
ABSTRACT
Informal caregiving, meaning taking health-related care of an older and/or disabled person in the personal network, often has consequences for paid work. Classically, scholars focus on two strategies of informal caregivers to adapt employment: stopping to work and reducing working hours. Two other plausible, but neglected, strategies may similarly have career consequences, namely changing jobs and becoming self-employed. First, we empirically assess whether experiencing a work-care conflict is a condition for choosing a work adaption strategy. Second, we theoretically and empirically take a life course (age at start of caregiving episode) and gender perspective on strategies to adapt paid work. We use detailed retrospective data on informal caregiving in the Netherlands (N = 3,673 caregiving episodes of 2,112 caregivers). Applying multilevel logistic regression analysis, we find that caregivers who felt that they had difficulties combining work and care, were more likely to choose any strategy. Especially caregivers who started to provide care at a young age (24 years or younger) were likely to reduce working hours or change jobs. When starting care in the early family formation stage (25–34 years), women were more likely to reduce working hours, whereas men were more likely to stop working in early middle age (45–54 years).
Introduction
Informal caregiving, meaning taking health-related care of older and/or disabled people in one’s personal network, is known to stand in conflict with employment. This conflict can occur throughout one’s entire working life as informal caregiving can intersect with work in different life stages and also multiple times (Fast et al., Citation2020). When experiencing a conflict between informal care and paid work due to role or time strain, informal caregivers may run into a situation where they need or want to adapt employment to better combine care and work. Yet, adapting paid work can have long-lasting consequences and come at a high cost, such as reduced (lifetime) wages or lower pension entitlements (Carmichael and Ercolani, Citation2016). To elucidate the mechanisms behind inequalities in the labour market between informal caregivers and non-caregivers it is, therefore, important to understand the strategies both female and male caregivers choose to adapt paid work in different life stages. In this exploratory study, we aim to provide theoretical and empirical insights into how informal caregiving influences employment over the life course and how that may differ for women and men. Thus far, scholars have focused on two strategies for informal caregivers to adapt their work: stopping work (including early retirement) and reducing working hours. They found that informal caregivers have a higher likelihood to do both (Van Houtven et al., Citation2013; Schmitz and Westphal, Citation2017; Gomez-Leon et al., Citation2019; Hohmeyer and Kopf, Citation2020; Raiber et al., Citation2022a). There are, however, more options that caregivers can choose from, both in the caregiving and paid work domain. We add – theoretically and empirically – two strategies on the employment side, namely changing to a new job and becoming self-employed (Henz, Citation2004; Fast et al., Citation2013). These strategies are relevant for combining work and childcare (Abendroth et al., Citation2014) and likely similarly relevant for working informal caregivers. We transpose the existing theoretical arguments from the childcare literature on choosing different strategies to adapt paid work to the case of informal caregiving. These additional strategies were not or hardly considered so far when it comes to informal caregiving because survey data on informal caregiving most often lack information about these additional strategies. All four strategies likely impact future employment and can have long-lasting consequences, resulting in potential inequalities between caregivers and non-caregivers, which is why it is relevant to look at all four of these strategies to better understand the employment consequences of informal care (Carmichael and Ercolani, Citation2016).
We fill this gap in the literature and focus on the active use of all four strategies, using survey data on caregivers that include explicit information on the occurrence of employment changes because of informal care provision rather than assuming that care provision was the reason to adapt paid work. Explicitly asking if the work adaption was because of providing informal caregiving has the advantage that (a) other reasons for adapting work (e.g. childcare duties) are excluded, and (b) the focus is on active and conscious decisions to adapt employment for the sake of caregiving. All in all, analysing the active use of multiple strategies instead of only two enables us to provide a richer understanding of how informal care affects employment.
In the first step, we look into the assumption that caregivers decide to pursue any of the four strategies because they experience a work-care conflict. After establishing that a work-care conflict is indeed a relevant reason to adapt paid work, as assumed by role conflict theories, we describe under which conditions, based on cost–benefit considerations and social norms related to both caregiving and paid work, caregivers choose a certain strategy. We do so by looking at employment adaption strategies from a life course perspective, more precisely the timing of informal caregiving in the life course, and a gender perspective. We also explore how both perspectives are interconnected as (a) informal caregiving may occur in different stages of a person’s life and therefore variously intersects with other life domains (Fast et al., Citation2013; Moen and DePasquale, Citation2017; Fast et al., Citation2020; Raiber et al., Citation2022b), and (b) caregiving and involvement in paid labour are highly gendered (Smith et al., Citation2020).
Previous research showed that strategies with regard to reducing labour supply are more often chosen closer to retirement and by women (Henz, Citation2004, Citation2006; Moussa, Citation2019; Smith et al., Citation2020), giving the impression that caregivers in later life stages and women are more likely to adapt paid work because of care. Caregivers in earlier life stages and male caregivers can similarly experience a work-care conflict and, subsequently, adapt paid work because of that conflict, yet their strategy might just be a different one. The strategies that were traditionally studied in the literature are likely those that are picked most by older adults and women. Looking at the alternative strategies (changing jobs or becoming self-employed), which were not observed in prior studies, could reveal that younger caregivers and men also adapt paid work, which then potentially has consequences for their career prospects as well. Put together, we explore to what extent caregivers (a) reduce working hours, (b) stop work, (c) change jobs, and (d) become self-employed if they experience high work-care conflict. We further explore whether the use of these strategies depends on the life stage in which a caregiving situation starts and whether female or male caregivers use different strategies.
We use retrospective primary data on informal caregivers in the Netherlands, collected among the sample of the Longitudinal Internet studies for the Social Sciences (LISS). We perform multilevel logistic regression analysis on 3,673 caregiver episodes of 2,112 caregivers who worked (at least for some time) while caregiving. Our observation window ranges from the first caregiving episode reported in 1954 until the moment of the survey in 2020. This unique dataset, based on a representative sample of the Dutch population, contains detailed information on past and current caregiving situations as well as a measurement of the active use of strategies to adapt paid work for separate caregiving episodes.
The work-care conflict
Caregiving may not only have a negative influence on the caregiver but also may have positive effects, such as personal growth (Pysklywec et al., Citation2020). Adapting paid work because of informal caregiving may relieve stress and a life with paid work and care combined can be more fulfilling. However, to choose a work adaption strategy, there must be some kind of work-care conflict where the caregiver is not able to satisfactorily combine caregiving duties with employment. Caregiving can conflict with paid work when the new social role – the role of caregiver – is competing with the work role (Greenhaus and Beutell, Citation1985). Care and paid work then compete both role- and time-wise. Three proximate causes of work-care conflict are generally distinguished: role strain, time constraints, and contradicting behaviour (Greenhaus and Beutell, Citation1985). Role strain means that worries of one role can spill over to another, making both roles more difficult and resulting in role strain. Time constraints refer to one role taking up too much time, not leaving sufficient time for the other role(s) as one can only devote time to one role at a time. Contradicting behaviour implies that behaviour and tasks in one role contradict the behaviour and tasks in the other role(s), which makes the roles incompatible (e.g. emotional closeness expected in the care role but emotional distance in the work role). For all three reasons, if the work-care conflict is getting too strenuous, caregivers have to decide how to handle it (Lilly et al., Citation2007). If a caregiver comes into a situation where care and paid work interfere to a worrisome level, either role- or time-wise, the caregiver might adapt paid work by considering the use of one of the here discussed strategies.
The decision-making process
Choosing a certain strategy to adapt paid work is not easily done and it is a process during which alternative options are weighted, including choosing none of the here discussed strategies. Not choosing a certain strategy represents situations in which the caregiver (a) has changed nothing at all, (b) has chosen a non-work-related strategy (e.g. changing the care situation), and/or (c) has chosen an alternative employment strategy (which we do or do not observe in this study). This means that not choosing a certain strategy not only includes alternative strategies, but also the option of not changing anything, which directs the attention to the active decision to use that particular strategy.
The theory of compensating differentials states that workers are willing to give up some of their employment prospects for better working conditions (Yu and Kuo, Citation2017). Caregivers can use different strategies to lower the work-care conflict and have better working conditions to provide care. Reducing labour supply by reducing working hours or stopping paid work altogether is examined most often in the informal care literature and the relationship between informal caregiving and reducing labour supply is supported by many empirical studies (Pavalko and Henderson, Citation2006; Schmitz and Westphal, Citation2017; Gomez-Leon et al., Citation2019; Hohmeyer and Kopf, Citation2020; Raiber et al., Citation2022a). A reduction of working hours or dropping out of employment can normally be arranged with the employer relatively quickly, thus offering an immediate reduction of the work-care conflict. Reducing labour supply, however, comes at the price of reduced monthly income and long-term negative consequences for the work career, such as fewer promotion opportunities and reduced pensions. Stopping paid work completely is then the more extreme form of labour supply reduction while reducing working hours is a less extreme one, particularly in the Dutch context with a large share of part-time workers (Hartog and Salverda, Citation2018).
In contrast to strategies that reduce the salience of the work role, caregivers might choose strategies that do not diminish the work role, but still have the potential to lower the work-care conflict. The first additional strategy, argued for in the childcare literature, is changing to another job that is easier to combine with informal care (Arai, Citation2000; Abendroth et al., Citation2014; Looze, Citation2017). As proposed in the theory of compensating differentials, caregivers might be willing to give up favourable features of their current job if their new job has better conditions to combine it with care provision, such as flexible working hours or an employer who has more understanding of what it means to be a caregiver (Yu and Kuo, Citation2017). However, finding a new job requires time and energy and could include the need to move. It may additionally bring the risk that caregivers harm their future employment because they choose less demanding jobs that are often associated with lower status and fewer career development opportunities (Arai, Citation2000; Abendroth et al., Citation2014).
Also discussed in the childcare literature is the strategy to become self-employed as it promises even more flexibility by choosing when and where to work (Arai, Citation2000; Budig, Citation2006; Matysiak and Mynarska, Citation2020; Lim, Citation2019). This is again a strategy that may make paid work and care more compatible but is also considered risky because starting your own company may fail and earnings are volatile (Ferrín, Citation2021). Becoming self-employed also requires energy, time, and financial investments (Conen and Debets, Citation2019). Especially for the solo self-employed, (the need for) higher earnings directly require long working hours (Arai, Citation2000). Furthermore, there are no mandatory disability and retirement schemes for the self-employed in the Netherlands (Conen and Debets, Citation2019). Self-employed persons have to arrange such (expensive) insurance themselves while wanting to invest profits into their company.
We consider four major factors influencing caregivers’ decision-making concerning paid work adaptions and choosing a certain strategy. Each of these factors presumably works out differently depending on the caregiver’s life stage and gender. We introduce the four factors here more generally and, in the next section, we relate them in more detail to life stage and gender. The first factor comprises family circumstances, other than the informal care provision, that may add to the work-care conflict, such as having young children. The second factor is caregivers’ (personal, household, or network) financial resources that determine to what extent changes in paid work can be afforded. For certain strategies to be chosen, like becoming self-employed, more financial resources are needed, meaning that caregivers have to weigh the benefits of choosing certain strategies against the costs of worse labour market outcomes (e.g. potentially lower wages). The third factor relates to norms and expectations regarding informal caregiving as well as employment (Hamilton and Adamson, Citation2013). The fourth factor is about the employers’ views on work commitment. People who show that they value something in their private sphere over work, such as caregiving, can deviate from ‘the ideal worker’ norm and be seen as less committed to paid work and this may have long-lasting consequences in the labour market (Ehrlich et al., Citation2019; Minnotte and Minnotte, Citation2021).
Gender and life stage
Life stages are highly gendered (Moen, Citation2001; Patterson and Margolis, Citation2019). Women and men in different life stages are in different relationships and social dependencies, especially when it comes to work and care (Moen, Citation2001). This implies different costs and benefits for men and women in choosing a certain strategy versus not choosing it. Similarly, there are norms on what men and women should do in the work and care domain. In the Netherlands, a country that still has traditional gender roles, women are generally seen as the primary caregiver and less involved in the workforce, whereas men are stereotypically the breadwinner who tends to value paid work over care (Kaufman and Uhlenberg, Citation2000; Smith et al., Citation2020; Vink, Citation2020). These views are internalized by male and female caregivers as well as employers, who might interpret a work reduction by men as a stronger sign of being less committed than for women as a result of deviating from the breadwinner norm (Cooklin et al., Citation2016). As a result, men could be more prone to pick strategies that keep a focus on paid work while combining it with care, that is, changing jobs and becoming self-employed. Women, in contrast, may be more likely to choose strategies that emphasize their care role by reducing work. However, these general explanations on gender differences are expected to be conditional on the life stages, which we discuss in the following after we explained the general mechanisms underlying the relation between each life stage and potential work adaptations.
We distinguish five life stages in which informal caregiving can start: (1) Young caregivers (24 or younger), (2) early family formation stage (25–34)Footnote1, (3) late family formation stage (35–44), (4) early middle age (45–54), and (5) late middle age (55 and older). Young caregivers form a special group because they started caregiving while still deciding on a job (Hamilton and Adamson, Citation2013) and are in a life stage in which caregiving is not yet socially expected (Bertogg et al., Citation2020). Young caregivers typically have fewer other responsibilities, such as childcare or financial expenses, which results in less dependence on their income, so fewer factors on the cost side to adapt work for care compared to other life stages. They are also more flexible to move to another location for a job. Nevertheless, young caregivers might focus more on educating themselves, gaining work experience, and developing relevant skills to find stable employment (Abendroth et al., Citation2014). For this age group, having few employment interruptions is important for accumulating human capital. Losses in or limited accumulation of human capital early in the work career can accumulate over the life course and set people back (Crystal et al., Citation2016). Thus, this (young) age group has to balance the need to improve their labour market position with the possibility to adapt paid work as they are less dependent on their income and have fewer restrictions in finding a new job or becoming self-employed. Because men and women in this life stage do not differ much in terms of resources and (own and employers’) expectations are not highly gendered in this pre-family life stage, gender differences are expectedly relatively small in this life stage.
Caregivers in the early family formation stage may have a stronger focus on investing in employment and career building, as it is still early in their work career, yet they are also planning a family (Fast et al., Citation2020). This not only includes having children but might also mean buying a house and obtaining a mortgage (Keijer et al., Citation2016). Combining the informal caregiving role, employment, and care for young children can create a so-called ‘triple burden’ with additional time issues and more strain, leading to even more work-care conflict (Brenna, Citation2021). Caregivers, as well as employers, might expect a work reduction in this life stage, but likely due to childcare and less as a result of informal care. Caregivers in the early family formation stage might not be able to afford to lose part of their income because of (further) reducing labour supply, yet cannot afford to do so career-wise, thus have higher costs of reducing labour supply compared to other life stages. It is likely that they choose a strategy that enables them to combine paid work and care, like changing jobs or becoming self-employed. Self-employment is arguably less favourable compared to switching jobs in this life stage as self-employment takes time and financial resources that might not be available. In this life stage of early family formation, men and women typically start following gendered paths more strongly than earlier in life. Partly as a result of this, men earn more than women, which makes it more costly for men to reduce their labour supply (Blau and Kahn, Citation2017). Strategies that maintain a strong focus on the work role will therefore presumably be more prominent among men than among women.
In the late family life stage, raising children and advancing in one’s career are still relevant (Fast et al., Citation2020), but caregivers might be a bit more established in the labour market and children are getting older, decreasing the triple burden. Therefore, changing jobs (and to some extent self-employment) might still be a better option in the late family stage, though the need to combine paid work and care might be slightly less than in the early family formation stage. The late family life stage is still, but less compared to the early family stage, gendered with women potentially experiencing a greater ‘triple burden’ and men typically fulfilling the breadwinner role.
Early and late middle age are the life stages in which it is typical and expected to care for someone in the personal network (Fast et al., Citation2020). In both age groups, employment is usually more stable and work careers are in a more advanced stage. Other obligations (e.g. paying a mortgage) may become less important, which makes labour supply adaptions more affordable for some. Especially caregivers in late middle age are getting closer to their retirement and have comparably less to lose if they are reducing paid work because of informal caregiving because they typically do not make big career steps anymore or they paid sufficient pensions contributions to receive their desired level of pension income (Damman et al., Citation2013). Changing jobs is arguably the less likely route because caregivers who are already near retirement might be less willing to do so due to the higher risks and the efforts involved in searching for another job. They also have fewer chances of finding a new job compared to younger people related to stereotypical views of older workers or less time for employers to get returns for investing in workers closer to retirement (Wanberg et al., Citation2016). Becoming self-employed could be an alternative for people in these life stages as they, or their partner, could have the required financial resources and work experience to take this risk. Contrastingly, setting up a business takes time before it becomes profitable, making it less attractive for these age groups as retirement is nearing. As care for children is not central anymore in this life stage and – under the condition that the household income level is satisfactory – the breadwinner role becomes less pressing, that is, men and women may experience and feel less pressure to follow traditional gender roles. Similarly, women and men might have already chosen gendered career paths in previous life stages and arranged alternative pension resources (like relying on the pension of their partner). We, therefore, believe that gender differences in the strategies chosen may be limited in this life stage.
Methods
Data
The empirical analysis was conducted on a sample of caregivers retrieved from the Longitudinal Internet studies for the Social Sciences (LISS), administered by CentERdata (Tilburg University, the Netherlands). The LISS respondents are based on a representative sample of the Dutch population (see www.lissdata.nl and Scherpenzeel and Das, Citation2010: for more information). The analysis is based on an additional module named ‘Retrospective informal care career’ (Verbakel and CentErdata, Citation2021). All LISS respondents were asked in January 2020 if they care or ever cared for someone in their personal network (response rate 83%, 5,315 respondents).Footnote2 Those who answered ‘yes’ (71%) and were aged 16–78 were asked retrospective questions about up to seven informal caregiving episodes in March 2020Footnote3 (response rate 87.5%, 3,061 respondentsFootnote4). For a maximum of three episodes, respondents provided detailed information, including questions on employment during the caregiving episode. If more than three episodes were indicated (in 26% of the cases in our sample), three episodes were randomly chosen. Retrospective data have been criticized to rely too much on the memory of the respondent; respondents would not be able to recall all their past activities (so-called ‘recall bias’, see Kjellsson et al., Citation2014). We are confident this is less of an issue in the current study as adapting work because of care is a very active and consequential decision, most likely remembered by respondents. Caregiving episodes that might have been forgotten are likely caregiving episodes with lower intensity and work-care conflict (Fast et al., Citation2020).
Sample selection
We only selected caregiving episodes of caregivers when (a) the extended questionnaire – including the questions on paid work – was filled in (up to three random episodes), (b) the age at onset of informal care provision was before retirement (65 or younger), and (c) the caregiver worked at some point during the caregiving episode. Caregivers were excluded if no start or end date of the first care episode was available as no caregiving episodes could be constructed (38 caregiving episodes of 38 caregivers excluded). If the start date was before the birth date of the respondent or below the age of five, the caregiving episode was excluded because these values were considered unrealistic and likely measurement errors (12 caregiving episodes of 7 caregivers). Note that changing the lower limit to 10 years did not change our results and that even if the caregiving started at age 5 or above the episode was only included when the caregiver also experienced employment at any time during the episode (point c above). In case the caregiving episode was not identifiable as informal care (but for instance as paid care work or formal volunteering), we excluded the episode (86 caregiving episodes of 35 caregivers excluded). Finally, after the deletion of missing values (1.42%, 53 caregiving episodes) our final sample consisted of 3,673 caregiving episodes nested in 2,112 caregivers. For 57% of respondents, we have the extended information (including work adaptions) on one episode, for 30% on two, and for 13% on three episodes.
Measures
Dependent variables. Caregivers were asked the following survey questions:
‘Did your work situation change at any point because of the care you provide(d) to ? (a) Did you start working fewer hours? (b) Did you stop working? (c) Did you start doing different work? (d) Did you start working in self-employment? (e) Did you stop attending an education program?’
Main predictors. The first set of predictors relates to the causes of work-care conflict. Our first main predictor was caregiving intensity, measured as the average hours of providing care per week between the start and end of a caregiving episode, divided by ten hours for ease of interpretation in the multiple regression models. We expect a non-linear effect of intensity because the more hours of care, the weaker the impact (e.g. the difference between 50 and 51 hours may matter less compared to the difference between 1 and 2 hours). This is why we included a squared term. Caregiving tasks were measured as the sum of tasks provided at the beginning of the caregiving episode, with a maximum of nine tasks, which were: companionship or emotional support, transportation, assistance when visiting a doctor, administrative help, housekeeping, personal care, nursing care, arranging or coordinating care, and/or other tasks. Difficulties to combine work and care were measured on a 5-point Likert scale, ranging from completely disagree to completely agree on the following item: ‘I find/found it stressful to combine my work with providing care to’.
The timing of the caregiving episode was included as the life stage in which the episode started. We created five distinct life stages: (1) below the age of 24 (young caregivers, with a minimum age of 5), (2) between the age of 25 and 34 (early family formation stage), (3) between the age of 35 and 44 (late family formation stage), (4) between the age of 45 and 54 (early middle age), and (5) between the age 55 and 65 (late middle age, with the maximum age corresponding to the state pension age). For the variable biological sex of the respondent, we used the predefined variable from the LISS panel, coded man (0) and woman (1).
Control variables. At the caregiving episode level, three variables, all measured at the end of the caregiving episode, were used to indicate the health status of the care recipient: (a) an indicator of dementia (no memory problems, some memory problems, or serious memory problems), (b) an indicator of mental health problems (no mental health problems, some mental health problems, or serious mental health problems), (c) and an indicator of physical health problems, measured by the sum of daily activities the care receiver had difficulties with (IADL and ADL, specifically: problems with walking, dressing, eating, housekeeping, grocery shopping, or preparing meals). The relationship of the caregiver to the care recipient, related to (gendered) norms about adapting work for care and differences between people who need care in these categories, was measured with three categories: (1) close family, including partner, (step-)parents(-in-law), and (step-)children (with health issues; so not regular childcare), (2) other family members, and (3) friends or neighbours. Three life course controls were added: duration of the caregiving episode was measured as the time in years between the start and end date of the caregiving episode. If the caregiver was still providing care at the moment of the interview, the interview date was taken as the ‘end’ date. Order refers to the chronological order of the particular episode in the caregiver’s life course, with seven episodes being the maximum. We additionally took into account potential period effects by controlling for the middle calendar year of the caregiving episode as (gendered) norms and values towards work and care changed over time.Footnote5
Employment-related adaptions depend on factors beyond gender and the life stage in which care is given, such as occupation, socioeconomic status, a partner providing alternative income, and support of other people in the social network. Many of these factors were not available retrospectively for the observation window. Yet, at the caregiver level, we controlled for the highest obtained educational level of the caregiver at the time of the survey to account for socioeconomic status, potentially fewer resources to finance formal care, and for the feasibility of certain strategies.Footnote6
Analytical strategy
To account for the hierarchical structure of our data in which caregiving episodes were clustered in caregivers, we performed multilevel logistic regression analysis (melogit in STATA 17; significant intraclass correlation coefficients for empty models for reducing working hours: 0.54, stopping to work: 0.61; changing jobs: 0.61; becoming self-employed: 0.77).Footnote7 In four separate models, we regressed each of the four strategies on the indicators of work-care conflict, life stage, gender, and control variables. This means we compared caregivers who choose a certain strategy to caregivers not choosing that strategy. For the presentation and interpretation of the results, we used marginal effects at the mean (MEM) (Mood, Citation2010). We included random coefficients for the life stage dummy variables in the models that estimated interactions between life stages and gender. Yet, these models only converged when all variances were kept equal and covariances were set to zero (predefined option in melogit), except for the model on becoming self-employed which did not converge even with equal variances. Thus, for the model on self-employment, we present the results from the model without random slopes.
Results
Descriptive and bivariate results
Caregivers adapted their work because of caregiving by using at least one strategy in 10.8% of their caregiving episodes. At first glance, this number seems low. Other scholars reported substantially higher adaption rates for informal caregivers. For instance, 30% of caregivers made a change in the work domain in Great Britain in 1994–95 (Henz, Citation2004) and 20% of caregivers in Canada in 2007 (Fast et al., Citation2013). In contrast to previous research, we included caregiving episodes over the complete past of a person, meaning that also caregiving episodes of short length were included, which could explain the lower work adaption rate. On average, caregivers indicated that they felt difficulties with combining work and care in 17.2% of the caregiving episodes, partly explaining the lower rate of adaptions compared to previous research. Additionally, as some caregiving episodes did not end at the moment of the interview, the number of adaptions might in reality be slightly higher. Among those caregivers choosing at least one strategy, 73.6% chose only one strategy and 26.4% chose multiple ones (18.6% chose two, 6.0% three, and 1.8% all strategies).
shows descriptive information on all variables. As expected in the Dutch context, a context where reducing working hours is relatively easily realised, reducing working hours happened most often, namely in 7.3% of the caregiving episodes. Stopping to work occurred in 3.8% of caregiving episodes, changing jobs in 1.7% of caregiving episodes, and becoming self-employed in 1.8% of caregiving episodes. The caregiving episodes started almost equally often in different life stages (between 21.3% and 23.1% for each life stage), with the exception that caregiving episodes started least often in late middle age (9.6%). This might sound surprising as we know from the literature that caregivers are on average middle-aged (De Boer et al., Citation2020). Note that the numbers presented here are based on a retrospective data collection where we asked caregivers – of different ages – when their caregiving episodes started. Our sample of caregivers is on average 53 years old with over half of the respondents being older than 55, so half of the respondents could not have an episode starting after age 55. Furthermore, we focus on the starting age of caregiving, meaning that respondents older than 55 who are currently caregiving still could have started their caregiving before this age.
Table 1. Descriptive statistics.
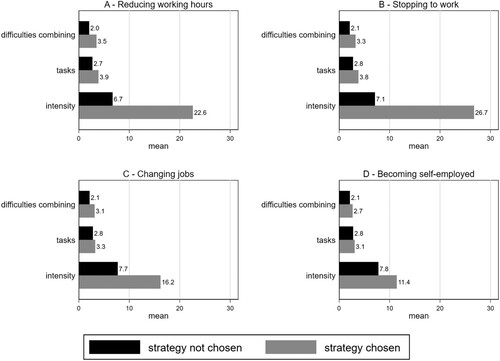
Work-care conflict. Regarding our measures of work-care conflict, we see that caregivers who used a strategy cared for more hours, had more tasks, and felt more difficulties in combining work and care. displays the average intensity, number of tasks, and difficulties combining work and care by strategy chosen versus not chosen. For becoming self-employed, the differences were smallest, but with still a notable difference in intensity. All bivariate differences were significant on the 5%-significance level based on t-tests, except for the relationship between the number of tasks and becoming self-employed.
Figure 1. Average values of intensity, number of tasks, and difficulties combining work and care for caregiving situations in which the strategy was (not) chosen. N = 3,673 caregiving episodes of 2,112 caregivers All differences were significant (p < 0.05), except for the number of tasks for becoming self-employed.
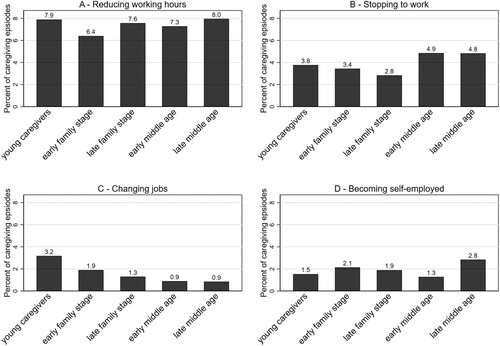
Life stages. Overall, bivariate relationships between the life stages and reducing working hours, stopping to work, and becoming self-employed were non-significant based on Pearson’s chi2 tests, but significant for changing jobs (chi2 = 16.2, p = 0.003). Some of the descriptive values lie close to each other, meaning that differences are in general relatively small (see ). Reducing working hours was the most prevalent in caregiving episodes that started in the oldest as well as the youngest life stage (7.9% for both), followed by the late family formation stage, early middle age, and the least in the early family formation stage (6.4%). Caregivers who started in early middle age stopped working the most (4.9%), followed by late middle age (4.8%) and then young caregivers (3.8%). Changing jobs was most likely in caregiving episodes that started in the youngest life stage (3.2%). Caregivers in episodes that started in the early family stage chose to change jobs in 1.9% of the episodes, in the late family stage in 1.3% of the episodes, and early and late middle age in less than 1% of the episodes. Last, we observed some small differences between the life stages for becoming self-employed, with late middle age being the life stage in which self-employment was chosen the most.
Figure 2. Percentage of caregiving episodes in which the strategy was chosen by life stage. N = 3,673 caregiving episodes of 2,112 caregivers. Differences between life stages are rather small and only for changing jobs, the life stages are distinct from each other on a 5%-significance level.
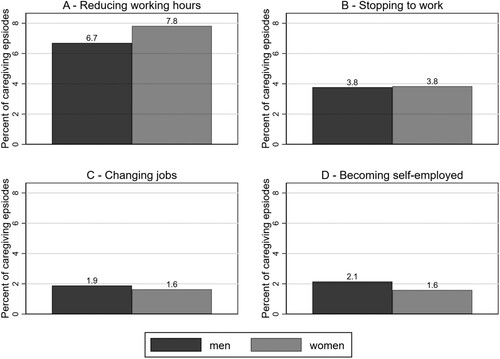
Gender. We observe that reducing working hours was chosen in 7.8% of caregiving episodes of women and 6.6% of the episodes of men (see ). There was no difference in stopping to work between women and men, both in 3.8% of their caregiving episodes. Changing jobs was chosen in 1.9% of the caregiving episodes of men, whereas women were slightly less likely to change jobs (1.7%). Becoming self-employed was chosen more often by men (2.1% of their episodes) than women (1.7% of their episodes). There were, however, no significant bivariate associations between the sex of the respondent and any of the four strategies based on chi2 tests.
Figure 3. Percentage of caregiving episodes in which the strategy was chosen by sex. N = 3,673 caregiving episodes of 2,112 caregivers. Differences were not statistically different on a 5%-significance level.
Work-care conflict by life stage and gender. By running bivariate linear regressions with clustered standard errors, we found that caregiving episodes that started in the young caregiving stage were characterized by lower intensity (compared to the early family formation stage and early middle age), fewer tasks (compared to all life stages except late middle age), and fewer difficulties with combining work and care (compared to the late family formation stage and early middle age). Women experienced, on average, higher caregiving intensity and had more difficulties with combining work and care.
Multiple regression results
Work-care conflict. We see that for all four strategies, higher work-care conflict was positively related to the likelihood that a certain strategy was chosen. Experiencing difficulties in combining work and care was the most predictive of choosing any of the four strategies. A one-point increase on this scale increased the likelihood to reduce working hours by 3 percentage points, the other strategies all by 1 percentage point. The results further show that a ten-hour increase in intensity increased the likelihood to reduce working hours and stop working by 3 percentage points for reducing hours and 1 percentage point for stopping work. Every additional task increased the likelihood to reduce working hours by 1 percentage point.Footnote8
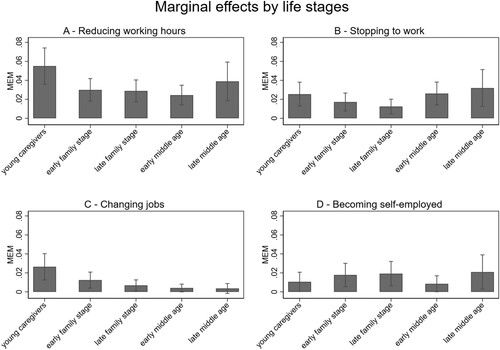
Life stages. The results for the different life stages are presented in . For stopping to work and becoming self-employed, it did not matter in which life stage the caregiving episode started. Yet, young caregivers were 3 percentage points more likely to reduce working hours compared to three of the other life stages, that is, the early family formation stage, late family formation stage, and early middle age. No other statistical differences were detected for reducing working hours. In a similar vein, young caregivers significantly differed from people in other life stages when it came to changing jobs. Young caregivers had a 2 percentage point higher likelihood to change jobs compared to the late family formation stage and caregivers in early and late middle age.
Figure 4. Marginal effects at the mean for choosing a strategy by life stage. N = 3,673 caregiving episodes of 2,112 caregivers. Life stages are significantly different from each other if the 95% confidence interval does not overlap with that of the other category.
Excluding the work-care conflict indicators (intensity, tasks, and having difficulties combining paid work and care) did not change the results for stopping work, changing jobs, and becoming self-employed (see Table A1 in the supplementary material). The difference between young caregivers and the other life stages in their likelihood to reduce working hours became non-significant, indicating that only when keeping work-care conflict stable, some of the differences between the life stages become apparent. This hints at the following: only if caregivers with similar levels of work-care conflict were compared, we were able to observe that young caregivers were more likely to reduce working hours; in the bivariate results this tendency was masked by the fact that young caregivers on average experience less work-care conflict.
Gender. shows there were no statistical differences between women and men in choosing a given strategy. When looking at the interactions between sex and life stage (see and Table A2 in the supplement), we observe that an average woman was significantly more likely compared to an average man to reduce working hours by 2.2 percentage points in the early family stage. Contrastingly, men were 2.8 percentage points more likely than women to stop working in early middle age.
Figure 5. Marginal effects at the mean for choosing a strategy in a certain life stage conditioned on sex. N = 3,673 caregiving episodes of 2,112 caregivers based on the models presented in Table A2 in the supplement material. Significant differences between men and women are highlighted by asterisks (* p < 0.05).
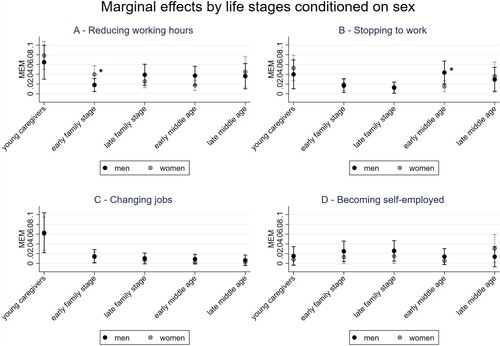
Table 2. Multilevel logistic regression analysis of reducing working hours, stopping to work, changing jobs, and becoming self-employed.
Conclusion
Starting to provide informal care means taking on a new role. Time and energy that before was available for other roles are reduced. A role that may get into conflict with the role of caregiver is the work role. In this study, we found that caregivers who experienced stronger work-care conflict were more willing to adapt paid work because of caregiving, supporting role conflict theories (Greenhaus and Beutell, Citation1985). Adding to existing literature, we not only considered the two typical strategies (reducing work hours and stopping to work) but added two alternative strategies related to the work sphere that informal caregivers can also use when they work and care at the same time: changing jobs and becoming self-employed. We proposed that in the decision process to choose or not to choose a certain strategy, it is important to consider the life stage in which a caregiving episode started, the caregivers’ gender, as well as the interaction between life stages and gender. We found that reducing working hours was associated with the timing of the start of the caregiving episode as this strategy was especially prevalent in caregiving episodes that started in the earliest life stage (age 24 or younger). Changing jobs was similarly more likely in the earliest life stage. For the other two strategies, stopping to work and becoming self-employed, we did not find an association with the life stage in which the episodes began. This shows that especially young caregivers need to and are more willing to reduce working hours or change jobs under the condition of an experienced work-care conflict. Theoretically, this finding may be interpreted as young caregivers being less dependent on their income and more flexible to change to another job, potentially by moving to another location for that new job. In later life stages, reducing working hours or switching jobs might not form a good alternative as caregivers are then too dependent on the income provided by paid work and/or are too settled or not flexible enough to relocate for a new job. This could mean that not choosing any strategy is then the better option compared to choosing a strategy with too many perceived disadvantages.
Regarding gender, we did not find indications that female and male caregivers generally made different decisions when it comes to the strategies. What we did see and what potentially explains the non-existent gender gap is that in certain life stages women and men were more (or less) likely to choose certain strategies. Reducing working hours was more likely in the early family stage for women compared to men. This is in line with the theoretical idea that informal care and childcare together create a ‘triple burden’ for women as the traditional caregivers, but not for men. In contrast, in early middle age (between age 45 and 54) men were more likely than women to drop out of employment. A potential explanation, as put forward by gender role theories, is that men consider stopping to work as a reasonable strategy to improve their work-care conflict when they are already established in the labour market and have built a career for themselves. The importance of men’s income for the household income (i.e. the male breadwinner model) might be lower in early middle age while women might still focus on their employment in this life stage. The fact that we did not find more gender differences could be because female and male caregivers might be very similar in their attributes. We kept constant, for instance, whether the caregiver provided care to a close family member (such as a partner or parent), other family members, or friends/neighbours. When controlling for different caregiving situations, similar caregivers choose similar work adaption strategies. In addition, the women and men in our sample already decided to become caregivers, which could mean that they highly valued care, were willing to spend time on caregiving, and had comparable views on their labour market engagement (e.g. men who provide care might not be the typical breadwinners). Alternatively, women and men might have different positions in the labour market before starting to informally care, with women working and earning less (Blau and Kahn, Citation2017; Hartog and Salverda, Citation2018). Given these different starting points, two mechanisms might hinder both sexes from choosing the expected strategies. First, women might have working conditions that facilitate combining work and care. For instance, they on average work fewer hours, which makes the option to even further reduce work hours less feasible. Also, women already work more often in sectors or occupations that facilitate combining work and care, so changing work likely will not bring additional advantages. Second, men have on average higher wages, which may make it more costly to choose any strategy that adjusts work in favour of a better work-care balance.
We had the opportunity to look at four work adaption strategies and at the same time concentrate on the active and conscious use of these strategies. With previous data sources, it was not possible to include these alternative strategies and to disentangle the life stage and gender effects of informal caregiving for each strategy separately. However, our approach also comes with limitations. First, though we accounted for selection effects into caregiving by only comparing people who provided care, other potential selection effects may exist for which we could not control. One example is that women and men may have different labour market situations before they started caregiving. For instance, there might be ceiling or bottom effects depending on the previous working hours which are already gendered. To better detect gender differences in work adaptions, future research is invited to include employment characteristics (such as type of job, sector, and working hours) at the start of the caregiving episode. Second, we had no direct measurements of the proposed theoretical mechanisms. We simplified the decision-making process of caregivers by assuming that caregivers in the same life stage are homogeneous, for instance regarding the available financial resources, presence of young children, etcetera. Yet, caregivers likely vary in their levels of financial resources and other caring tasks (which for instance depend on the presence and income of a partner), even when being in the same life stage. To cancel out some heterogeneity between caregivers, we included the highest level of education in our models. To better understand the mechanisms for choosing a certain work adaptation strategy, direct measurements of the mechanisms are to be preferred. Third, although we know that the work adaption took place during the caregiving episode, we cannot completely be sure that the work adaption took place in the same life stage as the one in which caregiving started (which is our measurement of life stages). As a result, our conclusions regarding life stage differences may be less precise. Typically, such measurement error underestimates effects. At the same time, we have reason to think that this issue will not have seriously affected our conclusions regarding life stages. Only in a minority of cases, we will have linked the work adaption to the wrong life stage. Especially longer caregiving episodes may span multiple life stages, but in our sample half of the caregiving episodes span for a maximum of 3 years, whereas our life stages span for 10 years. Furthermore, anticipation effects may occur. Although the course of caregiving situations can never be fully predicted, it can be argued that in a part of the caregiving episodes that in the end appeared to be long, caregivers could already anticipate the potential burden of it at its onset. After all, duration and what will be expected from caregivers are related to the relationship to the care recipient (e.g. parent, partner, child) and his/her health conditions. In such cases, the adaption may have taken place in the life stage in which the caregiving started.
To conclude, the Netherlands is a context in which working part-time is relatively easy to arrange, has similar employment protection and conditions as working full-time, and is less stigmatized compared to other countries (Hartog and Salverda, Citation2018; OECD, Citation2022). Looking at this context, we can draw some policy-related conclusions on the Netherlands and outside. Reducing working hours indeed proved the most chosen strategy and other strategies are used less frequently. The Dutch context can be considered a least likely case for strategies other than reducing working hours. This means that the differences in changing jobs for younger caregivers that we found in this context could be even stronger in others, making it important for policymakers to not only focus on the traditional group of caregivers in late middle age but also focus more on support for young caregivers. Other countries can infer from the Dutch case that more rights towards reducing working hours (but likely also other strategies for caregivers) can lead to a better combination of paid work and caregiving. However, decreasing working hours should ideally go hand in hand with financial security to not have an increasing number of caregivers suffer from poverty during caregiving or after it ended.
Competing interest
The authors report there are no competing interests to declare.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data ‘Retrospective informal care career: Main measurement’ that support the findings of this study is openly available in the LISS data archive, CentERdata at https://doi.org/10.17026/dans-xyf-v7vu. Replication files will be openly available via https://figshare.com/articles/software/Replication_syntax_article_Strategies_of_Informal_Caregivers_to_Adapt_Paid_Work/22101665.
Additional information
Funding
Notes on contributors
Klara Raiber
Klara Raiber is a Ph.D. candidate in Sociology at the Radboud University in Nijmegen, the Netherlands, and the SCOOP program. Her research focuses on gender, informal care, employment, and the life course perspective.
Mark Visser
Mark Visser is an Assistant Professor in the Department of Sociology at Radboud University, Nijmegen, the Netherlands. His major research interests include older workers and retirement, social inequality, voting behaviour and the welfare state.
Ellen Verbakel
Ellen Verbakel is a full professor General and Theoretical Sociology at Radboud University Nijmegen. She is particularly interested in family, work, and well-being, with a special focus on partner relationships, partner effects, and informal care provision.
Notes
1 This is a reasonable age range considering the Dutch context. On average, both women and men have their first child within this age range and the majority of people who can afford buying a house has already done so (Statistics Netherlands (CBS), Citation2019; Statistics Netherlands (CBS), Citation2018) Shifting the scale up by two years (first category till 26) did not change our main results.
2 Survey question: ‘Below we will ask you to indicate all the people known to you to whom you have ever offered informal care on account of their health issues. These people could be your partner, a family member, a friend, neighbor, acquaintance or colleague who needs or needed help because of physical, psychological or mental limitations or because of old age. Examples of informal care are doing household chores, helping with washing and dressing, keeping company, providing transport or performing odd jobs. You may have done so for a short period or for a long period. It could involve people known to you to whom you provided care in the past, but could also involve people known to you to whom are providing care at present. Care provided as part of your occupation or as a volunteer does not count. Please take a moment to think about the people known to you to whom you have provided or are providing informal care on account of health issues.’ (Verbakel and CentErdata, Citation2021).
3 Raiber et al. (Citation2021) found that the start of the COVID-19 pandemic in March 2020 did not influence the answer patterns regarding ongoing caregiving episodes.
4 Those not in the final sample even when indicating caregiving in the January questionnaire were not significantly different in age or sex compared to the respondents in the final sample.
5 Choosing the start year of the episode instead of the middle year did not change the results.
6 Education is partly related to some of the theoretical mechanisms and might mediate our main relationships. Excluding education did however not alter our findings.
7 The code underlying this article is open accessible via https://figshare.com/articles/software/Replication_syntax_article_Strategies_of_Informal_Caregivers_to_Adapt_Paid_Work/22101665
8 When excluding the item on felt difficulties to combine work and care, intensity became a significant predictor of changing jobs, and tasks became a significant predictor of stopping to work.
References
- Abendroth, A.-K., Huffman, M. L. and Treas, J. (2014) ‘The parity penalty in life course perspective: motherhood and cccupational status in 13 European countries’, American Sociological Review 79: 993–1014.
- Arai, A. B. (2000) ‘Self-employment as a response to the double day for women and men in Canada’, Canadian Review of Sociology/Revue Canadienne de Sociologie 37: 125–42.
- Bertogg, A., Nazio, T. and Strauss, S. (2020) ‘Work–family balance in the second half of life: caregivers’ decisions regarding retirement and working time reduction in Europe’, Social Policy & Administration, 55: 485–500.
- Blau, F. D. and Kahn, L. M. (2017) ‘The gender wage gap: extent, trends, and explanations’, Journal of Economic Literature 55: 789–865.
- Brenna, E. (2021) ‘Should I care for my mum or for my kid? sandwich generation and depression burden in Italy’, Health Policy 125: 415–23.
- Budig, M. J. (2006) ‘Intersections on the road to self-employment: gender, family and occupational class’, Social Forces 84: 2223–39.
- Carmichael, F. and Ercolani, M. G. (2016) ‘Unpaid caregiving and paid work over life-courses: different pathways, diverging outcomes’, Social Science & Medicine 156: 1–11.
- Conen, W. and Debets, M. (2019) ‘Precariousness and social risks among solo self-employed in Germany and The Netherlands’, in W. Conen and J. Schippers (eds.), Self-Employment as Precarious Work, Cheltenham: Edward Elgar Publishing, pp. 108–131.
- Cooklin, A. R., Westrupp, E. M., Strazdins, L., et al. (2016) ‘Fathers at work: work–family conflict, work–family enrichment and parenting in an Australian cohort’, Journal of Family Issues 37: 1611–35.
- Crystal, S., Shea, D. G. and Reyes, A. M. (2016) ‘Cumulative advantage, cumulative disadvantage, and evolving patterns of late-life inequality’, The Gerontologist, 57: 910–920.
- Damman, M., Henkens, K. and Kalmijn, M. (2013) ‘Late-career work disengagement: the role of proximity to retirement and career experiences’, Journal of Gerontology Series B 68: 455–63.
- De Boer, A., de Klerk, M., Verbeek-Oudijk, D., et al. (2020) Blijvende Bron van Zorg: Ontwikkelingen in het Geven van Informele Hulp 2014–2019, Den Haag: SCP.
- Ehrlich, U., Möhring, K. and Drobnič, S. (2019) ‘What comes after caring? The impact of family care on women’s employment’, Journal of Family Issues 41: 1387–419.
- Fast, J., Dosman, D., Lero, D., et al. (2013) The Intersection of Caregiving and Employment Across the Life Course, Edmonton, AB: University of Alberta.
- Fast, J., Keating, N., Eales, J., et al. (2020) ‘Trajectories of family care over the lifecourse: evidence from Canada’, Ageing and Society, 41: 1145–1162.
- Ferrín, M. (2021) ‘Self-employed women in Europe: lack of opportunity or forced by necessity?’, Work, Employment and Society, online first.
- Gomez-Leon, M., Evandrou, M., Falkingham, J., et al. (2019) ‘The dynamics of social care and employment in mid-life’, Ageing and Society 39: 381–408.
- Greenhaus, J. H. and Beutell, N. J. (1985) ‘Sources of conflict between work and family roles’, The Academy of Management Review 10: 76–88.
- Hamilton, M. G. and Adamson, E. (2013) ‘Bounded agency in young carers’ lifecourse-stage domains and transitions’, Journal of Youth Studies 16: 101–17.
- Hartog, J. and Salverda, W. (2018) ‘The labor market in The Netherlands, 2001–2016’, IZA World of Labor 418: 1–12.
- Henz, U. (2004) ‘The effects of informal care on paid-work participation in Great Britain: a lifecourse perspective’, Ageing and Society 24: 851–80.
- Henz, U. (2006) ‘Informal caregiving at working age: effects of job characteristics and family configuration’, Journal of Marriage and Family 68: 411–29.
- Hohmeyer, K. and Kopf, E. (2020) ‘Caught between two stools? informal care provision and employment among welfare recipients in Germany’, Ageing and Society 40: 162–87.
- Kaufman, G. and Uhlenberg, P. (2000) ‘The influence of parenthood on the work effort of married men and women’, Social Forces 78: 931–47.
- Keijer, M. G., Nagel, I. and Liefbroer, A. C. (2016) ‘Effects of parental cultural and economic status on adolescents’ life course preferences’, European Sociological Review 32: 607–18.
- Kjellsson, G., Clarke, P. and Gerdtham, U.-G. (2014) ‘Forgetting to remember or remembering to forget: a study of the recall period length in health care survey questions’, Journal of Health Economics 35: 34–46.
- Lilly, M. B., Laporte, A. and Coyte, P. C. (2007) ‘Labor market work and home care's unpaid caregivers: a systematic review of labor force participation rates, predictors of labor market withdrawal, and hours of work: labor market work and home care's unpaid caregivers’, Milbank Quarterly 85: 641–90.
- Lim, K. (2019) ‘Do American mothers use self-employment as a flexible work alternative?’, Review of Economics of the Household 17: 805–42.
- Looze, J. (2017) ‘Why Do (n't) they leave?: motherhood and women's job mobility’, Social Science Research 65: 47–59.
- Matysiak, A. and Mynarska, M. (2020) ‘Self-employment as a work-and-family reconciliation strategy? Evidence from Poland’, Advances in Life Course Research 45: 100329. https://www.sciencedirect.com/science/article/pii/S104026082030006X
- Minnotte, K. L. and Minnotte, M. C. (2021) ‘The ideal worker norm and workplace social support among US workers’, Sociological Focus 54: 120–37.
- Moen, P. (2001) ‘The gendered life course’, in G. Lk and R. H. Binstock (eds.), Handbook of Aging and the Social Sciences, Cambridge, MA: Academic Press, 179–196.
- Moen, P. and DePasquale, N. (2017) ‘Family care work: a policy-relevant research agenda’, International Journal of Care and Caring 1: 45–62.
- Mood, C. (2010) ‘Logistic regression: Why we cannot do what we think we can do, and what we can do about it’, European Sociological Review 26: 67–82.
- Moussa, M. M. (2019) ‘The relationship between elder care-giving and labour force participation in the context of policies addressing population ageing: a review of empirical studies published between 2006 and 2016’, Ageing and Society 39: 1281–310.
- OECD (2022) OECD Labour Force Statistics 2021.
- Patterson, S. E. and Margolis, R. (2019) ‘The demography of multigenerational caregiving: a critical aspect of the gendered life course’, Socius 5: 1–19.
- Pavalko, E. K. and Henderson, K. A. (2006) ‘Combining care work and paid work: do workplace policies make a difference?’, Research on Aging 28: 359–74.
- Pysklywec, A., Plante, M., Auger, C., et al. (2020) ‘The positive effects of caring for family carers of older adults: a scoping review’, International Journal of Care and Caring 4: 349–75.
- Raiber, K., Verbakel, E. and Visser, M. (2021) The impact of the COVID-19 lockdown on collecting informal caregiving data within the LISS panel in March 2020.
- Raiber, K., Verbakel, E. and Visser, M. (2022a) ‘Helping helpers? The role of monetary transfers in combining unpaid care and paid work’, International Journal of Care and Caring 6: 621–637.
- Raiber, K., Visser, M. and Verbakel, E. (2022b) ‘The wage penalty for informal caregivers from a life course perspective’, Advances in Life Course Research 53: 100490.
- Scherpenzeel, A. and Das, M. (2010) ‘True’ longitudinal and probability-based internet panels: evidence from The Netherlands’, in M. Das, P. Ester and L. Kaczmirek (eds.), Social and Behavioral Research and the Internet, Boca Raton: Taylor & Francis, pp. 77–103.
- Schmitz, H. and Westphal, M. (2017) ‘Informal care and long-term labor market outcomes’, Journal of Health Economics 56: 1–18.
- Smith, P. M., Cawley, C., Williams, A., et al. (2020) ‘Male/female differences in the impact of caring for elderly relatives on labor market attachment and hours of work: 1997–2015’, The Journals of Gerontology: Series B 75: 694–704.
- Statistics Netherlands (CBS) (2018) Women continue to postpone motherhood.
- Statistics Netherlands (CBS) (2019) Mijlpalen twintigers schuiven op.
- Van Houtven, C. H., Coe, N. B. and Skira, M. M. (2013) ‘The effect of informal care on work and wages’, Journal of Health Economics 32: 240–52.
- Verbakel, E. and CentErdata. (2021) LISS Panel – Retrospective Informal Care Career: Main Measurement, Tilburg and Nijmegen: DANS/KNAW.
- Vink, M. (2020) Who Brings Home the Bacon? How Gender Stereotypes Straitjacket Men and Women Into Traditional Relationships, Utrecht: University Utrecht.
- Wanberg, C. R., Kanfer, R., Hamann, D. J., et al. (2016) ‘Age and reemployment success after job loss: an integrative model and meta-analysis’, Psychological Bulletin 142: 400–426.
- Yu, W.-h. and Kuo, J. C.-L. (2017) ‘The motherhood wage penalty by work conditions: how do occupational characteristics hinder or empower mothers?’, American Sociological Review 82: 744–69.