
Abstract
Objective: Our objective was to understand the factors that determine whether an adult who is eligible for cochlear implantation (CI) choose to take up or not take up the implant.
Design: We conducted a qualitative in-depth interview study, informed by grounded theory methods of constant comparison to build a theory to describe why and how people decide to opt for CI or not.
Study sample: Our samples were patients from an audiology service in England.
Results: Our results describe the key factors in weighing up risks and benefits. These are influenced by living context and support, information and social identity. We identify the key features that impact decision making for adults eligible for cochlear implants. The importance of the patient lifeworld view is discussed.
Conclusions: This qualitative study provides the first in depth examination of how and why patients do and do not take up the offer of cochlear implants. It highlights the complex and iterative nature of this decision making and the individualised risks that trade off benefits of implantation.
Introduction
Severe-profound hearing loss (SPHL) affects over 900,000 people in the UK (Action on Hearing Loss Citation2015), and can have severe consequences on mental health, social inclusion and quality of life (Carlsson et al. Citation2015). For those with SPHL who have limited success with hearing aids, cochlear implantation (CI) is recommended as a suitable alternative (Raine Citation2013). However, the UK has strict criteria for candidacy for CI compared to international counterparts (Chundu and Flynn Citation2014; Vickers, De Raeve, and Graham Citation2016), negatively impacting the percentage of the population taking up CI in the UK compared to international populations (De Raeve and Van Hardeveld Citation2013; Raine et al. Citation2016). Recent research suggests that despite increasing numbers of cochlear implant surgeries, duration of living with a severe hearing loss before CI in adult patients is increasing (Appelbaum et al. Citation2017), and uptake in the adult candidate population in the US is shown to be as little as 5.6% (Sorkin Citation2013), a trend reflected in the UK (Raine Citation2013; Raine et al. Citation2016).
Low uptake of CI seemingly conflicts with extensive evidence showing that CI improves quality of life (Crowson et al. Citation2017) and improve outcomes in multiple domains when compared to hearing aids, including psychosocial health, functional health and social inclusion (Francis et al. Citation2002; Cohen et al. Citation2004; Bosdriesz et al. Citation2017), while being cost effective (Bond et al. Citation2009). Delaying implantation has been shown to be disadvantageous; evidence suggests a correlation between increasing duration of hearing loss prior to implantation (Blamey et al. Citation2013), as well as links between increasing age at time of implantation and poorer speech recognition scores (Blamey et al. Citation2013; Beyea et al. Citation2016; Hiel et al. Citation2016).
Research by Sorkin (Citation2013) identified seven barriers to uptake of CI in the USA; low general awareness, ignorance of professionals towards candidacy and outcomes, support for Deaf culture, financial issues, lack of standardised clinical practice, data concerning a lack of cost effectiveness and a lack of a dedicated organisation for CI. Similar findings in Japan & South East Asia (Okubo, Takahashi, and Kai Citation2008; Chundu and Stephens Citation2013) particularly highlighted concerns about costs. Work on shared decision making in CI has focussed on type of implant (Geyer et al. Citation2006; Clamp et al. Citation2013). Little is known about the decision made by the eligible patient on whether or not they pursue CI.
Given the important contribution made by cochlear implants to hearing function, it is important to understand the decision making process that the patient undertakes and the factors that influence their decisions. Our aims were to understand the adult who is eligible for CI.
To understand factors that adult candidates for CI consider when deciding to proceed or not proceed with CI, at any time between deciding to be referred and receiving the implant.
To seek the opinions of those who seek, have accepted or have rejected the option of CI, to understand views from a range of perspectives.
Methods
A grounded theory approach was used to generate a theory inductively. Benefits of the interpretative approach of grounded theory is the generation of theories that reflect the lived experiences of patients based on social constructs and individual priorities, taking into account multifactorial elements such as relationships and life events (Hallberg Citation2006; Lawrence and Tar Citation2013). Such an approach is therefore vital to explain how and why phenomena (in this case patient preferences to take up or reject CI) occur.
Ethical approval of the study was provided by the North of Scotland NHS Research Ethics Committee and the Health Research Authority in August 2017. The study was reviewed and approved by Gloucestershire Hospitals NHS Foundation Trust (GHNHSFT) Research and Development team and the Aston Governance committee in September and October 2017, respectively.
Recruitment was conducted between November 2017 and January 2018. The clinical database of the Hearing Services department of GHNHSFT was systematically searched by a member of the research team to identify potential participants who met the inclusion criteria; patients aged ≥18 years with a SPHL consisting of bilateral unaided pure tone audiometric air conduction thresholds worse than 90 dBHL at 2 and 4 kHz. These criteria were based on NICE guidelines valid at the time of the study (NICE Citation2009) regarding eligibility for CI for adults in the UK. Speech recognition scores were not considered as this part of the Cochlear Implant assessment would not take place prior to referral to a cochlear implant centre. Those unable to give informed consent independently and non-English speakers (with the exception of British Sign Language users) were excluded due to the size and limited scale of the study.
Purposive sampling was used initially to capture a varied range of experiences, lifestyles, education levels, genders and ages, with eligible participants (32 potential participants) being sent a postal invitation pack and asked to contact the principal researcher (BD) to organise a date and location for their interview. Ten participants were recruited using this method, while a further five participants were recruited through snowball sampling, which was essential given the small sample population and limited ability to find and recruit participants with cochlear implants who no longer actively attended the hearing services department. Participants were required to fulfil one of the following criteria:
Have a cochlear implant/s.
Be in the assessment process for a cochlear implant – either prior to or after being referred to a CI centre.
Have been offered a cochlear implant/s and be awaiting surgery.
Have been in the assessment process for a cochlear implant (as per item 2 above) and rejected the option to have surgery or undergo further assessment.
Interviews (all with researcher BD) took place between November 2017 and February 2018. Of the 15 participants, 11 interviews were conducted in the participant’s home and four were conducted in the hospital’s hearing services department, as per participant preference. Conducting interviews in participants’ homes deconstructs traditional power hierarchies between the researcher and the interviewee (Sivell et al. Citation2015), and discourages assertion of the participant’s “patient” identity, which may influence responses (Elwood and Martin Citation2000). With this in mind, for hospital-based interviews efforts were made to minimise the appearance of a clinical interaction where possible.
Interviews were semi-structured using a topic guide consisting of open-ended questions, generated from literature of a similar nature to this study, although regarding a paediatric population (e.g. Archbold et al. Citation2006; Chang Citation2017). Although the concept of preconceived ideologies is in conflict with the grounded theory approach, it is noted that generation of seed concepts from other sources can be appropriate to guide the field of enquiry in early stages (Urquhart, Lehmann, and Myers Citation2009) ().
Table 1. Topic guide for interviews.
Interview progression led towards more directed questioning in later interviews based on emerging theories and concepts, in keeping with the grounded theory approach (Knudsen et al. Citation2012). The interviews were audio-recorded and later transcribed by the interviewer.
Data analysis
Analysis of data took place in parallel with data collection. Data were analysed by line by line open coding (summarising meaning units within the interview transcripts). These open codes were compared and synthesised where they were similar within and between transcripts to form categories. Where possible, “in-vivo” coding was used to remain close to the participant’s narrative with minimal researcher influence (Smith and Firth Citation2011). Each of the first ten interviews was analysed using this method, with analysis of each interview taking place prior to performing the next interview.
Codes were initially developed by researcher BD and were checked and compared with parallel analysis by researcher HP. The categories were compared with new data and refined or removed where they did not fit the new data. Theoretical saturation was sought (Birks and Mills Citation2015).
Abstraction of the raw data using the process of constant comparison and correlation of codes created 22 initial categories, which were used to form the properties and dimensions of eight themes generated from the data from the initial ten interviews. A thematic framework consisting of pre-conditions, phenomenon of interest, contextual conditions, strategies and consequences was generated from these emergent themes (Corbin and Strauss Citation1990). The remaining five interviews were analysed using theoretical coding, conceived from the theories generated thus far, and results used to continuously scrutinise and adapt the thematic framework, properties and dimensions. This process of adaptation in keeping with ongoing findings ensures fulfilment of generation of theory grounded from data.
Findings
The participants
Fifteen participants were recruited. Of the 15, 12 females and 3 males, age range 30–87 (mean age: 63 years), five of whom did not want CI (one participant had historically undergone CI but no longer uses the implanted device) and ten who either had, were in the process of receiving or wanted a cochlear implant. All participants were white British. An overview of participant profiles is presented in , with participants identified throughout the report using the assigned numerical identifiers. To preserve anonymity further we present age brackets rather than specific ages.
Table 2. Characteristics of participants.
: Overview of participant profiles.
Examples of open coding, with in-vivo examples, subsequent selective coding and categorisation are shown in .
Table 3. Examples of transcript quotes with their subsequent open coding with “in-vivo” elements in italics, selective coding and categorisation.
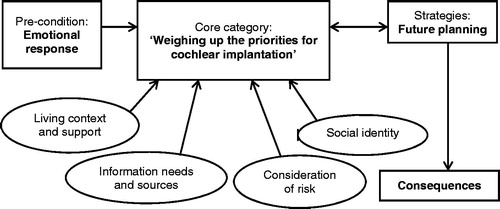
The final framework generated represents the decision-making process for participants in considering uptake of CI. A pre-condition to considering assessment for CI was quality of life, having been negatively impacted by the participant’s hearing loss and subsequent difficulties. At this stage, or after undertaking the assessment process for CI, participants were then required to make a decision whether to proceed with uptake of the CI, which was based significantly on their perception of the CI, consideration of the personal impact and their hopes and expectations of what it may give them, in terms of quality of life and planning for their future. Factors that shaped this decision included personal living context with physical and emotional support, information provision and degree of knowledge and understanding, consideration of cost and impact of risk, and the participant’s identity as a Deaf/deaf person in a “hearing world”.
Theme – weighing up priorities with CI
The theme “Weighing up priorities with CI” formed the core category in the decision-making process. This theme both interlinks with and influences all other themes, and dominated significantly in the decision whether or not to proceed with CI. The theme describes an active process of considering benefit vs. risk. Participants who decided not proceed with CI all cited negative expectations of outcome as a reason not to proceed; “But it doesn’t seem to be what would help me, I don’t know, that’s my feeling on it” (P2), “I’m scared that it could make me worse off” (P3), “…like cochlear implants but I don’t want to go down that route as I’m so afraid I’m going to end up worse than I am at the moment” (P4). Conversely, participants who wished to proceed with or had received implants expected improvements in hearing, which they linked to wider factors such as improvement in quality of life, perception of “fitting in” the hearing world and new experiences; “But having a kidney transplant is going to make my life better, and that’s the same with the implant, that is making your life better” (P7), “I’m looking forward to joining the hearing world. So I’m full of hope” (P13), “I do quite a lot of scuba diving, and I’d like to hear water” (P9).
Perception of CI was commonly influenced by others’ experience with cochlear implants, “I didn’t relish the idea of an implant but other people seemed to be managing better with it so I thought I’d go for it” (P10), with participants connecting to these implant users in social groups, in the community and from internet sources. Despite participants encountering others with both positive and negative experiences of CI, negative experiences were not enough to discourage some participants from desiring an implant; “…some of them were still struggling, some of them didn’t have such good, they couldn’t hear on the phone. It’s a wide spectrum isn’t there…” (P14), while others rejected CI despite observing the positive experiences of others; “…the ones that I know that have had it done, it’s been brilliant for them, it’s changed their lives really” (P2).
Participants considered the conditions of the process of receiving an implant, including the necessity to commit to surgery and rehabilitation both emotionally and physically, including travelling to appointments; “I understand it’s very stressful, not only when you have the operation but also the constant to-ing and fro-ing to have the thing adjusted” (P1), “…if you go for the cochlear implant it’s one of the things you have to accept…” (P10). They also considered and expressed both positive and negative views on the physical appearance of the implant, although no participant expressed it as a significant barrier; “Well, you have to put up with that sort of thing, at least being a lady I can cover it with my hair” (P7). The majority of participants compared their ability to cope, most commonly with hearing aids but also other hearing technologies and coping techniques, against their perception of the outcome they would have with CI, forming a significant factor in their decision.
Theme – emotional response
The theme “Emotional response”, represented a leading motivator for seeking help, as participants commonly referred to the impact of hearing loss on their life to make decisions regarding CI. This links to the core category of “Weighing up priorities with CI”, with many participants expressing an expectation that CI would improve their life; “I don’t know…a new lease of life” (P5); “…all I could go by was a dream or hope that it would give me a better life” (P8).
Less directly, participants spoke of the emotional cost of their hearing loss, with fear of isolation a recurring factor; “I’m becoming more and more isolated” (P3), “…it wasn’t really a great quality of life for me because I was very isolated” (P8), alongside tiredness, fear and distress. This was dependant on participants’ personalities, with some expressing deep sorrow and anguish; “I mean…it’s like having a nightmare, and when you wake up it’s still there” (P7), “if my hearing had gone altogether and there was nothing they could have done, I probably would have given up living” (P12), while others remained more upbeat; “I’ve not let it overtake my life because I have so many things to be grateful for, that you know, I can’t dwell on the negative things” (P4), or used humour as a method of coping; “So I did say to them, if it didn’t work it’s wonderful not to listen to anyone…” (P9).
While the majority described these factors in relation to being prompted to seek further help and therefore assessment for CI, those who wished not to have CI still described similar feelings of isolation, fear, and distress; “…I’m becoming more and more isolated …” (P3), although two participants asserted that it was not having a significant impact on their lives to warrant CI; “I don’t think my hearing loss is impacting on my life so badly that I want to go down that route, with all its cons as well as pros” (P1), “…but I don’t let it rule my life at all” (P4).
Theme – living context and support
The theme “Living context and support’ provided context for participants in decision making, that aligned with the core category “Weighing up”. Participants considered their perception of the personal impact CI would have on them in terms of their current and future living context, the support they had available to them and the process they would have to undergo to receive an implant.
The variety of lifestyles and living contexts influenced the narrative of participants, with a major factor for younger participants being importance of employment status with regards to both taking a risk; “My whole job, career, work, life…is communication. Severe facial palsy can completely change a huge amount of things” (P3), and ability to continue performing their job; “I mean I could have said no of course but then my hearing would have gone down a lot and I want to be active, and keep my jobs going” (P11). Support within the workplace, or lack thereof, played a role in a participant’s desire to have CI; “I think it’s to do with my work…I don’t get much help at work, I have tried …it’s a bit of an ongoing struggle…I just find myself struggling…” (P5), taking into account support to overcome difficulties and support in the process of obtaining an implant; “Going off for the tests and everything, I just had the day off or would swap my shifts around” (P11).
Support from other sources played a significant role, with many participants discussing the importance of ability to cope based on support from family and friends; “…people who were family and friends who knew I’ve got a deafness problem would take care to face me when they speak to me and speak clearly…” (P10), with some participants considering this as a contributing factor for not needing CI. Participants had a range of views regarding travelling to a CI centre, from positive to negative, and ability to travel to CI centres was often dependant on family, friends, NHS or community support, with one participant noting that she was unable to travel due to a lack of support; “So…to be able to keep travelling to Bristol wouldn’t have been possible” (P2).
A significant consideration was the impact of living alone, which had both positive and negative impacts on decisions to have CI, such as the positive influence of desire to be able to live independently; “…that was another reason I wanted the cochlear implant, was so that I could live independently…” (P8), and the negative influence of factors such as lack of support in recovery from surgery; “…one is that I live on my own and the recovery from it is quite difficult and lengthy” (P1). Individuals’ social responsibilities had a similar pattern, demonstrated with the example of needing to function for the sake of family obligations, which acted as a barrier due to the demands of the CI process; “I have grandchildren in London who require looking after as well…so it would be very inconvenient for me to be out of action” (P1), and a trigger to seek help to continue meeting said obligations.
Theme – information needs and sources
The theme “Information needs and sources” is a further element of context in decision making, emerged through participant discussion of concordance and discordance with audiology, CI centre and ENT staff. This links clearly to the core category of “Weighing up priorities with CI”, given that participants’ perception of CI is influenced heavily by the information they receive from multiple sources including the aforementioned healthcare staff, peers and the media.
The majority of participants spoke positively concerning NHS staff, with various commendations such as finding staff to be helpful, trustworthy, and supportive, with minimal direct discordance with staff members. However, many discussed discordance with the NHS generally, including waiting times, appointment lengths, lack of options and use of resources; “…sometimes it’s terribly difficult to get to see them” (P2), “I want to speak to the chairman, why are you changing the contracts with hearing aids, you’re wasting money” (P9), and eight participants considered or used private healthcare for these reasons. An element of discordance with healthcare staff was noted in relation to the theme “Social Identity”, whereby some participants expressed dissatisfaction in being treated by staff who did not have a hearing loss, described further in the “Social Identity” theme section.
The level of information provision as well as its source arose as a factor in participants’ decisions. Information levels varied dependant on the stage of the CI process the participant was in, which inevitably influenced satisfaction levels; “He knows the question I am giving, but he could not deliver the answer” (P9), “I’m aware of it, if my circumstances change I’m aware of what is available there, which is good” (P4). A recurring factor was the importance of the source of information, and the majority of participants discussed others’ experiences with CI and the general positive influence of subjective information; “…in terms of the post-operational experience, I would trust the people who’ve had it…” (P1).
Theme – consideration of risk
The “Consideration of risk” theme formed the second most influential and wide reaching element of context for participants in decision making besides the core category “Weighing up priorities with CI”, with which it was closely intertwined. Participants were aware of a wide range of risks including those resulting from surgery, health, unknown outcome with a CI, loss of residual hearing and irreversibility, and linked these risks to their living context, future, and quality of life. A key component of decision making was a comparison exercise between the cost and impact of the risk compared with their current difficulties and the potential positive outcome they perceived that they may receive with CI, with mixed feelings over whether this was worth the risk. This included both positive impressions; “…well, it’s something that’s going to be a wonderful thing if it works and therefore it’s worth the risk…” (P7); “I just felt I’ve got two choices, either take it or leave it, I’m going to either be completely cut off for the rest of my life or go for it” (P12), and negative impressions; “…I feel I may be just sort of taking the wrong chance to have anything done like that” (P2), playing an important role in the decision-making process.
Concern levels were highly variable and appeared to be influenced by different personalities, such as those with positive outlooks; “And I’m a positive person, my glass is always half full, not half empty” (P15), and those who were more easily distressed; “It was terrifying, honestly, I was quite morbid in the lead up…” (P8).
Theme – social identity
The categories of the theme of “Social identity” were often expressed passionately by participants. Linking this to the core category “Personal feelings, knowledge and anticipation of CI”, participants placed their view of how CI would impact them personally in the context of their identity as a hearing or Deaf/deaf person, such as desire to be “normal”; “Just because I wanted to be able to live a normal life. I just felt that the world was predominantly hearing…” (P8), or perceiving CI as conflicting with Deaf culture; “And so it took me a long long time before I plucked up the courage after, to admit that I had one” (P7).
Very few participants felt aligned fully with the Deaf community, with just one participant actively seeking to embrace Deaf culture as opposed to exploring CI further after a previous unsuccessful experience; “I feel now I’m with Deaf people rather than hearing” (P6), although three others considered embracing elements of Deaf culture, such as use of sign language as an alternative to CI; “I know how to do sign language, that’s not a problem. I can do sign language, not a problem, lip reading is not a problem, if it comes to that” (P9).
A clear message was the impact of discordance between participants and others without hearing loss, which was expressed in some guise by all participants. Some examples of this are discussion of barriers to living with hearing loss in a “hearing world”, experiences of discrimination, lack of understanding of issues and subsequent lack of help coping with hearing loss. The latter was significant when discussing experiences with healthcare staff, with a number of participants discussing experiences of “hearing” staff not understanding or appreciating issues and expressing a preference to be seen by deaf staff; “…I asked for someone in audiology who is deaf and can understand what I’m talking about, because a deaf person has experience and knows what it is better than a hearing person” (P9).
Finally, participants described different stages of acceptance of their hearing loss and the impact this has on their decisions regarding their care pathway, such as embracing use of hearing technologies or potential acceptance of rejecting hearing technologies to “go silent”; “I said, I go silent. I just go completely deaf. That’s the end for me” (P9).
Theme – future planning
As a strategy for decision making, the impact of the “Future planning” influenced choice in both groups of participants, and was linked to the core category “Weighing up priorities with CI” in that participants considered their future with or without CI based on how they perceived the implant would impact them personally.
Three participants spoke of not wishing to have or delaying having CI given the potential for technological or scientific advancements, “I think I was rather hoping that stem cell would come out for hearing loss, and that because I’ve got a hereditary disability, I thought well maybe stem, you know, things are happening, technology’s different” (P14), although one participant remarked that “…you can’t put your life on hold just on the possibility that something might come out…” (P8), indicating that consideration of current difficulties took priority over the advantages of waiting. Concern about future deterioration of hearing acted as an immediate trigger to seek CI; “Yes, obviously it wasn’t going to get any better” (P10), but three participants indicated that they would consider waiting for deterioration before considering CI, despite their current difficulties; “…if my hearing deteriorates considerably more and I know it’s bad at the moment then obviously I may go down that route” (P4).
Many considered the impact of their decision on their future life, taking into account factors such as age, health and potential restrictions on activities, such as one participant wishing to attend university; “…there’s no way I could have gone to uni without it, just no way” (P8). Three of the participants who declined to have CI spoke of the potential to go down the route in the future, indicating that their current decision is not permanent and remains open; “…but I wouldn’t discount it permanently…” (P1).
Theme – consequences
The theme of “Consequences” revealed multiple factors that contribute to the overall satisfaction of a participant with the outcome of the option they chose. This was influenced by the core category of “Weighing up priorities with CI”, with participants linking their outcomes to their perception and expectations of the implant and the process of receiving one.
Four of the five participants who had experienced CI were positive about their choice and often described their reliance on the implant; “…it’s made a very big difference to my life, I can’t speak for anyone else but it really has” (P14), “I mean if you took me off them now I don’t know what I’d do, I’d go mad” (P12), “…yeah so I need my hearing, and this has made an enormous difference” (P11). These participants did describe continuing difficulties such as listening to music, group conversations and hearing in background noise, and discussed negative elements of the process of obtaining an implant, such as difficulty recovering from surgery, but were generally positive about the choice. Only one participant with an implant had abandoned use due to poor sound quality; “[I thought] that would be much better sound than my hearing aid, obviously it wasn’t…no. When I first hear the sound, I couldn’t believe it… I was like oh my god, get that thing off! It was so loud, yes…very very loud” (P6).
One participant had experienced device failure at the first attempt at switch on, although he remained positive despite his disappointment. Of the five participants who actively rejected the option of CI (including the participant who used one historically), all described the negative impact of hearing loss and their continuing difficulties to different degrees, adding weight to the argument that the decision is multifactorial and not solely dependent on quality of life and ability to cope. Finally, one participant was not eligible for CI but expressed determination to continue being assessed until she was accepted.
Core category
The core category identified, “Weighing up priorities with CI”, was the core of the decision-making process because of its meaningful influence on the uptake of CI, in concurrence with the other themes, in all participants. The other themes both shaped and were influenced by the core category, and thus were closely interlinked. Participants considered their perception, hopes, expectations and negative impressions regarding CI in the context of these other factors, considering areas strongly linked to their “lifeworld” (Habermas Citation1987) such as potential social, financial and contextual gains and costs. This links robustly to the second most cogent theme, “Consideration of risk”, which participants used to decide whether their “Priorities with CI” would outweigh potential downsides e.g. impacts on their living context from negative surgical side effects, such as employment and ability to support family. See for summary of the theoretical framework.
Discussion
The framework generated is the first of its kind in the literature to set out the decision-making process, with a firm grounding in data from patients at the heart of the process. The framework is broad out of necessity to encompass the varied contextual and therefore highly individual factors that patients consider, which was captured comprehensively through the wide range of lifestyles, ages, genders, family and living contexts in the study population.
A clear theme generated from the results was the importance of the patient’s lifeworld, which formed and influenced all elements of the framework, from the time of deciding to seek help, through to factors considered in decision making, and finally in the strategies used to cope with the decision. Habermas’ theory of communicative action discusses three dimensions of the patients’ lifeworld; objective, social and subjective (Walseth and Schei Citation2011). The results of this study clearly demonstrate these dimensions in action, and the complexity of factors in decision making shows evidently the influence of social and subjective domains which may be underappreciated by clinicians. The social dimension differs from the paediatric literature where decisions are made in advocacy (e.g. Fitzpatrick, Jacques, and Neuss Citation2011) – here it is the relative burden to others of becoming a hospital patient that influences decision making. Caring and support roles were discussed as a responsibility to consider against the potential to pursue CI. This was clear from participants’ discussion of discordance and misunderstanding between clinicians and themselves, such as perceiving that a deaf member of staff would understand their issues more than a hearing clinician; “…I asked for someone in audiology who is deaf and can understand what I’m talking about, because a deaf person has experience and knows what it is better than a hearing person” (p. 9, 67–69).
Understanding the importance patients place on their interactions with healthcare staff, whether positive or negative, corresponds with the importance of communication and shared decision making in audiology, and the need to overcome pragmatics in interactions to achieve this (Walseth and Schei Citation2011). It is already established that conflict between the voice of medicine and the voice of the patient, concerning their lifeworld, is significant in chronic illness and disability, and causes poorer outcomes (Barry et al. Citation2001). It is hoped that the results of this study can be used to improve dialogue between clinicians and CI candidates, in information provision and practical, emotional and social support, encouraging provision of a “lifeworld-led care” that humanises and empowers patients (Todres, Galvin, and Dahlberg Citation2007) in keeping with the aims of the NHS constitution (Department of Health Citation2015).
The findings of this study reflect the decision making factors briefly speculated by Raine et al. (Citation2016), who correctly proposed that patients consider health and surgical risks and influence of loved ones in practical and emotional support with hearing loss, and acknowledge the consequences of age on capacity. Raine et al. (Citation2016) proposed lack of awareness as an influencing factor for decision making, but the majority of participants of the present study appeared sufficiently informed to make decisions regarding their care. The results of this study both support and conflict the results of a study by Hixon et al. (Citation2016) demonstrating reduced uptake of CI with increasing geographic distance from a CI centre, with only one participant considering herself physically unable to travel to receive CI and therefore preventing her from pursuing it. In this study, travelling was considered a negative factor by nine participants, including both those who accepted and rejected CI.
Comparisons can be made to literature discussing parental decisions for the paediatric CI candidate population, which generally support the findings of the present study, although the differences between parental vs. personal decisions and the differences in the lifeworld of a child and an adult must be acknowledged. When considering the core category found in this study, “Weighing up priorities with CI”, some sub categories inherently conflict with paediatric CI decision making, such as “ability to cope prior to CI” which generally would not apply to parents given the time scales of paediatric CI compared to adults. However, other sub categories of the core category alongside wider established themes were supported and replicated unequivocally in the literature. This included elements such as conditions of the CI process, related to the theme “Living Context and Support”, which was demonstrated as inherent to the decision making process by Yang, Reilly, and Preciado (Citation2018), who found that barriers to paediatric CI access include “pragmatics” such as taking time off work, and ability to navigate the healthcare system, aligning with the theme “Information Needs and Sources”; reflecting that parental and personal decisions are similarly impacted by healthcare system factors.
Studies by Li, Bain, and Steinberg (Citation2004), Hyde, Punch, and Komesaroff (Citation2010), Hardonk et al. (Citation2011) and Chang (2017) show that parental decisions have strong basis in topics related to Deaf/deaf culture, such as ability to communicate, use of sign language, importance of Deaf identity and significance of conforming in a hearing society, which aligns with the theme found in this study, “Social Identity”. Parents in the aforementioned studies considered Deaf culture with greater emphasis than findings of this study, although this is likely due to low representation of Deaf-identifying participants in the study population.
Linked to beliefs relating to Deaf culture, parental decisions are largely influenced by a parent’s hopes, expectations and aspirations for their child’s future, aligning with the themes “Future planning” and “Quality of life” established in this study, whereby participants reflected on and justified their decision based on their view of their future with or without CI (Li, Bain, and Steinberg Citation2004; Hyde, Punch, and Komesaroff Citation2010; Hardonk et al. Citation2011). The literature also establishes similar thought processes in parents regarding the “Consideration of risk” for their children, whereby parents considered potential costs and benefits, forming an important element of the decision-making process as found in this study (Hardonk et al. Citation2011; De Souza Vieira et al. Citation2014).
Overall, the existing literature supports the findings of this study in regards to decision making being complex, multifactorial and highly personal to patients in the context of their lived experience (Archbold et al. Citation2006; De Souza Vieira et al. Citation2014). Broadly, the results of the studies described above show very close similarities between parental decisions and the results of the present study, suggesting fittingness of our findings.
Use of snowball sampling was necessary due to the limited time frame of the study, difficulty accessing long term (>2 years) implant users from clinical advertisement, and the small population being studied. Although snowball sampling has advantages such as fostering trust and therefore improving uptake of participants to the study, it may have induced selection bias in the data (Shaghaghi, Bhopal, and Sheikh Citation2011), thus producing data that represents socially active participants with similar characteristics (Magnani et al. Citation2005). This may have particularly excluded those who have difficulty socialising due to their hearing loss, or those who do not or cannot attend local CI support groups such as older or disabled people or those without living support (Shaghaghi, Bhopal, and Sheikh Citation2011).
The recruited sample was notably limited in representation of the Deaf community, younger participants (≤40 years), and those who rejected CI. The general population of Gloucestershire from which the sample was drawn should also be considered, e.g. it has a lower non-white British population, higher average education levels and higher employment levels when compared to national standards (Li Citation2013). The National Health Service context is important in that patients do not incur direct cost for their implant, upgrades or care. Nonetheless, the framework is likely to apply to other populations within the UK and internationally. Although the perspective of the sample in question was captured sufficiently to achieve data saturation, this was limited to the recruited population and may be excluding further information that could be gleaned if recruitment continued to include a wider range of participants (Sadler et al. Citation2010).
Conclusions
As the first research of its kind in the adult CI candidate population, the present study proposes a model to be investigated further to explain why individuals choose to either be implanted or not. This model suggests that the process of weighing up is one of integration of what Habermas (Citation1987) refers to as the objective world (in which medical facts and indicators for amplification) meets the subjective world of the patient (with intentions, beliefs and emotions). Our model describes this process of integration as active and impactful on uptake and use of services.
Figure 1. The theoretical framework for decision making in adults eligible for cochlear implantation.
Declaration of interest
No potential conflict of interest was reported by the authors.
References
- Action on Hearing Loss. 2015. “Hearing matters.” London: Action on Hearing Loss. https://www.actiononhearingloss.org.uk/how-we-help/information-and-resources/publications/research-reports/hearing-matters-report/
- Appelbaum, E. N., S. S. Yoo, R. A. Perera, and D. H. Coelho. 2017. “Duration of Eligibility Prior to Cochlear Implantation: Have We Made Any Progress?” Otology & Neurotology 38 (9): 1273–1277. doi:10.1097/MAO.0000000000001544
- Archbold, S., T. Sach, C. O’Neill, M. Lutman, and S. Gregory. 2006. “Deciding to Have a Cochlear Implant and Subsequent after-Care: Parental Perspectives.” Deafness & Education International 8 (4): 190–206. doi:10.1179/146431506790560094
- Barry, C. A., F. A. Stevenson, N. Britten, B. Barber, and C. P. Bradley. 2001. “Giving Voice to the Lifeworld. More Humane, More Effective Medical Care? A Qualitative Study of Doctor–Patient Communication in General Practice.” Social Science & Medicine 53 (4): 487–505. doi:10.1016/S0277-9536(00)00351-8
- Beyea, J. A., K. P. McMullen, M. S. Harris, D. M. Houston, J. M. Martin, V. A. Bolster, O. F. Adunka, and A. C. Moberly. 2016. “Cochlear Implants in Adults: Effects of Age and Duration of Deafness on Speech Recognition.” Otology & Neurotology 37 (9): 1238–1245. doi:10.1097/MAO.0000000000001162
- Birks, M., and J. Mills. 2015. Grounded Theory: A Practical Guide. 2nd ed. London: Sage. ISBN 978-1-4462-9577-9
- Blamey, P., F. Artieres, D. Baskent, F. Bergeron, A. Beynon, E. Burke, N. Dillier, et al. 2013. “Factors Affecting Auditory Performance of Postlinguistically Deaf Adults Using Cochlear Implants: An Update with 2251 Patients.” Audiology and Neurotology 18 (1): 36–47. doi:10.1159/000343189
- Bond, M., S. Mealing, R. Anderson, J. Elston, G. Weiner, RS. Taylor, M. Hoyle, Z. Liu, A. Price, and K. Stein. 2009. “The Effectiveness and Cost-Effectiveness of Cochlear Implants for Severe to Profound Deafness in Children and Adults: A Systematic Review and Economic Model.” Health Technology Assessment 13 (44): 1–330. doi:10.3310/hta13440
- Bosdriesz, J. R., M. Stam, C. Smits, and S. E. Kramer. 2017. “Psychosocial Health of Cochlear Implant Users Compared to That of Adults with and without Hearing Aids: Results of a Nationwide Cohort Study.” Clinical Otolaryngology 43 (3): 828–834. doi:10.1111/coa.13055
- Carlsson, P. I., J. Hjaldahl, A. Magnuson, E. Ternevall, M. Edén, Å. Skagerstrand, and R. Jönsson. 2015. “Severe to Profound Hearing Impairment: Quality of Life, Psychosocial Consequences and Audiological Rehabilitation.” Disability and Rehabilitation 37 (20): 1849–1856. doi:10.3109/09638288.2014.982833
- Chang, P. F. 2017. “Breaking the Sound Barrier: Exploring Parents’ Decision-Making Process of Cochlear Implants for Their Children.” Patient Education and Counseling 100 (8): 1544–1551. doi:10.1016/j.pec.2017.03.005
- Chundu, S., and S. L. Flynn. 2014. “Audiogram and Cochlear Implant Candidacy – UK Perspective.” Cochlear Implants International 15 (4): 241–244. doi:10.1179/1754762813Y.0000000052
- Chundu, S., and N. Stephens. 2013. “Patients’ Involvement in Choosing a Cochlear Implant.” Cochlear Implants International 14 (3): 165–168. doi:10.1179/1754762812Y.0000000010
- Clamp, P. J., T. Rotchell, J. Maddocks, and P. J. Robinson. 2013. “What Factors Influence Patient and Parent Choice of Cochlear Implant Model for Children?” Cochlear Implants International 14 (3): 130–134. doi:10.1179/1754762812Y.0000000007
- Cohen, S. M., R. F. Labadie, M. S. Dietrich, and D. S. Haynes. 2004. “Quality of Life in Hearing-Impaired Adults: The Role of Cochlear Implants and Hearing Aids.” Otolaryngology–Head and Neck Surgery 131 (4): 413–422. doi:10.1016/j.otohns.2004.03.026
- Corbin, J. M., and A. Strauss. 1990. “Grounded Theory Research: Procedures, Canons, and Evaluative Criteria.” Qualitative Sociology 13 (1): 3–21. doi:10.1007/BF00988593
- Crowson, M. G., Y. R. Semenov, D. L. Tucci, and J. K. Niparko. 2017. “Quality of Life and Cost-Effectiveness of Cochlear Implants: A Narrative Review.” Audiology and Neurotology 22 (4–5): 236–258. doi:10.1159/000481767
- Department of Health. 2015. The NHS Constitution: The NHS Belongs to Us All. London: Department of Health. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/480482/NHS_Constitution_WEB.pdf
- De Raeve, L., and R. Van Hardeveld. 2013. “Prevalence of Cochlear Implants in Europe: What Do We Know and What Can We Expect?” Journal of Hearing Science 3 (4): 9–16. https://journalofhearingscience.com/media/attachments/2017/08/01/889707.pdf
- De Souza Vieira, S., M. C. Bevilacqua, N. M. L. A. Ferreira, and G. Dupas. 2014. “Cochlear Implant: The Complexity Involved in the Decision Making Process by the Family.” Revista Latino-Americana de Enfermagem 22 (3): 415–424. doi:10.1590/0104-1169.3044.2432
- Elwood, S. A., and D. G. Martin. 2000. “Placing” Interviews: Location and Scales of Power in Qualitative Research.” The Professional Geographer 52 (4): 649–657. doi:10.1111/0033-0124.00253
- Fitzpatrick, E. M., J. Jacques, and D. Neuss. 2011. “Parental Perspectives on Decision-Making and Outcomes in Pediatric Bilateral Cochlear Implantation.” International Journal of Audiology 50 (10): 679–687. doi:10.3109/14992027.2011.590823
- Francis, H. W., N. Chee, J. Yeagle, A. Cheng, and J. K. Niparko. 2002. “Impact of Cochlear Implants on the Functional Health Status of Older Adults.” The Laryngoscope 112 (8): 1482–1488. doi:10.1097/00005537-200208000-00028
- Geyer, M., F. K. Seymour, L. Stott, C. Lynch, M. Beukes, W. Aleksy, and J. M. Graham. 2006. “How we Do It: Patient Participation in Cochlear Implant Selection.” Clinical Otolaryngology 31 (1): 56–61. doi:10.1111/j.1749-4486.2006.01127.x
- Habermas, J. 1987. The Theory of Communicative Action, Volume 2: Lifeworld and System: A Critique of Functionalist Reason. 3rd ed. Boston, MA: Beacon Press. ISBN 080701401X 9780807014011
- Hallberg, L. R. M. 2006. “The “Core Category” of Grounded Theory: Making Constant Comparisons.” International Journal of Qualitative Studies on Health and Well-Being 1 (3): 141–148. doi:10.1080/17482620600858399
- Hardonk, S., S. Daniels, G. Desnerck, G. Loots, G. Van Hove, E. Van Kerschaver, H. B. Sigurjónsdóttir, C. Vanroelen, and F. Louckx. 2011. “Deaf Parents and Pediatric Cochlear Implantation: An Exploration of the Decision-Making Process.” American Annals of the Deaf 156 (3): 290–304. doi:10.1353/aad.2011.0027
- Hiel, A. L., J. M. Gerard, M. Decat, and N. Deggouj. 2016. “Is Age a Limiting Factor for Adaptation to Cochlear Implant?” European Archives of Oto-Rhino-Laryngology 273 (9): 2495–2502. doi:10.1007/s00405-015-3849-5
- Hixon, B., S. Chan, M. Adkins, J. B. Shinn, and M. L. Bush. 2016. “Timing and Impact of Hearing Healthcare in Adult Cochlear Implant Recipients: A Rural-Urban Comparison.” Otology & Neurotology 37 (9): 1320–1324. doi:10.1097/MAO.0000000000001197
- Hyde, M., R. Punch, and L. Komesaroff. 2010. “Coming to a Decision about Cochlear Implantation: Parents Making Choices for Their Deaf Children.” Journal of Deaf Studies and Deaf Education 15 (2): 162–178. doi:10.1093/deafed/enq004
- Knudsen, L. V., A. Laplante-Lévesque, L. Jones, J. E. Preminger, C. Nielsen, T. Lunner, L. Hickson, G. Naylor, and S. E. Kramer. 2012. “Conducting Qualitative Research in Audiology: A Tutorial.” International Journal of Audiology 51 (2): 83–92. doi:10.3109/14992027.2011.606283
- Lawrence, J., and U. Tar. 2013. “The Use of Grounded Theory Technique as a Practical Tool for Qualitative Data Collection and Analysis.” The Electronic Journal of Business Research Methods 11 (1): 29–40. https://pdfs.semanticscholar.org/1255/fb6a561e83eb23fad8490dfebd3c34b1a596.pdf
- Li, L. 2013. Census Briefing for Commissioners. Gloucester, England: Gloucestershire County Council, https://www.gloucestershire.gov.uk/media/1521102/census_briefing_for_commissioners_-_full_report.pdf
- Li, Y., L. Bain, and A. G. Steinberg. 2004. “Parental Decision-Making in Considering Cochlear Implant Technology for a Deaf Child.” International Journal of Pediatric Otorhinolaryngology 68 (8): 1027–1038. doi:10.1016/j.ijporl.2004.03.010
- Magnani, R., K. Sabin, T. Saidel, and D. Heckathorn. 2005. “Review of Sampling Hard-to-Reach and Hidden Populations for HIV Surveillance.” AIDS 19 (2): S67–S72. doi:10.1097/01.aids.0000172879.20628.e1
- NICE. 2009. Cochlear Implants for Children and Adults with Severe to Profound Deafness: Technology Appraisal Guidance. London: NICE. https://www.nice.org.uk/guidance/ta166
- Okubo, S., M. Takahashi, and I. Kai. 2008. “How Japanese Parents of Deaf Children Arrive at Decisions Regarding Pediatric Cochlear Implantation Surgery: A Qualitative Study.” Social Science & Medicine 66 (12): 2436–2447. doi:10.1016/j.socscimed.2008.02.013
- Raine, C. 2013. “Cochlear Implants in the United Kingdom: Awareness and Utilization.” Cochlear Implants International 14 (1): S32–S37. doi:10.1179/1467010013Z.00000000077
- Raine, C., H. Atkinson, DR. Strachan, and JM. Martin. 2016. “Access to Cochlear Implants: Time to Reflect.” Cochlear Implants International 17 (1): 42–46. doi:10.1080/14670100.2016.1155808
- Sadler, G. R., H. C. Lee, R. S. H. Lim, and J. Fullerton. 2010. “Recruiting Hard-to-Reach United States Population Sub-Groups via Adaptations of Snowball Sampling Strategy.” Nursing & Health Sciences 12 (3): 369–374. doi:10.1111/j.1442-2018.2010.00541.x
- Shaghaghi, A., R. S. Bhopal, and A. Sheikh. 2011. “Approaches to Recruiting ‘Hard-to-Reach’ Populations into Research: A Review of the Literature.” Health Promotion Perspectives 1 (2): 86–94. doi:10.5681%2Fhpp.2011.009
- Sivell, S., H. Prout, N. Hopewell-Kelly, J. Baillie, A. Byrne, M. Edwards, E. Harrop, S. Noble, C. Sampson, and A. Nelson. 2015. “Considerations and Recommendations for Conducting Qualitative Research Interviews with Palliative and End-of-Life Care Patients in the Home Setting: A Consensus Paper.” BMJ Supportive & Palliative Care 9 (1): e14. doi:10.1136/bmjspcare-2015-000892
- Smith, J., and J. Firth. 2011. “Qualitative Data Analysis: The Framework Approach.” Nurse Researcher 18 (2): 52–62. doi:10.7748/nr2011.01.18.2.52.c8284
- Sorkin, D. L. 2013. “Cochlear Implantation in the World’s Largest Medical Device Market: Utilization and Awareness of Cochlear Implants in the United States.” Cochlear Implants International 14 (1): S12–S12. doi:10.1179/1467010013Z.00000000076
- Todres, L., K. Galvin, and K. Dahlberg. 2007. “Lifeworld-Led Healthcare: Revisiting a Humanising Philosophy That Integrates Emerging Trends.” Medicine, Health Care and Philosophy 10 (1): 53–63. doi:10.1007/s11019-006-9012-8
- Urquhart, C., H. Lehmann, and M. D. Myers. 2009. “Putting the ‘Theory’ Back into Grounded Theory: Guidelines for Grounded Theory Studies in Information Systems.” Information Systems Journal 20 (4): 357–381. doi:10.1111/j.1365-2575.2009.00328.x
- Vickers, D., L. De Raeve, and J. Graham. 2016. “International Survey of Cochlear Implant Candidacy.” Cochlear Implants International 17 (1): 36–41. doi:10.1080/14670100.2016.1155809
- Walseth, L. T., and E. Schei. 2011. “Effecting Change through Dialogue: Habermas’ Theory of Communicative Action as a Tool in Medical Lifestyle Interventions.” Medicine, Health Care and Philosophy 14 (1): 81–90. doi:10.1007/s11019-010-9260-5
- Yang, C. Q., B. K. Reilly, and D. A. Preciado. 2018. “Barriers to Pediatric Cochlear Implantation: A Parental Survey.” International Journal of Pediatric Otorhinolaryngology 104: 224–227. doi:10.1016/j.ijporl.2017.11.026