
ABSTRACT
Little is known about covert trading behaviour in secure hospital settings. This study evaluated the nature, prevalence, and frequency of covert voluntary trading behaviour (VTB) and of coercive trading behaviour (CTB) between patients in secure psychiatric units. Ninety-six eligible patients in 18 low or medium secure wards across South London anonymously completed a questionnaire exploring their experiences of covert trading behaviour (including exchanging, lending, borrowing, or gifting personal property, money, or services) during their current hospital admission. About 70.2% reported engaging in some form of unauthorised VTB (38.3% ≥5 different behaviours). VTB was more commonly reported by male (74.7%) than female (36.3%) participants (odds ratio (OR) = 4.93, 95% confidence intervals (CI) = 1.28,19.05, p = 0.021). Engagement in any CTB behaviour was reported by fewer patients (31.9%). Participants were significantly more likely to report themselves as victims of coercive behaviours (8.6%–14.0% across different behaviours) rather than instigators (1.1%–5.5% across behaviours). Involvement in CTB was more common in patients reporting VTB (39.4%) compared to those not involved in VTB (14.3%; OR = 3.90, CI = 1.21,12.54). Covert patient trading appears commonplace in secure psychiatric inpatient settings and VTB participation may be linked with CTB engagement. Hospital policies to better monitor and regulate patient trading may help to reduce the incidence of CTB.
Introduction
Covert trading in the form of exchanging, lending, loaning, borrowing, or gifting personal property, money, or services between patients without permission from the multidisciplinary team is discouraged on secure forensic inpatient units as it is believed to be associated with disputes, illicit behaviour, bullying, and exploitation in secure settings (Gooch & Treadwell, Citation2015). Although there is presently no published research on the nature, prevalence, and frequency of trading in psychiatric hospitals, studies on bullying behaviours in prison have found that covert trading and borrowing amongst prisoners is an embedded part of prison culture (Gooch & Treadwell, Citation2015). As secure hospitals and prisons share comparably restrictive environments with an overlapping population, it is likely that covert trading is similarly commonplace in secure hospital settings.
Covert patient trading is difficult to monitor on secure forensic inpatient units as it can be easily hidden or overlooked by hospital staff. Monitoring of covert patient trading typically relies upon staff directly observing patients trading, trading behaviour coming to light following incidents, or patients voluntarily disclosing prohibited activities to staff. There are multiple factors that may deter a patient from disclosing unauthorised trading behaviour to hospital staff. With regards to voluntary trading behaviour (VTB), defined in this study as consensual trading between patients, such behaviour can often be mutually beneficial thereby providing an incentive for patients to conceal the activity. On the other hand, coercive trading behaviour (CTB) defined here as trading between patients in response to pressure, threats, intimidation, or bullying, may not be reported by patients due to peer pressure, fear of being labelled a ‘snitch’, and threats of retribution. Patients may also be apprehensive to disclose prohibited behaviour to staff more generally due to fear of punitive measures, such as rescinding leave or a change in zoning, which may impede their progress towards discharge (Gakhal & Oddie, Citation2014).
There is currently no published research that specifically investigates trading behaviours amongst psychiatric patients in a secure hospital setting. However, there have been several small-scale studies investigating the prevalence and nature of bullying in high and medium secure forensic units, which include behaviours that would be considered CTB. Much of the work in this area has been conducted by Professor Jane Ireland in high-secure forensic settings (Ireland & Bescoby, Citation2005; Ireland & Rowley, Citation2007; Ireland & Snowden, Citation2002; Ireland, Citation2004, Citation2005, Citation2006), while there are two small studies looking at bullying in medium-secure forensic settings (Cooper et al., Citation2011; Gakhal & Oddie, Citation2014). Each of these studies focuses on a broad definition of bullying that encompasses a wide range of direct and indirect forms of bullying behaviours. In summary, the research conducted by Ireland and colleagues suggests that bullying behaviour is prevalent amongst both male and female patients in high and medium secure hospital settings. The research also indicates that many patients are willing to disclose such behaviours via the use of anonymous questionnaires.
The primary aim of this study was to evaluate the nature (e.g. type of trading), prevalence, and frequency of covert VTB and CTB between patients on low and medium secure forensic inpatient units across South London. The authors anticipated that covert trading would be a prevalent and heterogenous behaviour amongst psychiatric patients detained in secure hospital settings. The study’s secondary aim was to consider whether there is a relationship of specific patient sociodemographic characteristics, admission status, and forensic history (e.g. age, gender, number of admissions to hospital, duration of current admission, previous custodial sentence, and leave status) with reported trading behaviour.
Methodology
Design and setting
The study utilised a cross-sectional survey design and took place across three South London NHS mental health trusts. All 18 medium and low secure forensic inpatient wards within the three trusts were included in the study. The 18 wards were comprised of secure acute admission units, a secure psychiatric intensive care unit, and secure rehabilitation units. Four of the wards were secure female units. The study was approved by the Research and Development Committee at South West London & St George’s Mental Health Trust. Ethical approval for the study was provided by the Essex Research Ethics Committee (REC reference 21/EE/0023).
Participants
All patients detained on the 18 secure wards at the time the study commenced were considered for participation (n = 228). The study inclusion criteria were fluency in English, the ability to read and write, having been admitted to the unit for at least a week, and having capacity to consent to participate. Patients were excluded if they were deemed unsafe to approach or if the clinical team was unhappy for the patient to participate in the study for any unforeseen reason.
After liaising with the clinical team from each of the 18 wards, 22 (9.6%) patients were identified as ineligible. The most common reasons for ineligibility were lack of English fluency and safety concerns due to acutely disturbed mental states. Of the remaining 206 eligible patients, 84 (40.8%) declined to participate when approached and 26 (12.6%) were repeatedly unavailable during the data collection period. In total, 96 (46.6%) eligible patients agreed to participate in the study and provided written informed consent for their (anonymised) data to be used for research purposes.
Procedure
On review of the available literature, there are presently no validated tools specifically for measuring trading behaviours in secure hospital or prison settings. Consequently, a novel questionnaire exploring participants’ experiences of covert trading behaviour during their current admission to hospital was developed. The questionnaire employed a combination of 19 multiple-choice and Likert scale questions to assess the nature and frequency of different types of covert VTB and CTB (for examples, see ). The questionnaire concluded with five multiple-choice questions about sociodemographic and admission-related characteristics (for examples, see ). The length of the questionnaire was purposely short, designed to be completed in less than 10 minutes, as it has been established that longer questionnaires can discourage participation in research exploring bullying in a secure hospital setting (Gakhal & Oddie, Citation2014).
Figure 1. Example questions concerning engagement in voluntary trading behaviour and engagement in coercive trading behaviour (left; 1a) and admission-related/forensic history information (right; 1b).
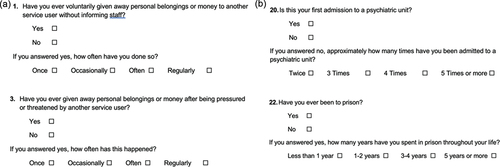
The study was advertised via a poster displayed within the communal area of each participating ward. Each patient who expressed an interest in participating in the study was given a Patient Information Sheet and provided with a verbal explanation from a member of the study team. If it was determined that the patient was eligible to participate in the study, they were asked to fill out a written consent form. On the data collection days, eligible consenting participants were subsequently provided with the study questionnaire to complete independently. Participants were reassured that the questionnaires were anonymous and that their responses would remain confidential.
Statistical analysis
Sociodemographic and admission-related characteristics of participating inpatients detained on low secure and medium secure wards (e.g. age group, whether present admission is first admission, leave status) and the prevalence/regularity of voluntary and coercive trading behaviours (e.g. giving away, lending, and trading/exchanging personal belongings) were recorded as frequencies and percentages. Mid-p McNemar tests (Fagerland et al., Citation2013) were used for comparisons of prevalence rates between different types of trading behaviours. Chi-square (and Fisher’s exact) tests were employed to measure associations between engagement in VTB, engagement in CTB, and patient characteristics. To analyse the combined contribution of relevant (potentially covarying) characteristics, multivariate logistic regression models were constructed; only patient-related variables showing associations at alpha level of p < 0.05 in univariate analyses were included in regression models. All statistical analyses were completed using SPSS (IBM, Version 27.0) with a criterion for statistical significance set at p < 0.05. Significant tests of association were described using odds ratios (ORs) and 95% confidence intervals (CI).
Results
Data were collected from 96 inpatients from three NHS Trusts (n = 35, 30, and 29). Two inpatients did not respond to any questions concerning sociodemographic and admission-related characteristics (and completed <20% of questions concerning trading behaviour) and were excluded from sample description and subsequent analyses.
Sociodemographic and admission-related characteristics of men and women in this secure care population are provided in . The vast majority were male, and two-thirds were aged between 26 and 49 years. Three-quarters of participants were detained on a medium secure unit (45 (47.9%) on medium secure acute admission wards, 7 (7.4%) on a medium secure psychiatric intensive care unit (PICU), and 18 (19.1%) on medium secure rehabilitation wards). About half of the participants had been detained on a unit for more than a year at the time of study. A little under 30% had no leave status, a fifth were allowed grounds leave only and half were allowed community leave. More than three-quarters of participants had had a previous stay in hospital, while close to a third had been in hospital on four or more occasions previously. Most participants had also previously been in prison with close to a quarter having spent three or more years there.
Table 1. Sociodemographic and admission-related characteristics of participating inpatients detained on low-secure and medium-secure wards (n = 94). Values represent frequency (percentage).
Prevalence and pattern of voluntary and coercive trading behaviours
Sixty-six (70.2%) individuals had engaged in some form of unauthorised VTB while on the secure ward; most had been engaged in more than one behaviour (56/94 or 59.6%) while more than a third (36/94 or 38.3%) reported involvement in 5 or more voluntary behaviours (‘high level’). Thirty (31.9%) participants had engaged in some form of CTB (16/94 or 17.0% reported engaging in 2 or more coercive behaviours); 27 (28.7%) reported being a victim of (some form of) CTB and 10 (10.6%) reported instigating (some form of) CTB.
The self-reported prevalence and frequency of different voluntary and coercive trading behaviours in participating secure unit inpatients are shown in . Voluntarily giving away and receiving personal belongings/money were the behaviours reported most frequently, although between 39.8% and 47.3% participants reported voluntarily trading, borrowing, and/or lending personal belongings/money. Receiving a loan and giving another service user a loan were the voluntary trading behaviours least commonly reported. Across voluntary behaviours, the majority of participants who reported engaging in a behaviour did so either ‘once’ or ‘occasionally’, with only a small proportion reporting engaging ‘often’ or ‘regularly’ (0% to 27.8%, depending on the specific behaviour – see ). Participants more frequently reported voluntarily giving away personal belongings/money than receiving them (p = 0.035) but there were no differences between giving/lending and receiving/borrowing for other (corresponding) voluntary behaviours.
Figure 2. Prevalence and frequency of inpatient-reported voluntary (left; 2a) and coercive (right; 2b) trading behaviours. Data labels represent prevalence percentage values for each behaviour. SU = service user. Note: 1 participant reported pressuring another service user to give away personal belongings/money but did not provide frequency data for this behaviour.
Engagement in coercive behaviours was less frequently reported; between 8.6% and 14.0% of participants reported being pressured or threatened to engage in each trading behaviour, while between 1.1% and 5.4% of patients reported coercing another service user to engage in each behaviour (). Engagement rates in each CTB were significantly less than that in the corresponding voluntary behaviour with the sole exception of receiving a loan from another service user (p = 0.119; for all other comparisons, p < 0.040). Participants more frequently reported themselves as victims of coercion than instigators of coercive behaviours (on other service users) for each comparable behaviour (for all comparisons, p < 0.040). While the number of participants who reported engaging in CTB was small, for those that did, frequency of engagement was widely distributed. For instance, around half of the participants reporting giving away (7/13 or 53.8%) and lending (6/13 or 46.2%) personal belongings/money after being pressured or threatened indicated this occurred ‘often’ or ‘regularly’.
Relationship between voluntary and coercive trading behaviour
There was a strong association between (reporting of) engagement with VTB and that of CTB (). CTB was reported by almost 40% (26/66 or 39.4%) of participating inpatients reporting VTB compared with only 14.3% of inpatients (4 individuals) not involved in VTB, an almost 4-fold increase in associated risk (OR = 3.90, CI = 1.21, 12.54, p = 0.017). More specifically, the odds of being a victim of CTB were elevated for participating inpatients reporting VTB (24/66 or 36.4%) compared with patients not involved in VTB (3/28 or 10.7%; OR = 4.76, CI = 1.30, 17.44, p = 0.012). Participants reporting VTB more often reported instigating CTB (9/66 or 13.6%) than those not involved in VTB (1/28 or 3.6%), although the difference was not significant (p = 0.148).
Figure 3. Venn diagram showing overlap between participating inpatients reporting engagement in voluntary trading behaviour (VTB) and engagement in coercive trading behaviour (CTB; as a victim or an instigator). Values represent frequencies (percentages).
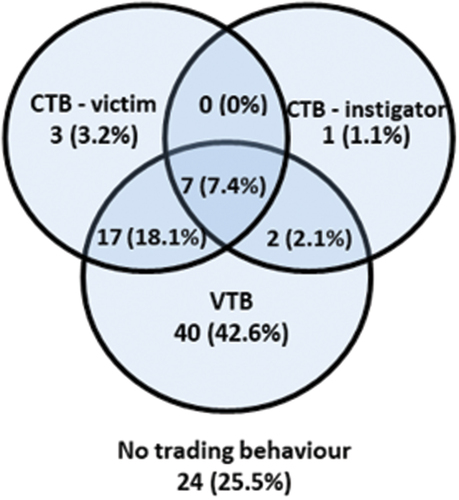
There were no significant differences between the proportion of patients with low (1–4 different behaviours) and high levels (≥5 different behaviours) of VTB in reported engagement with (any) CTB (11/30 or 45.5% versus 15/36 or 41.7%; p = 0.679), although 7 of the 10 patients who reported instigating CTB also reported high-level engagement with VTB.
Association of voluntary and coercive trading behaviours with patient characteristics
The individual characteristics of participating inpatients who reported engaging in voluntary and coercive trading behaviours and of those who did not report such engagement are described in . VTB was more frequently reported in male participants (74.7%) compared with female participants (36.3%) and by those in medium secure units (75.7%) compared with those in low secure units (54.2%); regression analyses that considered both variables indicated a significant increase in odds of VTB engagement in males (OR = 4.93, CI = 1.28, 19.05, p = 0.021) and a trend for those participants in medium security units (OR = 2.52, CI = 0.92, 6.90, p = 0.072). Rates of VTB appeared particularly high in medium secure PICUs (7/7 or 100%) and medium secure rehabilitation units (14/18 or 77.8%), although small numbers precluded formal comparisons with these subgroups. While rates of VTB were numerically greater in participants who had been in hospital ≥1 year, were currently on ‘grounds leave only’ status, and had not previously been in prison, these differences were not significant.
Table 2. Individual characteristics of participating inpatients reporting voluntary trading behaviour (VTB) and coercive trading behaviour (CTB).
There were no significant associations between individual characteristics and engagement in any coercive behaviour. In contrast to the findings concerning voluntary trading behaviours, the proportion of individuals reporting any coercive behaviour was (non-significantly; p = 0.271) greater in LSU patients than MSU patients.
Discussion
The results strongly support the hypothesis that covert patient trading is commonplace in secure psychiatric inpatient settings. Over 70% of participants admitted having participated in some form of covert VTB during their admission to hospital and over a third of participants disclosed engaging in five or more different forms of VTB. With regards to CTB, nearly 30% of participants disclosed having been a victim of CTB during their admission and more than one in ten admitted being a perpetrator of CTB. These findings are consistent with rates of direct bullying and victimisation found in prisons and secure psychiatric hospitals (Ireland et al., Citation2019). Furthermore, the study findings demonstrate that patients engage in a broad range of covert trading behaviours. This supports the notion that unauthorised patient trading is a normalised activity on secure psychiatric units, consistent with research conducted in prisons (Gooch & Treadwell, Citation2015).
The high prevalence of covert VTB is unsurprising given the inherently restrictive environment of a secure psychiatric ward and patients’ limited access to the community. Staff members in secure settings may even overlook incidents of covert VTB if they consider the behaviour to be harmless (Gooch & Treadwell, Citation2015). However, the significant prevalence of CTB highlighted in this study is a particular cause for concern. CTB may be easily disguised as VTB, especially if it is undisclosed and unmonitored (Gooch & Treadwell, Citation2015). The normalisation of covert patient trading amongst both patients and staff risks vulnerable patients being exploited by CTB under the guise of VTB. Although this may be intentional in some cases, the blurring of coercive versus voluntary behaviour means that patients may not always recognise that they are being victimised or that their actions are victimising others. This is supported by qualitative research conducted on a secure hospital ward where the majority of patients and staff considered that bullying could be accidental on the part of the perpetrator (Ireland, Citation2005).
Interestingly, this study demonstrated that the odds of being a victim of CTB were significantly elevated for patients who also engaged in VTB compared with patients not involved in VTB. This suggests that participating in VTB may increase an individual’s risk of being a victim of CTB. Previous research on bullying in secure hospital settings has found that the proportion of individuals who are classed as both victim and bully is often higher than those in the pure victim, pure bully, or not involved groups (Ireland & Power, Citation2004; Ireland & Rowley, Citation2007; Sekol, Citation2016). This implies that there is not always a clear distinction between bully/victim or engaging in voluntary/coercive trading behaviour. To this point, the differentiation of VTB and CTB used in this study is a likely oversimplification of what is almost certainly a complex spectrum of behaviours. Future in-depth (qualitative) investigations are needed to provide clarity about the extent of behavioural overlap and separability. Nevertheless, the current findings highlight that any measures implemented to reduce the incidence of CTB should also consider VTB and suggest there may be justification for the blanket prohibition of all covert patient trading on secure psychiatric wards.
There were two significant associations between specific patient characteristics and trading behaviours identified in the study. The first was an increased frequency of VTB for males compared to females. To date, there is no comparative research on gender differentials in trading behaviours in secure settings. As such, this is an area that requires further investigation. The second significant association was an increased frequency of VTB for patients detained on MSUs relative to LSUs. The latter association may be expected due to the inherently more restrictive environment of an MSU although, importantly, once gender was controlled for the security status of the unit in which the participant was detained was not significant (rather, there was a trend only). The study did not identify any significant associations between specific patient characteristics and CTB. While this may be a function of the small numbers of patients reporting CTB (Type 2 errors), it may also be partly explained by the non-specific sociodemographic items and/or the self-reported format of data acquisition that the questionnaire relied upon to ensure patient anonymity. Future research could mitigate this by designing a study with information obtained from patient medical records, enabling a wider range of sociodemographic, clinical, and admission-related variables to be investigated.
Although the study had a modest sample size, it was notably larger than that of previous research on bullying/intra-group aggression in secure psychiatric settings (e.g. Cooper et al., Citation2011; Gakhal & Oddie, Citation2014; Ireland, Citation2004). It also spanned 18 wards across three different UK NHS Trusts. The study also demonstrated that many patients were willing to disclose prohibited behaviour via an anonymous questionnaire that may otherwise have been difficult to measure. Nonetheless, the observed prevalence of VTB and CTB are likely to be an underestimate of the true prevalence due to the expectation that many patients will remain reluctant to disclose prohibited behaviour despite the study’s reassurance of anonymity. A related study limitation is the self-selecting participant sample. For example, patients who completed the study questionnaire may have been more willing to disclose prohibited behaviour than those who did not wish to participate. Only half of the eligible participants agreed to take part in the study. This could have been due to a range of factors, some of which may be related to participants’ underlying mental health difficulties, for example, distrust of staff or professionals due to paranoia, or disinterest, apathy, and amotivation due to low mood or negative psychotic symptoms. This limitation could be mitigated in the future by adapting the recruitment process to focus on building rapport with potential participants and extending the recruitment phase to account for fluctuations in mental state.
Conclusions
This is the first published study investigating trading behaviour in a psychiatric hospital setting and further research in this area is required. Future projects could be extended to investigate patient trading in high-secure psychiatric settings as well as general adult psychiatric inpatient populations. This study did not consider patient sexual trading, which would be important to investigate in the future research. One of the most common reasons for ineligibility in this study was a lack of English fluency. Participation could be increased in the future if translated questionnaires could be provided. Further, factors known to influence intra-group aggression among patients in secure psychiatric care, such as a normalisation of bullying, lack of support for victims, victim blaming, admiration of bullies, and the perception of bullies as skilled (Cooper et al., Citation2011; Ireland et al., Citation2016), could also be assessed to determine their relationship with covert trading, particularly CTB.
Research implications
The findings of this study raise awareness of the high prevalence rate of covert patient trading on secure psychiatric units. It is hoped that the findings can prompt the development of hospital policies to better monitor and regulate covert patient trading, thereby reducing the incidence of CTB.
Acknowledgements
The study authors would like to thank the research and development team at South West London and St Georges NHS Trust for their invaluable help and support throughout. The authors would also like to convey their gratitude to Dr Gunjan Sharma, Dr Daniele Maugeri, Dr Matthew Hartley, Dr Farah Jawahar, Dr Phoebe Collins, Dr Rosy Blunstone, and Dr Helen Souchon for their assistance with data collection.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Cooper, H. C., Terry, R., & Gudjonsson, G. (2011). Bullying behaviour among mentally disordered patients in a medium secure hospital environment and the relationship between bullying attitudes and violent cognitive style. Journal of Forensic Psychiatry & Psychology, 22(1), 126–137. https://doi.org/10.1080/14789949.2010.518246
- Fagerland, M. W., Lydersen, S., & Laake, P. (2013). The McNemar test for binary matched-pairs data: Mid-p and asymptotic are better than exact conditional. BMC Medical Research Methodology, 13(1), 1–8. https://doi.org/10.1186/1471-2288-13-91
- Gakhal, B., & Oddie, S. (2014). Bullying behaviours among mentally disordered offenders in a medium secure unit. Journal of Forensic Practice, 16(2), 156–165. https://doi.org/10.1108/JFP-03-2013-0020
- Gooch, K., & Treadwell, J. 2015. Prison bullying and victimisation. University of Birmingham Retrieved April 4, 2022, from https://www.birmingham.ac.uk/documents/college-artslaw/law/prison-bullying-and-victimisation.pdf
- Ireland, J. L. (2004). Nature, extent, and causes of bullying among personality-disordered patients in a high-secure hospital. Aggressive Behaviour, 30(3), 229–242. https://doi.org/10.1002/ab.20017
- Ireland, J. L. (2005). Exploring definitions of bullying among personality disordered patients in a maximum-secure hospital. Aggressive Behaviour, 31(4), 359–373. https://doi.org/10.1002/ab.20064
- Ireland, J. L. (2006). Bullying among mentally-ill patients detained in a high-secure hospital: An exploratory study of the perceptions of staff and patients into how bullying is defined. Aggressive Behaviour, 32(5), 451–463. https://doi.org/10.1002/ab.20145
- Ireland, J. L., & Bescoby, N. (2005). Behavioural assessment of bullying behaviour among personality disordered patients in a high secure hospital. Aggressive Behaviour, 31(1), 67–83. https://doi.org/10.1002/ab.20073
- Ireland, J. L., Ireland, C. A., Power, C. L., (2016). Attitudes towards prisoner-to- prisoner bullying and the association with prison environments: Examining the components. Journal of Aggression, Conflict and Peace Research, 8(2), 124–136. https://doi.org/10.1108/JACPR-05-2015-0172
- Ireland, J. L., & Power, C. L. (2004). Attachment, emotional loneliness, and bullying behaviour: A study of adult and young offenders. Aggressive Behaviour, 30(4), 298–312. https://doi.org/10.1002/ab.20035
- Ireland, J. L., & Rowley, J. (2007). Sectioned offenders presenting with enduring mental illness: A study exploring behaviours indicative of bullying. Aggressive Behaviour, 33(5), 377–388. https://doi.org/10.1002/ab.20189
- Ireland, J. L., Sebalo, I., McNeil, K., Murphy, K., Brewer, G., Ireland, C. A., Chu, S., Lewis, M., Greenwood, L., & Nally, T. (2019). Impacting on factors promoting intra-group aggression in secure psychiatric settings. Heliyon, 5(3), e01400. https://doi.org/10.1016/j.heliyon.2019.e01400
- Ireland, J. L., & Snowden, P. (2002). Bullying: An issue for secure hospitals. Journal of Forensic Psychiatry, 13(3), 538–554. https://doi.org/10.1080/0958518021000019434
- Sekol, I. (2016). Bullying in adolescent residential care: The influence of the physical and social residential care environment. Child & Youth Care Forum, 45(3), 409–431. https://doi.org/10.1007/s10566-015-9336-8