
ABSTRACT
Health is central to sustainable development, and thus a cross-cutting issue of the Sustainable Development Goal (SDG) 2030 agenda. Natural resource extraction projects in Africa have considerable potential to impact on health-related targets of the SDGs. This paper introduces the rationale and organization of the HIA4SD Project; a 6-year research for development (r4d) project that aims to inform and facilitate a policy dialogue at the national and international level on whether current regulatory approaches to impact assessment in Africa promote sustainable development, placing emphasis on SDG3 Good Health and Well-being. The HIA4SD Project has a focus on large-scale natural resource extraction projects and is implemented in four African countries, namely Burkina Faso, Ghana, Mozambique and Tanzania.
Background
Health is central to the three dimensions of sustainable development: environment, society and economy (United Nations Citation2014). This is embodied in the 17 Sustainable Development Goals (SDGs) of the 2030 agenda, where health features as a crosscutting issue (Lu et al. Citation2015; Dietler et al. Citation2019). The extraction of natural resource in Africa (e.g. minerals, metals, oil and gas project) has the potential to positively act on the SDG 2030 agenda linked to health, and thus to actively contribute to sustainable development, as conceptualised in (Listorti Citation1996; IFC Citation2018). Firstly, upgraded public infrastructures, such as health facilities and schools (SDG11), foster good health and well-being (SDG3), better education (SDG4), and improved access to clean water and sanitation (SDG6) (Carter and Danert Citation2003; Knoblauch et al. Citation2014a). Secondly, the creation of employment and income can reduce poverty (SDG1) and malnutrition rates (SDG2) on one hand, and improve health insurance coverage (SDG3) on the other hand (Bradley et al. Citation2013; Langston et al. Citation2015; Knoblauch et al. Citation2017a). Thirdly, public–private partnerships can synergise efforts for disease control and elimination programmes (SDG3) (Asante et al. Citation2011; Drewry et al. Citation2017; Knoblauch et al. Citation2017b; Saric et al. Citation2019). Finally, tax revenues and royalties from private sector companies are essential for national and local governments to work towards all SDGs (Otto et al. Citation2006).
Figure 1. Health-related SDGs that have a direct link to natural resource extraction projects.

The various potential positive effects of natural resource extraction projects are opposed by potential risks to public health due to their operations. Project-induced in-migration puts strains on local health systems (SDG3, SDG10 and SDG11), water and sanitation infrastructure (SDG6) and food security (SDG2) (Westwood and Orenstein Citation2016; Knoblauch et al. Citation2018). Environmental degradation, in combination with changing ecosystems, might alter patterns of vector-related diseases (Knoblauch et al. Citation2014b; Diakite et al. Citation2017) and exposure to hazardous emissions (SDG3) (Krieger et al. Citation2012; Ncube et al. Citation2012). Changing behaviours in project settings can result in increased levels of commercial sex work, substance abuse and negative effects on mental health (all SDG3) (Hossain et al. Citation2013; Shandro et al. Citation2017). Insufficient stakeholder involvement and adverse project-related impacts have the potential to result in local conflict and injustice (SDG16) (Le Billon Citation2003; Ruggie Citation2007). Additionally, extractive projects raised issues related to equality (SDG10) and gender equity (SDG5) (O’Faircheallaigh Citation2015; Leuenberger et al. Citation2019).
Impact assessment
An impact assessment approach lends itself to minimise negative consequences on the environment, society and public health of any large resource extraction project, while promoting sustainable development (Quigley et al. Citation2006). Countries worldwide have established the legal requirement that an environmental impact assessment (EIA) must be done prior to the implementation of a large development project. Indeed, according to Richard (Citation2012), 191 out of 193 United Nations (UN) member countries have some form of either national legislation or have signed some form of international legal instrument that refers to the use of EIA. EIA as policy tools also empowers the government to prosecute environmental offences in the law courts. However, experience with EIA has shown that government institutions in both industrialised and developing countries often lack the capacity to evaluate the quality of the assessments and are facing challenges in monitoring and enforcement (Morrison-Saunders et al. Citation2012; Zvijakova et al. Citation2014; Chanchitpricha and Bond Citation2018; Hacon et al. Citation2018).
International governance arrangements such as social accountability mechanisms and investor guidelines, as for example the World Bank Group’s safeguard policies, play an important role in strengthening compliance with sustainability frameworks (Kosack and Fung Citation2014; Fox Citation2015; World Bank Citation2019). However, the share of World Bank-funded major projects declined in the 1990s and – at present – is quite small in resource extraction projects. To compensate for its shrinking influence, the International Finance Corporation (IFC), as the private sector arm of the World Bank Group, has engaged with the private sector, which eventually led to the launch of the Equator Principles (EP) in 2003. Those principles are based on the social and environmental performance standards developed by IFC, and the environment, health and safety guidelines of the World Bank (Richard Citation2012). Currently, 101 financial institutions in 38 countries have officially adopted the EP (Equator Principles Citation2019).
Health in impact assessment
In contrast to EIA, only few countries have established a legal requirement for other forms of impact assessment such as social impact assessment (SIA), strategic environmental assessment (SEA), health impact assessment (HIA) and human rights impact assessment (HRIA), which have – at least partially – arisen through discontent with EIA practice (Harris-Roxas et al. Citation2012; Salcito et al. Citation2015; Pereira et al. Citation2017). This holds particularly true for Africa, where not a single country is actively promoting HIA through a policy, regulation or another means of endorsement (Winkler et al. Citation2013), although health in the context of natural resource extraction projects is a highly dynamic topic. On the one hand, the development of natural resource extraction projects poses a risk to public health if potential adverse impacts on health determinants and outcomes are not appropriately mitigated (Brisbois et al. Citation2019; Thondoo et al. Citation2019). On the other hand, (re-) emerging infectious diseases pose challenges to the extractive sector, illustrating the need for effective governance of health in the context of resource extraction (Viliani et al. Citation2017). Both situations call for prospective impact assessments that systematically judge the potential, and sometimes unintended, effects of natural resource extraction projects on the health of affected communities for identifying appropriate actions to manage those effects (Quigley et al. Citation2006). For strengthening the inclusion of health in impact assessment, different regulatory and legal approaches are at hand (Harris-Roxas et al. Citation2012). For example, a number of Asian countries (e.g. Lao People’s Democratic Republic, Thailand and Vietnam) have developed specific policies that specifically require HIA (ADB Citation2018). In the European region, strategies for strengthening the consideration of health in SEA and EIA have been explored (Fischer et al. Citation2010, Citation2012; Cave et al. Citation2018).
Currently, impact assessments of natural resource extraction projects in Africa are generally driven by the environmental sector, while the health and other sectors are insufficiently involved (Silveira and Neto Citation2014; Harris et al. Citation2015). Although human health is generally considered as a key issue in environmental legislations, there is usually little methodological guidance provided on how to actually address health in impact assessment. Moreover, with regards to health, the legal text on EIA generally has a strong focus on environmental determinants of health, while paying little attention to social determinants of health and health systems. Hence, in order to tap the full potential of impact assessment as a policy tool for coupling natural resource extraction projects with sustainable development, there is a need to work towards integrated impact assessments that are grounded in intersectoral collaboration and backed by policies and methodological guidelines that embraces the SDG 2030 agenda (Glasbergen Citation2011; Buse and Hawkes Citation2015).
The HIA4SD project
The overarching objective of the HIA4SD Project (full title: ‘Health impact assessment for engaging natural resource extraction projects in sustainable development in producer regions’) is to conduct research that informs and facilitates a policy dialogue, and ultimately policy change, for strengthening the application of impact assessment as a regulatory mechanism in Africa. The HIA4SD Project, which is co-funded by the Swiss Agency for Development and Cooperation (SDC) and the Swiss National Science Foundation (SNSF) under the r4d programme (www.r4d.ch), has a focus on large-scale natural resource extraction projects, while taking into account informal natural resource extraction activities such as artisanal and small-scale mining (ASM).
The HIA4SD project has a duration of 6 years and follows two main project phases. The research phase (Phase I, September 2017 – August 2020), aims at generating a sound evidence-base at the national and local level on strengths and limitations of current impact assessment practice in engaging natural resource extraction projects (e.g. minerals, metals, oil and gas) to work towards health-related targets of the SDGs in Africa. Guiding research questions of the HIA4SD Project are:
What is the current institutional setup for regulating and implementing the public health dimension in impact assessment of natural resource extraction projects (NREPs)?
What effects of natural resource extraction projects on health-related targets of the SDGs can be observed at the national and local level?
How do natural resource extraction projects interact with, and have an effect on, local health systems?
What policy options can be proposed for more actively engaging natural resource extraction projects in the SDG 2030 agenda?
In the communication and application phase of the project (Phase II, September 2020 – August 2022), the research results will inform a policy dialogue in each of the four project countries (see below) with the aim to identify how the current governance architecture can be amended to make full use of impact assessments as a regulatory mechanism to support producer regions in working towards the SDG 2030 agenda.
Study countries
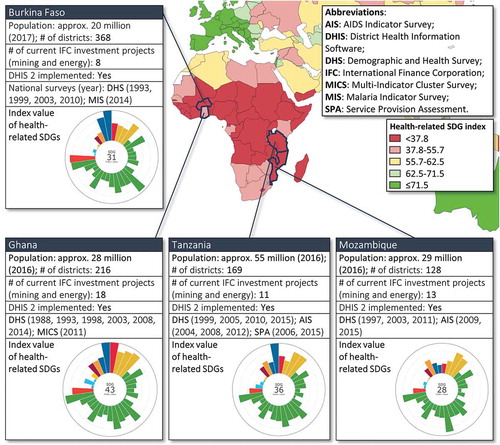
The HIA4SD Project is carried out in four African countries, namely Burkina Faso, Ghana, Mozambique and Tanzania. For the country selection the following criteria applied:
history of resource extraction (the number of current IFC investment project has been used as a proxy indicator);
implementation of the open source software platform ‘District Health Information Software 2ʹ (DHIS2; www.dhis2.org) to collect, manage and visualise routine health information system data;
availability of data from national Demographic and Health Surveys (DHS) and other national-level datasets; and
low health-related SDG index values (see ; index values represent all 33 health-related SDG indicators, ranging on a scale from 0 (worst observed value between 1990 and 2015) to 100 (best observed)) (Lim et al. Citation2016).
Figure 2. Summary statistic of the project country selection process (Sources for map and SDG index: Lim et al. (Citation2016) and IHME (Citation2019), respectively).
Organisation of the project
As illustrated in , the project activities are structured into three work streams (i.e. governance, impact research and capacity building), comprising 10 specific work packages (WPs). Here only a short description of each WP is provided. A detailed description of the quantitative and qualitative methods that are applied in the main research WPs (WP2, WP3 and WP4) of this inter- and trans-disciplinary project is available elsewhere (Farnham et al. Citation2020). The findings of the research WPs will inform and facilitate a policy dialogue at the national and international level on whether current regulatory approaches to impact assessment in Africa promote sustainable development, placing emphasis on SDG3 Good Health and Well-being. The empirical evidence produced under the HIA4SD Project will be published in a series of papers in the peer-reviewed literature. Key contributions of the project at the level of policy and practice include, but are not limited to, specific policy options, a policy dialogue, HIA teaching modules and excellence in HIA in the project countries.
Figure 3. Work streams of the project and specific work packages (WPs) in the respective project phases.
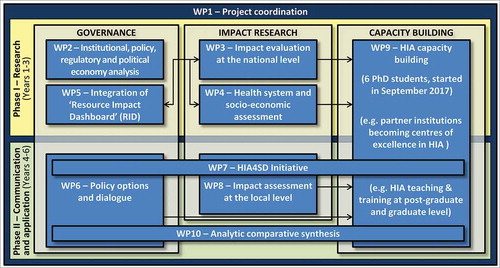
WP1 – project coordination
Continuous and efficient project coordination is essential for the successful implementation of the HIA4SD Project and facilitating broad stakeholder involvement. In two parallel and interlinked processes, coordination of the HIA4SD Project takes place at the international level (i.e. between project partner institutions) and at the level of the project countries (i.e. coordinating stakeholder involvement and research activities in each study country).
WP2 – institutional, policy, regulatory and political economy analysis
In order to map how different countries manage the institutional, economic, regulatory and political framework for implementing their EIA policies and to explain variation in their effectiveness, a combination of public policy analysis methods is applied including, but not limited to, institutional, network and political economy analysis. At the international level, regime theory is used as an additional method to inform the institutional and performance analysis of the private soft-law governance architecture, including but not limited to IFC, EP and private sector standards and industry guidelines in place.
WP3 – impact evaluation at the national level
While there is a growing body of case studies showing that natural resource extraction projects can result in a broad set of potential negative effects on public health in affected communities, there is little evidence describing overarching effects of natural resource extraction projects at the regional and national level. Under WP3, existing population-level databases are accessed to quantify and compare health indicators over time using, for example, time series analysis, matched geographical analyses in quasi-Poisson regression models and binominal regression models. The various impact evaluations place particular emphasis on using existing data sources, notably DHIS2, in order to assess the potential to integrate the project findings and methodologies into national policies with minimal resourcing.
WP4 – health systems and socioeconomic assessment
Since EIA is primarily driven by the environmental sector, the inclusion of the health sector in impact assessment is often arbitrary and opportunistic (Harris et al. Citation2015). By means of a systematic analysis of how natural resource extraction projects interact with the local health sector and local communities, WP4 aims to outline options how the involvement of the health sector in impact assessment can be shifted from being opportunistic to being strategic and sustainable. Qualitative research methods involving focus group discussions and key informant interviews are at the core of this WP. The socioeconomic assessment also comprises quantitative methods, such as cost-of-illness analysis.
WP5 – integration of ‘Resource Impact Dashboard’ (RID)
The logic of impact assessments is based on an ex-ante evaluation of negative externalities of a project in order to improve project design and to take corrective measures. Yet, research shows that the ‘Impact Statements’ not always anticipate actual impacts observed during operation (Kuipers and Maest Citation2006). The ‘Resource Impact Dashboard’ RID is an online platform that aims to foster evidence-based policy-making (http://www.resource-impact.org/). Under WP5 the health-specific indicators of the RID are refined based on findings of the HIA4SD Project. Moreover, the HIA4SD Project serves as a communication platform to disseminate the use of the RID.
WP6 – policy options and dialogue
WP6 is the continuation of WP2: while WP2 focuses on policy analysis and provides the information required to identify policy options, WP6 engages with policy makers, epistemic communities, operators and civil society actors at the national and international level in order to test and review policy proposals.
WP7 – HIA4SD initiative
Communication and dissemination of key findings is a central component of the second phase of the project. In order to share the research findings of the first phase with various project stakeholders, a website is launched under the label ‘HIA4SD Initiative’. At a later stage, the website is actively disseminated with the objective to encourage other institutions in Africa, Latin America and Asia to follow the example of our HIA4SD Project.
WP8 – impact assessment at the local level
Under WP8 two to three HIA case studies of natural resource extraction projects are developed in each partner country. The outputs of WP8 are important inputs to WP6 (Policy options and dialogue) and WP9 (HIA capacity building): (i) the HIA case studies support the policy dialogue process as they show concrete examples in the respective country; (ii) WP8 allows to train local collaborators in a standardised HIA approach; and (iii) the country-specific case studies can be readily built into the development of country-specific HIA teaching materials (see WP9).
WP9 – HIA capacity building
Capacity building is a continuous activity of the HIA4SD Project. In the first phase, project-internal capacity in HIA research and practice is built (six PhD students (one from each project country in Africa and one from Switzerland)). In the second phase, capacity in the use, oversight and regulation of HIA is developed at the national and regional level by capitalising on the internal capacity built in the first phase. Specifically, HIA teaching will be integrated into the curriculum of Public Health and Epidemiology MSc programmes of universities in the project countries. Furthermore, post-graduate training courses, on job-trainings and workshops targeting professionals from authorities and agencies involved or interested in impact assessment will be carried out in close collaboration between the southern and northern research partner institutions of the HIA4SD Project.
WP10 – analytic comparative synthesis
To maximise capitalisation of country-specific research and learning from generated evidence, an analytic, comparative synthesis is launched and undertaken under WP10. The activity within WP10 is fundamental for expanding the impact of the HIA4SD Project from the national level to the regional and global level through sharing and comparing of scientific and strategic findings across systems and cultures.
Conclusions and outlook
The HIA4SD Project aims at being part of the solution to the global problem of unsustainable extraction of natural resources, which includes adverse impacts on public health, ecosystems and the society in producer regions. The impact of the project, and its relevance for development and poverty alleviation in the study countries, will be achieved through a diversity of interlinked activities and outcomes as illustrated in . Cleary, the engagement of local stakeholders is crucial for the success of the project. This is addressed through early engagement of the central government, policy makers, Ministries of Health/Environment/Mining (or equivalents), resource extraction projects, academic/research institutions, impact assessors, the society as a whole and the affected communities in particular in all project countries. Transparent and offensive communication throughout project implementation will increase awareness of the role HIA can play to more actively engage natural resource extraction projects in positively acting on the wider determinants of health for promoting health and wellbeing in producer regions.
Figure 4. Pathway to impact at the national level (dotted lines meaning uncertain).
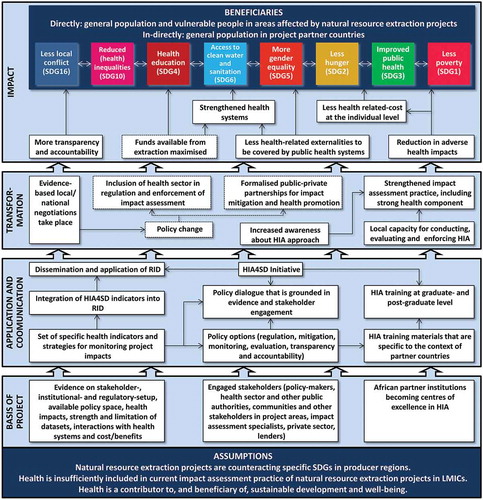
For the governmental stakeholders, the project generates evidence that justifies why health in impact assessment needs to be strengthened and, thus, enables them to pull natural resource extraction projects in responsibility of sustainable development by acting on health-related targets of the SDG 2030 agenda. For natural resource extraction projects, the outcomes of the project might lead to additional HIA-related regulatory requirements under the existing EIA legislation or new policy mechanisms that will be established as an outcome of the policy dialogue. At the same time, more sustainable natural resource extraction leads to: (1) reputational benefits; (2) good partnerships and community relations; (3) increased productivity linked to a healthier workforce; and (4) reduced health-related costs for the workforce. For the society and the affected communities, strengthened HIA practice will lead to better health outcomes and increased productivity, and thus more sustainable development.
Acknowledgments
We would like to thank the following colleagues for their valuable inputs during the conception of the project: Isaac Lyatuu, Dr. Belinda Nimako, Prof. Dr. Don de Savigny, Prof. Dr. Marcel Tanner and Prof. Dr. Jürg Utzinger. We are most grateful to the Swiss Programme for Research on Global Issues for Development (r4d programme) for supporting the HIA4SD Project.
Disclosure statement
The authors declare that they have no conflict of interest.
Additional information
Funding
References
- ADB. 2018. Health impact assessment: a good practice sourcebook. Manila:Asian Development Bank.
- Asante KP, Zandoh C, Dery DB, Brown C, Adjei G, Antwi-Dadzie Y, Adjuik M, Tchum K, Dosoo D, Amenga-Etego S, et al. 2011. Malaria epidemiology in the Ahafo area of Ghana. Malar J. 10:211.
- Bradley J, Rehman AM, Schwabe C, Vargas D, Monti F, Ela C, Riloha M, Kleinschmidt I. 2013. Reduced prevalence of malaria infection in children living in houses with window screening or closed eaves on Bioko Island, equatorial Guinea. PLoS One. 8(11):e80626.
- Brisbois B, Reschny J, Fyfe TM, Harder HG, Parkes MW, Allison S, Buse CG, Fumerton R, Oke, B. 2019. Mapping research on resource extraction and health: A scoping review. Extr Ind Soc. 6(1):250–259.
- Buse K, Hawkes S. 2015. Health in the sustainable development goals: ready for a paradigm shift? Globalization Health. 11:8.
- Carter RC, Danert K. 2003. The private sector and water and sanitation services - policy and poverty issues. J Int Dev. 15:1067–1072.
- Cave B, Pyper R, Gibson G, Fothergill J, Saunders P. 2018. New directive. New World? Health and Environmental Impact Assessment. Eur J Public Health. 28:493–494.
- Chanchitpricha C, Bond A. 2018. Investigating the effectiveness of mandatory integration of health impact assessment within environmental impact assessment (EIA): a case study of Thailand. Impact Assess Proj Apprais. 36(1):16–31.
- Diakite NR, Winkler MS, Coulibaly JT, Guindo-Coulibaly N, Utzinger J, N’Goran EK. 2017. Dynamics of freshwater snails and Schistosoma infection prevalence in schoolchildren during the construction and operation of a multipurpose dam in central Cote d’Ivoire. Infect Dis Poverty. 6:9.
- Dietler D, Leuenberger A, Bempong NE, Campbell-Lendrum D, Cramer C, Eggen RIL, Erismann S, Ferazzi S, Flahault A, Fletcher HA, et al. 2019. Health in the 2030 Agenda for sustainable development: from framework to action, transforming challenges into opportunities. J Glob Health. 9:020201.
- Drewry J, Shandro J, Winkler MS. 2017. The extractive industry in Latin America and the Caribbean: health impact assessment as an opportunity for the health authority. Int J Public Health. 62(2):253–262.
- Equator Principles. 2019. The equator principles: official website. [accessed 2019 Nov]. http://www.equator-principles.com.
- Farnham A, Cossa H, Dietler D, Engebretsen R, Leuenberger A, Lyatuu I, Nimako B, Zabre HR, Brugger F, Winkler MS. 2020. A mixed methods approach for investigating health impacts of natural resource extraction projects in Burkina Faso, Ghana, Mozambique, and Tanzania: a study protocol. JMIR Res Protoc(under review).
- Fischer TB, Matuzzi M, Nowacki J. 2010. The consideration of health in strategic environmental assessment (SEA). Env Impact Assess Rev. 30(3):200–210.
- Fischer TB, Nowacki J, Do Partidario MR. 2012. Strategic environmental assessment, health and health impact assessment. Eur J Public Health. 22:47–48.
- Fox JA. 2015. Social accountability: what does the evidence really say? World Dev. 72:346–361.
- Glasbergen P. 2011. Understanding partnerships for sustainable development analytically: the ladder of partnership activity as a methodological tool. Environ Policy Governance. 21(1):1–13.
- Hacon SD, Perisse ARS, Simos J, Cantoreggi NL, Winkler MS. 2018. Challenges and prospects for integrating the assessment of health impacts in the licensing process of large capital project in Brazil. Int J Health Policy Manag. 7(10):885–888.
- Harris P, Viliani F, Spickett J. 2015. Assessing health impacts within environmental impact assessments: an opportunity for public health globally which must not remain missed. Int J Environ Res Public Health. 12(1):1044–1049.
- Harris-Roxas B, Viliani F, Cave B, Divall MJ, Harris P, Harris P, Harris P, Soeberg M, Wernham A, Winkler MS, et al. 2012. Health impact assessment: the state of the art. Impact Assess Proj Apprais. 30(1):43–52.
- Hossain D, Gorman D, Chapelle B, Mann W, Saal R, Penton G. 2013. Impact of the mining industry on the mental health of landholders and rural communities in southwest Queensland. Australas Psychiatry. 21(1):32–37.
- IFC. 2018. Mapping the oil and gas industry to the sustainable development goals: an atlas. London (Washington DC and New York):IPIECA, IFC and UNEP.
- IHME. 2019. Health-related SDGs. Seattle: Institute for Health Metrics and Evaluation. [accessed 2019 Nov]. http://www.healthdata.org/data-visualization/health-related-sdgs.
- Knoblauch AM, Divall MJ, Owuor M, Archer C, Nduna K, Ng’uni H, Musunka G, Pascall A, Utzinger J, Winkler MS. 2017a. Monitoring of selected health indicators in children living in a copper mine development area in northwestern Zambia. Int J Environ Res Public Health. 14(3):17.
- Knoblauch AM, Divall MJ, Owuor M, Musunka G, Pascall A, Nduna K, Ng’uni H, Utzinger J, Winkler MS. 2018. Selected indicators and determinants of women’s health in the vicinity of a copper mine development in northwestern Zambia. BMC Womens Health. 18:11.
- Knoblauch AM, Divall MJ, Owuor M, Nduna K, Ng’uni H, Musunka G, Pascall A, Utzinger J, Winkler MS. 2017b. Experience and lessons from health impact assessment guiding prevention and control of HIV/AIDS in a copper mine project, northwestern Zambia. Infect Dis Poverty. 6:11.
- Knoblauch AM, Hodges MH, Bah MS, Kamara HI, Kargbo A, Paye J, Turay H, Nyorkor E, Divall M, Zhang Y, et al. 2014a. Changing patterns of health in communities impacted by a bioenergy project in northern Sierra Leone. Int J Environ Res Public Health. 11(12):12997–13016.
- Knoblauch AM, Winkler MS, Archer C, Divall MJ, Owuor M, Yapo RM, Pokou AY, Utzinger J. 2014b. The epidemiology of malaria and anaemia in the Bonikro mining area, central Cote d’Ivoire. Malar J. 13:9.
- Kosack S, Fung A. 2014. Does transparency improve governance? Annu Rev Pol Sci. 17:65–87.
- Krieger GR, Bouchard MA, de Sa IM, Paris I, Balge Z, Williams D, Singer BH, Winkler MS, Utzinger J. 2012. Enhancing impact: visualization of an integrated impact assessment strategy. Geospat Health. 6(2):303–306.
- Kuipers JR, Maest AS. 2006. Comparison of predicted and actual water quality at hardrock mines: the reliability of predictions in environmental impact statements. Bute and Boulder (US): Kuipers and Buka.
- Langston JD, Lubis MI, Sayer JA, Margules C, Boedhihartono AK, Dirks PHGM. 2015. Comparative development benefits from small and large scale mines in North Sulawesi, Indonesia. Extr Ind Soc. 2:434–444.
- Le Billon P. 2003. Fuelling war: natural resources and armed conflicts. Oxford: Oxford University Press.
- Leuenberger A, Farnham A, Azevedo S, Cossa H, Dietler D, Nimako B, Adongo PB, Merten S, Utzinger J, Winkler MS. 2019. Health impact assessment and health equity in sub-Saharan Africa: a scoping review. Env Impact Assess Rev. 79:106288.
- Lim SS, Allen K, Bhutta ZA, Dandona L, Forouzanfar MH, Fullman N, Gething PW, Goldberg EM, Hay SI, Holmberg M, et al. 2016. Measuring the health-related sustainable development goals in 188 countries: a baseline analysis from the global burden of disease study 2015. Lancet. 388(10053):1813–1850.
- Listorti JA. 1996. Bridging environmental health gaps: lessons for sub-Saharan Africa infrastructure projects. New York: The World Bank.
- Lu YL, Nakicenovic N, Visbeck M, Stevance AS. 2015. Five priorities for the UN sustainable development goals. Nature. 520(7548):432–433.
- Morrison-Saunders A, Baker J, Arts J. 2012. Learning from experience: emerging trends in environmental impact assessment follow-up. Impact Assess Proj Apprais. 21:43–56.
- Ncube E, Banda C, Mundike J. 2012. Air pollution on the Copperbelt Province in Zambia: effects of sulphur dioxide on vegetation and humans. Journal Env Sci. 3(1):34–411.
- O’Faircheallaigh C. 2015. Social equity and large mining projects: voluntary industry initiatives, public regulation and community development agreements. J Bus Ethics. 132(1):91–103.
- Otto J, Andrews C, Cawood F, Doggett M, Guy P, Stermole F, Stermole J, Doggett M. 2006. Mining royalties: a global study of their impact on investers, government and civil society. Washington D.C.: The World Bank.
- Pereira CAR, Perisse ARS, Knoblauch AM, Utzinger J, Hacon SD, Winkler MS. 2017. Health impact assessment in Latin American countries: current practice and prospects. Env Impact Assess Rev. 65:175–185.
- Quigley RL, den Broeder P, Furu P, Bond B, Cave B, Bos R. 2006. Health impact assessment international best practice principles. Fargo: International Association for Impact Assessment.
- Richard KM. 2012. Environmental impact assessment: the state of the art. Impact Assess Proj Apprais. 30(1):5–14.
- Ruggie JG. 2007. Business and human rights: the evolving international agenda. Am J Int Law. 101(4):819–840.
- Salcito K, Utzinger J, Krieger GR, Wielga M, Singer BH, Winkler MS, Weiss MG. 2015. Experience and lessons from health impact assessment for human rights impact assessment. BMC Int Health Hum Rights. 15:12.
- Saric J, Blaettler D, Bonfoh B, Hostettler S, Jimenez E, Kiteme B, Koné I, Lys J-A, Masanja H, Steinger E, et al. 2019. Leveraging research partnerships to achieve the 2030 agenda experiences from North-South cooperation. Gaia. 28(2):143–150.
- Shandro J, Jokinen L, Stockwell A, Mazzei F, Winkler MS. 2017. Risks and impacts to first nation health and the mount polley mine tailings dam failure. Int J Indig Health. 12(2):84–102.
- Silveira M, Neto MDA. 2014. Environmental licensing of major undertakings: possible connection between health and environment. Cien Saude Colet. 19(9):3829–3838.
- Thondoo M, Rojas-Rueda D, Gupta J, de Vries DH, Nieuwenhuijsen MJ. 2019. Systematic literature review of health impact assessments in low- and middle-income countries. Int J Environ Res Public Health. 16(11):2018.
- United Nations. 2014. Technical support team issues brief: health and sustainable development. Geneva:United Nations inter-agency technical support team (TST) for the United Nations General Assembly Open Working Group on Sustainable Development Goals.
- Viliani F, Edelstein M, Buckley E, Llamas A, Dar O. 2017. Mining and emerging infectious diseases: results of the infectious disease risk assessment and management (IDRAM) initiative pilot. Extr Ind Soc. 4(2):251–259.
- Westwood E, Orenstein M. 2016. Does resource development increase community sexually transmitted infections? An environmental scan. Extr Ind Soc. 3:240–248.
- Winkler MS, Krieger GR, Divall MJ, Cissé G, Wielga M, Singer BH, Tanner M, Utzinger J. 2013. Untapped potential of health impact assessment. Bull World Health Organ. 91(4):298–305.
- World Bank. 2019. Social safeguard policies. [accessed 2019 Nov]. http://web.worldbank.org/archive/website00660A/WEB/OTHER/6FE66435.HTM?Opendocument.
- Zvijakova L, Zelenakova M, Purcz P. 2014. Evaluation of environmental impact assessment effectiveness in Slovakia. Impact Assess Proj Apprais. 32(2):150–161.