
ABSTRACT
We conducted a network analysis of measures of dissociation and posttraumatic symptoms (PTS) with a varied sample of adolescents (N = 312), some of them previously exposed to war scenarios. The global measure of dissociation (A-DES) was uniquely linked to the arousal PTS symptom cluster (CRIES-13), in particular sleep problems, but not to the reexperiencing and avoidance clusters. Three of four (i.e., depersonalization/derealization, amnesia, mental partition/compartmentalization) dissociation clusters were uniquely linked to PTS severity, but not absorption. The results with the pooled groups were generally representative of both groups. The DP/DR relation to PTS was based on data from both samples, whereas the link between amnesia and partition/parts might have been driven by the normative group, although the refugee sample had significantly higher scores in those variables. The results replicate some previous findings with adult samples and suggest new paths for research and theory.
The relation between dissociative symptoms and posttraumatic and other psychiatric symptoms is of great theoretical and practical importance (Cardeña et al., Citation2012; Lanius et al., Citation2010). For example, one study reported that trait dissociation partly mediated the relation between different types of trauma and the severity of psychiatric symptoms among adults (N = 359) (Schimmenti, Citation2018). Furthermore, lingering dissociative responses to traumatic events predict long-term posttraumatic symptomatology (see review in Cardeña & Carlson, Citation2011).
Also relevant is the DSM-5 adoption of a dissociative subtype of PTSD characterized by marked depersonalization/derealization (American Psychiatric Association, Citation2013). A review of 16 different studies using latent class analysis/latent profile analysis (LCA/LPA; CitationEllickson-Larew et al., Citation2020) found that all supported the presence of a dissociative type of PTSD, but there are conceptual and empirical limitations to the proposal that only depersonalization/derealization (DP/DR) mark a particular PTSD subtype. First, some studies that have supported the original proposal have only used depersonalization/derealization items (e.g., Wolf et al., Citation2012), rather than a more comprehensive list of dissociative phenomena, including amnesia and partition/compartmentalization. The latter are of theoretical importance (e.g., Van Der Hart et al., Citation2006), and their association with DP/DR is supported by research (e.g., Schimmenti, Citation2018). Studies that have used a longer list of dissociative items have often found that other items such as gaps in awareness and memory, and sensory misperceptions should be included as part of the dissociative subtype (e.g., Ross et al., Citation2018). Third, in the DSM-5 criteria for PTSD, amnesia for the traumatic event is listed under Negative Alterations in Cognition and Mood (NACM) cluster, splitting dissociative symptoms among different clusters, diluting the relation between dissociation and PTSD (Ross et al., Citation2018). Four, only two of the 16 LCA/LPA studies listed by Ellickson-Larew et al. (CitationEllickson-Larew, et al., Citation2020) were conducted with adolescents (Bennett et al., Citation2015; Choi et al., Citation2017).
Probably most recent studies on the dissociative subtype of PTSD have employed LCA/LPA approaches, which categorize empirically a sample into different groups based on the covariation of their responses to questionnaires. In contrast, network analysis (NA, or “graph theory”) seeks to identify and illustrate the unique shared variance between psychiatric symptoms (Borsboom & Cramer, Citation2013). NA has become increasingly popular, with an issue of a journal of traumatic stress focused on it (Frewen et al., Citation2020), and it has been used to assess the symptom structure of PTSD (e.g., Mitchell et al., Citation2017). Fewer NA studies have looked at the relation between PTSD and dissociation, with only one with a teenage sample as far as we could ascertain.
An NA of dissociative phenomena in adults (N= 2,274) reported three clusters of symptoms, named “trance,” “experiential disconnectedness,” and “segregated behaviors” by the authors (Schimmenti & Sar, Citation2018). The first cluster included items that are more commonly known as absorption (and do not necessarily involve self-hypnosis, as the authors of the paper stated). The second cluster comprised amnesia items plus experiential disconnectedness, and the last cluster’s two items were amnesia-related (i.e., not remembering whether one has done something, doing something but not remembering doing it). Dissociative phenomena are connected to various pathologies, as seen in the common comorbidity of dissociative and other diagnoses (Cardeña & Spiegel, Citation1996), and an online adult sample (N = 6, 941) reported links between dissociative phenomena (measured by an unpublished measure from the first author) and hallucinations, grandiosity, paranoia, cognitive disorganization, anxiety, depression, distress intolerance, insomnia, and posttraumatic stress (CitationCernis et al., Citation2021). A study with adults (N = 219) with a history of childhood abuse found that PTSD symptoms clustered together and with derealization and depersonalization (Knefel et al., Citation2016). In online research (N = 557 adults) with participants with scores suggestive of a PTSD diagnosis, DP/DR were associated with trauma-related amnesia, and DP on its own related to self-destructive/reckless behavior and flashbacks (Cramer et al., Citation2020).
However, there is also evidence from NA studies that DP/DR do not exhaust the significant associations between dissociative and PTSD symptomatology (PTS). Research with 445 adult inpatients treated for sexual abuse employed a comprehensive questionnaire of dissociation, along with measures of PTS, general psychopathology, and sexual symptoms (Kratzer et al., Citation2020). Intrusive and hyperarousal symptoms were closely associated, whereas avoidance symptoms had mixed relations with the other two symptom clusters. Dissociative symptoms were associated primarily with intrusive symptoms, and somatic forms of dissociation related primarily to physical reactions to trauma. The five most influential symptoms in the network were visual intrusions, physical reactions to trauma reminders, dissociative amnesia, difficulties falling asleep, and difficulties staying asleep. In another study with a sample of adults reporting sexual abuse (N = 473), in the network that included dissociation symptoms DP and DR had the strongest positive association (as could be expected, since they usually co-occur, e.g., Cardeña & Gleaves, Citation2007); DP was also associated with nightmares and flashbacks, and DR was associated with arousal and negative alterations in cognition and mood such as problem with concentration (McBride et al., Citation2020).
A few studies have evaluated the relation between PTS and dissociation in children and teenage samples. Bennett et al. (Citation2015) selected 225 detained youth who likely fulfilled partial or full PTSD DSM-IV-TR diagnosis and used only the DP/DR items of a dissociation questionnaire. The 20 individuals scoring high in dissociation reported higher posttraumatic symptomatology and higher emotional dysregulation; peritraumatic dissociation was a significant mediator between trauma exposure and trait dissociation. Using DSM-5 criteria, Choi et al. (Citation2017) confirmed in a sample of 12–16 year-olds the DP/DR subtype of PTSD, but an “expanded model” using all 10 dissociation symptoms in their measure also detected a dissociative amnesia/detached arousal subtype. Of the close to 24% of the sample that were PTSD cases, more than half endorsed DP/DR, particularly girls (Choi et al., Citation2019). It is also relevant that in a sample of 12–19 years-old, dissociation mediated the relation between exposure to multiple types of traumatic victimization and internalizing problems such as depression and anxiety (Ford et al., Citation2018).
Two studies specifically used an NA approach in non-adult samples. In one, based on ratings by caretakers of 75 trauma-exposed 3–7 years-olds, dissociation was linked most strongly with arousal but also with reexperiencing and avoidance, as well as with externalizing symptoms (Cervin et al., Citation2020). In the second study, with 475 traumatized children and teens, the DSM-5 NACM cluster (which includes persistent negative emotions as well as amnesia for features of the trauma) was the most central of all PTSD symptom clusters across genders (Bartels et al., Citation2019).
In sum, various studies using LCA/LPA or NA with adult and minor samples have consistently found that, when measured, other dissociative symptoms in addition to DP/DR relate to PTS symptomatology. The single NA study with teens sampled a traumatized population (Bartels et al., Citation2019), so no NA research has been published on the relation of dissociation and posttraumatic symptomatology using a more comprehensive sample of teens. The use of such a broad sample is indicated when trying to identify “true” effects to assess whether a relation exists between different symptoms (Fisher et al., Citation2020), and this study fills that gap in the literature.
Another relevant body of the literature has found that sleep difficulties (included in the PTS arousal cluster) relate to dissociation. Besides the studies reviewed on adults (Kratzer et al., Citation2020; McBride et al., Citation2020), other converging lines indicate that irregular sleep cycles and unusual sleep experiences may enhance daytime hallucinations, fantasy-proneness, dissociation, and other unusual experiences, with moderate to strong correlations between sleep disturbances and dissociation (reviewed in Cardeña et al., Citation2017: Lynn et al., Citation2019; see also CitationCernis et al., Citation2021). Furthermore, sleep loss increases dissociation and affects memory (Van Heugten-van der Kloet et al., Citation2015) and improvement in sleep habits decreases dissociative symptoms (Van der Kloet et al., Citation2012). The link between dissociative phenomena and sleep abnormalities may be bidirectional (Buchnik-Daniely et al., CitationBuchnik-Daniely, et al., Citationin press). No study, however, seems to have probed whether this relation is also present among teens.
The main thrust of our NA was exploratory. Nonetheless, we expected the following, considering previous research:
Posttraumatic symptomatology will relate to various forms of dissociation and not only to depersonalization/derealization.
Following the proposal that a dissociative type of PTSD involves overmodulation of hyperarousal/reexperiencing, those two clusters will be more related to dissociation than avoidance.
Disturbed sleep phenomena and dissociation in adults will relate to each other.
Method
Participants
Data come from three groups of teenagers from a large Swedish multicultural city: 1) A “normative” group (n = 235) of teenagers from two lower (ages 13 to 15) and two higher (ages 16 to 20) secondary schools. 2) Newly immigrated adolescents from war-torn countries (n = 42; aged 13–19), recruited through a center for war victims. 3) Students from public schools in a large Swedish city, who had experienced war at age 4 or older before immigrating to Sweden (n = 35; aged 11–18) (for additional information on these samples and other analyses, see Gušić et al., Citation2016a, Citation2016b, Citation2017, Citation2018). Groups 2 and 3 reported high frequency and prevalence of various types of trauma including observing and suffering violence and loss, and high percentages had scores above cutoffs for potential PTSD and dissociative diagnoses. For the total sample (N = 312, Mage = 15.8, SD = 1.64), 44% reported being female, 55% male, and 1% did not respond to that question.
Procedure
Data collection was secured by the second author, a licensed psychologist with an immigrant background, after visiting schools and the center for war victims. Participants could ask her questions during the evaluation and contact her afterward if distressed. Informed consent was secured as well as consent of the legal guardian for students under 15. The Swedish ethics board approved this research.
Measures
The Children’s Revised Impact of Events Scale (CRIES-13; Children and War Foundation, Citation2005) is a 13-item self-report scale that measures posttraumatic reexperiencing, avoidance, and arousal phenomena in children and adolescents, with good psychometric properties, at least with samples from 7 to 18-years-of-age (Perrin et al., Citation2005). It is based on the Impact of Events Scale-Revised (IES-R) (Weiss & Marmar, Citation1997), and each item is scored on a 4-point scale (0 = Never, 1 = Rarely, 3 = Sometimes, and 5 = Often), for a range of 0 to 65.
The Adolescent Dissociative Experiences Scale (A-DES; Armstrong et al., Citation1997) queries on 30 types of dissociative phenomena, with scores ranging from 0 = Never to 10 = Always, for a total range of 0–300. The internal consistency of the A-DES has been found to be high in previous research (Farrington et al., Citation2001).
Analysis
Psychometric properties of the measures
We used both item- and factor-level network analyses to examine associations between PTS and dissociation. To establish which factors to include at the factor-level network analyses, the psychometric properties of the measures were explored. For CRIES-13, we examined two models using confirmatory factor analysis (CFA): (1) a unidimensional model in which a single factor explained covariance among items, and (2) the DSM-IV model with three factors representing reexperiencing, avoidance, and arousal. For ADES, we examined two models: a unidimensional model in which a single factor explained covariance among items, and a model with four theory-derived factors representing the typical factors obtained in FA of DES plus one factor focusing specifically on experiences of mental partition/compartmentalization, highlighted in the theory of trauma-related structural dissociation (Van Der Hart et al., Citation2006). These are the four factors A-DES: absorption (items 1, 10, 11, 12, 17, 28, e.g., I get so wrapped up in my toys or stuffed animals that they seem alive); amnesia (items 2, 4, 5, 7, 8, 14, 15, 18, 22, 24, 26, 27, e.g., I get back tests or homework that I don’t remember doing); DP/DR (items 6, 13, 25, 30, e.g., My body feels as if it doesn’t belong to me), and mental partition/compartmentalization (items 3, 9, 16, 19, 20, 21, 23, 29, e.g., I feel like there are different people inside of me). Each item of the ADES measure has 11 response options, but the distribution of scores was zero-inflated and DWLS estimation was used. Missing data (6.1% for CRIES and 1.4% for ADES) in the CFA analyses were handled using pairwise deletion.
Network analyses
We first estimated a PTS item network that included all 13 CRIES items and a single node representing dissociation and then evaluated a PTSD domain network that included the three PTSD clusters (reexperiencing, avoidance, and arousal) with a single node representing dissociation. To explore whether some aspects of dissociation were more strongly associated with PTS than others, we also estimated a network that included the four dissociation clusters and a single node representing PTS severity (sum score of the CRIES-13). All networks were estimated using the R library BGGM. Within a network framework, variables are called nodes (represented as circles when the network is plotted). Nodes are connected by edges (lines when plotted). Edges were estimated using partial correlations; that is, pairwise dependencies that account for all linear associations in the full set of variables. A 95% credible interval around each partial correlation was calculated and this interval was used to control for false positive rate. For the factor/domain networks, sum scores for each domain were used and for these analyses missing data were handled by imputing the mean score on the scale when computing the sum score. This is a valid method when item-level missingness is low (Parent, Citation2013), as in this case. Missing data in the item-level network analyses were handled using multiple imputation with predictive mean matching using the R library mice. We used 5 imputations and 10 iterations for each dataset. Networks were plotted using the Fruchterman-Reingold algorithm, which places nodes with many and strong edges to other nodes central in the network and strongly linked node pairs closely, while avoiding overlap of nodes and edges.
Inference from network estimates
We were mainly interested in links between dissociation and PTS. Thus, we a-priori defined which properties of the network we would infer. For the PTS item network, we analyzed the edge between the dissociation node and each of the PTS items and whether some PTS items were more strongly associated with dissociation than others. The same approach was taken for the PTS domain network, with edges between dissociation and PTS domains examined. Differences in the strength with which PTS items/domains were associated with PTS were tested by estimating posterior distributions for the estimates of interest and calculating the posterior probability that a specific association was stronger than another. Posterior probabilities above .975 or under .025 were used as indicators of true differences. We also calculated 95% credible intervals for the difference in the association between PTS items/domains and dissociation. Credible intervals for the difference that did not include zero were taken to indicate a true difference.
Results
Psychometric properties of the measures
Both the single- (n = 303, df = 65, X2 = 242.9, p < .001, RMSEA = .095, CFI = .946, TLI = .931, SRMR = .087) and 3-factor CRIES models (n = 303, df = 62, X2 = 230.9, p < .001, RMSEA = .095, CFI = .949, TLI = .936, SRMR = .071) had adequate fits (with the exception of the RMSEA index, which may be expected given the small n and df; Kenny, Citation2020), with the 3-factor model having a better fit. Ordinal alphas for the three PTS domain scales were adequate (reexperiencing = .83, avoidance = .82, arousal = .76). We adopted the 3-factor model of CRIES for all domain networks while the single-factor model was used when examining the dissociation items and their links to PTS.
The single- (n = 312, df = 405, X2 = 792.1, p < .001, RMSEA = .055, CFI = .966, TLI = .963, SRMR = .057) and 4-factor A-DES models (n = 312, df = 402, X2 = 785.4, p < .001, RMSEA = .056, CFI = .966, TLI = .963, SRMR = .056) had adequate and very similar fits. To facilitate interpretation, we used the single-factor scale that had an excellent alpha (.95) for the networks of PTS items/domains and the four dissociation domains to examine unique links between different domains of dissociation and overall PTS severity. The alphas of the four (absorption, amnesia, DP/DR, partition/compartmentalization) A-DES scales were adequate (.74, .91, .86, .92).
Network with separate PTS items and a single dissociation node
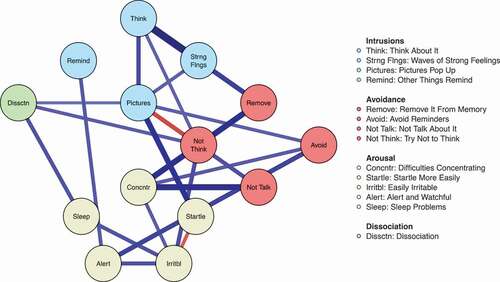
We estimated a network that included the 13 CRIES items and a single dissociation node. The network structure is displayed in and the posterior probabilities for differences are in . The major findings were that the node representing sleep difficulties had the strongest (point estimate) association with dissociation. This node was also significantly more strongly associated with dissociation than four other nodes (not talking, avoidance, removing from memory, and intrusive thoughts). The PTS node of thinking about the trauma event when not meaning to had the weakest association with dissociation and was significantly less strongly associated with dissociation than four of the other 12 nodes (being alert, mental pictures of the trauma appearing, sleep difficulties, and thinking about the trauma).
Table 1. Posterior probabilities (PPs) evaluating whether the symptom in the first column is more strongly linked to dissociation than the symptom in each row. PPs in which the 95% credible interval for the difference does not include zero are highlighted in bold
Figure 1. Network structure of PTSD symptoms and dissociation
Network with PTS domains and dissociation
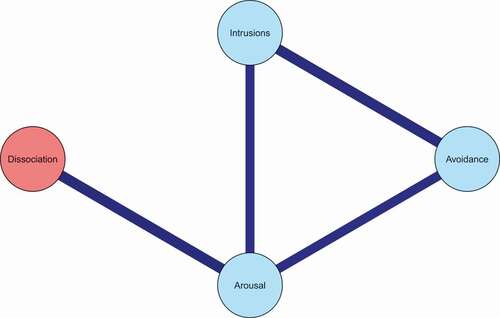
The network structure for the three PTS domains and dissociation is displayed in and the posterior probabilities and CIs for differences are in . The only edge that emerged between the PTS domains and dissociation, after using credible intervals to control for false positive rate, was between arousal and dissociation. This edge was also significantly stronger than the edges between dissociation and reexperiencing, and dissociation and avoidance, with no significant difference between the two latter edges.
Table 2. Posterior probabilities (PPs) evaluating whether the variable in the first column is more strongly linked to dissociation than the variable in the first row. Mean difference and a 95% credible interval for this difference are presented below the PPs
Figure 2. Network structure of PTSD symptom domains and dissociation
Network with dissociation domains and PTS severity
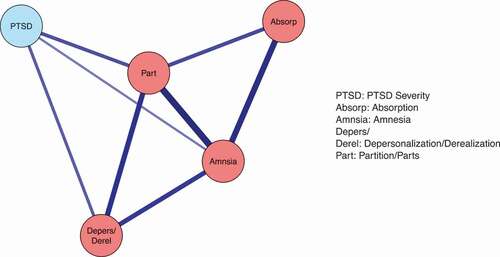
The network model including the four dissociation domains and PTS severity is presented in . Results revealed that all domains were uniquely related to PTS except for absorption. Furthermore, the partition/compartmentalization, DP/DR, and amnesia domains were more strongly related to PTS than absorption (all PPs <1.1%), and the first three domains did not differ significantly in their links to PTS (no PP <10% or >90%).
Figure 3. Network structure of dissociation domains and PTSD
Subsample analyses
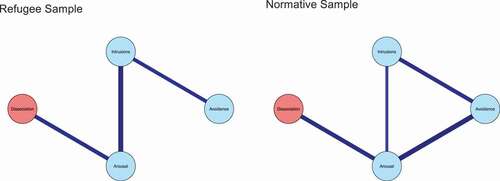
To examine whether the pooling of different samples (i.e., normative and refugee youth) affected results, we conducted sensitivity analyses using domain scores across the two subsamples (power was too low to conduct item-level subsample analyses). In , we show the distribution of the total score on the PTS and the dissociation scale in both samples. There was variation in both samples, but the correlations between the CRIES and A-DES were very similar across samples (Normative sample: Spearman’s rho = .46; Refugee sample: Spearman’s rho = .42; pooled sample: Spearman’s rho = .52; all correlations p < .01). In , we present the network for the three PTS scales and dissociation based on each subsample. In both groups, the only significant link that emerged between dissociation and PTS was between the PTS domain of arousal and dissociation, and the edge estimate was almost identical across groups (edge in normative sample = 0.41; edge in refugee sample = 0.38). For the domain network in which the four dissociation domains and PTS were included, no edges emerged between PTS and dissociation in the refugee sample (possibly because of low power). Therefore, we compared the zero-order correlations between the samples. In the normative sample, the correlations between PTS and absorption, amnesia, DP/DR and partition/compartmentalization were .29, .46, .45, and .49, respectively. The corresponding rho values in the refugee sample were .36, .39, .37, and .37. The pooled correlations were .39, .51, .48, and .53. To further examine possible differences, we carried out a multiple linear regression for each sample with the PTS total score as the dependent variable and the dissociation domains as independent variables. Because of low power in the refugee sample, we compared the standardized beta values (i.e., the size of the association between each independent variable and the dependent variable). For absorption, we found divergent results: the association was positive in the refugee sample (0.19) and negative in the normative sample (−0.15). For partition/compartmentalization and amnesia, there was no clear association in the refugee sample, while these variables were positively associated with PTS in the normative sample (standardized beta values = 0.33 and 0.20, respectively, for the first association p < .01). For DP/DR, there was a positive association with PTS in both the refugee (standardized beta value = 0.27) and normative samples (standardized beta value = 0.21) with the latter association p = .02. In sum, the link between DP/DR and PTS that appeared in the full sample was based on data from both samples, while the links between amnesia and partition/parts and PTS may have been driven by associations present in the normative sample, although the refugee sample had higher scores on both these variables (Mann Whitney U tests: ps < .001).
Figure 4. Histograms of PTS and dissociation for the subsamples
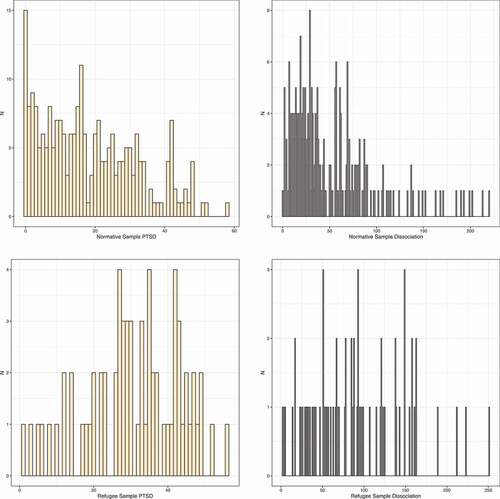
Figure 5. PTS-dissociation network for the subsamples
Discussion
The proposed 3-factor solution for the CRIES-13 was empirically supported, as was a four-factor solution for the A-DES including a partition/compartmentalization cluster. At the level of PTS items and a single dissociation node, sleep difficulties had the strongest association with dissociation, whereas thinking about the trauma when not meaning to had the weakest one. At the level of PTS domains, and consistent with the previous result, dissociation related only to the arousal (which contains the sleep difficulty item) cluster. Three (DP/DR, amnesia, partition/compartmentalization) dissociation clusters are related to PTS but not absorption. Finally, analyses separating the normative versus refugee youth revealed that the results with the pooled groups were generally representative of both groups. Multiple regression analyses pointed out that the DP/DR relation to PTS was based on data from both samples, whereas the link between amnesia and partition/parts might have been driven by the normative group although the refugee sample had significantly higher scores in those variables.
Our results replicate the link between arousal and dissociation reported by Cervin et al. (Citation2020). With respect to the overmodulation model in which dissociation is explained by an emotional overmodulation of hyperarousal and reexperiencing symptoms, our results only corroborated a relation between arousal and dissociation. A possible explanation is that reexperiencing of the traumatic event may not be as important when ongoing everyday stressors or even innocuous stimuli may suffice to produce great arousal and, then, physiological and cognitive dissociative reactions. Some studies support this interpretation, one from neurophysiology and the other from psychology. For instance, in a study by Lemche et al. (Citation2007), high right amygdala activity among depersonalization patients when observing a facial neutral expression greatly decreased when observing expressions with greater intensity, an opposite pattern to that of a non-clinical group. Notice that the stimuli that produced the overmodulation were new facial stimuli rather than previous traumatic ones. Similarly, in a questionnaire study with women sexually abused in childhood, compared with instances of later sexual revictimization (which would be reexperiencing) recent stressful life events were more related to acute and chronic traumatic symptoms, anxiety, dissociation, sexual problems, and sleep disturbances (Classen et al., Citation2002). Thus, in the presence of intense baseline levels of arousal even minor stresses may trigger dissociative reactions.
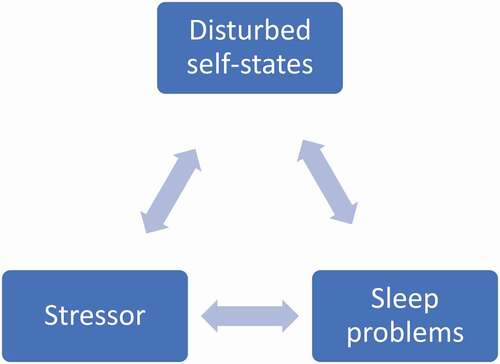
Our results showed that sleep problems in the arousal cluster were more strongly related to dissociation than other PTS items. There are various ways in which sleep problems and dissociative reactions may relate to each other. First, both experimentally induced stress and PTSD status related to sleep inefficiency (Kim & Dimsdale, Citation2007) and, as mentioned, stressors are also related to dissociative reactions in those prone to have them (Classen et al., Citation2002). Second, sleep problems and the ensuing fatigue can become stressors in themselves. Third, unusual sleep experiences and irregular sleep cycles may impair reality monitoring by blurring the distinction between dreaming and non-dreaming events, and weaken the continuity of identity based on stable memories. Thus, sleep problems, as well as acute reactions to trauma and stress (Cardeña & Carlson, Citation2011) may trigger disturbed and fragmented self-states (cf. Horowitz, Citation2011) and promote dissociation. shows this recursive model. Naturally, other variables such as exposure to trauma (Dalenberg et al., Citation2012, Citation2014) and deficits in meta-consciousness and self-regulation (Lynn et al., Citation2019) also predict dissociation. A recent study found that both distress/trauma and sleep disturbances had unique contributions to dissociation (Buchnik-Daniely et al., CitationBuchnik-Daniely, et al., Citationin press).
Figure 6. Proposed recursive interactions between stressors, sleep problems, and disturbed self-states
Analyses splitting the sample confirmed a robust relation between DP/DR and PTS, but gave clear indications that other dissociative symptoms including partition/compartmentalization should be considered in discussing the relation between dissociation and PTS. The finding that absorption did not relate to PTS is not surprising. A taxonomic analysis of the adult version of the A-DES posited that 8 items measuring DP/DR and amnesia, but not absorption, related to a pathological form of dissociation (Waller et al., Citation1996). In general agreement, in a study with psychic practitioners, the relation between a scale of absorption and a measure of psychopathology was significant but of lower magnitude than that for a general dissociation measure (Cardeña et al., Citation2015). One of the reasons is that absorption relates to creative, hypnotic, and other non-pathological activities (e.g., Hilgard, Citation1974), whereas other dissociative phenomena are more closely associated to pathology. The results of the analyses in the present paper after splitting the samples offer the intriguing hypothesis that a small positive association between absorption and PTS may occur only with less traumatized groups, whereas the opposite may be the case for traumatized groups. It may be that for the former absorption is associated with increases in arousal (for instance, in recollection of distressing events), whereas for the severely traumatized group absorption in distressing memories or perceptions may lead to over- rather than under-modulation of arousal (cf. Lanius et al., Citation2010). This distinction may be missed in linear analyses collapsing different groups.
Limitations. This study had a relatively modest N for NA, particularly for the traumatized groups, and included a heterogeneous sample of adolescents. Regarding the latter, it has been recommended to oversample extreme cases when studying dimensional psychopathological phenomena, of which both PTS and dissociation may be considered examples. This increases the statistical power to detect true associations in the target population, although it can lead to imprecision in determining the specific strength of this association (risk of exaggerating the effect) (Fisher et al., Citation2020). Because only one study had previously examined the links between PTS and dissociation in youth samples using NA, we consider this study an important first step in showing what the clearest links between PTS and dissociation may be, but future studies should include larger samples and with a wide range of traumatization. Second, the domains of PTS and dissociative symptoms were limited to the measures used. An interview study with some of this sample showed that a sense of lack of mental control was a cardinal aspect of the dissociative experience (Gušić et al., Citation2018), yet that aspect was not directly represented in the questionnaires used and should be added in future research. Third, sleep problems are transdiagnostic (Harvey, Citation2008) so greater specificity about their role in dissociation and the interplay between the two phenomena is required. Perhaps the strongest limitation is that our cross-sectional study evaluated self-report measures at one point in time and could not measure the processes through which different symptoms may interact and affect each other across time. Nonetheless, this may be the first NA study on the relation between dissociation and PTS phenomena among teenagers. The results confirmed some results while suggesting new paths for research, including the use of broad samples to evaluate to what extent the relation between dissociation and PTS should be considered dimensional or may differ across levels of traumatization (cf. Conway et al., CitationConway and Krueger, Citationin press).
(The data that support the findings of this study are available from the corresponding author, [author initials], upon reasonable request.)
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed. ed.).
- Armstrong, J. G., Putnam, F. W., Carlson, E. B., Libero, D. Z., & Smith, S. R. (1997). Development and validation of a measure of adolescent dissociation: The adolescent dissociative experiences scale. Journal of Nervous and Mental Disease, 185(8), 491–497. https://doi.org/https://doi.org/10.1097/00005053-199708000-00003
- Bartels, L., Berliner, L., Holt, T., Jensen, T., Jungbluth, N., Plener, P., Risch, E., Rojas, R., Rosner, R., & Sachser, C. (2019). The importance of the DSM-5 posttraumatic stress disorder symptoms of cognitions and mood in traumatized children and adolescents: Two network approaches. Journal of Child Psychology and Psychiatry, 60(5), 45–554. https://doi.org/https://doi.org/10.1111/jcpp.13009
- Bennett, D. C., Modrowski, C. A., Kerig, P. K., & Chaplo, S. D. (2015). Investigating the dissociative subtype of posttraumatic stress disorder in a sample of traumatized detained youth. Psychological Trauma: Theory, Research, Practice, and Policy, 7(5), 465–472. https://doi.org/https://doi.org/10.1037/tra0000057
- Borsboom, D., & Cramer, A. O. J. (2013). Network analysis: An integrative approach to the structure of psychopathology. Annual Review of Clinical Psychology, 9(1), 91–21. https://doi.org/https://doi.org/10.1146/annurev-clinpsy-050212-185608
- Buchnik-Daniely, Y., Vannikov-Lugassi, M., Shalev, H., & Soffer-Dudek, N. (in press). The path to dissociative experiences: A direct comparison of different etiological models. Clinical Psychology & Psychotherapy.
- Cardeña, E., Butler, L., Reijman, S., & Spiegel, D. (2012). Disorders of extreme stress. In I. B. Weiner, G. Stricker, & T. A. Widiger (Eds.), Handbook of psychology. Clinical psychology (2nd ed., pp. 497–548). Wiley.
- Cardeña, E., & Carlson, E. (2011). Acute Stress Disorder revisited. Annual Review of Clinical Psychology, 7(1), 245–267. https://doi.org/https://doi.org/10.1146/annurev-clinpsy-032210-104502
- Cardeña, E., & Gleaves, D. (2007). Dissociative disorders. In M. Hersen, S. M. Turner, & D. Beidel (Eds.), Adult psychopathology & diagnosis (5th ed., pp. 473–503). Wiley.
- Cardeña, E., Lynn, S. J., & Krippner, S. (2017). The psychology of anomalous experiences: A rediscovery. Psychology of Consciousness: Theory, Research, and Practice, 4(1), 4–22. https://doi.org/https://doi.org/10.1037/cns0000093
- Cardeña, E., Reijman, S., Lawaetz Wimmelmann, C., & Jensen, C. G. (2015). Psychological health, trauma, dissociation, absorption, and fantasy proneness among Danish spiritual practitioners. Psychology of Consciousness: Theory, Research, and Practice, 2(2), 170–184. https://doi.org/https://doi.org/10.1037/cns0000047
- Cardeña, E., & Spiegel, D. (1996). Diagnostic issues, criteria and comorbidity of dissociative disorders. In L. Michelson & W. J. Ray (Eds.), Handbook of dissociation (pp. 227–250). Plenum.
- Cernis, E., Evans, R., Ehlers, A., & Freeman, D. (2021). Dissociation in relation to other mental health conditions: An exploration using network analysis. Journal of Psychiatric Research 136, 460–467. https://doi.org/https://doi.org/10.1016/j.jpsychires.2020.08.023
- Cervin, M., Salloum, A., Ruth, L. J., & Storch, E. A. (2020). Posttraumatic symptoms in 3-7 year old trauma-exposed children: Links to impairment, other mental health symptoms, caregiver PTSD, and caregiver stress. Child Psychiatry & Human Development. https://doi.org/https://doi.org/10.1007/s10578-020-01093-3
- Children and War Foundation. (2005). Children’s Revised Impact of Event Scale (CRIES-13). https://www.childrenandwar.org/projectsresources/measures/
- Choi, K. R., Ford, J. D., Briggs, E. C., Munro-Kramer, M. L., Graham-Bermann, S. A., & Seng, J. S. (2019). Relationships between maltreatment, posttraumatic symptomatology, and the dissociative subtype of PTSD among adolescents. Journal of Trauma and Dissociation, 20(2), 212–227. https://doi.org/https://doi.org/10.1080/15299732.2019.1572043
- Choi, K. R., Seng, J. S., Briggs, E. C., Munro-Kramer, M. L., Graham-Bermann, S. A., Lee, R. C., & Ford, J. D. (2017). The dissociative subtype of posttraumatic stress disorder (PTSD) among adolescents: Co-occurring PTSD, depersonalization/ derealization, and other dissociation symptoms. Journal of the American Academy of Child & Adolescent Psychiatry, 56(12), 1062–1072. https://doi.org/https://doi.org/10.1016/j.jaac.2017.09.425
- Classen, C., Nevo, R., Koopman, C., Nevill-Manning, K., Gore-Felton, C., Rose, D. S., & Spiegel, D. (2002). Recent stressful life events, sexual revictimization, and their relationship with traumatic stress symptoms in women sexually abused in childhood. Journal of Interpersonal Violence, 17(12), 1274–1290. https://doi.org/https://doi.org/10.1177/088626002237856
- Conway, C. C., & Krueger, R. F., HiTOP Executive Consortium Board. (in press). Rethinking the diagnosis of mental disorders: Data-driven psychological dimensions, not categories, as a framework for mental-health research, treatment, and training. Current Directions in Psychological Science. https://doi.org/https://doi.org/10.1177/0963721421990353
- Cramer, A. O. J., Leertouwer, I., Lanius, R., & Frewen, P. (2020). A network approach to studying the associations between posttraumatic stress disorder symptoms and dissociative experiences. Journal of Traumatic Stress, 33(1), 19–28. https://doi.org/https://doi.org/10.1002/jts.22488
- Dalenberg, C. J., Brand, B. L., Gleaves, D. H., J:, D. M., Loewenstein, R. J., Cardeña, E., Frewen, P. A., Carlson, E. B., & Spiegel, D. (2012). Evaluation of the evidence for the trauma and fantasy models of dissociation. Psychological Bulletin, 138(3), 50–588. https://doi.org/https://doi.org/10.1037/a0027447
- Dalenberg, C. J., Brand, B. L., Gleaves, D. H., J:, D. M., Loewenstein, R. J., Cardeña, E., Frewen, P. A., Carlson, E. B., & Spiegel, D. (2014). Reality versus fantasy: Reply to Lynn et al. (2014). Psychological Bulletin, 140(3), 911–920. https://doi.org/https://doi.org/10.1037/a003668
- Ellickson-Larew, S., Escarfulleri, S., & Wolf, E. (2020). The dissociative subtype of PTSD: Forensic considerations and recent controversies. Psychological Injury and Law 13, 178–186. https://doi.org/https://doi.org/10.1007/s12207-020-09381-y
- Farrington, A., Waller, G., Smerden, J., & Faupel, A. W. (2001). The adolescent dissociative experiences scale: Psychometric properties and difference in scores across age groups. Journal of Nervous and Mental Disease, 189(10), 722–727. https://doi.org/https://doi.org/10.1097/00005053-200110000-00010
- Fisher, J. E., Guha, A., Heller, W., & Miller, G. A. (2020). Extreme-groups designs in studies of dimensional phenomena: Advantages, caveats, and recommendations. Journal of Abnormal Psychology, 129(1), 14. https://doi.org/https://doi.org/10.1037/abn0000480
- Ford, J. D., Charak, R., Modrowski, C. A., & Kerig, P. K. (2018). PTSD and dissociation symptoms as mediators of the relationship between polyvictimization and psychosocial and behavioral problems among justice-involved adolescents. Journal of Trauma and Dissociation, 19(3), 325–346. https://doi.org/https://doi.org/10.1080/15299732.2018.1441354
- Frewen, P., O’Donell, M., D’Andrea, W., Schmahl, & Schmahl, (Eds.). (2020). Special issue: Network analysis of traumatic stress. Journal of Traumatic Stress, 33(1), 5–9. https://doi.org/https://doi.org/10.1002/jts.22486
- Gušić, S., Cardeña, E., Bengtsson, H., & Søndergaard, H. P. (2016a). Adolescents’ dissociative experiences: The moderating role of type of trauma and attachment style. Journal of Child & Adolescent Trauma, 9, 341–351. https://doi.org/https://doi.org/10.1007/s40653-016-0107-y
- Gušić, S., Cardeña, E., Bengtsson, H., & Søndergaard, H. P. (2016b). Types of trauma in adolescence and their relation to posttraumatic stress and dissociation: A mixed-methods study. Psychological Trauma: Theory, Research, Practice, and Policy, 8, 568–576.
- Gušić, S., Cardeña, E., Bengtsson, H., & Søndergaard, H. P. (2017). Dissociative experiences and trauma exposure among newly arrived and settled young war refugees. Journal of Aggression, Maltreatment & Trauma, 26, 1132–1149.
- Gušić, S., Maleševic, A., Cardeña, E., Bengtsson, H., & Søndergaard, H. P. (2018). “I feel like I do not exist:” A study of dissociative experiences among war-traumatized refugee youth. Psychological Trauma: Theory, Research, Practice, and Policy, 10(5), 542–550. https://doi.org/https://doi.org/10.1037/tra0000348
- Harvey, A. G. (2008). Insomnia, psychiatric disorders, and the transdiagnostic perspective. Current Directions in Psychological Science, 17(5), 299–303. https://doi.org/https://doi.org/10.1111/j.1467-8721.2008.00594.x
- Hilgard, J. R. (1974). Imaginative involvement: Some characteristics of the highly hypnotizable and the non-hypnotizable. International Journal of Clinical and Experimental Hypnosis, 22(2), 138–156. https://doi.org/https://doi.org/10.1080/00207147408412993
- Horowitz, M. J. (2011). Stress response syndromes (5th ed). Jason Aronson.
- Kenny, D. A. (2020). Measuring model fit. http://davidakenny.net/cm/fit.htm
- Kim, E. J., & Dimsdale, J. E. (2007). The effect of psychosocial stress on sleep: A review of polysomnographic evidence. Behavioral Sleep Medicine, 5(4), 256–278. https://doi.org/https://doi.org/10.1080/15402000701557383
- Knefel, M., Tran, U. S., & Lueger-Schuster, B. (2016). The association of posttraumatic stress disorder, complex posttraumatic disorder, and borderline personality disorder from a network analytical perspective. Journal of Anxiety Disorders, 43, 70–78. https://doi.org/https://doi.org/10.1016/j.janxdis.2016.09.002
- Kratzer, L., Heinz, P., Schennach, R., Knefel, M., Schiepek, G., Biedermann, S. V., & Büttner, M. (2020). Sexual symptoms in post-traumatic stress disorder following childhood sexual abuse: A network analysis. Psychological Medicine, 1–12. https://doi.org/https://doi.org/10.1017/S0033291720001750
- Lanius, R. A., Vermetten, E., Loewenstein, R. J., Brand, B., Schmahl, C., Bremner, J. D., & Spiegel, D. (2010). Emotion modulation in PTSD: Clinical and neurobiological evidence for a dissociative subtype. American Journal of Psychiatry, 167(6), 640–647. https://doi.org/https://doi.org/10.1176/appi.ajp.2009.09081168
- Lemche, E., Surguladze, S. A., Giampietro, V. P., Anilkumar, A., Brammer, M. J., Sierra, M., Chitnis, X., Williams, S. C., Gasston, D., Joraschky, P., David, A. S., & Phillips, M. L. (2007). Limbic and prefrontal responses to facial emotion expressions in depersonalization. Neuroreport, 18(5), 473–477. https://doi.org/https://doi.org/10.1097/WNR.0b013e328057deb3
- Lynn, S. J., Maxwell, R., Merckelbach, H., Lilienfeld, S. O., Kloet, D.-V. H.-V. D., & Miskovic, V. (2019). Dissociation and its disorders: Competing models, future directions, and a way forward. Clinical Psychology Review, 73, 101755. https://doi.org/https://doi.org/10.1016/j.cpr.2019.101755
- McBride, O., Hyland, P., Murphy, J., & Elklit, A. (2020). Network analysis of posttraumatic stress experiences of adults seeking psychological treatment for childhood sexual abuse. Journal of Traumatic Stress, 33(1), 10–18 . https://doi.org/https://doi.org/10.1002/jts.22381
- Mitchell, K. S., Wolf, E. J., Bovin, M. J., Lee, L. O., Green, J. D., Rosen, R. C., Keane, T. M., & Marx, B. P. (2017). Network models of DSM-5 posttraumatic stress disorder: Implications for ICD-11. Journal of Abnormal Psychology, 126(3), 355–366. https://doi.org/https://doi.org/10.1037/abn0000252
- Parent, M. C. (2013). Handling item-level missing data: Simpler is just as good. The Counseling Psychologist, 41(4), 568–600. https://doi.org/https://doi.org/10.1177/0011000012445176
- Perrin, S., Meiser-Stedman, R., & Smith, P. (2005). The children’s revised impact of event scale (CRIES): Validity as a screening instrument for PTSD. Behavioural and Cognitive Psychotherapy, 33(4), 487–498. https://doi.org/https://doi.org/10.1017/S1352465805002419
- Ross, J., Baník, G., Dědová, M., Mikulášková, G., & Armour, C. (2018). Assessing the structure and meaningfulness of the dissociative type of PTSD. Social Psychiatry and Psychiatric Epidemiology, 53(5), 87–97. https://doi.org/https://doi.org/10.1007/s00127-017-1445-2
- Schimmenti, A., & Sar, V. (2019). A correlation network analysis of dissociative experiences. Journal of Trauma & Dissociation, 20(4), 402–419. https://doi.org/https://doi.org/10.1080/15299732.2019.1572045
- Schimmenti, A. (2018). The trauma factor: Examining the relationships among different types of trauma, dissociation, and psychopathology. Journal of Trauma & Dissociation, 19(5), 552–571. https://doi.org/https://doi.org/10.1080/15299732.2017.1402400
- Van Der Hart, O., Nijenhuis, E. R. S., & Steele, K. (2006). The haunted self: Structural dissociation and the treatment of chronic traumatization. W. W. Norton.
- Van der Kloet, D., Giesbrecht, T., Lynn, S. J., Merckelbach, H., & De Zutter, A. (2012). Sleep normalization and decrease in dissociative experiences: Evaluation in an inpatient sample. Journal of Abnormal Psychology, 121(1), 140–150. https://doi.org/https://doi.org/10.1037/a0024781
- Van Heugten-van der Kloet, D., Giesbrecht, T., & Merckelbach, H. (2015). Sleep loss increases dissociation and affects memory for emotional stimuli. Journal of Behavioral Therapy and Experimental Psychiatry, 47, 9–17. https://doi.org/https://doi.org/10.1016/j.jbtep.2014.11.002
- Waller, N., Putnam, F. W., & Carlson, E. B. (1996). Types of dissociation and dissociative types: A taxometric analysis of dissociative experiences. Psychological Methods, 1(3), 300–321. https://doi.org/https://doi.org/10.1037/1082-989X.1.3.300
- Weiss, D. S., & Marmar, C. R. (1997). The impact of event scale-revised. In J. P. Wilson & T. M. Keane (Eds.), Assessing psychological trauma and PTSD (pp. 399–411). Guilford.
- Wolf, E. J., Lunney, C. A., Miller, C. A., Resick, M. W., Friedman, P. A., & Schnurr, M. J. (2012). The dissociative subtype of PTSD: A replication and extension. Depression and Anxiety, 29(8), 679–688. https://doi.org/https://doi.org/10.1002/da.21946