
ABSTRACT
A blemish free, even-toned skin is universally associated with healthy skin. This reasoning makes people desire to have a flawless skin. Melanin is a naturally occurring pigment in humans. This pigment is responsible for skin, hair, and eye color, therefore determines our race and phenotypic appearance. On darker skin types, it is common that melanin production processes malfunctions. These malfunctions often lead to overproduction and secretion of melanin. As a result, unwanted pigmentary problems such melasma occur. Due to unknown etiology and its recurrence in nature, melasma is challenging to treat. The current available melasma treatment options often produce undesired side effects and suboptimum results. First-line topical treatments usually involve hydroquinone or topical steroids. Apart from the irritant reactions, this treatment mode is not suitable for all skin types. Skin care specialists are in search of an effective long-term cosmetics and cosmeceuticals to address hypermelanosis problems. Understanding of naturally occurring depigmenting agents provides an opportunity for more effective ways to manage melasma in all skin types. This review considers the benefits of naturally occurring ingredients which could help address skin pigmentation problems and broaden the choice for skin-lightening treatments.
Introduction
A blemish free, even skin tone is desirable by everybody. Flawless skin is considered a universal indication of beauty and healthy skin (Citation1). Melanin, a naturally occurring pigment in humans, is responsible for skin, hair, and eye color, therefore determines our race and phenotypic appearance (Citation2). It plays a vital protection role from cytotoxic ultraviolet (UV) radiation and oxidative stress (Citation3,Citation4). Melanin is produced from the melanosomes and transferred from melanocytes to keratinocytes (Citation2,Citation5,Citation6). Melanin production is controlled by the expression and activity of a copper containing enzyme, tyrosinase (Citation7). Tyrosinase is a vital enzyme involved in melanin synthesis. Tyrosinase regulates the catalytic processes of hydrolysis of tyrosine to l-DOPA as well as oxidation of DOPA to DOPA quinine (Citation2,Citation7–Citation9). When this process is malfunctioning, it often leads to overproduction of melanin. Over secretion of melanin causes unwanted skin problems such as post-inflammatory melanoderma, hyperpigmentation, and melasma (Citation4).
Melasma is a common, acquired hypermelanosis () of the face, which affects both sexes with a noticeable frequency in women (Citation10–Citation13). It is more common in people of darker skin phototypes due to high melanin content in these skin types (Citation14,Citation15). There seems to be an increased interest among people with skin of color requesting effective skin care treatments, this brings about great demand to investigate effective treatment modalities suitable for these skin types as the current literature is not sufficient. (Citation16–Citation20).
Table 1. Causes of acquired hypermelanosis (Citation41).
Melasma is characterized by light-to-dark brown symmetrical, homogeneous, irregular patches or macules (Citation21). Although its etiology is not clearly understood, sun exposure, hormones, pregnancy, use of phototoxic drugs, genetic influences, use of cosmetics, and anticonvulsant drugs are among the predisposing factors (Citation12,Citation13). Melasma is reported to have a significant negative impact on many women. Tremendous emotional stress and psychological distress are chronic emotions brought about by melasma (Citation22–Citation25).
According to statistical data, The American Academy of Dermatology estimates that melasma affects 5–6 million women in the United States (Citation26). Research shows that pigmentation disorders are the third (8, 8%) largest group of skin disorders in dermatology practices. In Brazil, pigmentary disorders are the second largest (11, 6%) complaint in women (Citation27). In South Africa, there is paucity of data in statistics. As a developing country with its diversity similar to America, the statistics may suggest similar patterns in South Africa.
Classification of melasma
Four clinical patterns () of hypermelanosis are cited in patients with melasma (Citation12,Citation28). These include, but are not limited to, a centrofacial, malar, and mandibular pattern. Melasma is not involved in the mucous membranes (Citation10,Citation26). Centrofacial is the most common pattern of melasma. This pattern involves the cheeks, forehead, upper lip, nose and chin. The malar pattern involves the cheeks and nose. The mandibular pattern involves lesions that occur over the ramus of the mandible.
Figure 1. Fitzpatrick skin phototype V with total face involvement melasma. (a) Female full face melasma involvement. (b) Male pattern melasma involving upper mentonian lesions, mandibular, zygomatic, temporal, and frontal (researchers’ collection).
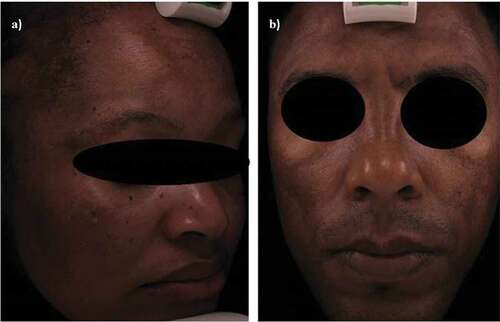
Studies conducted in Brazil on the incidence of topographies () concur that the facial area was the most affected; melasma was more noticeable on forehead, upper lip, zygoma, nose, chin, and parotid regions (Citation26,Citation28,Citation29). Other areas of the body such as forearms and neck may also be involved with melasma (Citation7).
Table 2. Frequency of facial features affected by melasma (adapted from Ref. (Citation29)).
Melasma is further classified according to the time it takes to resolve when treated. It is classified as either transient or persistent (Citation10,Citation30). Transient type is when melasma retracts within a year of termination of stimulus, e.g., post-pregnancy. Persistent melasma is seen when melasma persists more than a year after the stimulus has been removed (Citation12,Citation31).
Melasma is classified into four different histological types according to its depth in the skin (Citation10,Citation32). When melanin is distributed in the epidermis, it is illuminated more intense under the Wood’s lamp, a common tool for the diagnosis of melasma. This type is referred to as the epidermal type and is the most common. Dermal melasma is not as intense under Wood’s lamp and melanin is distributed in the dermis. In mixed type melasma, Wood’s lamp gives some interrupted intense illumination on some areas while others remain unchanged. On very dark individuals, Wood’s lamp cannot illuminate melasma due to the skin color acting as a competing chromophore. This type of melasma is classified as the intermediate melasma (Citation10,Citation30).
Histopathological studies have suggested a hyper functional effect on melanocytes (Citation32–Citation34). When compared to normal skin, the involved skin shows larger melanocytes which are extremely discolored with very noticeable dendrites and increased synthesis of eumelanin. Epidermal melanocytes were noticed to be filled with more mitochondria, Golgi apparatus, and rough endoplasmic reticulum. Ribosomes also reflected increased melanocytic activity (Citation34). Electronic microscopy studies revealed almost a similar finding to histology. Microscopically, there were more keratinocytes, melanocytes, and dendrites when compared to the uninvolved skin (Citation33).
South Africa is a country of multiple ethnicity and origin, covering a wide range of darker skin types (Citation35). Melasma is found more frequently and noticeable on Fitzpatrick skin types III–VI (darker skin phototypes) (Citation14,Citation15). Most intervention procedures (topical treatments, lasers and light, chemical peels) have been used but with undesired side effects and suboptimal results on darker skin types (Citation3,Citation16). The darker skin types tend to be sensitive to treatment interventions. Side effects like ochronosis when using hydroquinone (HQ), skin irritations to glycolic acid peels are common reported undesired effects. Darker skin types are more prone to post-inflammatory hyperpigmentation and have a greater chance of relapse (Citation14,Citation36,Citation37). Although medium depth peels, e.g., trichloroacetic acid, are recommended for management of melasma, they should be used with caution as there is a risk of developing hypertrophic scarring and unwanted permanent depigmentation (Citation17,Citation36,Citation37). Use of deep peels is completely prohibited as they are not suitable for darker skin types (Citation36,Citation37). Treatment interventions such as laser, although recommended in literature for melasma treatment, are not suitable for darker skin types (Citation14,Citation36–Citation38).
Diagnostic tools
Analysis of melasma is essential as it informs the treatment choice. There are few instruments that are used for melasma analysis. These include Wood’s lamp, dermoscopy, reflectance confocal microscopy, colimetry, mexametry, Melasma Area and Severity Index, and histology. Wood’s lamp examination is the most common melasma grading tool in which the skin is examined while exposed to the black light emitted by Wood’s lamp. This diagnostic tool was invented by a Caltimore physicist, Robert W. Wood, in 1903. Black light is invisible to the naked eye because it is in the UV spectrum with a wavelength just shorter than the color violet. The Wood’s lamp glows violet in a dark environment because it also emits some light in the violet part of the electromagnetic spectrum. A traditional Wood’s lamp is a low-output mercury arc covered by a Wood filter (barium silicate and 9% nickel oxide) and emits wavelength 320–450 nm (peak 365 nm). Wood’s lamp highlights the difference in pigmentation between affected and normally skin. Intensely seen pigmentation under this lamp responds better to topical treatment (Citation39,Citation40).
Treatment of melasma
Current modalities
Treatment of melasma is challenging to treat due to its recurrence nature. Current treatments of melasma include application of sunscreen, use of topical HQ alone or in combination with tretinoin, and or a corticosteroid (Citation7,Citation10,Citation13,Citation41). Superficial chemical peels and laser therapy are also common treatments (Citation21). HQ is considered the gold standard among the topical treatments of melasma; however, its use is associated with many undesirable side effects. Skin irritations, cytotoxicity, mutagenicity of melanocytes, contact dermatitis, and exogenous ochronosis in ethnic phototypes are amongst reported side effects (Citation42). Natural plant extracts have also been used in the treatment of melasma ().
Table 3. Studies evaluating the use of topical natural therapies as monotherapy versus other therapies used for treatment of Melasma.
Naturally occurring remedies for melasma treatment
The goal of treating melasma is to reduce hypermelanosis without causing hypopigmentation or irritation on the surrounding skin. There are many modalities available on the market; however, the side effects associated with them are significant. Naturally occurring depigmenting ingredients, e.g., kojic acid, vitamin C, soybean, licorice, arbutin, mequinol, niacinamide, glucosamine, aloesin, mulberry, hesperidin, ginseng, azelaic acid, umbelliferone (UMB), and grape seed, are presented in this study ().
Vitamin C (ascorbic acid)
Vitamin C is extracted from green leafy vegetables and citrus fruits. It is a water soluble vitamin with potent functions (Citation42). It has the ability to reduce dopaquinone to DOPA, therefore acting as an antioxidant found in large quantities in human skin (Citation3,Citation10,Citation43–Citation45). Vitamin C has an added benefit of photo protective effects by preventing absorption of both UVA and UVB harmful radiation as well as promotion of collagen synthesis (Citation46).
Literature provides evidence of the instability of vitamin C in the form of a solution. Many studies have concurred that it is quick to oxidize and decomposes in solution (Citation3,Citation45). Vitamin C obtained from fruits and vegetables has limited stability and permeability; this may result in unwanted skin irritations and allergy (Citation47). Ascorbate esters such as magnesium ascorbyl-2-phosphate are always added to any Vitamin C solution to stabilize it (Citation1,Citation3,Citation10,Citation45).
Recent literature demonstrates that the success of topical vitamin C is based on combination therapy. Vitamin C has been combined with iontophoresis (Citation43,Citation46,Citation48), with mesotherapy (Citation47), with laser Q-Switched ND:YAG laser (Citation49), or fractional Q-Switched Ruby Laser (Citation50). Due to its limited permeability being a charged molecule, combination therapies are aimed to assist vitamin C penetration ensuring better efficacy (Citation47). Clinical trials investigating efficacy of vitamin C with iontophoresis (Citation43) or comparing it with HQ (Citation51) have both revealed excellent results with minimal tolerable side effects ().
Solano et al. (Citation3) acknowledge vitamin C as an excellent antioxidant due to its ability to reduce back o-dopaquinone to dopa, thereby inhibiting melanin formation. Smit et al. (Citation6) suggest that vitamin C is a popular depigmenting agent currently used in most skin whitening formulations. Draelos (Citation1) echoes the same effects of vitamin C in the inhibition of melanin production, however contends that it is a poor lightening product when used alone; better results are achieved when combined with licorice extracts. Bandyopadhyay (Citation10) and Rendon and Gavira (Citation41) suggest that vitamin C is effective when used with MAP cream.
Kojic acid
Kojic acid is a naturally occurring hydrophilic fungus derivative, which acts as a tyrosinase inhibitor and an antioxidant (Citation52). It is best combined with corticosteroids to reduce irritation (Citation10,Citation41). It is commonly used in Asia and Japan with concentrations between 1% and 4%. Application of kojic acid creams is usually twice a day (Citation41,Citation53).
In recent studies, efficacy of topical kojic acid on melasma has been investigated by comparing it with HQ (Citation54), used as monotherapy comparing it with its separate different combinations (Citation52). On both studies, no side effects were observed and results suggested its action as a possible tyrosinase inhibitor. Results achieved on both studies suggested that kojic acid has limited efficacy when used as monotherapy, being a hydrophilic molecule, encounters greater resistance by the cutaneous barrier; however, combination therapies have resulted in significant skin-lightening effects ().
Soybean
Stimulation of collagen synthesis, protection against photodamage induced by UVB, antioxidant, anti-inflammatory, and moisturizing effects are among other properties of soybean (Citation55). Natural soybeans contain two serine protease inhibitors, Bowman–Birk inhibitor and the soybean trypsin. The two proteases act by interfering with the protease activated receptor 2 pathway (keratinocyte phagocytosis of melanosomes and melanosome transfer). The therapeutic effect of this process is the pigment lightening effect (Citation1,Citation41).
In an in vivo study (), Yucatan dark-skinned swine were treated with soybean and soya milk paste for a period of 9 weeks (Citation56). Histopathology of the sites treated showed that both soybean and soya milk reduced melanin deposits into the epidermis through phagocytosis of melanosomes, which resulted in reduced color; additionally, both soybean and soya milk extract demonstrated the ability to prevent sun-induced pigmentation (Citation56). It is interesting to note that these results were achieved without an additional vehicle to exert their depigmenting properties. This is an added advantage as the thick stratum corneum is the primary barrier to transdermal treatments (Citation57).
Licorice
Licorice extract has the ability to inhibit tyrosinase activity through its principal active compound glabridin which results in the suppression of melagonesis (Citation4). Liquiritin and isoliquirtin are other two popular active agents of licorice, both act as melanin disperser or removal of epidermal melanin (Citation58,Citation59).
In a clinical trial studies, topical liquiritin has been compared with a vehicle cream (Citation58), used as monotherapy on an efficacy study (Citation59,Citation60). The results of all three studies () proved licorice as safe, lightening agent with added anti-inflammatory benefits (Citation59). Nano technology demonstrated a possibility of loading large amounts of licorice for enhanced efficacy (Citation60).
Mequinol
Mequinol is used as an alternative to HQ due to fewer properties that lead to irritation of the skin. Mequinol is the formulation of 0.01% tretinoin and a penetration enhancer (Citation61). This is a scheduled concentration and, therefore, requires a prescription. Though its pathway is unclear, mequinol is thought to be a tyrosinase inhibitor (Citation62). Mequinol has been found to be effective in treating dyspigmentation, even on darker skin types, without causing any side effect (Citation1). A pilot study investigated the efficacy of topical 2% mequinol and 0.01% tretinoin for melasma on men (Citation62). The study demonstrated positive results as complete clearance was noted in 12 weeks with minimal tolerable side effects ().
Niacinamide
Niacinamide is the active form of vitamin B3 found in yeasts and root vegetables. It is an important precursor of nicotinamide adenine dinucleotide and nicotinamide adenine dinucleotide phosphate (Citation42). A recent clinical trial investigated topical niacinamide; the study results demonstrated its efficacy in both subjective and objective measures (Citation63). Additionally, side effects were mild and tolerable (). Other studies conducted both in in vitro and in humans have found niacinamide to have inhibitory mechanism on melanosome transfer to keratinocytes (Citation34,Citation64). Additionally to depigmenting effects, topical niacinamide has antiaging properties as it decreased collagen oxidation and improved ageing-induced sallowness (Citation65).
Glucosamine
Glucosamine is an amino-monosaccharide which is found in all human tissues. When an amino acid group is added to glucose, the result is the production of the sugar. The molecule product is then acetylated to N-acetyl glucosamine (Citation66). N-acetyl glucosamine has been found to have lightening effects on hypermelanosis due to its reduction of melanin in the melanocytes by prevention of tyrosinase glycosylation (Citation51,Citation66). A recent randomized clinical trial (Citation66) indicated that N-acetyl glucosamine combined with nicotinamide could be a good alternative to HQ when treating melasma. Results of this study demonstrated efficacy in both subjective and objective measures (). Subjects were instructed against direct sun exposure and daily use of sun protection factor, SPF 15. Combination of niacinamide and glucosamine has been found to have even better results compared to use of glucosamine alone (Citation67).
Arbutin
Arbutin is a HQ derivative found in cranberries, pears, wheat, and blueberries (Citation68). Its mechanism of action is based on inhibition of melanogenesis by binding tyrosinase without influencing the messenger RNA transcription of tyrosinase (Citation45). Its efficacy is dependent on its concentration; the higher the concentration, the better the results. In melasma management, arbutin has been used in combination with lasers (Citation69) as an ingredient in a hydrogel mask (Citation70) or combined with Ellagic acid (Citation71). In all these studies, there have been no undesirable side effects. In a randomized single-blind placebo study (Citation71), 1% topical arbutin brought about a significant response with no side effects.
In vitro studies have shown improvement in the appearance of hyperpigmentation, reduction in melanin content in melanocytes as well as reduction in tyrosinase activity; when compared to HQ, arbutin had demonstrated less toxic effects, making it a better choice (Citation53). Chawla et al. (Citation72) observed that tyrosinase hydroxylation and DOPA activity of tyrosinase inhibition effect are dose dependent. This effect may be due to the chemical structure of dA as de-oxysugars have the ability to increase skin penetration and binding affinity for tyrosinase (Citation3,Citation72).
Researchers endorse that α arbutin has an enhanced efficacy compared to arbutin itself and is less toxic when compared to HQ (Citation73,Citation74). Its action is achieved without affecting the mRNA expression enzymes. This has been demonstrated in cultured human melanoma cells. Its effects are further demonstrated by its effectiveness of inhibition of mushroom tyrosinase in vitro (Citation75,Citation76).
Aloesin
Aloesin is a compound which is derived from aloe extracts. In an in vitro study conducted by Jones et al. (Citation77), aloesin proved to have the ability of inhibiting melanin production from mushroom and murine sources. Choi et al. (Citation78) investigated aloesin pigmentary inhibition effects on UV-induced pigmentation on human skin. The study involved topical application of aloesin on the human forearm that has been exposed to UV radiation four times daily for 15 days. Aloesin was found to have suppressed pigmentation by 34%. This result suggested that aloesin could be used for hypermelanosis which is due to UV radiation. Melasma could also benefit as the literature has cited sun exposure to stimulate the formation of melasma. There is dearth of data regarding its efficacy on melasma.
Mulberry extract
Mulberry extract is a Morus alba L. derivative plant from Moraceae family. The root bark has been found to have skin depigmenting effects due to its inhibitory action of dopa oxidase activity of tyrosinase and its superoxide scavenging activity (Citation53). An in vitro investigative study looked at the effects of compounds found in dried mulberry leaves on melanin biosynthesis (Citation79). The result of this study was significant as cultured melan-a cells responded positively. It was discovered that dried mulberry leaves have an inhibitory effect on tyrosinase action and on melanin formation in melan-a cells (Citation79). A randomized clinical trial investigated 75% topical mulberry oil compared to a placebo in the treatment on melasma (Citation80). Results demonstrated that mulberry was a safe and effective lightening agent with added antioxidant benefits with mild side effects such as itching ().
Hesperidin
Hesperidin is a bioflavonoid which is fund mostly in peels and membranes of citrus fruits (Citation81); it known for its anti-inflammatory and antioxidant effects (Citation82). In vitro studies conducted have demonstrated good result when treating hypermelanosis due to its ability to inhibit melanin without causing cytotoxicity (Citation82,Citation83). A recent efficacy in vitro demonstrated hesperidin to decrease tyrosinase activity with added antioxidant and skin barrier strengthening effects (Citation84). Other benefits of hesperidin are antiaging; it protects against UVA-induced fibroblast damage as well as protection of collagen damage induced by oxidation (Citation85).
Ginseng
For thousands of years, ginseng has been traditionally used eastern Asia due to its versatility to treat various diseases such as hypertension, liver and kidney dysfunction, diabetes mellitus, and wound healing (Citation86). Red ginseng and white ginseng are the two traditional preparations of ginseng having a ginsenosides as the most important constituent of ginseng (Citation87). White ginseng comes from peeled, dried ginseng root while the red ginseng is produced by steaming fresh ginseng root and then drying it to acceptable moisture content, red ginseng is more potent than the white ginseng (Citation86). In vitro and observational studies investigated its melanogenic effect demonstrated that ginseng reduced melanin content, tyrosinase activity as well as perception of UVB-induced ROS (Citation21,Citation88,Citation89). Efficacy of oral ginseng has been investigated in a clinical study (Citation88). Both subjective and objective measurements showed significant improvement at completion of the study (). In the study, mild side effects were controlled as soon as ginseng was stopped.
Azelaic acid
Azelaic acid is a nine carbon, naturally occurring, nontoxic saturated non-phenolic dicarboxyl acid. Original use of azelaic acid was on the treatment of acne (Citation53). Due to effects on tyrosinase, it has been used to treat hypermelanosis of the skin (Citation90,Citation91). Azelaic acid works on the mitochondrial enzymes resulting in direct cytotoxic effect towards melanocytes; it also inhibits DNA synthesis. It also has an effect on reduction of free radicals production (Citation53). Studies done in Indo-Malay-Hispanic studies discovered that 20% concentration of azelaic acid is equivalent to those of 2% HQ (Citation90). Baliña and Graupe (Citation91) indicate a similar efficacy for 20% azelaic acid compared to 4% HQ, both in terms of lesion size reduction, pigmentary intensity, and overall response. Azelaic acid is well tolerated with minimal side effects such as a burning sensation, mild erythema, pruritis, cutaneous irritations, and scaling (Citation90,Citation91). There is dearth of data pertaining recent studies in azelaic acid on melasma; this topic requires more studies.
Umbelliferone
UMB is a phenolic compound of plant origin from the Apiaceae (Umbelliferae) family such as carrots and coriander (Citation92,Citation93). Due to its ability to absorb UV light in at several wavelengths (300, 305, 325 nm), this compound is mainly used in sun protection factors as the key ingredient (Citation92). Other effects include non-toxicity to the skin, antioxidant, and anti-inflammatory properties (Citation93). The use of this ingredient in melasma requires more research on its efficacy as there is paucity of data regarding its effectiveness.
Grape seed extract
Grape seed extract contain an antioxidant proanthocyanidin (Citation94). Oral intake of grape seed () extract for 6 months resulted in lightening effects of melasma (Citation94). There is however dearth of data regarding its efficacy on topical use.
Limitations of these treatments
Natural therapies have a potential to be used as alternative management for melasma; however, paucity of data regarding their efficacy and potential side effect profile needs to be addressed. More controlled clinical trials are lacking to determine their role. Only a few natural ingredients have been incorporated into topically applied cosmetics or cosmeceuticals often due to lack of parallel human studies (Citation10,Citation26,Citation41,Citation42).
Preventative measures
Although its etiology is not clearly understood, sun exposure, hormones, pregnancy, use of phototoxic drugs, genetic influences, use of cosmetics, and anticonvulsant drugs are cited among predisposing factors (Citation12,Citation13). UV radiation is cited as being the main cause of melasma as it induces the increase in melanogenic activity (Citation12,Citation32). Melasma has been found to reduce during cold winter months and worsens with hot summer climates. In intertropical regions, melasma incidence is observed to have an increased tendency (Citation95,Citation96).
Melasma is also thought to be induced by heat. Authors identified nighttime workers, who are exposed to heat of ovens, e.g., bakers, and professionals exposed to high intensity of light, e.g., dentists, experience great resistance when treating melasma. Worsening of the melasma is also reported as being worse after being exposed to their working condition (Citation97,Citation98).
All these studies suggest that safe sun practice is key to all individuals. If melasma is common among other family members, children should be taught about safety sun exposures. Being a female categorizes one as being at risk due to pregnancy hormones. Use of depigmenting cosmetics as preventative therapy would be proper when pregnant even before melasma starts to appear. Genetic predisposition has been noted in melasma studies (Citation26,Citation27). This reasoning suggests that whenever there is family history, members at risk should try and avoid melasma triggers.
Patient counseling
Melasma is not just a cosmetic concern but rather a medical concern due to its disfiguring nature. It has been associated with significant negative psychological and emotional effects. Decrease in social functioning, reduced productivity at work, and low self-esteem are reported side effects due to melasma (Citation7,Citation22). Tremendous emotional stress and psychological distress are chronic emotions brought about by melasma (Citation7,Citation22–Citation25). Grimes (Citation33) indicates that these symptoms lead to unnecessary stress, ailments, disorders, and often disease.
In Brazil, studies of quality of life on patients suffering from melasma have been conducted from all geographic regions. It was found that quality of life of these patients was affected by melasma which was related to emotional well-being, skin appearance, embarrassment, and frustration. In response to the Melasma Quality of Life Scale (MelasQol) questionnaire, it was observed that most of the time patients reported discomfort, expressed feelings of frustration, agreed to being embarrassed about their skin appearance. Patients further indicated that facial lesions caused great dissatisfaction, low self-esteem lower productivity at work or school as well as withdrawal from social life (Citation99,Citation100).
The findings of the studies of quality of life on patients suffering from melasma suggest that melasma is more than just a cosmetic concern. These MelasQol findings propose that melasma treatments should not be only clinical-based treatments but rather also addressed the psychological aspect as well.
Discussion and conclusion
New, effective, treatment products for melasma are in huge demand. Until melasma can be treated successfully, and its cause identified, researchers work tireless on this subject matter. Development of effective bleaching preparations for hyperpigmented lesions remains a challenge in the cosmetic industry (Citation2,Citation6). This brings about a necessity for development of effective treatment products with no or fewer side effects for management of melasma for all skin phototypes.
Although HQ has remained the gold standard in treating hypermelanosis of the skin, various naturally occurring alternatives are being investigated, due to their lack of side effects. Alternative melasma management is required for darker skin phototypes as these skin phototypes are intolerant to use HQ. Prolonged use of HQ leads to worse pigmentary changes. Besides temporal relief, use of HQ on darker skin types is not the best choice and should be avoided (Citation10,Citation13).
Plant extracts have a potential to relieve symptoms of skin discoloration with minimal tolerable side effects. This suggests that naturally occurring ingredients or plant extracts ingredients could be used successfully in treating melasma even on darker skin types without risk of aggravating the condition. There have been no detrimental side effects reported on long-term use of the naturally occurring ingredients reviewed.
Stability of the depigmenting product choice should play a vital role. Vitamin C from fruits and vegetables has to be stabilized for it to be effective. This should alert the patients to familiarize themselves with efficacy of ingredients listed on the packaging as only proper actives will have a desired effect of the treatment. Most depigmenting creams and solutions have Vitamin C in the list of their active ingredients. It is concerning which form of vitamin C is usually used as the packaging does not always state clearly.
Counseling of patients is of importance during the treatment. Treatment time is an important factor to consider when dealing with melasma cases. In the researcher’s experience in skin care practice, patients who suffer from melasma tend to be impatient and request rapid treatment intervention. Some ingredients such as liquiritin have proved to be effective in a short period of time (Citation58). Discontinuation of use of cosmetics which contain perfume is also another important factor that patients should be aware. Patient compliance is of utmost important for optimum results when treating melasma.
Lack of proper sun protection practices has remained a challenge. This challenge is notable especially on darker skin phototypes. They have a misconception that their skin does not get sun damage; hence, no sun tan is noticed on these skin types. It is imperative that during therapy, sun exposure is limited. Lack of sun protection practice reverses the result of the therapy. Photo protection should play an integral part in the skin care regimen of all individuals. Its importance should not be underestimated or overlooked. An American study analyzing data dating from 1992 National Health Interview survey regarding sun protection behaviors found that out of 1583 African-Americans, only minority respondents were aware of sun protection. The findings suggested that only 3 in 10 adults practiced sun protection, while in adolescents 69% were sunburnt while less than 40% practiced sun protection. Parents did not adequately protect their children from the sun and imitation tanning practices were found to be common among females and young adults (Citation101). Good sun protection habits are vital for a desired outcome to be achieved for all skin phototypes.
Current skin pigment analysis tools are not suitable for use on darker skin types. A universal melasma analysis tool, Wood’s lamp, cannot detect melasma on darker skin types. Due to high epidermal melanin content in darker skin types acting as a competing chromophore, it is challenging to contrast melasma from normal skin (Citation10,Citation30). This necessitates updated skin analysis tools which will enable analysis of all skin types.
Literature has demonstrated melasma to have negative impact on quality of life (Citation22–Citation25). It is significant that all studies looking at effectiveness of treating melasma should also consider measuring the difference on quality of life as well. Studies cited in this review reported the use of natural therapies in melasma management and the possibility that naturally occurring depigmenting ingredients offer potential to expand the choices for treating hypermelanosis and a better choice of effective antimelanogesis topical treatments when dealing with all skin phototypes inclusive of the darker skin phototypes as they get affected the most by melasma.
Disclosure statement
The authors indicate no potential conflict of interest.
Correction Statement
This article has been republished with minor changes. These changes do not impact the academic content of the article.
Additional information
Funding
References
- Draelos ZD. The combination of 2% 4-hydroxyanisole (mequinol) and 0.01% tretinoin effectively improves the appearance of solar lentigines in ethnic groups. J Cosmet Dermatol. 2006;5:239–44. doi:10.1111/j.1473-2165.2006.00260.x.
- Yao C, Oh J, Oh IG, Park C, Chung JH. [6]-Shagaol inhibits melanogenesis in B16 mouse melanoma cells through activation of the ERK pathway. Acta Pharmacological Sinica. 2013;34:289–94. doi:10.1038/aps.2012.134.
- Solano F, Bringati PM, Ghahem G. Hypopigmenting agents: an updated review on biological, chemical and clinical aspects. Pigment Cell Res. 2006;90:550–71. doi:10.1111/j.1600-0749.2006.00334.x.
- Fu B, Li H, Wang X, Lee FS, Cui S. Isolation and identification of flavonoids in licorice and a study of their inhibitory effect on tyrosinase. J Agric Food Chem. 2005;53:7408–744. doi:10.1021/jf051258h.
- Boissy RE. Melanosome transfer to and translocation in the keratinocytes. Exp Dermatol. 2003;12:5–12. doi:10.1034/j.1600-0625.12.s2.1.x.
- Smit N, Vicanova J, Pavel S. The hunt for natural skin whitening agents. Int J Mol Sci. 2009;10(12):5326–49. doi:10.3390/ijms10125326.
- Gupta AK, Gover MD, Nouri K, Taylor S. The treatment of melasma: a review of clinical trials. J Am Acad Dermatol. 2006;55:1048–65.
- Ortonne JP, Balloti R. Melanocytic biology and melanogenesis: what’s new? J Dermatol Treat. 2000;11:S15–16.
- Yaar M, Gilchrest BA. Melanocytic biology: before, during and after the Fitzpatrick era. J Invest Dermatol. 2004;122:xvii–xxix.
- Bandyopadhyay D. Topical treatment of melasma. Indian J Dermatol. 2009;54:303–09. doi:10.4103/0019-5154.57602.
- Vachiramon V, Suchonwanit P, Thadanipot K. Melasma in men. J Cosmet Dermatol. 2012;11:151–57. doi:10.1111/j.1473-2165.2012.00613.x.
- Sialy R, Hassan I, Kaur I, Dash RJ. Melasma in men: a hormonal profile. J Dermatol. 2000;27:64–65. doi:10.1111/j.1346-8138.2000.tb02122.x.
- Haddad AL, Matros LF, Brunstein F, Ferreira LM, Silva M, Costa D Jr. A clinical prospective, randomised, double-blind trial comparing skin whitening complex with HQ vs. placebo in the treatment of melasma. Int. J. Dermatol. 2003;42(2):153–56. doi:10.1046/j.1365-4362.2003.01621.x.
- Grimes PE. The safety and efficacy of salicylic acid chemic peels in darker racial-ethnic groups. Am Soc Dermatologic Surgery. 1999;25:18–22. doi:10.1046/j.1524-4725.1999.08145.x.
- Alam M, Pongprutthipan M. Body Rejuvenation. London: Springer Science+ Business; 2010. p. 239–43.
- Battle EF, Soden CE. The use of lasers in darker skin types. In Seminars in cutaneous medicine and surgery. 2009;28(2):130-140. Frontline Medical Communications.
- Grimes P. Aesthetics and cosmic surgery for darker skin types. USA: Lippincott Williams &Wilkins; 2008. p. 117-118, 49-51, 75-80.
- Edalatkhah H, Amani F, Rezaifar G. Prevalence of melasma in women in Ardebil city in 2002. Iran J Dermatol. 2004;7:72–77.
- El-Essawi D, Musial JL, Hammad A, Lim HW. A survey of skin disease and skin related issues in Arab Americans. J Am Acad Dermatol. 2007;56:933–38. doi:10.1016/j.jaad.2007.01.031.
- Werlinger KD, Guevara L, González CM, Edward TR, Caetano R, Haley RW, Pandya AG. Prevalence of self-diagnosed melasma among premenopausal Latino women in Dallas and Fort Worth, Tex. Arch Dermatol. 2007;143(3):423–31. doi:10.1001/archderm.143.3.424.
- Song M, Mun JH, Ko HC, Kim BS, Kim MB. Korean red ginseng powder in the treatment of melasma: an uncontrolled observational study. J Ginseng Res. 2011;35:170–75. doi:10.5142/jgr.2011.35.2.170.
- Balkrishnan R, McMichael AJ, Camacho FT. Development and validation of a health-related quality of life instrument for women with melasma. Br J Dermatol. 2003;149:572–77. doi:10.1046/j.1365-2133.2003.05419.x.
- Pawaskar M, Parikh P, Markowski T, Mcmichael AJ, Feldman SR, Balkrishnan R. Melasma and its impact on health-related quality of life in Hispanic women. J Dermatolog Treatment. 2007;18:5–9. doi:10.1080/09546630601028778.
- Cestari T, Hexsel D, Viegas M, Azulay M, Hassun K, Almeida ART, Rêgo VR, Mendes AM, Filho JW, Junqueira H. Validation of melasma quality of life questionnaire for Brazilian Portuguese language: the melasqol-bp study and improvement of qol of melasma patients after triple combination therapy. Br J Dermatol. 2007;156:13–20. doi:10.1111/j.1365-2133.2006.07591.x.
- Halder RM, Rodney IJ. Why are there so few effective treatments for pigmentary disorders of the skin? Expert Rev Dermatol. 2012;7(2):109–12. doi:10.1586/edm.12.9.
- Tamega Ade A, Miot LD, Bonfietti C, Gige TC, Marques ME, Miot HA. Clinical patterns and epidemiological characteristics of facial melasma in Brazilian women. J Eur Acad Dermatol Venereol. 2013;27:151–56. doi:10.1111/j.1468-3083.2011.04430.x.
- Ortone JP, Arellano I, Berneburg M, Cestari T, Chan H, Grimes P, Hexsel D, Im S, Lim J, Lui H, et al. A global survey of the role of ultraviolet radiation and hormonal influences in the development of melasma. J Eur Acad Dermatol Venereol. 2009;23:1254–62. doi:10.1111/j.1468-3083.2009.03295.x.
- Hexcel D, Lacerda DA, Cavalcante AS, Machado Fiho CA, Kalil CLPV, Ayres EL, Azulay-Abulafia L, Weber MB, Serra MS, Lopes NF, et al. Epidemiology of melasma in Brazilian patents: a multicenter study. Int J Dermatol. 2013;53:440–44. doi:10.1111/j.1365-4632.2012.05748.x.
- Handel AC, Lima PB, Tonolli VM, Miot LDB, Miot HA. Risk factors for facial melasma in women: a case-control study. Br J Dermatol. 2014;171:588–94. doi:10.1111/bjd.2014.171.issue-3.
- Hann SK, Im S, Chung WS, Kim Do Y. Pigmentary disorders in the South East. Dermatol Clin. 2007;25:431–38. doi:10.1016/j.det.2007.04.002.
- Ni Z, Mu Y, Gulati O. Treatment of melasma with Pycnogenol. Phytother Res. 2002;16:567–71. doi:10.1002/ptr.1085.
- Kang WH, Yoon KH, Lee ES, Kim J, Lee KB, Yim H, Sohn S, Im S. Melasma: histopathological characteristics in 56 Korean patients. Br J Dermatol. 2002;146(2):228–37. doi:10.1046/j.0007-0963.2001.04556.x.
- Grimes P, Yamada N, Bhawan J. Light microscopic, immunohistochemical, and ultrastructural alterations in patients with melasma. Am J Dermatopathol. 2005;27:96–101. doi:10.1097/01.dad.0000154419.18653.2e.
- Tse TW, Hui E. Tranexamic acid: an important adjuvant in the treatment of melasma. J Cosmet Dermatol. 2013;12:57–66. doi:10.1111/jocd.2013.12.issue-1.
- SA statistical Release P0 302 mid- year population estimates [online] Available at: https://www.statssa.gov.za/publications/P0302/P03022016.pdf [ Accessed 21 September 2017].
- Shankar K, Godse K, Aurangabadkar S, Lahiri K, Mysore V, Ganjoo A, Vedamurty M, Kohli M, Sharad J, Kadhe G, et al. Evidence-based treatment for melasma: expert opinion and a review. Dermatol Ther December. 2014;4(2):165–86. doi:10.1007/s13555-014-0064-z.
- Talakoub L. Wesley NO. Differences in perceptions of beauty and cosmetic procedures performed in ethnic patients. In Seminars in cutaneous medicine and surgery. 2009;28(2):115-129. Frontline Medical Communications.
- Grimes. P. Aesthetics and cosmic surgery for darker skin types. USA: Lippincott Williams &Wilkins; 2008. p. 117–118, 49–51, 75–80.
- Goh CL, Dlova CN. A retrospective study on the clinical presentation and treatment outcome of melasma in a tertiary dermatological referral centre in Singapore. Singapore Med J. 1999;40:455–58.
- Ponzio HA, Cruz M. Acurácia do exame sob a lâmpada de Wood na classificação dos cloasmas. An Bras Dermatol. 1993;68:325–28.
- Rendon MI, Gaviria JI. Review of skin- lightening agents. Am Soc Dermatologic Surgery. 2005;31:886–89. doi:10.1111/j.1524-4725.2005.31736.
- Zhu W, Gao J. The use of botanical extracts as topical skin-lightening agents for the improvement of skin pigmentation disorders. J Investigative Dermatol Symp Proc. 2008;13:20–21. doi:10.1038/jidsymp.2008.8.
- Huh CH, Seo KI, Park YJ, Lim JG, Eun HC, Park KC. A randomized, double-blind, placebo-controlled trial of vitamin C iontophoresis in melasma. Dermatology, 2003;206(4):316–320.
- Katsube T, Imawaka N, Kawano Y, Yamazakib Y, Shiwakuc K, Yamane Y. Antioxidant flavonol glycosides in mulberry (Morus alba L) leaves isolated based on LDL antioxidant activity. Food Chem. 2006;97:25–3. doi:10.1016/j.foodchem.2005.03.019.
- Ebanks JP, Wickett RR, Raymond EB. Mechanisms regulating skin pigmentation: the rise and fall of complexion coloration. Int J Mol. 2009;10:4066–87. doi:10.3390/ijms10094066.
- Taylor MB, Yanaki JS, Draper DO, Shurtz JC, Coglianese M. Successful short-term and long-term treatment of melasma and postinflammatory hyperpigmentation using vitamin C with a full-face iontophoresis mask and a mandelic/malic acid skin care regimen. J Drugs in Dermatol. 2013;12(1):45–50.
- Balevi A, Ustuner P, Özdemir M. Salicylic acid peeling combined with vitamin C mesotherapy versus salicylic acid peeling alone in the treatment of mixed type melasma: A comparative study. Journal of Cosmetic and Laser Therapy.2017;19 (5):294–299.
- Lee GSK. Intravenous vitamin C in the treatment of post-laser hyperpigmentation for melasma: a short report. J Cosmet Laser Ther. 2008;10:234–36. doi:10.1080/14764170802187193.
- Lee MC, Chang SC, Huang YL, Chang SL, Chang CH, Lin YF, Hu S. Treatment of melasma with mixed parameters of 1,064-nm Q-switched Nd: YAG laser toning and an enhanced effect of ultrasonic application of vitamin C: a split-face study. Lasers Med Sci. 2015;301:159–63. doi:10.1007/s10103-014-1608-2.
- Zhou HL, Hu B, Zhang C. Efficacy of 694-nm fractional Q-switched ruby laser (QSRL) combined with sonophoresis on levorotatory vitamin C for treatment of melasma in Chinese patients. Lasers Med Sci. 2016;315:991–95. doi:10.1007/s10103-016-1938-3.
- Espinal-Perez LE, Moncada B, Castanedo-Cazares JP. A double-blind randomised trial of 5% ascorbic acid vs. 4% hydroquione in melasma. Int J Dermatol. 2004;43:604–07. doi:10.1111/j.1365-4632.2004.02134.x.
- Deo SK, Dash KN, Sharma YK, Virmani NC, Oberai C. Kojic acid vis-a-vis its combinations with hydroquinone and betamethasone valerate in melasma: a randomized, single blind, comparative study of efficacy and safety. Indian J Dermatol. 2013;58(4):281. doi:10.4103/0019-5154.113940.
- Halder RM, Richards GM. Management of dyschromias in ethnic skin. Dermatol Ther. 2004;17:151–57. doi:10.1111/dth.2004.17.issue-2.
- Monteiro RC, Kishore BN, Bhat RM, Sukumar D, Martis J, Ganesh HK. A comparative study of the efficacy of 4% hydroquinone vs 0.75% Kojic acid cream in the treatment of facial melasma. Indian J Dermatol. 2013;58:2:157. doi:10.4103/0019-5154.108070.
- Leyden JJ, Shergill B, Micali G, Downie J, Wallo W. Natural options for the management of hyperpigmentation. J Eur Acad Dermatol Venereol. 2011;25:1140–45. doi:10.1111/j.1468-3083.2011.04130.x.
- Paine C, Sharlow E, Liebel F, Eisinger M, Shapiro S, Seiberg M. An alternative approach to depigmentation by soybean extracts via inhibition of the PAR-2 pathway. I Invest Dermatol. 2001;116:587–95. doi:10.1046/j.1523-1747.2001.01291.x.
- Hakozaki T, Minwalla L, Zhuang J, Chhoa M, Matsubara A, Miyamoto K, Greatens A, Hillebrand GG, Bissett DL, Boissy RE. The effects of niacinamide on reducing cutaneous pigmentation and suppression of melanosome transfer. Br J Dermatol. 2002;147:20–31. doi:10.1046/j.1365-2133.2002.04834.x.
- Amer M, Metwalli M. Topical liquiritin improves melasma. Int J Dermatol. 2000;39:299–301. doi:10.1046/j.1365-4362.2000.00943.x.
- Toosi P, Esmaili AM, Saeedi M. Evaluation of licorice efficacy on melasma. Iran J Dermatol. 2013;16, 3 ( 65):118–119.
- Shamsi Meymandi S, Mohammadzadeh Shanehsaz S, Ansari Dogaheh M. Efficacy of licorice extract in the treatment of melasma: a randomized, double-blind, placebo-controlled clinical trial. J Dermatol Cosmet. 2016;7(1):1–9.
- Davis EC, Callender V. Post inflammatory hyperpigmentation, a review of the epidemiology, clinical features and treatment options in kin of color. J Clin Aesthet Dermtol. 2010;3(7):20–31.
- Keeling J, Cardona L, Benitez A, Epstein R, Rendon M. Mequinol 2%/tretinoin 0.01% topical solution for treatment of melasma in men: a case series and review of the literature. Cutis. 2008;81:179–83.
- Navarrete-Solís J, Castanedo-Cázares JP, Torres-Álvarez B, Oros-Ovalle C, Fuentes-Ahumada C, González FJ, Martínez-Ramírez JD, Moncada B. A double-blind, randomized clinical trial of niacinamide 4% versus hydroquinone 4% in the treatment of melasma. Dermatology research and practice, vol. 2011, Article ID 379173, 5 pages, 2011.
- Minwalla L1, Zhao Y, Cornelius J, Babcock GF, Wickett RR, Le PIC, Boissy RE. Inhibition of melanosome transfer from melanocytes to keratinocytes by lectins and neoglycoproteins in an in vitro model system. Pigment Cell Res. 2001;14(3):185–94.
- Bissett DL, Miyamoto K, Sun P, Li J, Berge CA. Topical niacinamide reduces yellowing, wrinkling, red blotchiness and hyperpigmented spots in aging facial skin. Int J Cosmet Sci. 2004;26:231–38.
- Iraji F, Mehrpour K, Asilian A, Siadat AH, Mohaghegh F. A Comparituve study to evaluate the efficacy of 4% N-acetyl glucosamine + 2% nicotinamide cream versus 4% hydroquinone cream in the treatment of facial melasma: a randomized, double-blind, split face clinical trial. J Tissue Res. 2009;9(1):1767.
- Kimball AB, Kaczvinsky JR, Li J, Robinson LR, Matts PJ, Berge CA, Miyamoto K, Bissett DL. Reduction in the appearance of hyperpigmentation after use of moisturisers with a combination of topical niacinamide and N-acetyl glucosamine: results of a randomised, double blind, vehicle controlled trial. Br J Dermatol. 2010;162:435–41.
- Baliña LM, Graupe K. The treatment of melasma 20% azelaic acid versus 4% HQ cream. Int J Dermatol. 1991;30(12):893–95.
- Polnikorn N. Treatment of refractory melasma with the MedLite C6 Q-switched Nd: YAG laser and alpha arbutin: a prospective study. J Cosmet Laser Ther. 2010;12(3):126–31.
- Han TY, Son IP, Jang WS, Chang HS, Kim JH, Sim YH, Kim DH, Kim BJ, Kim MN, Lee HK, et al. Efficacy of hydrogel mask with 2% arbutin for melasma. Korean J Dermatol. 2011;49(3):210–16.
- Ertam I, Mutlu B, Unal I, Alper S, KivCAk B, Ozer O. Efficiency of ellagic acid and arbutin in melasma: a randomized, prospective, open‐label study. J Dermatol. 2008;35(9):570–74.
- Chawla S, DeLong MA, Visscher MO, Wickett RR, Manga P, Boissy RE. Mechanism of tyrosinase inhibition by deoxyArbutin and its second-generation derivatives. Br J Dermatol. 2008;159(6):1267–74.
- Picardo M, Carrera M. New and experimental treatments of cloasma and other hypermelanoses. Elsevier. 2007;25(3):353–62.
- Hamed SH, Sriwiriyanont P, deLong MA, Visscher MO, Wickett RR, Bossy RE. Comparative efficacy and safety of deoxyarbutin, a new tyrosinase-inhibiting agent. J Cosmet Sci. 2006;57:291–308.
- Sugimoto K, Nishimura T, Nomura K, Sugimoto K, Kuriki T. Inhibitory effects of alpha-arbutin on melanin synthesis in cultured human melanoma cells and a three-dimensional human skin model. Biol Pharm Bull. 2004;27:510–14.
- Boissy RE, Visscher M, DeLong MA. Deoxyarbutin: a novel reversible tyrosinase inhibitor with effective in vivo skin lightening potency. Exp Dermatol. 2005;14:601.
- Jones K, Hughes J, Hong M, Jia Q, Orndorff S. Modulation of melanogenesis by aloesin: a competitive inhibitor of tyrosinase. Pigment Cell Res. 2002;15:335–40.
- Choi S, Park AI, Lee SK, Kim JE, Chung MH. Aloesin inhibits hyperpigmentation induced by UV radiation. Clin Exp Dermatol. 2002;27:513–15.
- Lee SH, Choi SY, Kim H, Hwang JS, Lee BG, Gao JJ, Kim SY. Mulberroside F isolated from the leaves of morus alba inhibits melanin biosynthesis. Biol Pharm Bull. 2002;25:1045–48.
- Alvin G, Catambay N, Vergara A, Jamora MJ. A comparative study of the safety and efficacy of 75% mulberry (Morus alba) extract oil versus placebo as a topical treatment for melasma: a randomized, single-blind, placebo-controlled trial. J Drugs in Dermatol. 2011;10(9):1025–31.
- Barbulova A, Colucci G, Apone F. New trends in cosmetics: by-products of plant origin and their potential use as cosmetic active ingredients. Cosmetics. 2015;2:82–92.
- Kim SS, Kim MJ, Choi YH, Kim BK, Kim KS, Park KJ, Park SM, Lee NH, Hyun GG. Down-regulation of tyrosinase, TRP-1, TRP-2 and MITF expressions by citrus press-cakes in murine B16 F10 melanoma. Asian Pac. J. Trop. Biomed. 2013;3:617–22.
- Kim B, Lee YJ, Lee HY, Nam KY, Park J, Lee SM, Kim JE, Lee JD, Hwang JS. Hesperidin suppresses melanosome transport by blocking the interaction of Rab27A-melanophilin. Biomol. Ther. Seoul. 2013;21:343–48.
- Lee HJ, Lee WJ, Chang SE, Lee GY. Hesperidin, a popular antioxidant inhibits melanogenesis via Erk1/2 mediated MITF degradation. Int J Mol Sci. 2015;16(8):18384–95.
- Proteggente AR, Basu-Modak S, Kuhnle G, Gordon MJ, Youdim K, Tyrrel R, Rice-Evans CA. Hesperetin glucuronide, a photoprotective agent arising from flavonoid metabolism in human skin fibroblast. Photochem Photobiol. 2003;78:256–61.
- Kimura Y, Simuyoshi M, Sakanaka M. Effects of ginsenosides Rb1 on skin changes. J Biomed Biotehnol. 2012;2012:94624.
- Kim K. Effects of ginseng and ginsenosides on melanogenesis and their mechanism of action. J Ginseng Res. 2015;39(1):1–6.
- Lee Y, Kim KT, Kim SS, Hur J, Ha SK, Cho CW, Choi SY. Inhibitory effects of ginseng seed on melanin biosynthesis. Pharmacogn Mag. 2014;10(Suppl. 2):S272e5.
- Hwang EY, Kong YH, Lee YC, Kim YC, Yoo KM, Jo YO, Choi SY. Comparison of phenolic compounds contents between white and red ginseng and their inhibitory effect on melanin biosynthesis. J Ginseng Res. 2006;30:82e7.
- Garcia-Lopez, M. Double-blind comparison of azelaic acid and hydroquinone in the treatment of melasma. Acta Derm Venereol (Stockh), 1989;143:58–61.
- Baliña LM, Graupe K. The treatment of melasma 20% azelaic acid versus 4% hydroquinone cream. Int J Dermatol. 1991;30(12):893–95.
- Mazimba O. Umbelliferone: Sources, chemistry and bioactivities review. Bulletin of Faculty of Pharmacy, Cairo University. 2017;55(2):223–232.
- Ashraf Z, Rafiq M, Seo SY, Babar MM, Zaidi NUSS. Design, synthesis and bioevaluation of novel umbelliferone analogues as potential mushroom tyrosinase inhibitors. J Enzyme Inhib Med Chem. 2015;30(6):874–83.
- Yamakoshi J, Sano A, Tokutake S, Saito M, Kikuchi M, Kubota Y, Kawachi Y, Otsuka F. Oral intake of proanthocyanidin-rich extract from grape seeds improves chloasma. Phytother Res. 2004;18:895–99.
- Victor F, Gelber J, Rao B. Melasma: a Review. J Cutaneous Med Surgery: inc Med Surg Dermatol. 2004;2:94–102.
- Katsambas A, Antoniou CH. Melasma. Classification and treatment. J Eur Acad Dermatol Venereol. 1995;4:217–23.
- Mahmoud BH, Ruvolo E, Hexsel CL, Liu Y, Owen MR, Kollias N, Lim HW, Hamzavi IH. Impact of long-wavelength UVA and visible light on melanocompetent skin. J Invest Dermatol. 2010;130:2092–97.
- Mahmoud BH, Hexsel CL, Hamzavi IH, Lim WH. Review, effects of visible light on the skin. Photochem Photobiol. 2008;84:450–62.
- Purim KS, Avelar MF. [Photoprotection, melasma and quality of life in pregnant women]. Rev Bras Ginecol Obstet. 2012;34:228–34.
- Costa MC, Eljaiek HV, Abraham LS, Azulay-Abulafia L, Ardigo M. In vivo reflectance confocal microscopy in a typical case of melasma. An Bras Dermatol. 2012;87:782–84. doi:10.1590/S0365-05962012000500021.
- Buller DB, Cokkinides V, Hall HI, Hartman AM, Saraiya M, Miller E, Paddock L, Glanz K. Prevalence of sunburn, sun protection, and indoor tanning behaviors among Americans: review from national surveys and case studies of 3 states. J Am Acad Dermatol. 2011;65(5):S114–e1. doi:10.1016/j.jaad.2011.05.033.