
ABSTRACT
Problem: Early onset, prevalence, and predictors of substance use – tobacco, alcohol-drinking, alcohol-drunkenness, and drugs – were studied in 13 and 14-year-old boys and girls in Sweden. Methods: Self-reported data in four communities were used (n = 1,716). A large set of psychological and social factors were tried as predictors of early onset use (n = 1,459). Results: There were few gender differences and low prevalence. Primary predictor for early onset in tobacco use was availability; perceived parental approval for alcohol use, and delinquent behaviors for alcohol-drunkenness and drug use. Conclusions: Individual behavioral factors and parental norms seem to be most important in this age.
In the Western world, the onset of substance use has been described as a transition-marker, i.e., a symbolic way to end childhood (Sande, Citation2002). Adolescents learn about tobacco, alcohol, and drugs through media, peers, and family members (Velleman, Citation2009). Many of them associate alcohol with pleasure (Ander et al., Citation2017). For some, this may also be the case for tobacco and drugs. However, early substance onset has been found to predict later development of abuse or dependence as well as depressive problems (Pitkänen et al., Citation2005). For instance, early substance onset is related to an increased risk of developing neurological, psychological, and social problems later in life, such as drug use, mental health issues, criminality, and low academic achievement (Bolland et al., Citation2016; Hawkins et al., Citation1992). Overall, most research on the onset of substance use focuses on adolescents who are 15 years or older, that is, in their mid-adolescence. Studies that include several substances and onset in younger ages are scarce (Donovan & Molina, Citation2011). The present study investigated early onset of substance use among 13–14-year-olds in Sweden. The first two years as teens, ages 13–14 years, are here referred to as early adolescence in accordance with Steinberg (Citation2017).
In Sweden, turning 18 years old legally permit the person to buy cigarettes and snuff, and to purchase alcoholic beverages at pubs and restaurants. Purchases from the state alcohol retail monopoly require the person to be 20 years old. Use of cannabis and other drugs are illegal, except when some other drugs are prescribed. International research from recent years shows a decrease in adolescent substance use in many countries in the western world (Miech et al., Citation2017; Pape et al., Citation2018). The yearly Swedish national substance surveys show the same declining trend. Alcohol consumption among 15- and 16-year-olds has decreased significantly since the 1970s; 40% of the boys and 44% of the girls had consumed alcohol during the past year. Also, the use of cigarettes and snuff has decreased; 10% of the boys and 14% of the girls reported smoking, and 10% of the boys and 2% of the girls reported having used snuff (Gripe, Citation2015). The use of cannabis is low among Swedish 15- and 16 years old’s compared to adolescents in other European nations; 7% compared to 16% (ESPAD Group, Citation2016). There are few previous Swedish studies on the substance use of adolescents younger than 15 years old (Svensson, Citation2000). Thus, this paper contributes to new knowledge.
Factors related to early onset of substance use in adolescence
Hanna et al. (Citation2001) indicate that early onset of smoking is an indicator of problem behaviors and those who start smoking at age 13 or younger were more likely to use alcohol, drugs and have school problems (Hanna et al., Citation2001). Studies that explore gender as a predictor for use have shown inconsistent results (Duncan et al., Citation2011): There are studies showing that boys more often than girls drink in early adolescence (Adolfsen et al., Citation2014; Donovan, Citation2004), and studies with the opposite findings, that is, that girls more than boys drink at the age of 13 (Dooley & Prause, Citation2007).
It has been indicated that peer influence is a major cause of initiation to alcohol use and has also been shown that adolescents whose parents had alcohol problems initiated their heavy consumption of alcohol earlier than their peers, e.g.,, (Monahan et al., Citation2009; Pisinger et al., Citation2017). The links to parents are twofold: biological (genetics) and psychosocial (parental norms, communication, modeling, etc.). The present study had no data on genetics, only psychosocial data. Cleveland et al. (Citation2008) have proposed that family factors are more influential in early adolescence, while peers become more influential in mid-adolescence. Other studies have argued that parents exert influence primarily through their norms, while peers do so through their behavior (Pedersen & Skrondal, Citation1998). Therefore, it is reasonable to assume that parents and peers influence adolescents’ consumption of different substances, possibly in diverse ways. Although many studies claim there is an association between early substance onset and later problems (Grant & Dawson, Citation1997; Pitkänen et al., Citation2005), there are few studies aiming to answer the question of why (Rossow, Citation2006). However, Maimaris and McCambridge (Citation2013) suggest that there is no robust evidence of effects of age of first drink on later drinking-related problems. Early onset of drinking and extensive use of alcohol can be related to personality traits such as impulsivity and a lack of behavioral control, such as delinquency (Donovan & Jessor, Citation1985). Norström and Pape (Citation2012) found evidence supporting a combined explanation, since extent of use predicts later problems also when impulsivity and delinquency are controlled for.
Aim of study
The aim of this study was to investigate age of onset and prevalence of substance use in early adolescence, i.e., among 13- to 14-year-old girls and boys. Furthermore, we investigated which factors are most strongly associated with early onset in the use of tobacco, alcohol-drinking, alcohol-drunkenness, and use of drugs.
Materials and methods
This study is part of a multidisciplinary research program, Longitudinal Research on Development In Adolescence (LoRDIA), which follows adolescents from the age of 12 and 13 until they are adults, focusing on health and ill-health, substance use and misuse, family and peer relations, integration and school functioning, by panel surveys and school register data in four waves. All students in sixth and seventh grades (12– 13 years old) in four small- and medium-sized municipalities in the south of Sweden – with 9,000 to 36,000 inhabitants – were invited to participate via letters delivered to their parents through mail and to the students themselves through their schools. Two are classified as ‘Product manufacturing municipalities,’ one is a ‘Commuting municipality’ and the forth is classified as ‘Suburb to larger city.’ When combined, these four communities have the very same percentage of adult population with higher education as the national average (i.e., 30%) (Statistics Sweden [Statistiska centralbyrån], Citation2017).
The information letter was translated into 32 different languages to match the parents’ first languages as provided from school registers. The letters informed about the study, including opt-out consent; i.e., the parents were given the opportunity to decline their child’s participation, as was the child. The study was approved by the Regional Research Review Board in Gothenburg (No.362–13: 2013-09-25, 2014-05-20).
The data were collected through comprehensive self-report questionnaires (paper and pencil in Swedish language) distributed yearly in classroom by the research team. Anyone who needed got assistance to understand the questions. The questionnaires in each wave had first been piloted in student samples of the same age, including students with cognitive disabilities, and somewhat adapted to ensure that they were understood and manageable to all students. Therefore, no students were excluded. It took about one hour to complete for most, and about 20 min more for students with cognitive disabilities, after some of these were offered help in reading. Additionally, register data were collected from the schools on absenteeism and academic achievements for all students. This study concerns the first two waves, which were conducted in 2013 and 2014, the latter when the students were 13 and 14 years old. No incentives were offered in these two waves.
The study population and the two samples
The numbers of invited students, and those who opted out, changed in the first two years. In the first year, 2,108 students were invited. Of these, 318 opted out (202 on parents’ decision, and 116 on students’ own decision). In the second year, 64 changed their previous decisions and opted in (9 change of parents’ decision and 55 students’ decision). In addition, 42 new students were invited since they had moved to the municipalities. None of these opted out. Therefore, the study population increased from 1,790 in Wave 1 to 1,896 in Wave 2.
Not all students in the study population participated in the data collections. In Wave 1, the number of participants was 1,515 (85% of the 1,790 students in the study population at the time), In Wave 2, the number of participants was 1,459 (77% of the 1,896 students in the final study population). In total, 1,716 students participated by completing the questionnaires in one or both of the two waves (91% of the final study population). These students constitute Sample I, used for estimating the prevalence and onset age of substance use. The 1,459 respondents in Wave 2 constitute Sample II, which was used to analyze factors associated with the early onset of substance use.Footnote1
Variables on substance use
Substance use: All questions regarded use of the specified substances over the past 12 months were put into dichotomous variables (yes/no): Tobacco use (two questions: having used cigarettes and having used snuff (snus in Swedish)Footnote2; Alcohol use (more than one glass); Alcohol drunkenness (having ever been drunk); and Drug use (two questions: having used cannabis and having used other kinds of drugs).
Age of onset: The onset ages of using various substances were based on the questions ‘How old were you when you used the following substances for the first time (specifying the above), if ever?’ The students were given the following options: 11 years or younger, 12 years, 13 years, 14 years, and never.
Internal validity, i.e., within waves, was estimated using the data on whether the students had used the substances, based on the pairs of questions above. Absolute agreement was substantial or almost perfect.Footnote3
The consistency of data between waves concerning substance use and onset was checked comparing replies in Waves 1 and 2 (paired data, based on 1265 who participated in both waves). We estimated the systematic correlation (Gamma) of onset age. The Gamma for alcohol use was satisfactory, while for alcohol drunkenness, tobacco, and drugs, the Gamma values were almost perfect.Footnote4 Therefore, the data on all substances were regarded as highly consistent.Footnote5 Data from the two waves were combined to get a complete dataset for Sample I. For onset age, the data of Wave 1 were primarily used, because the earliest time was most likely to give a better opportunity to recall the exact time of previous onset. Non-users in Wave 1 were given the onset data from Wave 2, and new participants in Wave 2 were added.
Factors associated with early onset
Factors associated with early onset were analyzed in Sample II, collected in Wave 2. The demographic variables were Gender (girl/boy); Age (13 or younger/14+); and Ethnicity (Swedish background/other) which was constructed from three questions: Whether students took Swedish as a second language in school, were born in another country, or spoke languages other than Swedish at home. Three items concerned the availability of substances: Availability of tobacco, Availability of alcohol, and Availability of drugs were all based on yes/no-questions (i.e., would it be possible for you to get hold of the following items within 24 hrs from now? Cigarettes, beer, legal alcohol, smuggled alcohol, cannabis, etc.) Here, all types of alcohol were combined, as were different kinds of tobacco.
There were several psychological variables, constructed as index scales. Internal consistency in these scales is represented as Cronbach´s alpha-values in parentheses (α), as measured in Sample II. Alpha values above 0.70 were regarded as satisfying, while alpha values above 0.50 were regarded as acceptable for group analysis (Streiner & Norman, Citation1989).
The behavior scale used was the Delinquent Behaviors Scale, a shorted version of a longer scale from The Swedish National Council for Crime Prevention (BRÅ), and comprised nine questions (e.g., If and how often [have you] destroyed streetlamps or windows, stolen belongings from others, bought or sold stolen goods, been armed). Due to skewness, the variable is here dichotomized as to No or minor (0–1 points) vs. Yes, some, or frequent delinquent behavior (2+ points). Personality dimensions were measured using the Junior Temperament and Character Inventory (J-TCI), which is the TCI version for adolescents. The TCI and J-TCI were based on Cloninger’s bio-psycho-social model of personality and consisted of four temperament scales and three-character scales (Cloninger et al., Citation1994). The Swedish version of J-TCI was validated based on the LoRDIA data (Boson et al., Citation2017). The temperament scales were: Novelty-seeking (e.g., impulsivity, need for excitement and exploration; 18 items; α =.69); Harm avoidance (e.g., emotionality, anxiety, fear of the unknown; 20 items; α = 82); Reward dependence (e.g., reward-seeking behavior, attachment, and social dependence; nine items; α = .58); and Persistence (e.g., endurance, commitment to complete tasks despite fatigue; six items; α = .31). Due to poor consistency, the subscale Persistence was not included in our analysis. The character scales were: Self-directedness (e.g., goalsetting, ability to fulfill, self-acceptance; 20 items; α = .73); Cooperativeness (e.g., cooperation with and tolerance of others, empathy, and helpfulness; 20 items; α = .69); and Self-transcendence (e.g., spiritualism, feeling united with the world; 10 items; α = .71). Svrakic et al. described maturity as a combination of self-directedness and cooperativeness (Svrakic et al., Citation1993). These two scales were summed into a variable called Maturity (40 items, α = .78).
Emotional maltreatment was based on two subscales from the Childhood Trauma Questionnaire (CTQ), Emotional Abuse, and Emotional Neglect (Bernstein & Fink, Citation1998; Gerdner & Allgulander, Citation2009). An example of an Emotional Abuse question is: ‘People in my family called me things like “stupid,” “lazy,” or “ugly.”’ An example of an Emotional Neglect question is: ‘There was someone in my family who helped me feel that I was important or special’ (reversed scoring). The scales consisted of five items each, with replies using five-point Likert scales. However, due to skewness, the two scales were here combined and dichotomized (yes/no) as being over the threshold for more than minimal problems. Emotional symptoms were a subscale from the Strengths and Difficulties Questionnaire, SDQ (Goodman, Citation2001) that included five items (e.g., ‘I am often sad, feeling low, or want to cry’), with replies using three-point Likert scales (α = .76). Psychological health (CHESS, Citation2012) measured positive health with three items (e.g., ‘How do you enjoy life right now?’) and replies using three- and four-point Likert scales (α = .76).
Three psychosocial scales were used, measuring family climate (Bloom, Citation1985): Family conflict (e.g., ‘Members of my family seldom lose their temper’ [reversed coding]) (α = .64), Family cohesion (e.g., ‘In my family we help and support each other’) (α = .71), and Family sociability (e.g., ‘My family feels uncomfortable when interacting with others’ [reversed coding]) (α = .62). Another family-relation scale used was Perceived parental approval of substance use. It was created for LoRDIA and consists of five questions (i.e., ‘It is ok for my parents that I … use alcohol/cannabis/cigarettes/snus/get drunk’), with replies using four-point Likert scales. These items were first combined to one index scale, indicating some perceived parental tolerance for adolescent substance use. Due to skewness, however, this was then dichotomized to ‘Yes, approve of some substances’ vs. ‘No, approve of no substances.’ Since items concerning various substances were combined, the scale does not indicate parental acceptance of the adolescent’s particular use, only some more permissive attitude of some substance use as perceived by the youngster.
Two scales concerned peer factors: Being out with friends was a scale consisting of three questions (e.g., ‘Being out in the town in the evenings without doing anything special’ (α = .58). Substance use and problem behaviors among friends was constructed for LoRDIA based on seven items (e.g., ‘How many of your friends (inside and outside of school) smoke/use snuff/have tried drugs/think it’s ok to belong to a group that uses drugs’). Replies used a four-point Likert scale (α = .89).
Two variables concerned different aspects of the socio-economy: Problematic housing area is a scale based on four items (e.g., ‘Vandalism is common where I live’) and dichotomized to yes (approve some items) or no (not approve). The student’s economic situation, originally from the CAN survey (Gripe, Citation2015), was an item that compared the respondent’s economic situation to that of his or her classmates (less, about the same, more).
Statistical analyzes
Descriptive data were used to investigate the onset ages and prevalence of substance use (), and candidate predictor variables (), in relation to gender and cohort age. Chi-square tests and independent-sample t-tests were used to test the significance of differences between the groups. Based on the Bonferroni correction, only p-values below .001 were considered statistically significant in .
Table 1. Prevalence of substance use among 13- and 14-year-old girls and boys (Sample II) in the past 12 months, by gender and age.
Table 2. Description of factors potentially associated with early substance use, compared between gender and age.
Bivariate logistic regression analyses were conducted to evaluate which factors were associated with the use of different substances. Variables that were statistically significant in the bivariate models were entered into multivariate logistic regression models using the Wald forward selection method, in order to further evaluate which variables were most strongly associated with the outcomes. All potential explanatory variables were checked for multicollinearity, which was not indicated. All statistical analyses were conducted using SPSS 21.
Results
Onset ages of different substances
and show the average onset ages for substance use among girls and boys, respectively. The respondents reported their age of onset as starting at 11 or younger and continuing up to 14 years, and not yet having used (Sample I).
Figure 1. The percentage that had initiated use of various substances at different ages, girls (N = 861).
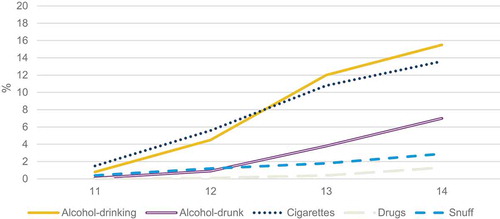
Figure 2. The percentage that had initiated use of various substances at different ages, boys (N = 855).
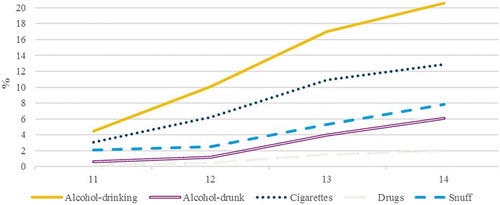
As shown in and , there was a relatively steady increase in the onset of use of various substances from 11 years or younger up to 14 years for both genders, although boys started with somewhat higher percentages at age 11. The boys also appear to have a steeper increase up to 14 years of age with regard to alcohol consumption and using snuff. The other substance use progressions were, however, quite similar between genders, i.e., regarding smoking cigarettes, drinking alcohol to the state of drunkenness, and using drugs.
Prevalence of substance use
shows the prevalence of substance use among students participating in Wave 2 (i.e., Sample II), comparing gender and the two age-groups. Here and in the coming regressions, the two types of tobacco (cigarettes and snuff) were combined to space.
Alcohol and tobacco were the substances most used by early adolescents, although still by a relatively small minority. More boys than girls in early adolescence used alcohol. There were no gender differences in the use of tobacco, alcohol to the state of drunkenness, or use of drugs. Substance use was considerably higher among 14-year-old students, compared to those 13 or younger. This was found for all substance use patterns.
Description of factors potentially associated with the early onset of substance use
presents a descriptive overview of the psychological and social variables potentially associated with substance use in the regressions presented below.
The table shows that there were some statistically significant relationships among the various descriptive variables with regard to gender and age. Boys more often than girls reported emotional maltreatment, but they also reported fewer emotional symptoms and better psychological health. Boys also showed higher scores on novelty-seeking and reported more delinquent behaviors than girls did, while girls reported higher scores on harm avoidance, reward dependence, and maturity compared to boys. The 14-years-old also reported more perceived parental approval of substance use, and more availability of various substances. A less expected result was that 14-year-olds tended to score higher on novelty seeking.
Factors associated with substance use among 13- and 14-year-olds
Based on Sample II, the logistic regression analyses of factors potentially associated with four types of substance use (tobacco use, alcohol drinking, alcohol drunkenness, and drug use) were tested in steps (see Statistical Analyses above). To save space, only the optimized models are shown in . (The outcomes of the bivariate analyses are available upon request).
Table 3. Prediction of early use of tobacco, alcohol-drinking, alcohol-drunkenness, and drug use in Swedish 13- and 14-year-olds. Inclusion order (step), Odds ratios (OR) with 95% confidence intervals (95% CI) estimated by logistic multivariate regression analyses, using the Wald forward selection method.
shows that all four models succeeded in capturing relatively good predictive ability, with R2 between .40 and .52. To help interpretation, a few examples are given. Availability of the specific drug increases the odds of using cannabis by nearly 25 times and tobacco by nearly 16 times. The odds ratio (OR) of novelty-seeking for alcohol drinking was 1.30, which can be interpreted as indicating that the odds of drinking increase by 30%, which is also a very impressive figure from novelty-seeking moving up just 1/18 on the scale. The corresponding figures on length of the other scales are given in the table. also presents the steps in which the variables were entered in the model.
Four groups of variables crystallized as the predictors in the optimized models of various patterns of substance use in early adolescence. The availability of the respective substances (tobacco, alcohol, and drugs) constituted the first group of predictors. The second group, the psychological and behavioral factors of the adolescents, included novelty-seeking and delinquent behaviors. The third group included two family relationship factors, i.e., the perceived parental approval of substance use and family conflict. The fourth group concerned peer relationships, i.e., being out with friends in the evenings, and substance use and problem behavior among peers.
The model predicting tobacco use included more variables than the other models. These were, in order of inclusion: Availability of tobacco, perceived parental approval, delinquent behavior, being out with friends, novelty-seeking, and substance use and behavior problems among peers. The model for alcohol drinking included, in rank order, perceived parental approval, novelty seeking, delinquent behavior, availability of alcohol, and being out with friends. The next model concerned alcohol consumption to the state of drunkenness and included delinquent behavior, perceived parental approval, and family conflict. Lastly, the model for drug use included delinquent behavior and availability of drugs.
Discussion
The present study contributes to knowledge about early onset of substance use by estimating the courses of onset age development for boys and girls in relation to various substance use patterns up to the age of 14, and the actual prevalence for boys and girls 13 and 14 years of age concerning tobacco use, alcohol drinking, drinking to the state of drunkenness, and drug use.
The development of onset shows a steady increase in the proportion of boys and girls who had experienced the onset of different substance use in the ages from 11 to 14 years. The onset curves are quite similar between genders concerning most substances. For two substance use patterns, however, the onset curves of boys increased more rapidly, i.e., alcohol and snuff use. We have not seen curves of this type published before, but estimates of onset at different ages have often been published and the development of substance use in this period has been discussed (Dooley & Prause, Citation2007). The results in this study are consistent with previous Swedish studies on 15- and 16-year-olds (Gripe, Citation2015), in the sense that alcohol drinking and tobacco use are the most prevalent patterns, while drunkenness and drug use are less frequent. The last two may also be regarded as more deviant and norm-breaking for adolescents, and even for adults. Although smoking and alcohol drinking are indeed related to severe health risks, drunkenness, and drug use also involve particular social, psychological, and neurological risks (Hawkins et al., Citation1992). Bolland et al. (Citation2016) indicated that girls who begin to drink alcohol before they are 12 years old continue to drink noticeably more than other girls until they are 17 years old or more. In the present study, 1% of the girls had experience of alcohol use in preadolescence and might according to the study be a risk group for future alcohol-related problems.
The present study uses multivariate regression models were used to extract the main factors explaining early onset in four substance-use patterns from a large number of different psychological and social factors. Those factors that contributed the most were selected for optimized models, i.e., parsimonious models with a relatively good predictive ability. The factors can be grouped into four categories: Availability of substances, psychological behavioral factors of the adolescent (novelty-seeking, delinquent behavior), family relationship factors (perceived parental approval, family conflict), and peer relationship factors (being out with friends in the evenings, and substance use and behavioral problems among friends).
The findings indicate that availability tends to be strongly associated with tobacco and drug use as well as with alcohol drinking. However, it was not associated as a statistically significant variable in the final multivariable model of alcohol drunkenness. To reduce availability has been a traditional focus in Swedish prevention strategies, with restrictions to sell tobacco, snuff, and alcohol to adolescents, and criminalizing possession of drugs. Despite an acceptance in the general population for these restrictions, they cannot succeed alone. Therefore, the person in focus as well as the social network are also expected factors to show up as factors explaining substance use.
Among the psychological behavioral factors, novelty-seeking predicts the early onset of the use of tobacco and alcohol-drinking but not the more norm-breaking patterns of drunkenness or the use of drugs. Novelty-seeking is a heritable temperament factor, related to impulsivity and sensation-seeking, i.e., willingness to search for sensations, and found to represent an increased risk of adolescent substance use (Lubman et al., Citation2004). It has been found to be strongly related to alcohol problems in adults, especially those with early onset and rapid course, i.e., ‘Type II alcoholism’ (Cloninger et al., Citation1996). Therefore, this finding is of interest through its lack of prediction of drunkenness and use of drugs at early onset of 13–14-year-olds. Instead, delinquency was shown to be the primary predictor of drunkenness and of drug use in this early age; and it also appears to contribute to early onset of the other substances.
Both these factors are associated with out-acting personality and risky behaviors, but in theory, they relate to different cerebral systems. While novelty seeking indicates an inclination to be more easily excited, delinquent behaviors indicate problems of inhibition Both are moderately heritable, and both may increase risks, especially so when combined. Still, they should not be mixed up, since prevention and guidance may focus differently. Thus, personality is important, but also more complex. Although maturity as measured in the JTCI was not yet a significant factor in this age, personal growth should later help to handle such risks. Maturation depends on social relations, which leads us to family and peer factors (Cloninger et al., Citation1994).
The importance of the family was captured by two variables: Perceived parental approval of substance use, and Family conflict. Our findings indicate that these factors are important, especially perceived parental approval. This variable is one of the strongest predictors for early onset in the use of tobacco, drinking of alcohol and drunkenness. It is however not a predictor of the use of drugs. These findings are partly in accordance with Chassin et al. (Citation2009) who claim that adolescents with parents who are permissive, neglectful, or uninvolved tend to be more influenced of their peers’ substance use, and that this might also include early onset. The study adds evidence to the claim that at 13–14 years of age, family factors are influential (Cleveland et al., Citation2008), and that parents exert influence through their norms (Pedersen & Skrondal, Citation1998). When parents neglect to communicate norms, the adolescent lacks parental guidance in these matters. Parallel studies based on the LoRDIA, show that style of that communication is indeed important, especially for those disruptive temperaments (Kapetanovic et al., Citation2017).
The two peer factors contribute only moderately as predictors: Being out with friends predicts use of tobacco as well as alcohol, but not the two more norm-breaking patterns, i.e., drunkenness and drug use. In agreement with Cleveland et al. (Citation2008) (.), the study indicates that the influence of peers at this age is not as strong as family factors. The results of this study show that adolescents’ personality and family factors are stronger predictors on early onset among 13–14-year-old adolescents than peer influences. Such findings are likely to change when the study is repeated in mid-adolescence (Donovan & Molina, Citation2011).
The findings of the present study suggest that it is vital to adapt prevention strategies to take into account both age and type of substance, with selected interventions aimed at the multifactorial character of early adolescent substance use such as availability, parents and others toward peers.
Strengths and limitations
Although the statistically significant associations observed in this study do not necessarily indicate causality, the findings suggest that the phenomenon is multi-factorial. This study had the opportunity to include a broad menu of variables. Still, other studies might produce functioning models based on other variables.
The LoRDIA does not yet provide data directly on heredity. Heritability is, however, not a precise factor, because there is not just one genetic link influencing substance use, but many, including the two personality factors discussed above. Heritability also includes social heritage, which is here represented by parental norms. Therefore, heritability is in other ways represented in the models. We also lack data on socioeconomic status of the family (e.g., family income and parents’ education). This limitation results from collecting data with student questionnaires, and at this age it was judged that they could not provide valid data on those factors.
Despite the longitudinal design of the LoRDIA, this study is limited to cross-sectional analysis, since it focuses on the very beginning, i.e., the onset, of substance use. Later studies will have a more developmental character.
There are other limitations that should be addressed. Representativeness of the data depends on the chosen municipalities, those who opted out, and those who actually participated. The four communities are small and middle-sized and one of them is close to one of the largest cities. Taken together, these had the same distribution of education as the country. Those who opted out did not differ from the study population in terms of gender, migration status, academic merits, or absenteeism. Of the remaining study population, 91% were present and responded to questionnaires in one or both waves. There were modest gender differences in response rate, and non-responders had somewhat more often migrated to Sweden, had lower academic merits, and were absent significantly more often. The latter, however, were still on a very low level, having a mean absence of only about 2% more than the participants, which does not signify problematic absenteeism. The combined response rate among immigrant students in one or both waves was still quite high (87%).
Data quality was assessed in several ways. The internal validity of substance use variables showed nearly perfect agreement within waves, and consistency in replies between the waves was substantial. Most scales had been previously tried in studies on adolescents, although some were modified to be manageable also for student with cognitive problems. Others were constructed for use in the LoRDIA data set. The scales had construct validity and internal consistency of scales was checked were shown to be satisfactory or at least acceptable for group analyses. Thus, the data are of acceptable quality in terms of validity and reliability.
Conclusion
In conclusion, the present study is one of few that highlights onset age in various substance use and prevalence among early adolescents in Sweden. The results demand reflection over key elements of preventive programs against early onset. The traditional focus on availability is not enough. Individual personality factors and parental norms seem to be most important in this age, with some additional contribution of peer group factors. As they grow older, the relationships between these may shift, and other factors may occur.
This should have some practical implications, possibly explaining some of the difficulties in forming successful preventive programs (SBU, Citation2015). In other words, preventive measures need to be applied differently to different age groups. This study demonstrates the multifactorial character of early adolescent substance use. Prevention of substance use needs to integrate support to in the adolescents personal development, and to help their parents in this mission, based on the knowledge that personal preconditions differ. There are still many unanswered questions. Future studies should replicate the importance of various factors in older age groups, for use, heavy use, and development of dependence. The change over time concerning associated factors should be studied longitudinally.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
Notes
1 Based on register data from the school administrations, the study population was compared to all invited students in terms of demographic details (including gender and immigration status, the latter of which was indicated by studying Swedish as a second language), and school achievements (grade merits and absenteeism, including sick leave as well as other permitted and non-permitted absences). There were no significant differences in demographic details or in school achievements between the study population and those who opted out. Within the study population, those who were absent and did not participate in data collection were compared to those who were present and took part. Thus, both Sample I and Sample II were compared to non-participants within the study population. Girls participated somewhat more than boys (Sample I: 94% vs. 91 %; Sample II: 88% vs. 83%). Immigrant students participated less than other students (Sample I: 87% vs. 92%; Sample II: 82% vs. 90%). Non-participants were absent from school more often (percentage of hours per year) than participants (Sample I: 7.6 [±6.8] vs. 6.2 [± 6.3]; Sample II: 7.4 [±7.5] vs. 6.1 [±6.2]) and had lower merit points (Sample I: 184 [± 60.4] vs. 206 [± 45.0]; Sample II: 195 (±53.4) vs. 207 (±43.8)). It should be noted that among students of foreign decent, about half were studying Swedish as a second language, signifying that these persons were not only immigrants, but also lacked a functional grasp of Swedish when they started in Swedish school. Some of them may have immigrated quite recently, because there was a large influx of refugees in those years. Therefore, they were expected to face greater difficulties in school. Those who studied Swedish as second language had significantly lower merit points (p < .001) and more absenteeism (p < .003) compared to others.
2 Chewing tobacco is a practically non-existing in Sweden, probably due to the tradition of snuff using. E-cigarettes and vaping are also extremely un-common, and especially among those who never smoked cigarettes (Gripe, Citation2015).
3 Absolute agreement varied from 99.1% to 99.9% (Wave 1) and from 97.9% to 98.9% (Wave 2), except for using alcohol (not specified as being drunk), in which agreement was 91.1% and 93.1%, respectively, in the two waves. The reason for the lower agreement regarding alcohol use may be that the question specified ‘at least one glass,’ which was not the case in the paired onset question.
4 The Gamma was 0.78 for alcohol use and 0.95 for alcohol drunkenness. The correlation concerning use of other substances varied from 0.92 (cigarettes) to 0.96 (snuff) and 0.97 (cannabis).
5 In addition, 3.4% of those who in the first wave reported having never consumed alcohol, reported in the second wave that they had. The corresponding figures were as follows: for getting drunk, 0.5%; smoking a cigarette, 1.5%; using snuff, 0.6%; and using cannabis, 0.2%. These could not be interpreted as a lack of consistency, but rather new users.
References
- Adolfsen, F., Strøm, H. K., Martinussen, M., Natvig, H., Eisemann, M., Handegård, B. H., & Koposov, R. (2014). Early drinking onset: A study of prevalence and determinants among 13‐year‐old adolescents in Norway. Scandinavian Journal of Psychology, 55(5), 505–512. https://doi.org/10.1111/sjop.12151
- Ander, B., Abrahamsson, A., & Bergnehr, D. (2017). ‘It is ok to be drunk, but not too drunk’: Party socialising, drinking ideals, and learning trajectories in Swedish adolescent discourse on alcohol use. Journal of Youth Studies, 20(7), 841–854. https://doi.org/10.1080/13676261.2016.1273515
- Bernstein, D., & Fink, L. (1998). CTQ: Childhood trauma questionnaire: A retrospective self-report. Psychological Corp.
- Bloom, B. L. (1985). A factor analysis of self‐report measures of family functioning. Family Process, 24(2), 225–239. https://doi.org/10.1111/j.1545-5300.1985.00225.x
- Bolland, K. A., Bolland, J. M., Tomek, S., Devereaux, R. S., Mrug, S., & Wimberly, J. C. (2016). Trajectories of adolescent alcohol use by gender and early initiation status. Youth & Society, 48(1), 3–32. https://doi.org/10.1177/0044118X13475639
- Boson, K., Brändström, S., & Sigvardsson, S. (2017). The Junior Temperament and Character Inventory (JTCI): Psychometric properties of multi-informant ratings. Psychological Assessment, 30(4), 550-555. https://doi.org/10.1037/pas000513
- Chassin, L., Hussong, A., & Beltran, I. (2009). Adolescent substance use. In R. M. Lerner & L. Steinberg (Eds.), Handbook of adolescent psychology (pp. 723–757). Wiley.
- CHESS. (2012) . Skolans betydelse för barns och ungas psykiska hälsa [The importance of schools for youth mental health]. Stockholms Universitet: Centre for Health Equitity Studies.
- Cleveland, M. J., Feinberg, M. E., Bontempo, D. E., & Greenberg, M. T. (2008). The role of risk and protective factors in substance use across adolescence. Journal of Adolescent Health, 43(2), 157–164. https://doi.org/10.1016/j.jadohealth.2008.01.015
- Cloninger, C. R., Przybeck, T. R., & Svrakic, D. M. (1994). The Temperament and Character Inventory (TCI): A guide to its development and use. Center for Psychobiology of Personality, Washington University.
- Cloninger, C. R., Sigvardsson, S., & Bohman, M. (1996). Type I and type II alcoholism: An update. Alcohol Research and Health, 20(1), 18-23. PMCID: PM 6876531.
- Donovan, J. E. (2004). Adolescent alcohol initiation: A review of psychosocial risk factors. Journal of Adolescent Health, 35(6), 529.e7–529.e18. https://doi.org/10.1016/j.jadohealth.2004.02.003
- Donovan, J. E., & Jessor, R. (1985). Structure of problem behavior in adolescence and young adulthood. Journal of Consulting and Clinical Psychology, 53(6), 890. https://doi.org/10.1037/0022-006X.53.6.890
- Donovan, J. E., & Molina, B. S. (2011). Childhood risk factors for early-onset drinking. Journal of Studies on Alcohol and Drugs, 72(5), 741–751. https://doi.org/10.15288/jsad.2011.72.741
- Dooley, D., & Prause, J. (2007). Predictors of early alcohol drinking onset. Journal of Child & Adolescent Substance Abuse, 16(2), 1–29. https://doi.org/10.1300/J029v16n02_01
- Duncan, S. C., Gau, J. M., Duncan, T. E., & Strycker, L. A. (2011). Development and correlates of alcohol use from ages 13–20. Journal of Drug Education, 41(3), 235–252. https://doi.org/10.2190/DE.41.3.a
- ESPAD Group. (2016). Results from the European school survey project on alcohol and other drugs (ESPAD Report 2015). European School Survey Project on Alcohol and Other Drugs.
- Gerdner, A., & Allgulander, C. (2009). Psychometric properties of the Swedish version of the Childhood Trauma Questionnaire—Short Form (CTQ-SF). Nordic Journal of Psychiatry, 63(2), 160–170. https://doi.org/10.1080/08039480802514366
- Goodman, R. (2001). Psychometric properties of the strengths and difficulties questionnaire. Journal of the American Academy of Child & Adolescent Psychiatry, 40(11), 1337–1345. https://doi.org/10.1097/00004583-200111000-00015
- Grant, B. F., & Dawson, D. A. (1997). Age at onset of alcohol use and its association with DSM-IV alcohol abuse and dependence: Results from the national longitudinal alcohol epidemiologic Survey. Journal of Substance Abuse, 9, 103–110. https://doi.org/10.1016/S0899-3289(97)90009-2
- Gripe, I. (2015). Skolelevers drogvanor 2015 [Substance use among students 2015] (CAN Rapport 154). The Swedish Council for Information on Alcohol and Other Drugs.
- Hanna, E. Z., Yi, H.-Y., Dufour, M. C., & Whitmore, C. C. (2001). The relationship of early- onset regular smoking to alcohol use, depression, illicit drug use, and other risky behaviors during early adolescence: Results from the youth supplement to the third national health and nutrition examination survey. Journal of Substance Abuse, 13(3), 265–282. https://doi.org/10.1016/S0899-3289(01)00077-3
- Hawkins, J. D., Catalano, R. F., & Miller, J. Y. (1992). Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: Implications for substance abuse prevention. Psychological Bulletin, 112(1), 64. https://doi.org/10.1037/0033-2909.112.1.64
- Kapetanovic, S., Bohlin, M., Skoog, T., & Gerdner, A. (2017). Structural relations between sources of parental knowledge, feelings of being overly controlled and risk behaviors in early adolescence. Journal of Family Studies, 26(2), 226 -242. https://doi.org/10.1080/13229400.2017.1367713
- Lubman, D. I., Yücel, M., & Pantelis, C. (2004). Addiction, a condition of compulsive behaviour? Neuroimaging and neuropsychological evidence of inhibitory dysregulation. Addiction, 99(12), 1491–1502. https://doi.org/10.1111/j.1360-0443.2004.00808.x
- Maimaris, W., & McCambridge, J. (2013). Age of first drinking and adult alcohol problems: Systematic review of prospective cohort studies. Journal of Epidemiology and Community Health, 68(3), 268–274. https://doi.org/10.1136/jech-2013-203402
- Miech, R. A., Schulenberg, J. E., Johnston, L. D., Bachman, J. G., O’Malley, P. M., & Patrick, M. E. (2017). National adolescent drug trends in 2017. Findings released. University of Michigan.
- Monahan, K. C., Steinberg, L., & Cauffman, E. (2009). Affiliation with antisocial peers, susceptibility to peer influence, and antisocial behavior during the transition to adulthood. Developmental Psychology, 45(6), 1520. https://doi.org/10.1037/a0017417
- Norström, T., & Pape, H. (2012). Associations between adolescent heavy drinking and problem drinking in early adulthood: Implications for prevention. Journal of Studies on Alcohol and Drugs, 73(4), 542–548. https://doi.org/10.15288/jsad.2012.73.542
- Pape, H., Rossow, I., & Brunborg, G. S. (2018). Adolescents drink less: How, who and why? A review of the recent research literature. Drug and Alcohol Review, 37(S1), S98–S114. https://doi.org/10.1111/dar.12695
- Pedersen, W., & Skrondal, A. (1998). Alcohol consumption debut: Predictors and consequences. Journal of Studies on Alcohol, 59(1), 32–42. https://doi.org/10.15288/jsa.1998.59.32
- Pisinger, V. S., Holst, C. A., Bendtsen, P., Becker, U., & Tolstrup, J. S. (2017). Perceived parental alcohol problems and drinking patterns in youth: A cross-sectional study of 69,030 secondary education students in Denmark. Preventive Medicine, 105, 389–396. https://doi.org/10.1016/j.ypmed.2017.01.003
- Pitkänen, T., Lyyra, A. L., & Pulkkinen, L. (2005). Age of onset of drinking and the use of alcohol in adulthood: A follow‐up study from age 8–42 for females and males. Addiction, 100(5), 652–661. https://doi.org/10.1111/j.1360-0443.2005.01053.x
- Rossow, I. (2006). Inferences of associations and implications for prevention: the case of early drinking onset. In Elster J, Melberg H. O., and kog, O., (eds (eds), Pp. 259-272. explaining behavior: Essays in hounor of Ole-Jörgen Skog. Oslo: Unipub forlas/Oslo Academic press: Understanding choice.
- Sande, A. (2002). Intoxication and rite of passage to adulthood in Norway. Contemporary Drug Problems, 29(2), 277–303. https://doi.org/10.1177/009145090202900204
- SBU. (2015). Interventions to prevent misuse of alcohol, drugs and gambling in youth. Swedish Agency for Health Technology Assessment and Assessment of Social Services.
- Statistics Sweden [Statistiska centralbyrån]. (2017). Befolkningens utbildning [Population education level]. Statistics Sweden. http://www.scb.se/hitta-statistik/statistik-efter- amne/utbildning-och-forskning/befolkningens-utbildning/befolkningens-utbildning/
- Steinberg, L. (2017). Adolescence (11th ed.). McGraw Hill Education.
- Streiner, D. L., & Norman, G. R. (1989). Health measurement scales: A practical guide to their development and use. Oxford University Press.
- Svensson, R. (2000). Risk factors for different dimensions of adolescent drug use. Journal of Child & Adolescent Substance Abuse, 9(3), 67–90. https://doi.org/10.1300/J029v09n03_05
- Svrakic, D. M., Whitehead, C., Przybeck, T. R., & Cloninger, C. R. (1993). Differential diagnosis of personality disorders by the seven-factor model of temperament and character. Archives of General Psychiatry, 50(12), 991–999. https://doi.org/10.1001/archpsyc.1993.01820240075009
- Velleman, R. (2009). Influences on how children and young people learn about and behave towards alcohol: A review of the literature for the Joseph Rowntree Foundation (part one) (1859357156). Joseph Rowntree Foundation.