
Abstract
Objectives: The ultimate goal of this research is to reduce thoracic injuries due to traffic crashes, especially in the elderly. The specific objective is to develop and validate a full-body finite element model under 2 distinct settings that account for factors relevant for thoracic fragility of elderly: one setting representative of an average size male and one representative of an average size Japanese elderly male.
Methods: A new thorax finite element model was developed from medical images of a 71-year-old average Japanese male elderly size (161cm, 60 kg) postmortem human subject (PMHS). The model was validated at component and assembled levels against original series of published test data obtained from the same elderly specimen. The model was completed with extremities and head of a model previously developed. The rib cage and the thoracic flesh materials were assigned age-dependent properties and the model geometry was scaled up to simulate a 50th percentile male. Thereafter, the model was validated against existing biomechanical data for younger and elderly subjects, including hub-to-thorax impacts and frontal impact sled PMHS test data. Finally, a parametric study was conducted with the new models to understand the effect of size and aging factors on thoracic response and risk of rib fractures.
Results: The model behaved in agreement with tabletop test experiments in intact, denuded, and eviscerated tissue conditions. In frontal impact sled conditions, the model showed good 3-dimensional head and spine kinematics, as well as rib cage multipoint deflections. When properties representative of an aging person were simulated, both the rib cage deformation and the predicted number of rib fractures increased. The effects of age factors such as rib cortical thickness, mechanical properties, and failure thresholds on the model responses were consistent with the literature. Aged and thereby softened flesh reduced load transfer between ribs; the coupling of the rib cage was reduced. Aged costal cartilage increased the severity of the diagonal belt loading sustained by the lower loaded rib cage.
Conclusions: When age-specific parameters were implemented in a finite element (FE) model of the thorax, the rib cage kinematics and thorax injury risk increased. When the effect of size was isolated, 2 factors, in addition to rib material properties, were found to be important: flesh and costal cartilage properties. These 2 were identified to affect rib cage deformation mechanisms and may potentially increase the risk of rib fractures.
Keywords:
Introduction
Thorax injuries comprise a large amount of injuries sustained by occupants involved in frontal crashes (Carroll et al. Citation2010; Japanese Police Citation2013; Yaguchi et al. Citation2011). The risks of fatal and severe injuries are higher for older than younger occupants (Carroll et al. Citation2010; Wang Citation2013). The reasons for this are increased fragility (break easily) and frailty (do poorly) of thorax due to aging (Wang Citation2013) and because restraint systems are not satisfactorily designed considering these characteristics of older occupants.
In Japan, where the proportion of elderly is the largest (UN 2012) and the occupant stature is smaller than in Europe and United States (Research Institute of Human Engineering Quality of Life 2008), the elderly account for more than half of the traffic related fatalities and severe injuries (Japanese Police Citation2013). Male elderly drivers have the highest risk of sustaining a thorax injury (Yaguchi et al. Citation2011). According to projected societal trends, the current situation will increase in significance not only in Japan but also in most of the developed countries in the following decades (United Nations Citation2012).
Traditionally, experiments with postmortem human subjects (PMHS) have been carried out to provide biomechanical data. Based on such data, response corridors have been developed (Ash et al. Citation2012; Kroell et al. Citation1974; Lebarbé and Petit Citation2012) and used in biofidelity evaluations of current crash test dummies (Lemmen et al. Citation2012, 2013; Shaw et al. Citation2010) and to define injury criteria and thresholds (Davidsson et al. Citation2014). PMHS data can also be used to validate human body finite element (FE) models, which enable assessments of restraint performance early in the design of vehicles and restraints. In addition, these models have the potential to predict injuries in greater detail compared to crash test dummies and can easily be designed to account for population factors such as body size or age-specific characteristics.
The ultimate goal of this research is to reduce thoracic injuries due to traffic crashes, especially in the elderly. The specific objective is to develop and validate a full-body FE model under 2 distinct settings that account for factors relevant for thoracic fragility of elderly: one setting representative of an average size male and one representative of an average size Japanese elderly male.
Method
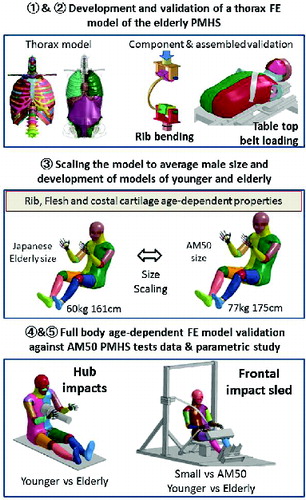
The methodology of this study includes the following steps:
Characterization of the anatomy and biomechanics of a Japanese elderly size PMHS.
Development and validation of a thorax FE model of the elderly PMHS.
Scaling the new model to the AM50 size and implementation of younger and elderly properties.
Full-body age-dependent FE model validation against AM50 PMHS tests data.
Parametric study to evaluate contribution of age factors to rib fracture predictability.
shows a scheme of the methodology used in this study. Detailed explanations of each of the steps are provided below.
Characterization of the Anatomy and Biomechanics of a Japanese Elderly Size PMHS
Computed tomography (CT) images of an elderly PMHS and a series of test data taken from the same specimen (hereafter denoted baseline specimen) were obtained and provided by the University of Virginia Center for Applied Biomechanics Laboratory (Salzar and Subit Citation2014; Subit and Salzar Citation2014). All imaging, testing, and handling procedures were reviewed and approved by an independent oversight committee at the University of Virginia. The baseline specimen selected was a 71-year-old male of 161 cm height and 60 kg weight. The CT images were processed (Mimics v11, Materialise, Leuven, Belgium; Rhinoceros v4, McNeel & Associates, Seattle, WA) to extract the geometry of the rib cage. The geometry was compared to a sample of postmortem CT data sets obtained from 28 Japanese elderly males at Tsukuba Medical/Autopsy Centre in a different study (Ejima et al. Citation2014). The baseline specimen was considered representative of the targeted population by confirming that its rib cage geometry fell within one standard deviation of the limits for rib cage bounding box, rib total length, and rib inclination angle with respect to the spine.
An original series of 10% nominal chest compression tabletop tests was conducted on the baseline specimen (Salzar and Subit Citation2014; Subit and Salzar Citation2014). In the experiments, the specimen was positioned supine and rigidly mounted through the spine to a tabletop test fixture. A 5-cm-wide belt, constructed of spectra fiber-reinforced sail cloth to prevent belt elongation during loading, was positioned across the torso diagonally, passed through a D-ring, and attached to a trolley driven by a hydraulic ram linked to a universal test machine. Ramp and hold anterior thoracic loading was applied at 1.2m/s under 3 different thoracic tissue conditions in chronological order: Intact, denuded (superficial skin, fat, and muscles removed), and eviscerated (organs, vasculature, and visceral fat removed).
After the tabletop tests, components of the specimen were harvested and utilized to conduct bending tests on 9 ribs (Perz et al. Citation2013), intercostal muscle tensile tests (Hamzah et al. Citation2013), and costal cartilage shear tests (Subit and Salzar Citation2014).
Development and Validation of a Thorax FE Model of the Elderly PMHS
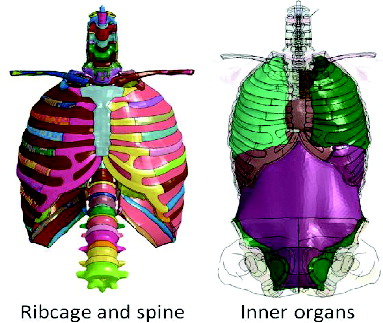
The CT images of the baseline specimen were processed to extract detailed geometry of the thoracic region of the specimen, including ribs, costal cartilage, sternum, clavicles, spine, inner organs (lungs, mediastinum, heart, liver, and a simplified abdominal organ model, including the stomach, intestines, kidneys, and bladder), and a simplified thoracoabdominal flesh model (including skin, muscles, and fat).
Based on the extracted geometry, a mesh was constructed (Hypermesh v11, Altair, Troy, MI). Bones were modeled as an external layer of shell elements, representing the cortical bone, filled with solid brick elements, representing spongy bone. Inner organs were meshed with tetrahedral elements. The attachments between organs and surrounding structures were defined based on anatomy literature and upon consultation with forensic physicians. A model of the external flesh including skin, fat, and thoracoabdominal muscles was built by filling the volume occupied by these structures with combined brick and tetrahedral elements.
A balance between model geometric accuracy and computational time requirements was achieved by establishing a target of minimum calculation timestep of 0.3 ms. All simulations were conducted with LS-DYNA FE code (mpp971s R5.1.1, LSTC, Livermore, CA). The final thorax model, shown in , contains a total of 126,725 shell and 439,448 solid elements of approximate average element size of 3 mm.
Component Validation
Rib models were developed and validated according to a new modeling methodology proposed by Kato et al. (Citation2014). This methodology consists of extracting the geometry of the rib and its variable cortical thickness from the CT images and automatically implementing them into the rib model. Thereafter, a rib bending test is iteratively simulated for different combinations of material parameters (e.g.,Young's modulus, yield stress, etc.), defined within ranges from the literature, until an optimal rib force–displacement response of the rib model is obtained. This methodology was assessed with 9 rib models and the corresponding rib bending tests from the baseline specimen (Kato et al. Citation2014). The variable cortical thickness and the average material properties from the 9 ribs were implemented into all of the ribs of the assembled elderly thorax model. Such properties are presented in (dotted line for elderly properties).
Costal cartilage was modeled as an elastoplastic material with elderly properties derived from Yamada and Evans (Citation1970). The cartilage model was validated by simulating the shear experiments also conducted on the baseline specimen (Subit and Salzar Citation2014). The intercostal muscles were modeled as a viscoelastic material and validated by simulating intercostal tensile tests also conducted on the baseline specimen (Hamzah et al. 2013). The material model and parameters used to simulate the lungs and mediastinum were adopted from Mendoza-Vazquez et al. (2013). In their study, the properties were defined by simulating drop tests with perfused porcine lungs (Hayamizu et al. Citation2003). The liver was modeled with an Ogden rubber material with hyperelastic and rate-dependent characteristics and validated against a series of high-rate compression tests with perfused porcine livers as described in detail by Sato et al. (Citation2013). Finally, the flesh material model was defined as a viscoelastic model with strain rate–dependent stress–strain behavior in compression from PMHS muscle coupon tests in compression (McElhaney et al. 1976) and in tensile according to muscle tissue properties by Yamada and Evans (Citation1970).
Assembled Validation
The validated components were assembled and the structural response of the rib cage was validated by simulating the table-top tests (Salzar and Subit Citation2014; Subit and Salzar Citation2014). A geometrically accurate FE model of the spine constraint system and the load cells array system were developed from the CT images of the specimen, which were taken from the subject with the spinal support bar in the “as tested” position.
Three different versions of the thorax model were built to replicate intact, denuded, and eviscerated tissue conditions. To simulate the experiments, a model of the belt was carefully developed and the carriage displacement curve measured at each of the experiments (Salzar and Subit Citation2014) was prescribed to the carriage model to which the belt ends were attached. To validate the thorax models, belt force vs. table carriage displacement curves from the simulations were compared to those obtained from the experiments, which allowed evaluating the contribution of the different tissues to the thoracic structural effective stiffness of the model.
Scaling the New Model to the AM50 Size and Implementation of Younger and Elderly Properties
The elderly thorax FE model was merged with the head and the extremities of a full-scale model previously developed (JAMA model; Zama et al. Citation2010), producing a full-body model with a total of 684,074 elements. In order to enable validation against existing AM50 PMHS experimental data, the full-body model geometry was scaled up by applying a scaling factor based on body height of 1.09 in the X, Y, and Z directions. In doing so, 2 body size versions were created: the original 60 kg and 161 cm Japanese elderly size model (hereafter denoted small size) and the 77 kg and 175 cm model (denoted AM50 size).
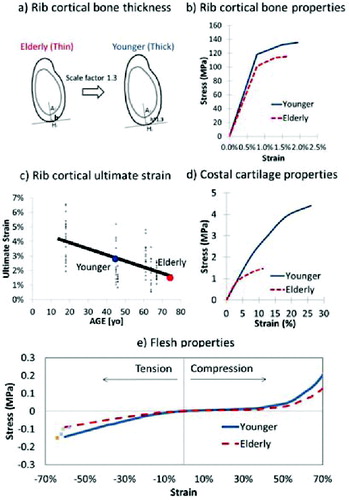
Based on literature data, 5 age-dependent factors (rib cortical thickness, rib cortical material properties, rib cortical failure strain, costal cartilage material properties, and flesh material properties) were implemented in the models using the elderly properties previously defined (representative of 65 to 85 years of age) as a reference to define younger setting (representative of 20 to 40 years of age). summarizes these age-dependent settings and explanations are provided below.
Cortical bone thickness (Stein and Granik Citation1976) and ultimate stress (Burstein et al. Citation1976; Dokko et al. Citation2009; Yamada and Evans Citation1970) decrease with age. Ito et al. (2009) proposed scaling factors for rib cortical bone thickness as a function of age based on Stein et al. (1976) and bone material properties from elderly to adults by increasing elastic modulus and plastic stress in tandem. In the current study, the same approach was applied to scale the thickness (scaling factor of 1.3, according to Ito et al. 2009) and the material properties from our baseline elderly specimen to younger properties as illustrated in .
Age-dependent rib cortical bone ultimate strains were defined by applying linear regression to values obtained from rib cortical bone coupon test data from PMHS of different ages (Kemper et al. Citation2005). This regression line provided an estimation of ultimate failure strain of 1.5 and 3% for 75 and 40 years of age, respectively. shows the experimental ultimate strain values as a function of age by Kemper et al. (Citation2005) and the linear regression line utilized to estimate the elderly and the younger settings in this study.
Age-dependent costal cartilage and muscle tissue tensile ultimate strains reported by Yamada and Evans (Citation1970) were utilized to define elderly and younger settings of the cartilage solid model and the flesh model as shown in . Yamada and Evans's tensile muscle test data were complemented with non-age-dependent flesh compression test data by McElhaney et al. (1976) under the assumption that changes of muscle properties with age are proportional in compression and in tension.
Full Body Age-Dependent FE Model Validation Against AM50 PMHS Test Data
Hub Impacts
Kroell et al. (1974) conducted a series of hub frontal thorax impact tests with PMHS in seated posture with legs and arms straightened and the spine unrestrained. Force–deflection corridors developed from such experiments are currently utilized for evaluation of AM50 crash test dummies (Lemmen et al. Citation2012). Dokko et al. (Citation2011) reprocessed Kroell et al.'s test data by separate younger (8 specimens) and elderly (7 specimens) groups, showing tendencies of stiffer response for the younger. Further reanalysis of these data shows that a smaller number of fractures occurred for the younger (2 on average) in comparison with the elderly (10 on average).
In the current study, the experimental force–deflection age-dependent corridors developed by Dokko et al. (Citation2011) were utilized to validate the thorax response to impacts of the AM50 size model developed. For this, a model of the 24 kg cylindrical impactor used to deliver the impact during the experiments was generated following descriptions from the original publication (Kroell et al. Citation1974). The AM50 size model was positioned seated with the legs and the arms straight. The impactor model was aligned with the center of the thorax in the compressive direction at the fourth rib height. In this setup, 2 impacts were simulated, one with younger and one with elderly properties. The velocity of the impactor just before the impact was set to 6.7 m/s (Kroell et al. Citation1974). The force–deflection response of the thorax and the number of fractures were extracted from the simulations and compared to the corresponding age-dependent corridors and reported fractures.
Frontal Sled
Shaw et al. (Citation2009) conducted a series of 40 km/h frontal impact sled tests with 3 PMHS specimens (averaging 53 years of age, 73 kg weight and 178 cm height). The PMHS were seated on a rigid planar seat, with the feet and knees constrained and the torso restrained with a custom-made 3-point shoulder andlap belt. A video motion tracking system was utilized to measure 3-dimensional trajectories of the body and thoracic deformation. From these experiments, an average of 6 fractured ribs was reported, evenly distributed between the right and the left part of the rib cage.
In the current study, belt load, body motion trajectories, chest multipoint deformation, and number of fractures from the experiments were utilized to evaluate the biofidelity of the AM50 size model with elderly and younger properties. A detailed model of the sled was developed from the original sled (Shaw et al. Citation2009). Boundary conditions were set according to the original experimental data and a frontal impact was simulated by prescribing sled motion measured at the experiments into the sled model. Loads, trajectories, chest deformation measurements, predicted number of rib fractures, and locations of these were extracted from the simulations and compared to those from the experiments.
Parametric Study to Evaluate Contribution of Age Factors to Rib Fracture Predictability
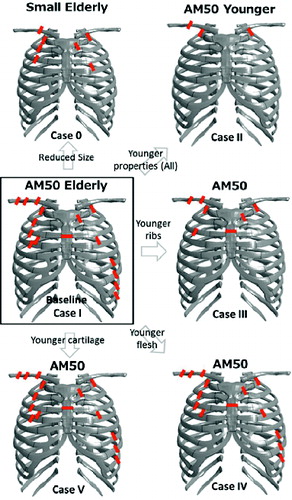
A simulation parametric study was conducted in order to understand the effect of body size and age-dependent thoracic factors on the model under frontal sled conditions. A total of 6 simulated cases were included in the analysis, including one case with the small size and 5 with the AM50 size model. Within the AM50 size model, elderly and younger thoracic characteristicswere combined in order to understand the effect of the age-dependent parameters previously defined. The study design matrix conditions (size- and age-dependent thoracic factors) and the simulation output variables obtained (number of fractured ribs, location of the fractures, shoulder belt peak force, and sternum deflection) are presented in the Results section.
Results
Elderly Thorax Model Validation Against Elderly PMHS Data
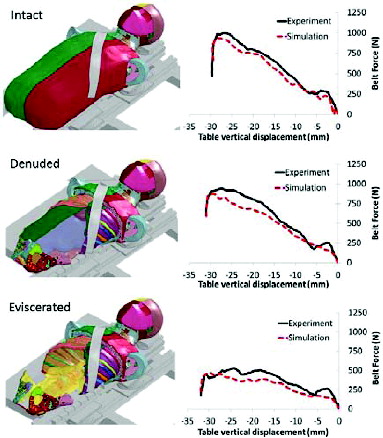
The results of comparing simulations and experiments for each of the tissue conditions under tabletop test conditions are presented in . Force–displacement curves show belt force as measured at the right shoulder side (engaged by the belt) and the table carriage displacement applied to the belt ends both in the experiments and in the simulations. The results show that the force–displacement curves from the simulations (in dotted lines) were in good agreement with the corresponding experimental measurements.
Full Body Age-Dependent Model Validation Against AM50 PMHS Test Data
The results from the validation of the AM50 size model with age-dependent settings against PMHS data are presented in . Hub impactor simulation force–deflection results (, top) show that the models with elderly and younger properties were in agreement with experimental one standard deviation age-dependent corridors. The model with elderly and younger properties predicted 12 and 2 rib fractures, respectively. Sled tests simulation results (, bottom) show head and spine trajectories, shoulder belt loads, and rib cage multipoint deflection from the simulations in comparison to the corresponding experimental measures (Shaw et al. Citation2009). Trajectories of the head and the spine in the x, y, and z directions were objectively evaluated according to a 4-level (poor, moderate, good, excellent) biofidelity ranking system proposed by Rhule et al. (Citation2002). The results (Rhule scores and ranks presented in Table A1, see online supplement) show that head and spinal motions tended to score good to excellent. Similarly, shoulder belt loads (good) and thoracic multipoint deflections (excellent) for both elderly and younger settings presented in were in agreement with the experiments. Under these conditions, the elderly setting predicted 10 fractures (5 on each side of the rib cage) and the younger setting predicted 2 rib fractures.
Parametric Study to Evaluate Contribution of Age Factors to Rib Fracture Predictability
shows the parametric study design matrix including simulated case number (column 1), human body model size and age-dependent properties group (columns 2 to 5), and the simulation results including number of fractured ribs and their location (columns 6 and 7), shoulder belt peak force (column 8), and sternum deflection (column 9). shows schematic images of the rib fracture locations listed in column 7.
![Figure 5 Summary of AM50 size full-body model validation results with younger (blue thick lines) and elderly (red thick lines) settings. (Top) hub impact simulation results for younger and elderly are presented separately against their corresponding one standard deviation PMHS age-dependent corridors (developed by Dokko et al. [Citation2011] from experiments by Kroell et al. [Citation1974]). (Bottom) simulation results for upper body trajectories, shoulder belt forces, and multipoint chest deflections in compressive direction for younger and elderly in comparison to the corresponding experimental measurements from 3 PMHS tests (Nos. 1358, 1359, and 1360 in Shaw et al. Citation2009) in grey continuous lines.](/cms/asset/e71512ca-4cb9-4d41-b0ba-5a24bb39ad4b/gcpi_a_1014552_f0005_oc.jpg)
Table 1 Parametric study design matrix and simulation results
Cases 0 and I allow comparing the effect of body size on fracture output with elderly properties. The small model predicted 5 rib fractures with a peak shoulder belt force of 5,084 N, whereas the larger predicted 10 rib fractures with a peak load of 6,556 N. From cases I to V, the model size was set to AM50, which allows analyzing the differences between elderly and younger properties isolated from body size effects. When all properties were shifted from the elderly to younger (cases I and II), predicted rib fractures decreased from 10 to 2. With case I as a baseline for elderly properties, cases III to V show the effect of implementing younger properties for one factor at a time. From these comparisons, younger rib cortical bone (thickness, material properties, and failure strain level together), younger flesh, and younger costal cartilage produced a reduction of 7, 2, and 1 rib fractures, respectively.
Discussion
Structural thoracic response of the developed elderly thorax modelhas been validated under intact, denuded, and eviscerated conditions (). When the flesh attached to the rib cagewas removed, the resulting effective stiffness decreased by 16% with respect to the intact case. When the inner organs were removed, overall stiffness was about half of that in the intact case. Although only one PMHS was utilized in this validation, the tendencies observed with the model and the experiments, in terms of the contribution of each of the tissue conditions to thoracic effective stiffness, are consistent to an experimental study from Kent et al. (2005) in which 2 PMHS specimens were subjected to comparable tabletop tests with diagonal belt loading under the same tissue conditions as in the present study. Thorax response against hub impacts and sled frontal impacts have been validated with existing PMHS data. Under sled conditions, thorax multipoint deformation behaved in agreement with the experiments regardless of the age-dependent thoracic properties implemented ().
Rib cortical bone was modeled by implementing age dependency for bone thickness, material properties, and failure strain levels. When combining these values with other age-dependent factors such as flesh and costal cartilage properties, the effect of switching from elderly to younger properties reduced predicted fractures from 12 to 2 in hub impacts and from 10 to 2 in frontal impact sled conditions. These numbers of fractures for younger and elderly fall within reasonable margins expected according to those reported from the corresponding experiments (Kroell et al. Citation1974; Shaw et al. Citation2009). Furthermore, when the contribution of aged ribs only was analyzed in frontal sled conditions (cases I and III in the parametric study), a reduction of 7 rib fractures was obtained, which implies that ribs account for a major contribution of the rib fracture output but other factors may also affect. Limitations concerning rib fracture predictability should be noted at this point. Existing rib cortical bone properties in literature show large inter- and intra-specimen variability (Kemper et al. Citation2005). These limitations must be kept in mind when addressing quantified conclusions from current and future studies using the model. Additional experimental work to define statistically significant age-dependent characteristics and statistical approaches for prediction of fractures need to be addressed in the future.
The effect of body size under the same sled impact conditions could be seen when comparing small size (case 0) and AM50 size (case I) in the parametric study, which predicted 5 and 10 fractures, respectively. When setting the restraint systems for these 2 cases, it was ensured that landmark points overpassed by the shoulder belt and angles of the belt with respect to the rib cage were the same in both cases. Hence, the significantly different fracture levels can be attributed to a decrease in energy due to the substantial difference in body mass (77 kg vs. 60 kg) as shown by the forces produced by the seat belt (5,084 and 6,556 N).
Thoracic flesh, fat, and muscles may play a role protecting the rib cage. However, no studies on the effect of aged fleshmuscles on potential injury outcome have been found. By the age of 30, sarcopenia, a degenerative loss of skeletal mass, quality, and strength associated with aging, begins to occur. Muscle strength has usually decreased by about 50% by the age of 80 years (Marieb Citation2010). This decrease is consistent with age dependent material properties reported by Yamada et al. (1970) and was implemented in our model. Isolated aged flesh mechanical properties changes (case I and IV) did play a role on reducing rib fractures nearby the belt path in the simulations, one on the upper (R4) and one on the lower (L9) loaded part of the rib cage.
Costal cartilage may affect load distribution on the rib cage (Forman Citation2009). Simulated case I predicted 10 fractures, mainly concentrated near the belt pass. When only the cartilage material properties were stiffened (case V with respect to case I), a reduction of 1 rib fracture occurred on the lower loaded rib cage (L9). This reduction can be attributed to an increase of work sustained by the stiffer costal cartilage along the belt pass.
An FE model of the thorax has been developed from CT images of an elderly PMHS whose body size and rib cage geometry fall within the average Japanese elderly male population. The model has been validated against an original series of tests obtained from the same specimen. When the model was scaled up to AM50 size and age-dependent properties were implemented, the thorax model presented sensitivity to both size- and age-dependent characteristics in frontal impacts. When elderly settings were considered, the model responded with reduced thorax stiffness and increased rib fracture risk. In descending order, rib cortical bone, flesh, and costal cartilage properties affected the predicted number of rib fractures.
Acknowledgments
Dr. Shiotani and Dr. Hayakawa from Tsukuba Medical Center are sincerely acknowledged for their advice and guidance in human anatomy–related issues.
Supplemental Materials
Supplemental data for this article can be accessed on the publisher's website.
Appendix
Download Zip (17.9 KB)References
- Ash JH, Lessley DJ, Forman JL, Zhang Q, Shaw CG, Crandall JR. Whole-body kinematics: response corridors for restrained PMHS in frontal impacts. Paper presented at: IRCOBI Conference; 2012.
- Burstein AH, Reilly DT, Martens M. Aging of bone tissue: mechanical properties. J Bone Joint Surg. 1976;58:82–86.
- Carroll J, Adolph T, Chauvel C, et al. Overview of serious thorax injuries in European frontal car crash accidents and implications for crash test dummy development. Paper presented at: IRCOBI Conference; 2010.
- Davidsson J, Carroll J, Hynd D, et al. Development of injury risk functions for use with the THORAX demonstrator; an updated THOR. Paper presented at: IRCOBI Conference; 2014.
- Dokko Y, Ito O, Ito Y, Mori F, Ohashi K. Validation of adult and elderly FE thorax models against the age-specific corridors of chest impact [in Japanese]. Paper presented at: JSAE Annual Congress; 2011.
- Dokko Y, Ito O, Ohashi K. Development of human lower limb and pelvis FE models for adult and the elderly. Warrendale, PA: SAE; 2009. SAE Technical Paper No. 2009–01
- Ejima S, Kato R, Mikami K, et al. Morphology analysis with autopsy imaging for characterizing the human ribcages geometry [in Japanese]. Paper presented at: Conference on Computational Engineering and Science; 2014.
- Forman JL. The Structural Characteristics of the Costal Cartilage: The Roles of Calcification and the Perichondrium, and the Representation of the Costal Cartilage in Finite Element Models of the Human Body [PhD dissertation]. Charlottesville, VA: University of Virginia; 2009.
- Hamzah M, Subit D, Boruah S, et al. An inverse finite element approach for estimating the fiber orientations in intercostal muscles. Paper presented at: IRCOBI Conference; 2013.
- Hayamizu N, Watanabe I, Ishihara T, Miki K. Measurement of impact response of pig lung. In Proceedings of JSME Tokai Branch Conference; 2003:
- Ito O, Dokko Y, Ohashi K. Development of adult and elderly FE thorax skeletal models. Warrendale, PA: SAE; 2009. SAE Technical Paper No. 2009-01-0381.
- Japanese Police. Annual report on road traffic fatal accidents and traffic law enforcement violations [in Japanese]; 2013.Available at: https://www.npa.go.jp/toukei/index.htm#koutsuu. Accessed: April 18, 2015.
- Kato R, Yamamoto Y, Antona-Makoshi J, Mikami K, Sato F, Ejima S. A methodology to develop rib finite element models that account for cortical bone thickness [in Japanese]. Paper presented at: JSAE Annual Congress; 2014.
- Kemper AR, McNally C, Kennedy EA, et al. Material properties of human rib cortical bone from dynamic tension coupon testing. Warrendale, PA: SAE; 2005. SAE Technical Paper No. 2005–22-0010.
- Kent R, Murakami D, Kobayashi S. Frontal thoracic response to dynamic loading the role of superficial tissues, viscera and the rib cage. Paper presented at: IRCOBI Conference; 2005.
- Kroell CK, Schneider DC, Nahum AM. Impact tolerance and response of the human thorax II. Warrendale, PA: SAE; 1974. SAE Technical Paper No. 741187.
- Lebarbé M, Petit P. New biofidelity targets for the thorax of a 50th percentile adult male in frontal impact. Paper presented at: IRCOBI Conference; 2012.
- Lemmen P, Been B, Carroll J, et al. Development of an advanced frontal dummy thorax demonstrator. Paper presented at: IRCOBI Conference; 2012.
- Lemmen P, Been B, Carroll J, et al. An advanced thorax–shoulder design for the THOR dummy. Paper presented at: ESV Conference; 2013.
- Marieb E. Human Anatomy and Physiology. San Francisco, CA: Pearson Education, Inc; 2010.
- McElhaney JH, Roberts VL, Hilyard JF. Handbook of Human Tolerance. Tsukuba, Japan: JARI; 1976.
- Mendoza-Vazquez M, Brolin K, Davidsson J, Wismans J. Human rib response to different restraint systems in frontal impacts: a study using a human body model. Int J Crashworthiness. 2013;18:516–529.
- Perz R, Toczyski J, Kindig M, et al. Evaluation of the geometrical properties distribution along the human ribs using different x-ray imaging methods. Paper presented at: IRCOBI Conference; 2013.
- Research Institute of Human Engineering Quality of Life (HQL). Japanese Body Size Data Book 2004–2006 [in Japanese]; 2008. Available at: http://www.hql.jp/database/size2004. Accessed: April 18, 2015.
- Rhule HH, Maltese MR, Donnelly BR, et al. Development of a new biofidelity ranking system for anthropomorphic test devices. Stapp Car Crash J. 2002;46:477–512.
- Salzar R, Subit D. Development of a transfer function for the evaluation of the elderly thoracic response. Paper presented at: JSAE Annual Congress; 2014.
- Sato F, Yamamoto Y, Ito D, et al. Hyper-viscoelastic response of perfused liver under dynamic compression and estimation of tissue strain thresholds with a liver finite element model. Paper presented at: IRCOBI Conference; 2013.
- Shaw G, Parent D, Purtsezov S, Crandall J, Törnvall F. Torso deformation in frontal sled tests: comparison between Thor NT, Thor NT with the Chalmers SD-1 shoulder, and PMHS. Paper presented at: International Proceedings of the IRCOBI Conference; 2010.
- Shaw G, Parent D, Purtsezov S, et al. Impact response of restrained PMHS in frontal sled tests: skeletal deformation patterns under seat belt loading. Stapp Car Crash J. 2009;53:1–48.
- Stein ID, Granik G. Rib structure and bending strength: an autopsy study. Calcif Tissue Res.1976;20:61–73.
- Subit D, Forman J. Shear loading of costal cartilage; 2014. Available at: http://arxiv.org/abs/1405.2308
- Subit D, Salzar R. Ribcage kinematics under belt loading in intact, denuded and eviscerated conditions. In: Proceedings of the JSAE Annual Congress, 2014.
- Wang S. Population variability: influence of crash injury outcomes. In: JSAE Annual Congress Forum, 2013.
- United Nations, Department of Economic and Social Affairs. World Population Prospects: The 2012 Revision. 2012. Available at: http://esa.un.org/wpp
- Yaguchi M, Omoda Y, Ono K, Masuda M. Traffic accident analysis towards the development of and advanced frontal crash test dummy indispensable for further improving vehicle occupant protection performance. In: Proceedings of the ESV Conference, 2011.
- Yamada H, Evans FG. Strength of Biological Materials. Baltimore, MD: Williams & Wilkins; 1970.
- Zama Y, Antona J, Mikami K, et al. Development of finite element human model for events of frontal impact. In: Proceedings of the JSAE Annual Congress, 2010.