
Abstract
Aim: This ecological study was carried out to determine the cyclic trends in the rate of perinatal and infant mortality and among children aged under 15 years who died in traffic accidents or from drowning, respiratory disease or cancer.
Methods: Monthly data on the numbers of live births, perinatal and infant deaths, and deaths from respiratory disease, cancer, traffic accidents, accidental drowning, and submersion in children aged under 15 years were obtained from the Hungarian nationwide population register. The data were aggregated over the study period and cyclic trends were investigated using the Walter–Elwood and negative binomial regression methods.
Results: Significant double-peak (May and November) trends were found in mortality rates for perinatal and infant deaths, respectively. Additionally, significant (p-value < .001) seasonal variation in monthly mortality rates for deaths from respiratory diseases was observed with a peak in February, and a significant single peak was observed in mortality rates in July in both deaths from traffic accidents and drowning among children aged 0–14 years. However, there was no seasonal variation in monthly mortality rates for deaths from childhood cancer.
Conclusions: Since cyclic trends in mortality suggest some effect of environmental factors in etiology, we might speculate that perinatal mortality may have been related to respiratory infections. A significant single peak was observed in mortality rates in July in both deaths from traffic accidents and drowning among children aged 0–14 years which could be related to environmental factors, such as temperature, air masses, and fronts. However, there was no seasonal variation in monthly mortality rates for deaths from childhood cancer. All of these novel findings could prove useful in preventive strategies, but further cohort studies are needed to investigate this hypothesis.
Seasonality in infant mortality is known.
What is known
A significant cyclic trend was found in infants’ mortality, with a peak in deaths in winter during the post-perinatal period and double peaks in May and November during the perinatal period, which might be associated with respiratory syncytial virus infections.
Winter-peak cyclic trends were observed in both preterm and low birthweight mortality.
A significant cyclic trend was observed in mortality, with a peak in deaths from traffic accidents and drowning in July for children aged 0–14 years, but seasonal variation was not found in monthly deaths from childhood cancer.
What is new
Introduction
The most significant differences in mortality are age-related. The chance of death is relatively high for a newborn baby at the beginning of the human lifespan. Then, mortality rates decrease and reach a minimum around the ages of 10–20 years. The most frequent numbers of deaths occur in infants aged under 1 year. Then, road traffic injuries are the leading cause of death among children aged 0–14 years, causing 34% of childhood (0–14 years) injury deaths annually [Citation1].
Accidental drowning is a significant problem worldwide, particularly for children under the age of 15 years [Citation2,Citation3], and a considerable number of children aged between 0 and 14 years die from cancer or from respiratory diseases [Citation4].
The seasonality of a disease suggests some effect of environmental factors in etiology (e.g. infections). The present ecological study was carried out to determine both the annual and the cyclic trends in the mortality rate for the most frequent causes of death in Hungary during the 20-year interval between 1 January 1995 and 31 December 2014.
Materials and methods
Study population
The 20-year period between 1995 and 2014 was considered in this analysis. The data on cause of death were classified according to the 10th revision of the International Classification of Diseases (ICD10) codes. Monthly data on the numbers of live births, stillbirths, early neonatal deaths, infant deaths (including those tied to certain conditions originating in the perinatal period; ICD10: P00 − P96) as well as infant congenital malformations, deformations and chromosomal abnormalities (ICD10: Q00–Q99), deaths from cancers (ICD10: C00 − D48), deaths from respiratory diseases (ICD10: J00–J99), and deaths from external causes (ICD10: V01 − Y89) aged under 15 years were obtained from the nationwide population register maintained by the Hungarian Central Statistical Office [Citation5].
Monthly birth and infant death data were available with birth weight and gestational age. Preterm birth based on less than 37 completed weeks of gestation and a birth weight of less than 2500 g was regarded as a low birth weight. The age of the infant death was categorized for neonatal (0–27 days) and postneonatal (28–364 days) mortality according to World Health Organization (Geneva) recommendations [Citation6].
The perinatal mortality rate was calculated as the sum of the numbers of stillbirths (a baby born dead after the 24th week of gestation) and early neonatal deaths (the death of a live-born baby within 7 days of birth) during a year divided by the total number of births (the sum of the numbers of live births plus stillbirths in the same year), expressed per 1000 births per year.
Additionally, monthly numbers of infant deaths from congenital malformations were available. Monthly infant mortality rates were calculated as the numbers of infant deaths divided by the numbers of births in the same month of the year.
Monthly mortality rates for childhood cancer and deaths from respiratory diseases were calculated as the number of deaths divided by the population in the same month of the year. Additionally, analyses were carried out on mortality rates for deaths in traffic accidents (ICD10: V01 − V19) and from accidental drowning and submersion (W65 − W74). Monthly mortality rates for childhood traffic accidents and drowning were also allocated as the number of deaths divided by the population in the same month of the year. Since monthly data on the childhood population aged 0–14 years were not available, we extrapolated from the monthly numbers of deaths and births to estimate the monthly population of children in this age group.
Statistical methods
Data on the month of death were aggregated over the study period and cyclic trends were investigated using the Walter–Elwood and the negative binomial regression methods [Citation7,Citation8]. Both methods adjust for the population at risk by grouping the data into months and were used to investigate single or double peaks of seasonality. We used the Walter–Elwood method to analyses double-peak seasonality using six sectors based on the assumption that the observed events occur 6 months apart and the events are repeating regularly every 6 months. Thus, the monthly data are aggregated using the months from the first half of the year and adding the corresponding data from the second half of the year (e.g. January and July). However, the negative binomial regression method was carried out in multiple variable analyses since this method allows for adjustment of confounding for the study of seasonal patterns [Citation8]. Rate ratios (RR) together with their corresponding 95% confidence intervals (95% CI) were computed. Trends in the annual number of deaths by cause of death were also investigated using negative binomial regression. All analyses were performed using R statistical software version R-3.4.0 for Windows (cran.r-project.org).
Results
Overall, 20,042 deaths were registered during the study period among children aged 0–14 years, of which 13,804 (68.9%) were infant deaths, 1319 (6.9%) were childhood cancer deaths, 667 (4.0%) were deaths from respiratory diseases, and 2330 (11.6%) were deaths from external causes (including 601 deaths in road accidents and 256 deaths from drowning). In addition, 4217 deaths from congenital malformation were registered during the 20-year period ().
Table 1. The aggregate monthly numbers of deaths by cause of death in Hungary between 1995 and 2014.
Perinatal and postneonatal infant mortality
During the 20-year interval, there were 1,930,273 live births, 8224 perinatal deaths (including 6550 neonatal deaths and 1674 stillbirths), and 13,804 infant deaths. The numbers of infant deaths were 9173 (66%) and 4631 (34%) during the neonatal and postneonatal period, respectively. Approximately 30% (4217/13,804) of infant deaths were due to congenital malformations. There were 160,112 (8.3%) and 12,160 (88%) preterm birth in live-born babies and infant deaths, respectively. The numbers of the low birth weight were 162,754 (8.4%) and 11,906 (86%) in live births and infant deaths, respectively. Thus, significantly (p < .001) higher proportions of the preterm births and low birth weights were observed in infant deaths compared to live-born babies.
The annual perinatal mortality rate declined from a maximum of 6.2 per 1000 births in 1995 to a minimum of 2.6 per 1000 births in 2014, and there was a significant RR trend per annum of 0.953 (95% CI [0.949–0.957]; p < .001). A similar decreasing trend was detected for the annual rate of infant mortality with an annual RR of 0.965 (95% CI [0.961 − 0.969]; p < .001).
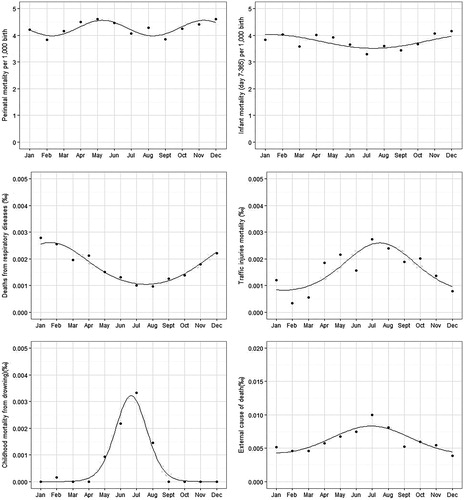
A double-peak model was fitted to characterize the seasonal variation of perinatal mortality using both the Walter–Elwood and negative binomial regression methods (). The peaks were observed in May and November (p < .001) (). Similar, significant (p < .001) double peak seasonal trends were detected in all infant mortality, infant mortality during neonatal and postneonatal period, and in preterm and low birth weight babies. After adjusting these factors to the seasonality in multiple negative binomial regression models, the single peak seasonal effect remained significant (p < .05) with a peak in December. Although 30% of infant deaths were due to congenital malformations, no cyclic trend was found in the mortality rates in for deaths from congenital malformations.
Figure 1. Seasonal variation in monthly numbers of perinatal deaths (a) and post-perinatal infant deaths (b) as well as deaths from respiratory diseases (c), in traffic accidents (d), and from drowning (e) in children aged 0–14 years.
Trends in childhood mortality
Annual childhood (aged 0–14 years) mortality declined from a maximum of 1706 deaths in 1995 to a minimum of 332 deaths in 2012 (RR: 0.959, 95% CI [0.957–0.962]; p < .001).
Similarly, a significant decreasing trend was found in mortality rates from deaths due to external causes (RR: 0.944, 95% CI [0.937–0.951]; p < .001), traffic accidents (RR: 0.939, 95% CI [0.926–0.951]; p < .001), and drowning (RR: 0.941, 95% CI [0.922–0.961]; p < .001). Likewise, a significant decline was observed in mortality rates from childhood cancer (RR: 0.970, 95% CI [0.961–0.979]; p < .001) and from respiratory diseases (RR: 0.908, 95% CI [0.898–0.919]; p < .001).
The aggregate monthly numbers of deaths by cause of death in Hungary between 1995 and 2014 are summarized in . There was no cyclic trend in mortality from all causes of death among children aged under 15 years or in monthly mortality rates for deaths from childhood cancer. However, there was significant (p-value < .001) seasonal variation in monthly mortality rates for deaths from respiratory diseases with a peak in February (). In addition, a significant (p-value: .002) single peak was observed in mortality rates in July in both deaths from road accidents and drowning ().
We studied whether the seasonal pattern in mortality for traffic accidents and drowning was better described by a cosine function with a period of 6 months, but no significant double-peak seasonality was found.
In addition, both the Walter–Elwood method and the negative binomial regression method produced similar results for the single variable analyses of seasonality.
Discussion
Main findings
The annual infant and childhood mortality rates have decreased in Hungary during the past two decades, both overall and by cause of death. Significant double-peak trends (May and November) were found in mortality rates for perinatal, neonatal and postneonatal infant deaths, respectively. Similar cyclic trends were detected in preterm and low birth weight babies. However, the pattern of seasonal effect is modified after adjusting these factors to the seasonality in multiple negative binomial regression models, where a significant single peak seasonal effect with a maximum in December was observed.
A winter peak cyclical trend was found in mortality rates for respiratory diseases. In addition, a significant single peak was observed in mortality rates in July in both deaths from traffic accidents and drowning among children aged 0–14 years. However, there was no seasonal variation in monthly mortality rates for deaths from childhood cancer, suggesting that environmental factors play a less important role in the etiology of childhood cancer mortality.
Comparisons with other studies
Many developed countries have experienced a decrease in the perinatal mortality rate [Citation9,Citation10]. The level of perinatal mortality is an important indicator of the quality of obstetric and paediatric care in a country. We found a significant declining trend in perinatal mortality during the 20-year interval. However, the perinatal mortality rate has been higher in Hungary than in all the countries in the European Union prior to the 2004 enlargement [Citation11,Citation12].
In our study, significant double-peak seasonality was also noted in perinatal mortality in Hungary in May and November, months which mark the end of spring and autumn in the continental climate, respectively. Furthermore, the monthly mean precipitation is high in Hungary both in May and November [Citation13]. In a prospective study of Filipino mothers, Popkin and colleagues found that seasonality was also a significant determinant of mortality during the first 7 days of life in the wet season [Citation14]. Borchers and colleagues reported double peaks of respiratory syncytial virus (RSV) infection in spring and autumn in temperate regions [Citation15]. Bloom-Feshbach and colleagues described the peak of the flu epidemic and RSV epidemic in the continental climate in the Northern Hemisphere in February [Citation16]. However, the RSV virus period around the peak time was estimated as 4–6 months. Thus, we can hypothesize the role of RSV infections in perinatal mortality and that of the concurrent peak of influenza and RSV infections in postperinatal mortality.
Apostolidou and colleagues found a highly significant seasonal variation in postneonatal deaths from infections in winter [Citation17]. Douglas and colleagues also reported more sudden infant deaths in winter than summer [Citation18]. Additionally, Arroyo and colleagues described that pollutant concentrations, noise, and temperature influenced the weekly average number of newborns with low birthweight [Citation19].
We found significant double-peak trends (May and November) in mortality rates for perinatal, neonatal, and postneonatal infant deaths, respectively. The winter peak (December) of the seasonality pattern remained after adjusting for birthweight in the multiple negative binomial regression model. This finding reveals that low birthweight is a very significant risk factor for infant deaths. However, in winter, the risk of infant deaths is increasing due to environmental effects, most likely by infections.
Gaillard and colleagues reported that first, second, and third trimester fetal growth characteristics were associated with risks of preterm birth and small size for gestational age at birth [Citation20]. Furthermore, Olsson and colleagues described an association between some environmental factor and adverse pregnancy outcome in a register-based cohort study [Citation21]. Thus, we might suppose that environmental effects during the first trimester could increase the risk of perinatal mortality in babies born in May which is reflected in the second peak of the seasonality pattern.
A February peak cyclic trend was found in mortality rates from respiratory diseases. Since RSV is among the most important pathogenic infections in childhood, this could be associated with significant mortality in children aged under 15 years [Citation17].
Parkkari and colleagues reported a continuous decline in childhood injury deaths in Finland over the four decades between 1971 and 2010 [Citation22], a result which is consistent with our findings.
There was no seasonal variation in monthly mortality rates for deaths from childhood cancer. However, a significant single-peak cyclic trend in mortality rates was found for deaths from road accidents and drowning in July, which is the holiday season. A similar summer peak for traffic accidents, childhood drowning, and adolescent injury mortality was observed in Japan by Shinsugi and colleagues [Citation23].
Although annual trends have been decreasing in Hungary over the last two decades, both in childhood mortality rates overall and by cause of death, the country still reported the second highest rate of infant mortality out of 24 European countries in the 2011 and 2012 tables produced by the Organization for Economic Co-Operation and Development [Citation24].
Strengths and weaknesses of our study
In this ecological study, we have investigated the annual and seasonal pattern of mortality in children aged 0–14 years. Significant double-peak models were observed to characterize the seasonal variation in mortality rates for infant deaths and perinatal mortality, respectively. In addition, similar cyclic trends were detected in preterm and low birth weight babies. In spite of the lack of direct evidence for infections in the analyses, we can speculate that these infections may play a role in the etiology of infant mortality in preterm and low birth weight babies. In spite of the different pattern of seasonality that was found in the multiple regression analyses, the findings confirmed the effect of seasonality in infant deaths. Furthermore, our study has revealed the relationship between environmental effects and infant deaths at population level.
Additionally, we investigated the cyclic trends in the leading causes of death among children aged 0–14 years and found no seasonal variation in monthly mortality rates for deaths from childhood cancer. However, a significant summer peak was noted in deaths from traffic accidents and drowning, and a winter peak was observed in deaths from respiratory diseases. In spite of our use of data from the published registry in the analyses, the reliability of our findings is still high since the major causes of death on the death certificates are provided by either the deceased person’s general practitioner or treating hospital. The proportion of misclassified cause of death is very low. The trends might supply important clues on the etiology of perinatal mortality. Additionally, we have demonstrated the performance of the Walter–Elwood method in double-peak seasonality analyses and compared it with that of negative binomial regression. Nevertheless, both methods have high power to detect cyclic trends. However, multiple variable analysis could be only carried out using negative binomial regression which is a statistical test that allows for adjustment of confounding for the study of seasonal patterns.
Conclusion
We provided a detailed description of seasonal effects related to mortality rates for deaths among children under 15 years. Significant single-peak seasonality was found in mortality from traffic accidents and drowning during the summer holiday season, and there was a significant double-peak seasonal effect on infant and perinatal mortality. Nevertheless, preterm deaths, low birth weight infant deaths, stillbirth, neonatal, and postneonatal mortality are increased by seasonal effects. Since cyclic trends in the etiology of mortality show some effect of environmental factors, we might speculate that perinatal mortality may have been related to respiratory infections. A significant single peak was observed in mortality rates in July in both deaths from traffic accidents and drowning among children aged 0–14 years which could be related to environmental factors, such as temperature, air masses, and fronts. However, there was no seasonal variation in monthly mortality rates for deaths from childhood cancer. All of these novel findings could prove useful in preventive strategies, but further cohort studies are needed to investigate this hypothesis.
Ethical approval
No ethical approval was necessary based on the Hungarian Acton the usage of statistical data (Act XLVI 1993, Sec. 10).
Acknowledgments
Authors wish to thank employee of the Department of Data Support at Hungarian Central Statistical Agency for their assistance. We wish to thank to Miss Katalin Virág her assistance.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Armour-Marshall J, Wolfe I, Richardson E, et al. Childhood deaths from injuries: trends and inequalities in Europe. Eur J Public Health. 2012;22(1):61–65.
- Peden MM, McGee K. The epidemiology of drowning worldwide. Inj Contr Saf Promot. 2003;10(4):195–199.
- Vincenten J, Michalsen A. Priorities for child safety in the European Union: agenda for action. Inj Contr Saf Promot. 2002;9(1):1–8.
- Pearce MS, Parker L. Childhood cancer registrations in the developing world: still more boys than girls. Int J Cancer. 2001;91(3):402–406.
- The Hungarian Central Statistical Office. Demographic yearbook. Budapest: KSH; 1995–2014.
- World Health Organization. Neonatal and perinatal mortality: country, regional and global estimates. Geneva: WHO Press; 2006.
- Stolwijk AM, Straatman H, Zielhuis GA. Studying seasonality by using sine and cosine functions in regression analysis. J Epidemiol Commun Health. 1999;53(4):235–238.
- Walter SD, Elwood JM. A test for seasonality of events with a variable population at risk. J Epidemiol Community Health. 1975;29(1):18–21.
- Richardus JH, Graafmans WC, Verloove-Vanhorick SP, et al. Differences in perinatal mortality and suboptimal care between 10 European regions: results of an international audit. BJOG. 2003;110(2):97–105.
- Scioscia M, Vimercati A, Maiorano A, et al. A critical analysis on Italian perinatal mortality in a 50-year span. Eur J Obstet Gynecol Reprod Biol. 2007;130(1):60–65.
- Zeitlin J, Wildman K, Bréart G, et al. PERISTAT: indicators for monitoring and evaluating perinatal health in Europe. Eur J Public Health. 2003;13(3 Suppl):29–37.
- Zimbeck M, Mohangoo A, Zeitlin J. The European perinatal health report: delivering comparable data for examining differences in maternal and infant health. Eur J Obstet Gynecol Reprod Biol. 2009;146(2):149–151.
- Hungarian Meterology Office, Budapest, Hungary. [cited 21 Mar 2019]. Available from: http://met.hu/en/eghajlat/magyarorszag_eghajlata/altalanos_eghajlati_jellemzes/csapadek/.
- Popkin BM, Guilkey DK, Schwartz JB, et al. Survival in the perinatal period: a prospective analysis. J Biosoc Sci. 1993;25(3):359–370.
- Borchers AT, Chang C, Gershwin ME, et al. Respiratory syncytial virus – a comprehensive review. Clin Rev Allergy Immunol. Rev. 2013;45(3):331–379.
- Bloom-Feshbach K, Alonso WJ, Charu V, et al. Latitudinal variations in seasonal activity of influenza and respiratory syncytial virus (RSV): a global comparative review. PLoS One. 2013;8(2):e54445.
- Apostolidou I, Katsouyanni K, Touloumi G, et al. Seasonal variation of neonatal and infant deaths by cause in Greece. Scand J Soc Med. 1994;22(1):74–80.
- Douglas AS, Allan TM, Helms PJ. Seasonality and the sudden infant death syndrome during 1987–9 and 1991–3 in Australia and Britain. BMJ. 1996;312(7043):1381–1383.
- Arroyo V, Díaz J, Carmona R, et al. Impact of air pollution and temperature on adverse birth outcomes: Madrid, 2001–2009. Environ Pollut. 2016;218:1154–1161.
- Gaillard R, Steegers EA, de Jongste JC, et al. Tracking of fetal growth characteristics during different trimesters and the risks of adverse birth outcomes. Int J Epidemiol. 2014;43(4):1140–1153.
- Olsson D, Mogren I, Forsberg B. Air pollution exposure in early pregnancy and adverse pregnancy outcomes: a register-based cohort study. BMJ Open. 2013;3(2). [pii: e001955].
- Parkkari J, Mattila V, Kivistö J, et al. Fatal childhood injuries in Finland, 1971–2010. Inj Prev. 2013;19(3):171–176.
- Shinsugi C, Stickley A, Konishi S, et al. Seasonality of child and adolescent injury mortality in Japan, 2000–2010. Environ Health Prev Med. 2015;20(1):36–43.
- Organization for Economic Co-Operation and Development. Health: key tables from OECD Available from: http://www.keepeek.com/Digital-Asset-Management/oecd/social-issues-migration-health/infant-mortality-2013-2_inf-mort-table-2013-2-en#page1.