
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
The surge in aging societies has increased the relevance of retirement as a research topic. Utilizing the public data obtained from the China Family Panel Studies, this paper applies a regression discontinuity approach to assess the impact of China’s current Public Pension Program on the medical expenditures of the elderly. The results reveal that the Public Pension Program increases out-of-pocket medical expenditures, hospitalization expenditures, and other injury and illness expenses. The results also report that being insured by Basic Social Health Insurance has a mitigating effect on the medical expenditures of the elderly; furthermore, there are significant differences in the use of medical resources between regions and urban and rural areas in China. Therefore, ensuring the sustainability of pension funds and social health insurance funds and developing customized private insurance according to areas can play a positive role in improving the use of medical resources and relieving the medical burden on the elderly population.
1. Introduction
More and more countries are falling into the category of “aging societies”; consequently, retirement has attained great significance as an area of study. Retirement is an important milestone and a determinant of a vast population’s quality of life. It also reflects the state of public health and the utilization of health care resources in a country (Levi & Kène, Citation2018). The pension provided by the Public Pension Program in China is about 50% of the pre-retirement salary on the national average. Owing to a gradual decline in birth rates and a simultaneous increase in life expectancy rates, over 12% of China’s population is aged 60 years or older, exceeding the 10% threshold set by the United Nations for an aging society. By 2019, China’s elderly population dependency ratio had already spiraled to 17.8% (http://www.stats.gov.cn/). Traditional family care is gradually deteriorating in China as a result of the country’s rapidly aging population, coupled with its under-developed pension system (Chen, Dennis, Tang, & Wu, Citation2017; Wu & Li, Citation2014).
Although elderly people approaching retirement typically possess sufficient property, savings, and pension assets, unexpected fluctuations in health conditions, asset prices, and health insurance plans can pose challenges for retired senior citizens to retain their savings and assets (Dayaram & Mcguire, Citation2019). The incentive benefits offered upon retirement are typically more inclined toward those from the lower income groups as well as individuals with limited access to annuity entitlements and supplementary health insurance (Rust & Phelan, Citation1997). People without pensions are more likely to retire early, which places greater demands on pre-retirement savings. These savings are needed to meet various expenses after retirement. A surge in the aging population increases the number of pension payments, warrants the establishment of health and long-term care insurance programs, and exerts significant pressure on the health care system (Gong, Kendig, & He, Citation2016; Kumagai & Takabayashi, Citation2008).
The health conditions of individuals post retirement determine the medical expenses that need to allocated toward elderly healthcare. Although this study conducted an assessment of the impact of China’s current Public Pension Program on the medical expenditures of the elderly, this evaluation is still incomplete. This research primarily applies the regression discontinuity approach to identify strategies to control the endogenous problems faced by the elderly in receiving their pensions. It also aims to verify whether pensions can play a role in the utilization of medical and health services for the elderly in China.
2. Literature review
As the rate of aging and medical expenditures continue to increase, understanding the medical expenditures of the retirees under public pension programs is crucial. Public pension programs not only provide basic security for workers after retirement but also resolve any inequalities in terms of health conditions and socioeconomic statuses that may have existed among employees before their retirement (Szabó, Allen, Stephens, & Alpass, Citation2018). Moreover, Kail (Citation2016) found that individuals covered by stable insurance plans tend to be healthier upon retirement.
Social insurance contributions paid by employees finance the public social security system. However, controlling the increase in medical expenditures and reducing the burden on public pensions under the pay-as-you-go system and aging societies remains a concern for many scholars. Some studies have demonstrated that per capita medical expenditures on individuals aged 65 and above are higher than those incurred for other age groups (Olaniyan, Olayiwola, & Odubunmi, Citation2011), and out-of-pocket expenditures rise sharply for the elderly toward the end of life (Fahle, Mcgarry, & Skinner, Citation2016; Wei & Zhou, Citation2019). The increase in medical expenditures has put enormous pressure on the income of elderly households and forced them to reduce their spending in other areas. In addition, increased medical expenditures subsequently increase public pension benefits and social insurance burden rates (Kumagai & Takabayashi, Citation2008). Moreover, pensioners who have contributed less to the public health insurance system have higher health care expenditures (Fourcade, Duval, & Lardellier, Citation2013). Differences in the treatment and utilization of medical and health services among patients are overwhelmingly dependent on affordability (Xian et al., Citation1944; Zhao, Zhang, Fu, Wang, & Zhang, Citation2020). High out-of-pocket costs can limit people’s access to health care (Krůtilová, Citation2016). Hence, the population in poverty often has limited access to health services and treatment due to financial constraints.
In terms of reducing medical expenditures, Zhang, Nikoloski, and Mossialos (Citation2017) found that the expansion of health insurance coverage had a positive effect on lowering out-of-pocket expenditures for inpatients. However, Bruno and Melanie (Citation2013) argue that the expansion of coverage may also reduce the technical efficiency of healthcare services. Moreover, private health insurance can play an essential role in transferring the risk of illness, specifically by reimbursing the medical expenses incurred by the insured person for the treatment of illnesses during the insurance period, which is more beneficial for middle-aged and older people (Baggio et al., Citation2018; Kwon, Park, & Mcbride, Citation2018). Studies have also confirmed that supplementary health insurance can play a crucial role in providing the low-income populations with access to health services (Carré, Thomas, Jusot, Wittwer, & Christelle, Citation2019). Our study focuses on the impact of the Public Pension Program on the medical expenditures of the elderly and adopts a different research methodology from existing studies to draw empirical conclusions and provide a valuable reference for policy reform.
3. Materials and methods
3.1. Data
The analysis was based on the most recently obtained data from the 2018 survey public data conducted by the China Family Panel Studies (CFPS). The CFPS is implemented by the Chinese Social Science Survey Center (ISSS) of Peking University. It aims to track and collect data at three levels – namely, the individual, familial, and community levels – to evaluate the changes in China’s society, economy, population, education, and health. Any researcher can use the relevant questionnaire and data after applying through the website (https://opendata.pku.edu.cn/dataverse/CFPS). The purpose of our paper was to explore the impact of the Public Pension Program on the medical expenditures of the elderly. Therefore, individuals who had been receiving their pensions from the Public Pension Program were included in the study, followed by other screening variables and samples. The final study comprised 7,303 samples.
3.2. Method
The ordinary least squares (OLS) is the general method used to estimate the impact of pension income on the medical expenditures incurred on the elderly:
where is medical expenditure for the elderly, and
indicates whether an individual is eligible for pension; that is, when individuals receive pension,
takes the value of 1, otherwise, the value of
is 0.
represents the effect of control variables. Individuals are not random in terms of pension receipts and medical expenditures. Income and expenditure are influenced by a wide range of factors such as individual characteristics and socioeconomic status. This makes it hard to control for all variables that may affect both pension receipts and medical expenditures. Moreover, the estimate of the coefficient
is biased in the case of the omission of variables. To study the impact of China’s current Public Pension Program on the medical expenditures of the elderly, this paper uses the regression discontinuity approach, a technique widely used in recent years to identify causal effects.
Under the statutory retirement age of 60, the pension was available after retirement, so the probability of receiving the pension near the age of 60 increased abruptly. Using the statutory retirement age as a breakpoint, we selected a control group and an experimental group near the breakpoint and identified the effects of treatment on the experimental group (comprising the individuals who receive the pension). China’s current retirement system allows for an early retirement scheme for employees who are seriously ill as well those grappling with disabilities or total incapacitation. Therefore, the retirement system only makes an exogenous jump in the probability of receiving the pension at the age specified in the policy; however, the probability of receiving the pension does not necessarily change from 0 to 1 at the breakpoint. The individual’s age only increases the probability of receiving the pension, so our paper uses the fuzzy regression discontinuity (FRD) regression model to estimate the average effect of the policy on “compilers” (i.e., those individuals whose forcing variable is above the threshold and have received the policy treatment) around the threshold:
Where is the treatment variable indicating whether an individual is eligible for pension, i.e., when individuals receive their pensions,
takes the value of 1, otherwise, its value is 0. Although satisfying the age condition
does not necessarily result in receipt of pension, it can be introduced into the health expenditure equation as an instrumental variable for pensions to control for the endogeneity of retirement decisions.
is the assignment variable (or the driver variable), wherein
represents the age of the individual.
EquationEquation (2)(2)
(2) represents the causal effect of pension income on
(medical expenditure), which is mentioned in EquationEquation (3)
(3)
(3) .
explains the local average treatment effect of pensions around the age breakpoint, and
is a polynomial function of
.
In this study, FRD is estimated by two-stage least squares (2SLS). Specifically, the one-stage regression equation can be expressed as:
where is the instrumental variable for processing state
. In the empirical analysis section, different bandwidths and multiple
forms are used to ensure the robustness of the results.
3.3. Variable descriptions
As delineated in , the explained variables include out-of-pocket medical expenses, hospitalization expenses, and injury and illness expenses. The explanatory variables include gender, residence in urban/rural areas, family size, household income, whether the individuals were insured for social health insurance, and regional variables.
Table 1. Description of variables
depicts the results of the descriptive statistics for the sample, reporting the means and Standard Deviation (SD) for all samples, receiving or not receiving pensions, respectively. The age range of the sample was 45–93. As indicated in , in the overall sample, there were more males than females and more individuals from rural than urban areas. In terms of family size, on average, most households were made up of 3–4 members. It was found that in terms of medical expenditure, individuals who received the pension spent more, on an average, on out-of-pocket medical expenses, hospitalization expenses, and other illness and injury expenses as compared to individuals without pensions. The rural population accounted for a relatively high proportion of the non-pensioned individuals. Individuals with pensions participated more actively in social health insurance than those without pensions.
Table 2. Descriptive summary
4. Results
4.1. The relationship between age and pension receipt
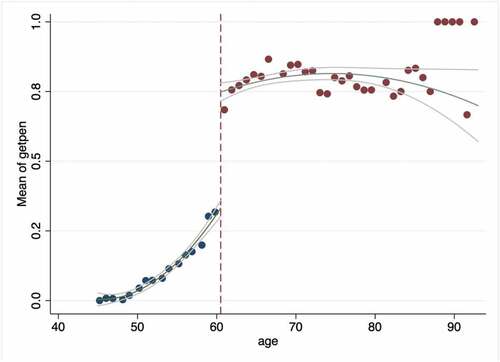
illustrates visually the relationship between the assignment variable (age) and the treatment variable (whether an individual is eligible for pension), which is also a one-stage regression in the FRD estimation. We concluded that in China, there has been a significant increase in the retirement rate of individuals having attained the statutory retirement age (Feng, Li, & Smith, Citation2020), with a clear jump point around age 60. Specifically, this jump point occurs at age 60.5, which is largely consistent with the general policy of pension being offered to individuals having completed 60 years of age. The slight deviation between 60 and 60.5 may be due to seasonality in the actual payment of pensions. For example, some local governments have the tendency to provide pensions to the current year’s retirees in the middle or at the end of the year.
Figure 1. Age and pension status.
The regression adds an age interaction term. D represents the general treatment status, 1 for over 60.5 years and 0 for under 60.5 years. The age control functions are age_left = age−60.5, and D_age_left = D× age_left, wherein the polynomials represent the age breakpoint difference. As reported in , regressions (1), (2), and (3) were performed using the rdrobustFootnote1 command in Stata to obtain the optimal bandwidth of 5.311. To check the robustness of our results, we set up three bandwidths: optimal bandwidth, 50 % optimal bandwidth, and double optimal bandwidth. The hypothesis that reaching retirement age increases the probability of receiving the pension is well-supported by the fact that almost all variables are highly significant at different bandwidths. At the optimal bandwidth, reaching age 60 increases the probability of receiving the pension by 35% and is highly significant at the 1% level.
Table 3. Impact of policy age on receiving pension
4.2. Pensions and medical expenditures
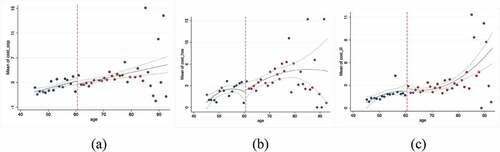
The study used a two-stage least squares approach to estimate the causal effect of pension income on medical expenditures. First, graphical analysis was used to determine whether the outcome variable jumps at the breakpoint. As shown in , out-of-pocket medical expenses, hospitalization expenses, and other injury and illness expenses jumped at the breakpoint.
Figure 2. Impact of pensions on medical expenditures: (a) cost_oop; (b) cost_hos; (c) cost_ill.
Next, reports the estimated results for the second stage with regard to different bandwidths (optimal bandwidth, 50% optimal bandwidth, and double optimal bandwidth). Regression controls other variables and polynomial functions of age. Overall, on a yearly basis, receiving pension can increase the out-of-pocket medical expenditure of the elderly by 1,942 yuan, hospitalization expenditures by 2,538 yuan, and other injury and illness expenses by 1,203 yuan under the optimal bandwidth. All increases are significant at the 1% level. The regression results under the 50% optimal bandwidth imply that pensions encourage the elderly to spend more each year on health care than the optimal bandwidth estimates. This is possibly because the effect is more significant as the optimal bandwidth decreases and the sample size on either side of the breakpoint decreases. According to the sample, the median monthly pension payment is 950 yuan, and the average is 1,475.66 yuan. According to the income of 950 yuan, the annual pension income is 11,400 yuan, which can cover the annual increase in medical expenditures.
Table 4. Impact of pensions on medical expenditures
4.3. Analysis of the heterogeneous treatment effect
4.3.1. Urban/rural residence
Owing to the differences in income, healthcare, and education levels between urban and rural areas in China, urban dwellers tend to have higher standards of living than individuals in rural areas. For the purpose of examining the effect of the Public Pension Program on the heterogeneity on health care expenditures between urban and rural households, the sample was divided into two sub-samples – urban and rural – for regression. As shown in , in terms of out-of-pocket medical expenditures, the 50% optimal bandwidth is more than double the annual expenditure in rural areas (6,142 yuan) than in urban areas (2,702 yuan). A possible explanation for this disparity is that unequal social insurance coverage leads to differences in healthcare utilization and health outcomes across socioeconomic groups (David, Dobkin, & Maestas, Citation2008).
Table 5. Impact of pensions on medical expenditures: Urban
Table 6. Impact of pensions on medical expenditures: Rural
In China, the urban and rural populations have two systems of social health insurance, with urban populations paying higher premiums and obtaining higher reimbursement rates and, therefore, incurring lower out-of-pocket health expenditures than those residing in rural areas. In terms of hospitalization expenditure, the optimal bandwidth is higher for urban expenditures than for the rural ones; however, the coefficient for the rural population is not significant. Urban areas also incur twice the amount of expenditures incurred by rural areas in terms of medical expenses other than that incurred from hospitalization. Pension incomes also vary greatly between urban and rural areas. The sample analysis revealed that the median pension in urban areas was 2,075.50 yuan per month with a mean value of 2,213.66 yuan, while the median pension in rural areas was 100 yuan per month with a mean value of 566.38 yuan. Therefore, the urban population incurs higher hospitalization and other medical expenses as compared to those incurred by individuals in rural areas. Moreover, the urban population usually has the awareness and additional financial wellbeing to purchase commercial health insurance and provide themselves with a higher level of medical protection.
4.3.2. Different regions
The inequality in and the unbalanced distribution of healthcare resources in China not only exists between rural and urban areas but also among different regions of the country depending on their economic development levels. For the purpose of regression analysis, the sample was classified into three sub-samples – namely, the east, middle, and west regions – to investigate the regional differences in the medical expenditures of the elderly under the Public Pension Program. (The details of the regressions are shown in Appendix ).
In the regressions with the optimal bandwidth, 50% optimal bandwidth and double optimal bandwidth, the highest expenditures were found in the eastern region with the optimal bandwidth. However, the results were not significant in the central and west regions in terms of out-of-pocket expenditures and those on other injury and illness expenses. Moreover, the hospitalization expenditure, 50% optimal bandwidth, was higher in the west than in the central region. This may be explained by the fact that the east region is significantly at a better position than the central and western regions in terms of household income status and level of medical development. There are still other selection biases – including differences in social health insurance in the deductible, reimbursement ratio, and cap line – that differ within the same region and may cause the regression to be insignificant.
4.3.3. Social health insurance
Whether or not an individual is covered by social health insurance also has a significant impact on residents’ medical expenditures. The impact of social health insurance on medical expenditure under the Public Pension Program was analyzed by dividing the sample into two parts according to whether the people were insured. As shown in , the elderly individuals who were insured for social health insurance had lower out-of-pocket medical expenses, hospitalization expenses, and other injury and illness expenses than those who were uninsured. However, only the expenditures on other injury and illness expenses were significant in both regressions under the optimal bandwidth (Model 37 and Model 46). This finding indicates that social health insurance could play a role in reducing residents’ expenses when seeking medical treatment for illness or accidental injuries.
Table 7. Impact of pensions on medical expenditures: Insured
Table 8. Impact of pensions on medical expenditures: Uninsured
4.4. Validity test of regression discontinuity estimation
4.4.1. Age manipulation test
Through the above analysis, this study used a variety of bandwidth settings, all of which derive consistent estimation results, indicating the robustness of the regression discontinuity (RD) estimation. The validity of the RD identification strategy requires that economic individuals cannot (at least completely) manipulate the assignment variable (i.e., age), and if the assignment variable can be manipulated, then the RD estimation is probably biased. This study uses the rdcont test introduced by Bugni and Canay (Citation2018), and the results are reported in . The p-value of the sample non-random test for breakpoint regression at the critical value is 0.307, which cannot reject the original hypothesis, indicating that the assignment variable (age) density function is a continuous function at the critical value and there is no human intervention.
Table 9. RDD non-randomized approximate sign test
4.4.2. Balance test of control variables
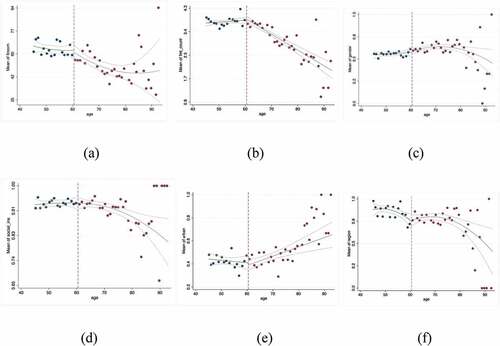
Another method to test the validity of the RD estimates is to assess the continuity of the control variables (Lee & Lemieux, Citation2010). Theoretically, if RD is valid, then the treatment variable (whether an individual is eligible for pension) should not be different before and after the breakpoint from the effect of other variables. First, the graphical analysis () demonstrates that the six control variables are continuous before and after the breakpoint.
Figure 3. Continuity test of control variables: (a) fincom; (b) fml_count; (c) gender; (d) social_ins; (e) urban; (f) region.
Next, use the estimation method to find out whether the estimated specific coefficient is significant. The regression sets the control variables as the dependent variables for the age breakpoints and then estimates the parameter estimates for different age bandwidths. reports the results of applying the first-order interaction term regression model to the covariate balance test. Column 5 shows the coefficients for the age breakpoints (age = 60.5 years). For these facts that have occurred before the age breakpoint and should not be restricted by pension age, the coefficient is not significant at the 10% level. This implies that the covariates in the model are not cut off near the driving variable and are not affected by retirement age, supporting the validity of the RD identification strategy. Three bandwidths were used to ensure the robustness of the test results.
Table 10. Continuity test of control variables
4.5. Placebo tests
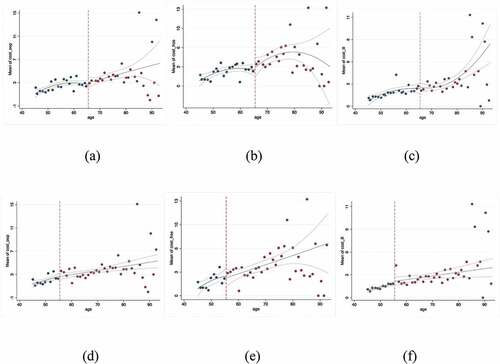
To ensure the robustness of the results, a placebo test was also applied. The idea was that changing the age breakpoint should not have a significant effect on the elderly’s medical expenditures. New age breakpoints of 65.5 years and 55.5 years, respectively, were set. If the effect of this breakpoint on medical expenditures was not significant, it would be more certain that the effect of changes in the elderly’s medical expenditures on pension income is not due to the heterogeneity brought about by the ages change.
illustrates the continuity of the dependent variables at the new age breakpoints. Out-of-pocket medical expenses, hospitalization expenses, and other injury and illness expenses are all continuous at the new breakpoint. Further regression estimates were performed using the age breakpoint as the main independent variable. reports the results of the placebo test with p-values greater than 0.1 for each coefficient. The table shows that the location of the new breakpoint does not have a significant effect on medical expenditure and the consumption of medical changes smoothly with age, so the RD estimate with a breakpoint of 60.5 years is valid.
Table 11. Placebo test
Figure 4. Placebo tests: (a) cost_oop; (b) cost_hos; (c) cost_ill; (d) cost_oop; (e) cost_hos; (f) cost_ill; (a)–(c) breakpoint age = 65.5 years; (d)–(f) breakpoint age = 55.5 years.
5. Discussion
Under the Public Pension Program, the elderly tends to spend pension more for medical consumption than before retirement. And our study found that the Public Pension Program increases out-of-pocket medical expenditures of the elderly by 1,942 yuan, hospitalization expenditures by 2,538 yuan, and other injury and illness expenses by 1,203 yuan, on a yearly basis. On the one hand, the increased demand for medical services may due to the physical condition of the elderly after retirement (Bíró & Elek, Citation2018; Calvo, Sarkisian, & Tamborini, Citation2012; Wallace, Haveman, & Wolfe, Citation2017); on the other hand, the complex and variable disease spectrum and rising healthcare costs have led to medical consumption comprising a large percentage of household consumption expenditures (Shai, Citation2018).
Another important finding is that, considering the imbalance in the distribution of medical resources and the differences in the level of economic development between regions, urban and rural areas in China, we carried out a heterogeneity analysis and concluded that in terms of out-of-pocket medical expenditures, the annual expenditures in rural areas (6,142 yuan) is more than double in urban areas (2,702 yuan). We also found that hospitalization expenditures are higher in the western region than in the central region. These findings support the view of Xian et al. (Citation1944) and David et al. (Citation2008) that inequalities in healthcare are greater in less economically developed regions. Unequal social insurance coverage leads to differences in healthcare utilization across socioeconomic groups. Furthermore, we find that individuals with social health insurance have lower medical expenditures, which should be attributed to the mitigating effect of social health insurance in terms of the residents’ medical expenditures.
Our study uses a regression discontinuity approach, which effectively avoids the problem of endogeneity and confirms the validity of the RD estimates through a series of tests. Undeniably, this study still has limitations. Although the RD regression has excellent internal validity, the findings cannot be generalized to other age groups in the population because only the elderly near the breakpoint are considered a part of the specific sample. The model yields only a local average treatment effect (Christelis, Georgarakos, & Anna, Citation2020).
The results of this study provide productive directions for the reform of Public Pension Programs and social health insurance systems. Increasing life expectancy, low fertility, and a growing ratio of retirees to the working population have plagued the pay-as-you-go social security systems in many countries (Roy, Citation2018; Schreiber, Citation2018). In addition to demographic factors, the low investment returns of China’s pension funds have also shocked its sustainability. Increasing the investment return of pensions through innovative investment mechanisms could be an improvement measure. In response to regional differences in medical resources and the economy, the role of traditional family care and child support should be fulfilled, and the level of social security contributions should be appropriately increased within the acceptable range of rural residents to increase the health insurance fund and pension fund. Increasing the level of government subsidies for health insurance contributions in rural areas, improving the reimbursement ratio of medical reimbursement, and reducing the threshold of reimbursement reduce the medical expenses and pension burdens of rural residents. Other policy measures that can be considered are that regions can explore the establishment of a contribution adjustment mechanism linked to the level of local economic development. Individuals should also improve their health to avoid excessive medical treatment and wastage of medical resources.
The findings also reflect China’s high social health insurance coverage, but its guarantee level is low. Retirees have a higher burden of medical expenditures that cannot be met only by social insurance, especially for the elderly with lower economic levels. Private health insurance can provide broader health coverage and reduce financial burden on patients (Baggio et al., Citation2018; Paccagnella, Rebba, & Weber, Citation2013). Private health insurance can be customized according to different areas that include both the product and the relevant guarantee level at different rates. Correspondingly, as a supplement to social insurance, private pension insurance also needs to develop and design differentiated commercial pension insurance products for people with different life cycles. The government could consider raising tax benefits to incentivize individuals to purchase.
6. Conclusions
In the context of a rapidly aging population, the design of health insurance, the estimation of health care demands are important determinants of social welfare and economic development (Wang & Wang, Citation2020). The rising proportion of the aging population will bring a huge burden of pension and medical care to society. Studying the medical expenditures of the elderly after retirement and the utilization of medical resources is of practical significance for reforming and improving social endowment insurance and medical insurance. Accordingly, our study uses a RD approach to assess the impact of China’s current Public Pension Program on the medical expenditures of the elderly. First, research has shown that China’s current Public Pension Program has increased the cost of medical care for the retired elderly, that is, it has increased the use of medical resources by pensioners. Second, regional differences exist in the allocation and utilization of healthcare resources in China. Finally, financing for the intergenerational allocation of income remains an important issue in the future. Future research should include a broader range of key descriptive variables and explore more proven research methodologies to allow for more comprehensive analysis.
Acknowledgments
The authors wish to thank the study participants for their contribution to the research.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Notes on contributors
Xu Si
Xu Si received the B.S. degree in Economics from Sichuan Agricultural University, China, in 2016, and the M.S. degree in management from the School of Insurance, Southwestern University of Finance and Economics, China, in 2019. She is currently pursuing the Ph.D. degree with the School of Insurance, Central University of Finance and Economics. Her main research interests include social security actuary, health economy, machine learning.
Fu-Ling Chu
Fu-Ling Chu, received the Ph.D. in Economics from Renmin University of China in 1998, is currently a professor in the Department of Labor and Social Security and Director of the Social Security Research Centre at the School of Insurance, Central University of Finance and Economics. His main research interests include social security theory, policy and management.
Notes
1 The default triangular kernel function was used to construct the local polynomial estimators.
References
- Baggio, S., Dupuis, M., Wolff, H., Bodenmann, P., Bowen, M., & Bowen, M. (2018). Associations of lack of voluntary private insurance and out-of-pocket expenditures with health inequalities. evidence from an international longitudinal survey in countries with universal health coverage. Plos One, 13(10), e0204666.
- Bíró, A., & Elek, P. (2018). How does retirement affect healthcare expenditures? Evidence from a change in the retirement age. Health Economics, 27(5), 803–818.
- Bruno, W., & Melanie, C. (2013). Efficiency of health care delivery systems: Effects of health insurance coverage. Applied Economics, 45(28–30), 4082–4094.
- Bugni, F. A., & Canay, I. A. (2018). Testing continuity of a density via g-order statistics in the regression discontinuity design. Cemmap Working Papers.
- Calvo, E., Sarkisian, N., & Tamborini, C. R. (2012). Causal effects of retirement timing on subjective physical and emotional health. Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 68(1), 73–84.
- Carré, B., Thomas, M., Jusot, F., Wittwer, J., & Christelle, G. M. (2019). Does the take up of public insurance programs improves health care consumption of poor individuals? European Journal of Public Health(Suppl4), 29(Supplement_4). doi:10.1093/eurpub/ckz187.143
- Chen, D., Dennis, P., Tang, K., & Wu, D. (2017). Retirement saving and mental health in China. Health Promotion International, 33(5), 801–811.
- Christelis, D., Georgarakos, D., & Anna, S. G. (2020). The impact of health insurance on stockholding: A regression discontinuity approach. Journal of Health Economics, 69, 102246.
- David, C., Dobkin, C., & Maestas, N. (2008). The impact of nearly universal insurance coverage on health care utilization: Evidence from medicare. American Economic Review, 98(5), 2242–2258.
- Dayaram, K., & Mcguire, A. (2019). Retirement reforms: Occupational strain and health. Industrial Relations A Journal of Economy and Society, 58(1), 522–542.
- Fahle, S., Mcgarry, K., & Skinner, J. (2016). Out-of-pocket medical expenditures in the United States: Evidence from the health and retirement study. Fiscal Studies, 37(3–4), 785–819.
- Feng, J., Li, Q., & Smith, J. P. (2020). Retirement effect on health status and health behaviors in urban China. World Development, 126. doi:10.1016/j.worlddev.2019.104702
- Fourcade, N., Duval, J., & Lardellier, R. (2013). Redistribution des revenus opérée par l’assurance maladie entre groupes d’âge et groupes sociaux. Revue D’épidémiologie Et de Santé Publique, 61(Supplement_3), S170–S175. doi:10.1016/j.respe.2013.05.015
- Gong, C. H., Kendig, H., & He, X. (2016). Factors predicting health services use among older people in China: An analysis of the China health and retirement longitudinal study 2013. BMC Health Services Research, 16(1). doi:10.1186/s12913-016-1307-8
- Kail, B. L. (2016). The mental and physical health consequences of changes in private insurance before and after early retirement. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 71(2), 358–368.
- Krůtilová, V. (2016). Access to health care and the out-of-pocket burden of the European elderly. Acta Universitatis Agriculturae Et Silviculturae Mendelianae Brunensis, 64(6), 1961–1970.
- Kumagai, N., & Takabayashi, K. (2008). On the causality among social insurance burden rate, health care expenditures and public pension. The Hiroshima Economic Review, 32(2), 33–44.
- Kwon, E., Park, S., & Mcbride, T. D. (2018). Health insurance and poverty in trajectories of out-of-pocket expenditure among low-income middle-aged adults. Health Services Research, 53(6), 4332–4352.
- Lee, D. S., & Lemieux, T. (2010). Regression discontinuity designs in economics. Journal of Economic Literature, 48(2), 281–355.
- Levi, V. D. B., & Kène, H. (2018). When is quitting an escape? How different job demands affect physical and mental health outcomes of retirement. European Journal of Public Health, 28(5), 815–819.
- Olaniyan, O., Olayiwola, S., & Odubunmi, S. (2011). The impact of health expenditure on the elderly in Nigeria. Pakistan Journal of Social Sciences, 8(4), 212–218.
- Paccagnella, O., Rebba, V., & Weber, G. (2013). Voluntary private health insurance among the over 50s in Europe. Health Economics, 22(3), 289–315.
- Roy, S. B. (2018). Effect of health on retirement of older americans: A competing risks study. Journal of Labor Research, 39(1), 56–98.
- Rust, J., & Phelan, C. (1997). How social security and medicare affect retirement behavior in a world of incomplete markets. Econometrica, 65(4), 781–831.
- Schreiber, P. (2018). Widowhood and retirement timing: Evidence from the health and retirement study. The B.E. Journal of Economic Analysis & Policy, 18(3). doi:10.1515/bejeap-2017-0178
- Shai, O. (2018). Is retirement good for men’s health? Evidence using a change in the retirement age in Israel. Journal of Health Economics, 57, 15–30.
- Szabó, Á., Allen, J., Stephens, C., & Alpass, F. (2018). Is retirement associated with physical health benefits? A longitudinal investigation with older New Zealanders. Age and Ageing, 48(2), 267–272.
- Wallace, G. L., Haveman, R., & Wolfe, B. (2017). Health status, health shocks, and asset adequacy over retirement years. Research on Aging, 39(1), 222–248.
- Wang, X., & Wang, C. (2020). How does health status affect marginal utility of consumption? Evidence from China. International Journal of Environmental Research and Public Health, 17(7), 1–20. doi:10.3390/ijerph17072234
- Wei, N., & Zhou, L. L. (2019). Time-to-death and health care expenditure: Evidence from China. Journal of Population Ageing, 13(4), 485–495.
- Wu, X., & Li, L. (2014). The motives of intergenerational transfer to the elderly parents in China: Consequences of high medical expenditure. Health Economics, 23(6), 631–652.
- Xian, W., Xu, X., Li, J., Sun, J., Fu, H., & Wu, S. (1944). Health care inequality under different medical insurance schemes in a socioeconomically underdeveloped region of China: A propensity score matching analysis. BMC Public Health, 19(1), 1–9. doi:10.1186/s12889-019-7761-6
- Zhang, A., Nikoloski, Z., & Mossialos, E. (2017). Does health insurance reduce out-of-pocket expenditure? Heterogeneity among China’s middle-aged and elderly. Social Science & Medicine, 190, 11–19.
- Zhao, Y., Zhang, L., Fu, Y., Wang, M., & Zhang, L. (2020). Socioeconomic disparities in cancer treatment, service utilization and catastrophic health expenditure in China: A cross-sectional analysis. International Journal of Environmental Research and Public Health, 17(4), 1–13. doi:10.3390/ijerph17041327
Appendix
Table A1. The impact of pensions on medical expenditures: East
Table A2. The impact of pensions on medical expenditures: Middle
Table A3. The impact of pensions on medical expenditures: West