
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Objective: The objective of this study was to identify pedestrian risk behaviors that result in traffic accidents and characterization of the accidents experienced by participants in this study to provide information for the generation of integral preventive strategies.
Methods: The study was correlational, descriptive, and transversal and followed a quantitative approach divided into 2 stages. In the first stage, an observational study was performed to identify the manifested risk behaviors of pedestrians, which served as a basis for the construction and design of a questionnaire. In the second stage, the questionnaire was applied to a group of 1,536 participants. Pearson’s correlation coefficient was applied to establish associations between gender and age with respect to risk behaviors.
Results: The 3 behaviors that participants reported performing always or very often include using electronic gadgets (except mobile phones), not using a pedestrian crosswalk, and using a mobile phone. In addition, 18.5% were involved in at least one road accident as a pedestrian in the last 5 years. Of the total number of registered accidents, 21% resulted in pedestrian injuries, 48.3% of which were serious. These were due to external causes not related to human factors or unidentified (58.5%) and behavior factors as a whole (41.4%, 31.5% of which were caused by pedestrians). Pearson’s correlation coefficient showed evidence of a correlation between age and risk behaviors.
Conclusions: All subjects in this study performed several risky actions as pedestrians, at least occasionally, and at least one fifth had been involved in a road accident as a pedestrian. It is known that the surroundings can positively or negatively influence individuals’ behaviors; therefore, once prevention measures are identified, it is possible to influence risk behaviors. Therefore, road safety education and the physical environment must be considered together, and efforts focused on optimum infrastructure also need to consider road safety education.
Introduction
Road accidents represent a serious problem worldwide in public health. The World Health Organization (WHO 2015) estimates that road accidents cause the deaths of 1.25 million people worldwide and was one of the 10 leading causes of death worldwide in 2016 (WHO 2018). This is accentuated in poorer countries, where the death rate associated with road accidents reaches 28.5 deaths per 100,000 inhabitants. Several international studies demonstrate a high incidence of pedestrian injuries due to traffic accidents. The Pan American Health Organization/WHO (2013) reported that in 2010 more than 23,500 pedestrians died on public roads as a consequence of road accidents in Latin America and the Caribbean; worldwide this number increased to 270,000 pedestrians per year. Runovers are a predominant factor in road accidents in Latin America, unlike in developed countries (Cabrera et al. Citation2009).
Bambaren (Citation2004) noted that of 2,001 road accidents registered over a 1-year period in Peru, 58% had consequences for pedestrian, 63% of the serious cases and 78% of the deceased were associated with Pedestrian Traffic Accident. The International Organization of Traffic Accidentology (Citation2015) reported that in the Dominican Republic and Guatemala, the most vulnerable road users are usually pedestrians, and the Secretaría de Salud (Citation2015) has recognized pedestrian accidents as being among the leading 20 causes of death in Mexico for more than 2 decades.
Causal factors identified in most road accidents are human factors (Alfaro-Basso Citation2008; Arias Citation2011). Mako and Szakonyi (Citation2016) identified that 44% of the fatalities in pedestrian crossings in Hungary during the period 2004–2013 were associated with pedestrian behaviors, with the most common risk behavior being crossing the street without precautions (67%).
Likewise, in a study conducted in Mexico, Baptista and Reyes (Citation2014) found that more than 50% of those surveyed stated that they do not use pedestrian crossings regularly. Echeverry et al. (Citation2005) conducted a study in Cali, Colombia, and found that 64.4% of eyewitnesses to a road accident reported that the pedestrian was the main party responsible. Although there are studies that indicate that adolescents are especially vulnerable to accidents due to factors inherent to their age, such as lack of maturity, lack of experience, and reckless behavior (Bustos et al. Citation2014), risk behaviors while using the pathways are present in all age groups to a greater or lesser degree. Zegeer and Bushell (2012) pointed out that there are causes inherent to the individual that influence the incidence of pedestrian accidents, such as age (especially children and the elderly) and disability. Among the elderly, the inherent conditions of their age and/or health lead to risk-taking in their role as pedestrians, mainly including not using bridges or crosswalks, because they have limited mobility and prefer to use shortcuts. Furthermore, today’s society is characterized by the regular use of mobile devices. This influences the behavior of pedestrians and can increase the risk of accidents, because the distraction produced by this activity affects individuals’ abilities to react to an unexpected event (Collet et al. Citation2010). However, Velázquez et al. (Citation2017) pointed out that although there is evidence that human behavior generates risks, this can only be considered as an immediate cause before the accident but not the root cause, because these behaviors are regularly conditioned by the environment, such as road conditions (Koh et al. Citation2014; Uttley and Fotios Citation2017), lack of traffic signs (Olszewski et al. Citation2015), and, more generally, management and regulation of the traffic system. To understand the root problem, it is essential to identify pedestrian risk behaviors that may result in traffic accidents, as well as characterization of the accidents experienced by study participants, in order to provide information for the generation of comprehensive prevention strategies, the objective of the present study.
Geographic context
Chandran et al. (Citation2012) pointed out that, according to the WHO, 90% of fatalities worldwide (approximately 1.16 million) and 92% of road accidents resulting in disability (more than 38 million cases) occur in low- and middle-income countries, though they account for only 48% of registered vehicles worldwide. Therefore, relevant studies and research are needed to address this problem. Information gathering was carried out in the city of Heroica Matamoros, Tamaulipas, Mexico, considering that it reflects the reality of many underdeveloped countries, where, in general, investment in road infrastructure and means of control for regulatory compliance are limited to large cities but scarce in provinces with lower economic income, which promotes risk behaviors by users of public roads in the absence of a road culture promoted by optimal environmental conditions. Similar to other Latin American cities, Matamoros is characterized by road signs practically limited to traffic lights and stop signs, with few pedestrian crossings and narrow or uneven sidewalks, obstructed by objects that limit their use.
Matamoros has a population of 520,367 (National Institute of Statistics and Geography Citation2015), the second-highest population among municipalities in Tamaulipas. As shown in , the number of accidents increased from 2010 to 2016 to 659 per 100,000 inhabitants, with an average of 20.71% of accidents resulting in death.
Table 1. Traffic accidents with pedestrian injuries in Heroica Matamoros, Tamaulipas, 2010–2016.Table Footnotea
Methods
The methodological design was descriptive and correlational. The study is of a transversal type and used a quantitative approach divided into 2 stages. In the first stage, an observational study was conducted to identify risk behaviors manifested by pedestrians. Three intersections with the highest traffic flow in the urban area were selected as observation points, identified from a previous count using a Safe Pace radar, which was located on public lighting poles at an approximate height of 3 m at 7 road crossings. As a result, 3 observation points were established: (1) Sixth Street and Canals, (2) Sixth Street and Blvd. Manuel Cavazos Lerma, and (3) Ave. Lauro Villar and Acción Cívica, which were above average (refers to the average of the number of vehicles that circulate in the seven points where the previous count was made) (2,128 vehicles). For the fieldwork, the observers (2 at each point), were located as close as possible to the bridges and pedestrian steps closest to the intersection.
The information was obtained during 3 working days with a total of 12 h of observation divided into 2 daily periods as follows: Monday from 7:00 a.m. to 9:00 p.m. and 2:00 p.m. to 4:00 p.m., Wednesday from 9:00 a.m. to 11:00 a.m. and 4:00 p.m. to 6:00 p.m, and Friday from 11:00 a.m. to 1:00 p.m. and 6:00 p.m. to 8:00 p.m. People with visible mobility problems, such as the use of a cane, crutches, or wheelchair, were ruled out and it was ensured that the pedestrian paths were in condition to be used.
In the second stage a survey was applied, for which sample selection was based on a nonrandom convenience sample. The inclusion criteria were as follows:
Was a pedestrian.
Was 14 years of age or older.
Was an inhabitant of the city.
The sample was calculated probabilistically, based on the following formula:
(1)
(1)
where Z = 1.96, α = 0.05, e = 0.025, and p = 0.5.
A confidence level of 95%, accuracy of 2.5%, and maximum variance were assumed. The sample for phase 2 included 1,536 participants.
The design of the questionnaire was made based on the referents of the previous observational study, in which the risk behaviors observed in 9 affirmative statements were classified. The instrument has a Likert response scale regarding the frequency with which the individual presents a risk behavior: Never = 1, almost never = 2, sometimes = 3, frequently = 4, and always = 5. Questions were also added about the characteristics of the participants regarding age and gender, as well as background on formal training in road safety and involvement in road accidents as a pedestrian. The reliability of the instrument was measured with Cronbach’s alpha coefficient obtaining a value of .779.
Descriptive statistics and Pearson’s correlation coefficient were used for analysis of the results.
Results
Stage 1
Four hundred twelve observations were obtained, of which 10 were discarded due to incomplete information, leaving a final record of 402 observations. It was found that risk behaviors performed by pedestrians were observable in at least 49% of the sample. The most common risk behaviors were (1) not using bridges and/or pedestrian crossings, (2) crossing the street without precautions, (3) using mobile devices, and (4) not using sidewalks. To a lesser degree, not obeying road signs and crossing avenues between vehicles in motion were identified ().
Table 2. Risk behaviors observed in pedestrians.
Stage 2
The sample consisted of people aged 14 to 60 years old. Adolescents and young adults between 14 and 23 years old represented the highest percentage (56%), whereas participants between 49 and 60 years old represented only 5%. The sample consisted of 728 men (47.3%) and 808 women (52.6%).
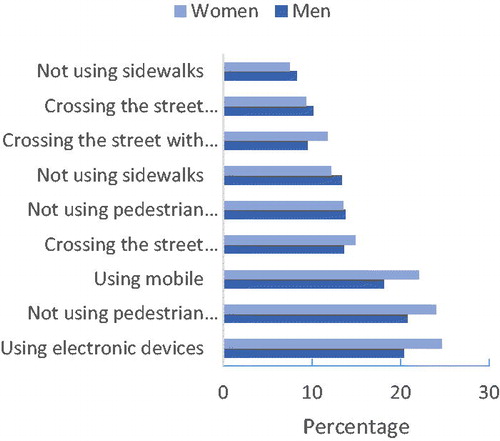
In addition, 71.9% of subjects reported never receiving any training in road safety education. All risk behaviors included in the questionnaire were reported at least occasionally by the respondents. The 3 behaviors that participants performed always or very frequently were (1) using electronic devices (except mobile phones), (2) not using pedestrian crossings, and (3) using a mobile phone (). Two of these risk behaviors can cause distractions, which results in the possibility of a collision with a vehicle (Matsui et al. Citation2013).
Table 3. Pedestrian risk behaviors.
Pearson’s correlation coefficient showed that there is a correlation between age and some risk behaviors, indicating that at a younger age, the use of mobile devices (including cell phones) and other risk behaviors such as crossing streets between moving vehicles or walking in groups on the street is more frequent. At older ages, the most frequent risk behavior is not using pedestrian crossings or bridges ().
Table 4. Correlation between age and risk behavior.
Although there were no significant correlations between gender and risk behaviors (P > .05 in all cases), there were slight variations in the responses between men and women with regard to behaviors performed frequently or always. Although these small differences, ranging from 0.25 to 4.3%, may suggest a greater tendency for women to use electronic and mobile devices when walking and not use pedestrian crossings, no firm conclusion can be drawn because these differences are not statistically significant ().
Figure 1. Comparative graph of risk behaviors by gender, expressed in percentages with respect to each sample.
Furthermore, 285 respondents (18.5%) reported being involved in at least one road accident as a pedestrian in the last 5 years ().
Figure 2. Pedestrian accident characterization.
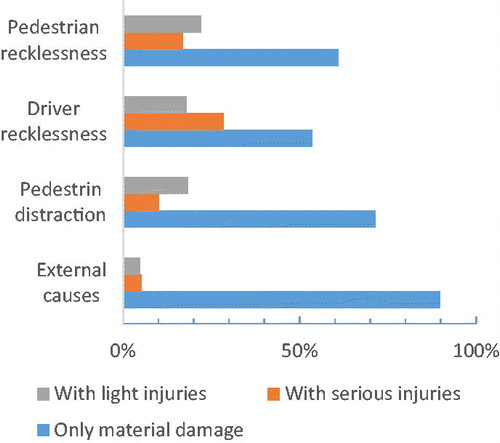
Pedestrian distraction included the use of a mobile device when walking (4% of the 49 cases reported), and risk behaviors included conscious actions or omissions due to an inadequate assessment of road risk. With regard to drivers, it is not possible to determine whether the risk behaviors (mainly speeding and not respecting road signs) were the result of a distraction or a conscious action. However, it has been reported that risky behaviors on the part of vehicle drivers are factors that can result in pedestrian overruns (Jiménez-Mejías et al. Citation2016).
Discussion
Risk behaviors among pedestrians are observable and in many cases pedestrians are aware of them (as reported by 49% of our sample). According to the results of the survey, all of the respondents had some risk behaviors in their role as pedestrians. This coincides with other studies that show that risk behaviors are common among users of public roads (Baptista and Reyes Citation2014; Echeverry et al. Citation2005; Mako and Szakonyi Citation2016).
One fifth of respondents reported that they had been involved in a traffic accident in the last 5 years as a pedestrian. Among these, 21% resulted in pedestrian injuries, 48.3% of which were serious; that is, they required hospitalization. These were due to external causes not related to human factors or unidentified (58.5%) and behavioral factors as a whole (41.4%, 31.5% of which were caused by the pedestrian). Nevertheless, it is important to evoke the multicausality model of losses of Bird and Germain (Citation1990), who are pioneers in the discipline of risk prevention, by establishing 2 important points. First, any loss generated by an accident is a consequence of a combination of causal agents and not a single cause and, second, the act or omission of the human factor is not the root cause, because the origin will always lie in a fault in the system. Therefore, once prevention measures are identified, it is possible to influence risk behaviors.
Novoa et al. (Citation2009) pointed out that there is not enough evidence that actions centered on the human factor results in a decrease in accidents, unlike others focused on the vehicle or infrastructure. It is important to include these actions as part of a comprehensive prevention program in which road safety education and the physical environment must be considered together, and efforts focused on optimum infrastructure also need to consider road safety education.
Although the city of Heroica Matamoros, Tamaulipas, Mexico, can be considered an exemplar of many Latin American cities, in terms of infrastructure, legislation, and road culture, the results cannot be generalized, so a subsequent multicenter study to identify risk behaviors in pedestrians in different contexts is necessary. However, the present study provides a broader view of pedestrian risk behaviors that can lead to road accidents and the importance of a favorable environment in their prevention and reduction.
References
- Alfaro-Basso D. Problemática sanitaria y social de la accidentalidad del transporte Terrestre [Health and social problems of land transport accidents] . Rev Perú Med Exp Salud Pública. 2008;25:133–137.
- Arias W. Una reseña introductoria a la psicología del tránsito [An introductory review to the psychology of transit]. Revista de Psicología. 2011;13:113–119.
- Bambaren C. Características epidemiológicas y económicas de los casos de accidentes de tránsito atendidos en el Hospital Nacional Cayetano Heredia [Epidemiological and economic characteristics of the cases of traffic accidents treated at the Hospital Nacional Cayetano Heredia]. Rev Med Hered. 2004;15:30–36.
- Baptista P, Reyes J. Los jóvenes y la educación para la cultura de la seguridad vial [Young people and education for the road safety culture]. Revista Panamericana de Pedagogía Saberes y Quehaceres del Pedagogo. 2014;21:101–119.
- Bird F, Germain G. Liderazgo Práctico en el Control de Pérdidas [Practical Leadership in the Control of Losses]. Loganville: Det Norske Veritas; 1990.
- Bustos E, Cabrales RG, Cerón M, Naranjo MY. Epidemiología de lesiones no intencionales en niños: revisión de estadísticas internacionales y nacionales [Epidemiology of unintentional injuries in children: review of international and national statistics]. Bol Med Hosp Infan Mex. 2014;71(2):68–75.
- Cabrera G, Velásquez N, Valladares M. Seguridad vial, un desafío de salud pública en la Colombia del siglo XXI [Road safety, a public health challenge in the Colombia of the 21st century]. Rev Fac Nac Salud Publica. 2009;27:218–225.
- Chandran A, Vieira TR, Guo Y, Bishai D, Pechansky F. Road traffic deaths in Brazil: rising trends in pedestrian and motorcycle occupant deaths. Traffic Inj Prev. 2012;13(suppl. 1):11–16.
- Collet C, Guillot A, Petit C. Phoning while driving I: are view of epidemiological, psychological, behavioral and physiological studies. Ergonomics. 2010;53:589–601.
- Echeverry A, Mera JJ, Villota J, Zárate LC. Actitudes y comportamientos de los peatones en los sitios de alta accidentabilidad en Cali [Attitudes and behaviors of pedestrians in high accident sites in Cali]. Colomb Méd. 2005;36(2):79–84.
- International Organization of Traffic Accidentology. Factores de Riesgos en Siniestros Viales [Risk Factors in Road Accidents]. 2015. Available at: http://www.accidentologiavial.net/factores-de-riesgos-en-siniestros-viales/. Accessed June 27, 2018.
- Jiménez-Mejías E, Martínez-Ruiz V, Amezcua-Prieto C, Olmedo-Requena R, Luna-del-Castillo JD, Lardelli-Claret P. Pedestrian- and driver-related factors associated with the risk of causing collisions involving pedestrians in Spain. Accid Anal Prev. 2016;92:211–218.
- Koh PP, Wong YD, Chandrasekar P. Safety evaluation of pedestrian behavior and violations at signalized pedestrian crossings. Saf Sci. 2014;70:143–152.
- Mako E, Szakonyi P. Evaluation of human behavior at pedestrian crossings. Transportation Research Procedia. 2016;14:2121–2128.
- Matsui Y, Hitosugi M, Doi T, Oikawa S, Takahashi K, Ando K. Features of pedestrian behavior in car-to-pedestrian contact situations in near-miss incidents in Japan. Traffic Inj Prev. 2013;14:S58–S63.
- National Institute of Statistics and Geography. México en Cifras [Mexico in figures]. Ciudad de México, Mexico: INEGI (Autonomous institute); 2015. Available at: http://www.beta.inegi.org.mx/app/areasgeograficas/?ag=28#. Accessed June 27, 2018.
- National Institute of Statistics and Geography. Accidentes de Tránsito Terrestre en Zonas Urbanas y Suburbanas [Road Traffic Accidents in Urban and Suburban Areas]. Ciudad de México, Mexico: INEGI (Autonomous institute); 2018. Available at: http://www.inegi.org.mx/sistemas/olap/proyectos/bd/continuas/transporte/accidentes.asp. Accessed June 27, 2018.
- Novoa A, Pérez K, Borrell C. Efectividad de las intervenciones de seguridad vial basadas en la evidencia: una revisión de la literatura [Effectiveness of evidence-based road safety interventions: a review of the literature]. Gac Sanit. 2009;23:553–553.
- Olszewski P, Szagała P, Wolan˙ski M, Zielin˙ska A. Pedestrian fatality risk in accidents at unsignalized zebra crosswalks in Poland. Accid Anal Prev. 2015;84:83–91.
- Pan American Health Organization/World Health Organization. Más de 23.500 Peatones Mueren Anualmente en América Latina y el Caribe [More than 23,500 Pedestrians Die Annually in Latin America and the Caribbean]. Washington, DC: WHO (World Health Organization); 2013.
- Secretaría de Salud [Secretariat of Health]. Boletín de Información Estadística 2014–2015 [Statistical information bulletin 2014–2015]. Ciudad de México, Mexico: Government of Mexico; 2015.
- Uttley J, Fotios S. The effect of ambient light condition on road traffic collisions involving pedestrians on pedestrian crossings. Accid Anal Prev. 2017;108:189–200.
- Velázquez Y, Zamorano B, Ruíz L. Siniestralidad vial en la frontera norte de Tamaulipas. Enfoque en los procesos administrativos de control [Road Accident Rate in the Northern Border of Tamaulipas. Focus on Administrative Control Processes]. Estudios Fronterizos. 2017;18(36):1–24.
- World Health Organization. Lesiones Causadas por el Tránsito [Injuries Caused by Traffic]. 2015. Available at: http://www.who.int/mediacentre/factsheets/fs358/es/. Accessed June 28, 2018.
- World Health Organization. Las 10 Principales Causas de Defunción. 2018 [The 10 leading causes of death]. Available at: http://www.who.int/es/news-room/fact-sheets/detail/the-top-10-causes-of-death. Accessed June 28, 2018.
- Zegeer Ch, Bushell M. Pedestrian crash trends and potential countermeasures from around the world. Accid Anal Prev. 2012;44:3–11.