of articulation), speech quality is slightly worse for the pierced speakers. However, this trend was not significant. With regard to the spontaneous speech samples (), which were rated by the SLPs only, there is a tendency for slightly better (i.e. lower) ratings for the speakers with the removed piercing with respect to speech rate and fluency.
Figure 2. Speech quality ratings for the sentence from the reading text separately for each speech quality dimension, speaker group (non-pierced speakers versus pierced speakers with removed piercings versus pierced speakers with piercings in place), and rater group (naïve male raters versus naïve female raters versus SLPs). The black lines indicate ±1 SD ranges.
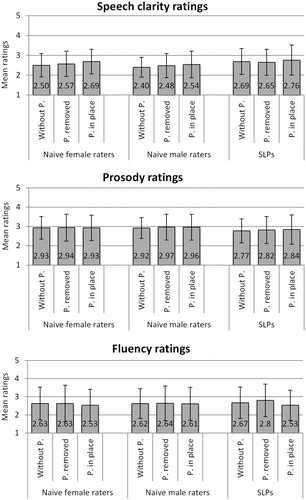
Figure 3. Differences in speech clarity ratings for the word sequences with the different target consonants and consonant combinations between the groups of non-pierced subjects and subjects with piercing in place. The black lines indicate +1 SD ranges.
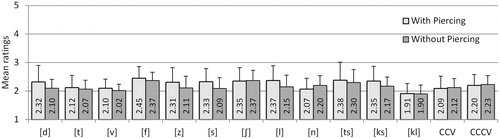
Figure 4. Speech quality ratings of the SLPs for the spontaneous speech samples, separated by speaker group and speech quality characteristic. The black lines indicate ±1 SD ranges.
In addition, we analyzed the relation between the position and size of the piercing and speech quality. The piercing position was determined as the distance from the tongue tip measured at the protruded tongue and varied between 6 and 25 mm. The size was determined as the length of the piercing stick and varied between 19 and 28 mm. This analysis was conducted only for the pierced speaker group using the ratings for the read sentences pooled across raters and quality dimensions. For the relation between piercing position and quality rating, the Pearson correlation coefficient was very low (r = 0.120) and not significantly different from zero (p = .307). For piercing length, the correlation coefficient was low as well (r = 0.269) and not significant (p = .126).
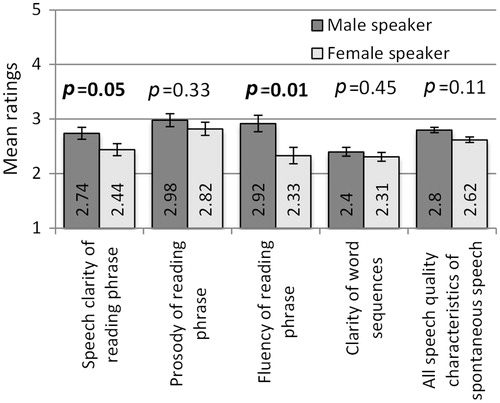
Furthermore, we analyzed the influence of the speakers’ sex on the ratings. As shown in , there was a moderate influence of the speakers' sex on the perceptual ratings of the speech clarity and fluency in the reading phrase setting. On average, the speech quality of women was judged to be higher than the speech quality of men, independently from the piercing state (pierced versus non-pierced).
Figure 5. Influence of the speakers’ sex on the speech quality ratings for the different sample types. The black lines indicate the ranges of ±1 standard error.
Finally, we analyzed the effect of the rater group on the speech quality ratings based on the read sentences and the word sequences (only these sample types were rated by all three rater groups) pooled across all three speaker groups.
As shown in , there were some significant differences between the average ratings of male laypersons, female laypersons, and SLPs, but the trends were not consistent for the different quality dimensions. In detail, the ratings of the female laypersons, as well as those of the female SLPs, in respect of speech clarity of reading phrase and clarity of word sequences were highly significantly worse than those of the male laypersons. In respect of the prosody of reading phrase, the male ratings were slightly significantly worse than those of the SLPs.
Figure 6. Influence of the rater group on the speech quality ratings for the different sample types. The black lines indicate the ranges of ±1 standard error.

Discussion and conclusions
The present study investigated the effect of a tongue piercing on speech quality. Therefore, both laymen and SLPs rated the quality of a read sentence, read word sequences, and spontaneous speech spoken by long-term tongue-pierced and non-pierced male and female adults. Speech quality was assessed with respect to the five dimensions speech clarity, speech rate, prosody, rhythm, and fluency. Although the estimation of the interrater reliability (see Supplemental data) showed a slightly higher reliability for the expert group compared to the laypersons, to our surprise, neither the SLPs nor the laypersons were able to distinguish the groups of pierced and non-pierced speakers for either type of speech (read speech versus spontaneous speech). Even the perception of the word sequences with alveolar consonants, which we expected to be most likely disturbed due to the piercing positions, did not significantly differ between the pierced and non-pierced groups (apart from a non-significant numerical trend). Furthermore, speech quality of the pierced speakers did not significantly improve, when they removed their piercing. The position or length of the piercing did not influence intelligibility either. However, the gender differences in respect of speech clarity and fluency of reading phrases between the male and female speakers of the study were not unexpected. There are a number of studies reporting similar findings, explained by gender differences in vowel production, voice onset time, and articulatory speed on one hand and sociophonetic priming on the other hand (for overview see (Citation17)).
In respect of piercing, our data suggested that long-term tongue piercings do not affect speech quality. This was true for the investigation of the reading text, the word sequences and the spontaneous answers to the standardized questions. However, a bias due to varying utterance length cannot be completely ruled out. On the other hand, the results of this sample were congruent with those of the reading text and word sequences. In total, our data confirm the findings of the few previous studies, in which speech quality was assessed with much smaller groups of participants wearing tongue piercings than in the present study (Citation10,Citation15). Hence, tongue-pierced people are apparently able to compensate the effect of the tongue piercing to the limits of perceptual differentiation. This ability of speech adaptation has been shown for several other types of "perturbations". For example, speakers can immediately compensate for a bite block between the teeth that fixes the mandible position with respect to the palate, such that the quality of spoken vowels is not affected (Citation18). Other kinds of perturbations that were extensively studied are artificial palates, which change the speakers’ shape of the hard palate (Citation19). Also here, speakers compensate for their altered palate shape very soon. For both bite block and artificial palate perturbations, the compensation for consonants, in particular, fricatives, usually takes longer than for vowels (Citation19,Citation20). Similar to the compensation for a tongue piercing, near-perfect compensation with regard to speech quality was even shown for the more severe cosmetic "tongue split", where the anterior tongue blade is split along the midline of the tongue. Bressman (Citation21) presented a case study where the speech of a subject with a split tongue was rated to be highly intelligible and acceptable, apart from slight distortions of the sibilants/s/and/z/. The limit of oral modifications that can still be compensated with regard to speech production is, however, difficult to define. For example, after oral or oropharyngeal resections, e.g. after surgically treated oral cancer, the speech function can often not be fully restored (Citation22). With regard to the present study, all the participants carried their piercing for at least 2.5 years. While we could not prove any negative influence of the piercing on speech quality after this rather long time, there are multiple indications for speech problems during the first weeks after piercing (Citation10,Citation14). However, conclusive statements about the severity and duration of these problems would ideally require a longitudinal study with a bigger group of subjects for weeks or months after piercing.
Finally, although long-term tongue piercings do not affect speech quality, one should be aware of the other oral risks associated with these piercings like, for example, alveolar bone abnormalities, chipping of the teeth and gingival recession.
Supplementary Material
Download PDF (64.3 KB)Acknowledgements
Special thanks to all the speaker and rater participants of the study.
Disclosure statement
The study was approved by the Ethics Committee of the University Hospital Aachen, Germany. The authors respected the rules of the Declaration of Helsinki and obtained written informed consent from all participants. The authors report no declarations of interest.
Related Research Data
References
- Makkai T, McAllister I. Prevalence of tattooing and body piercing in the Australian community. Commun Dis Intell Q Rep 2001;25:67–72.
- Gutsche P, Schmalz G, Landthaler M. Prevalence of piercing in a German population. Eur J Dermatol 2008;18:26–8.
- Bone A, Ncube F, Nichols T, Noah ND. Body piercing in England: a survey of piercing at sites other than earlobe. BMJ 2008;336:1426–8.
- Laumann AE, Derick AJ. Tattoos and body piercings in the United States: a national data set. J Am Acad Dermatol 2006;55:413–21.
- Levin L, Zadik Y, Becker T. Oral and dental complications of intra-oral piercing. Dent Traumatol 2005;21:341–3.
- Ziebolz D, Hornecker E, Mausberg RF. Microbiological findings at tongue piercing sites: implications to oral health. Int J Dent Hyg 2009;7:256–62.
- Campbell A, Moore A, Williams E, et al. Tongue piercing: impact of time and barbell stem length on lingual gingival recession and tooth chipping. J Periodontol 2002;73:289–97.
- Dougherty SL, Tervort-Bingham K. Assessment of the alveolar bone surrounding the mandibular anterior teeth of individuals wearing a tongue stud. J Dent Hyg 2005;79:8.
- De Moor RJG, De Witte AMJC, De Bruyne MAA. Tongue piercing and associated oral and dental complications. Endod Dent Traumatol 2000;16:232–7.
- Farah CS, Harmon DM. Tongue piercing: case report and review of current practice. Aust Dent J 1998;43:387–9.
- Stirn A. Body piercing: medical consequences and psychological motivations. Lancet 2003;361:1205–15.
- Keogh IJ, O’Leary G. Serious complication of tongue piercing. J Laryngol Otol 2001;115:233–4.
- Yu CH, Minnema BJ, Gold WL. Bacterial infections complicating tongue piercing. Can J Infect Dis Med Microbiol 2010;21:e70–4.
- Stead LR, Williams JV, Williams AC, Robinson CM. An investigation into the practice of tongue piercing in the South West of England. Br Dent J 2006;200:103–7.
- Van Borsel J, Cornelis C. Tongue piercing and speech. J Otolaryngol Head Neck Surg 2009;38:11–15.
- Heinen E. [Auswirkungen eines Zungenpiercings auf den Sprechvorgang] [thesis]. Aachen, Germany: Medical Faculty of the RWTH Aachen University; Dec 2013, 1–166p. [in German].
- Simpson AP. Phonetic differences between male and female speech. Lang Ling Compass 2009;3:621–40.
- Fowler CA, Turvey MT. Immediate compensation in bite-block speech. Phonetica 1980;37:306–26.
- Brunner J, Perturbed speech. In: How compensation mechanisms can inform us about phonemic targets. Saarbrücken: Südwestdeutscher Verlag für Hochschulschriften; 2009.
- McFarland DH, Baum SR. Incomplete compensation to articulatory perturbation. J Acoust Soc Am 1995;97:1865–73.
- Bressmann T. Speech adaptation to a self-inflicted cosmetic tongue split: perceptual and ultrasonographic analysis. Clin Linguist Phon 2006;20:205–10.
- Pauloski BR, Logemann JA, Rademaker AW, et al. Speech and swallowing function after oral and oropharyngeal resections: one-year follow-up. Head Neck 1994;16:313–22.