
Abstract
Objective: Analyses of crash data have shown that older, obese, and/or female occupants have a higher risk of injury in frontal crashes compared to the rest of the population. The objective of this study was to use parametric finite element (FE) human models to assess the increased injury risks and identify safety concerns for these vulnerable populations.
Methods: We sampled 100 occupants based on age, sex, stature, and body mass index (BMI) to span a wide range of the U.S. adult population. The target anatomical geometry for each of the 100 models was predicted by the statistical geometry models for the rib cage, pelvis, femur, tibia, and external body surface developed previously. A regional landmark-based mesh morphing method was used to morph the Global Human Body Models Consortium (GHBMC) M50-OS model into the target geometries. The morphed human models were then positioned in a validated generic vehicle driver compartment model using a statistical driving posture model. Frontal crash simulations based on U.S. New Car Assessment Program (U.S. NCAP) were conducted. Body region injury risks were calculated based on the risk curves used in the US NCAP, except that scaling was used for the neck, chest, and knee–thigh–hip injury risk curves based on the sizes of the bony structures in the corresponding body regions. Age effects were also considered for predicting chest injury risk.
Results: The simulations demonstrated that driver stature and body shape affect occupant interactions with the restraints and consequently affect occupant kinematics and injury risks in severe frontal crashes. U-shaped relations between occupant stature/weight and head injury risk were observed. Chest injury risk was strongly affected by age and sex, with older female occupants having the highest risk. A strong correlation was also observed between BMI and knee–thigh–hip injury risk, whereas none of the occupant parameters meaningfully affected neck injury risks.
Conclusions: This study is the first to use a large set of diverse FE human models to investigate the combined effects of age, sex, stature, and BMI on injury risks in frontal crashes. The study demonstrated that parametric human models can effectively predict the injury trends for the population and may now be used to optimize restraint systems for people who are not similar in size and shape to the available anthropomorphic test devices (ATDs). New restraints that adapt to occupant age, sex, stature, and body shape may improve crash safety for all occupants.
Introduction
The current design process for vehicle restraint systems relies extensively on crash tests with a few anthropomorphic test devices (ATDs). For example, the midsize male and small female ATDs are the only adult ATDs used in FMVSS and New Car Assessment Programs (NCAP) in the United States, Europe, China, and many other countries. However, obese, older, and female occupants are at increased risk of death and serious injury compared to midsize, young, and male occupants (Bose et al. Citation2011; Boulanger et al. Citation1992; Kent, Henary, and Matsuoka Citation2005; Morris et al. Citation2002, Citation2003; Rupp et al. Citation2013; Zhu et al. Citation2010). These vulnerable populations may not be sufficiently represented by the two widely used ATD sizes. From an injury biomechanics point of view, these higher injury risks are due in part to differences in geometric, compositional, and material characteristics of bones and soft tissues in the human body (Hu et al. Citation2012; Kent, Lee, et al. Citation2005). Therefore, injury assessment tools, such as computational human models, used for optimizing vehicle safety designs for those vulnerable populations should incorporate these characteristic differences. Current finite element (FE) human models for adults, such as models from the Global Human Body Models Consortium (GHBMC) and the Total Human Model for Safety (THUMS) from Toyota, have approximately the same adult body sizes (large male, midsize male, and small female) as current physical ATDs and do not consider variations in skeleton geometry and external body shape outside of those anthropometric categories. As a result, they cannot be used to evaluate the injury risks for elderly and obese occupants or others who differ markedly in size and shape from the ATDs.
Over the past few years, mesh morphing methods have been applied to morph midsize male human models into other body sizes or ages (Jolivet et al. Citation2015; Schoell et al. Citation2015; Vavalle et al. Citation2014). Our research group has developed a parametric human FE modeling approach that allows the size and shape of an FE human model to be rapidly varied based on age, sex, stature, and body mass index (BMI; Hwang et al. Citation2016a; Zhang et al. Citation2017a). The parametric approach eliminates the time-consuming process of building entirely new human models for each desired occupant size and shape and enables population-based simulations with a large set of human models representing a diverse population. This approach has been applied to morph the THUMS v4 midsize male model into occupants with a wide range of stature and BMI (Hwang, Hallman, et al. Citation2016; Shi et al. Citation2015). The impact responses of those models were compared to cadaver tests through subject-specific validations (Hwang, Hu, et al. Citation2016; Zhang, Cao, Wang, et al. Citation2017). The same approach has also been applied to morph the GHBMC midsize male model into 100 human models with a wide range of age, stature, and BMI for both men and women (Zhang, Ca, Fanta, et al. Citation2017). A small set of these morphed models (n = 6) was used in U.S. NCAP frontal crash simulations to investigate the human size and shape effects on occupant impact responses (Hu, Zhang, Fanta, et al. Citation2017). However, due to the small sample size, quantitative relationships between occupant characteristics and injury risks could not be analyzed.
The objective of the current study was to use a large set of FE human models representing a diverse population to examine the increased injury risks for older, obese, and/or female occupants in frontal crashes and to identify safety concerns associated with these vulnerable populations.
Methods
Baseline FE human model
In this study, the midsize male simplified occupant model from the GHBMC (M50-OS V1.8.4) was used as the baseline model to be morphed into a large set of diverse human models. The GHBMC M50-OS model has been validated extensively against cadaver tests that are relevant to frontal crashes, including a 23-kg hub impact to the thorax with an initial velocity of 6.7 m/s, a 48-kg bar impact to the abdomen with an initial velocity of 6 m/s, and a frontal sled test condition with an 11.1-m/s crash pulse. In the frontal sled condition similar to the simulation condition in the current study, the correlation and analysis ratings for the body excursions as well as reaction forces on the knee and seat ranged from 0.55 to 0.83. More details of the model validation can be found in Schwartz et al. (Citation2015) and the GHBMC (Citation2016).
Diverse FE human models through mesh morphing
Anthropometric targets were generated for a total of 103 human models, including 3 models corresponding to the 3 sizes of adult ATDs (small female, midsize male, and large male) and 50 men and 50 women selected by uniform Latin hypercube sampling (ULHS) with the age (20 to 80 years old), stature (5th to 95th percentile), and BMI (5th to 95th percentile) distributions based on National Health and Nutrition Examination Survey data for the years 2011–2014 for the U.S. population (Fryar et al. Citation2016). A weighting factor for each ULHS-sampled occupant was calculated based on the distribution of age, stature, and BMI in men and women of the U.S. adult population. The weighting factor indicates the percentage of the U.S. population represented by each model. For each model, this means the percentage of the population who are closer to the model in scaled size and age than to any other model of the same sex. Weighting factors ranged from 0.2 to 2.4% for the 100 models through ULHS.
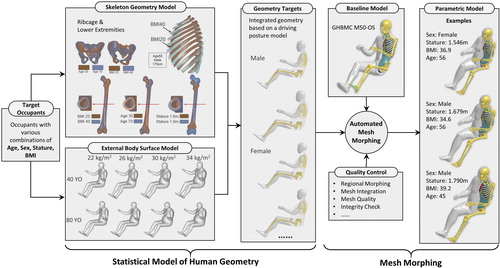
A detailed method for morphing the GHBMC model into any given age, sex, stature, and BMI has been presented by Zhang, Cao, Fanta, et al. (Citation2017) and Hu, Zhang, Fanta, Hwang, and Reed (Citation2017). For the sake of completeness, the whole-body mesh morphing method is briefly presented here. As shown in , the process begins with statistical models of skeletal components, including rib cage, pelvis, femur, and tibia, along with external body shape models of human geometry that describe morphological variations within the population as functions of age, sex, stature, and BMI. Mesh morphing methods were then used to morph a baseline human model into target geometries while maintaining high geometric accuracy and good mesh quality. Given a target sex, age, stature, and BMI, the statistical human geometry models developed previously predict thousands of points that define the body posture (Park et al. Citation2016; Reed et al. Citation2000, Citation2002), the size and shape of the external body surface (Reed and Parkinson Citation2008), and rib cage (Shi et al. Citation2014; Wang et al. Citation2016) and lower extremity (Klein Citation2015; Klein et al. Citation2015) bone geometries. The skeleton and external body shape geometries were integrated based on the landmarks and joint locations shared in both skeleton and external body shape models. Once the target geometries were developed, the baseline model was morphed to match the target geometries using a landmark-based 3D nonlinear interpolation technique based on radial basis functions. The entire morphing process is automated and requires less than 10 min per model using a typical desktop computer. Because the target geometry was based on the statistical human geometry models developed independent of the GHBMC models, the geometries of the morphed small female, midsize male, and large male models are slightly different from the corresponding GHBMC models.
Figure 1. Rapid development of human FE models for a diverse population by mesh morphing.
Vehicle model for crash simulations
In this study, an FE model of a midsize sedan was used for all crash simulations. This vehicle was equipped with a driver airbag, a crushable steering column (3 kN), a constant load limiter (2.85 kN), a retractor pretensioner (2 kN), and an anchor pretensioner (2 kN) but no knee airbag. This model has undergone extensive validation against vehicle crash test data, including both midsize male and small female Hybrid III ATDs in both driver and front seat passenger locations under U.S. NCAP frontal crash (35 mph) and FMVSS 208 unbelted crash (25 mph) conditions. The average difference in joint injury probability (using absolute values) is 3.2% for belted ATDs in the U.S. NCAP frontal crash condition and 2.3% for unbelted ATDs in FMVSS 208 conditions. Validation results can be found in Hu, Klinich, et al. (Citation2017). All of the main injury measures predicted by the ATD model were highly correlated with the test data.
Occupant positioning procedure
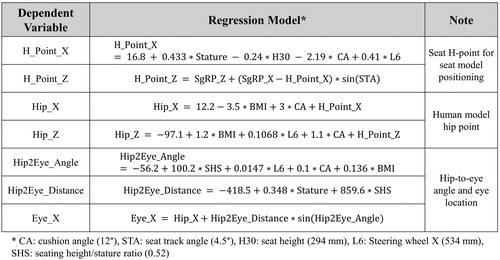
For each crash simulation, the morphed human model was positioned as a driver according to a driving posture model developed based on measurements from 68 volunteers (Reed et al. Citation2002). The driving posture model predicts occupant posture and position variables as a function of occupant body dimensions and vehicle package factors, as shown in . In this study, a constant ratio of sitting height to stature (= 0.52) was assumed for all 103 morphed models; thus, only stature and BMI were used as the input parameters to define the driver dimensions. Note that the 5th and 95th percentile sitting height–to-stature values are 0.50 to 0.54 for the U.S. population. The vehicle package factors, including seat height (H30 = 294 mm), steering wheel X (distance from the center of steering wheel to the ball of foot reference point) (L6 = 534 mm), and seat track angle (A27 = 4.5°), were all set as constant for predicting the driving postures. Based on the regression model shown in , the model-predicted driver hip and eye locations (only in the X direction) were used to position the morphed human models, and the predicted driver-selected seat H-point location was used to position the seat before each simulation. For each simulation, the driver’s hands were positioned on the steering wheel by adjusting the shoulder and elbow angles, and the right and left feet/shoes were positioned onto the gas pedal and the floor, respectively, by adjusting the hip, knee, and ankle angles. After the morphed human models and the vehicle seat were repositioned, the seat belt was fitted onto the occupant with mid-sternum point (shoulder belt) and mid-abdomen point (lap belt) as the guiding points. In this study, the occupant positioning and seat belt fitting were conducted in a semi-automatic manner using Matlab and Ls-PrePost.
Figure 2. Driving posture model used in this study (Reed et al., Citation2002).
For small and obese female models, the driver positioning procedure occasionally resulted in initial penetration between the steering wheel and the abdomen of the occupant. In these cases, the occupant model and seat model were moved rearward along the seat track to keep a minimum 10-mm gap between the occupant abdomen and the steering wheel.
Injury measures and injury risk curve scaling
For each simulation, injury measures for the head (head injury criterion [HIC] and brain injury criterion [BrIC]), neck (force and Nij), chest (deflection), and knee–thigh–hip (femur force) were output. The injury risks were calculated based on the injury risk curves provided by the U.S. NCAP. However scaling was used for the neck, chest, and knee–thigh–hip (KTH) injury risk curves based on the sizes of the bony structures in the corresponding body regions. Age effects were also considered for predicting the chest injury risk.
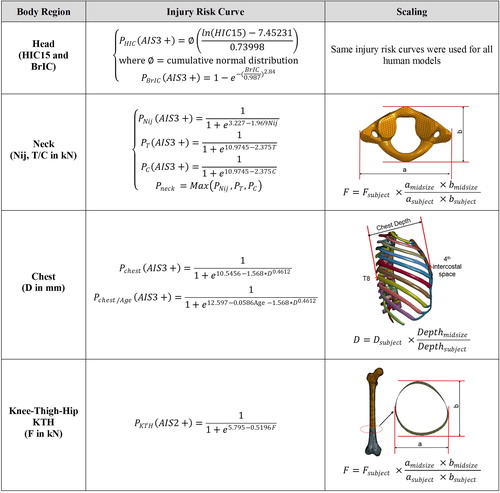
All injury risk curves and scaling methods used in this study are shown in . The neck forces (tension/compression) and the intercepts for calculating the Nij were normalized based on the size of the C1 vertebra. The chest deflection was normalized by chest depth, which is measured between the spinal process of T8 vertebra to the mid-sternum at the fourth intercostal space. The femur force was normalized based on the cross-sectional area of the femur where a load cell was defined for measuring femur force.
Figure 3. Injury risk curves and scaling method.
Results
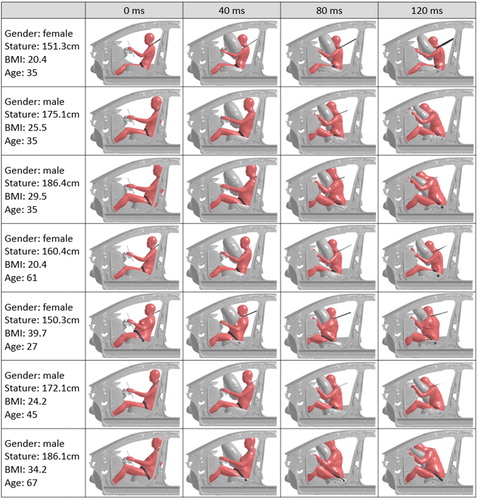
A total of 103 U.S. NCAP frontal crash simulations with the morphed human models were conducted. Seven examples of simulated driver kinematics are shown in . Both stature and body shape exhibited significant effects on occupant kinematics. In particular, taller occupants tended to pitch forward more than shorter occupants, and their heads and necks tended to wrap around the top of the airbag. The torsos of obese occupants pushed the airbag upward during and subsequent to deployment. This pattern is most evident for small female models because the abdomen was close to the airbag before the event.
Figure 4. Examples of occupant kinematics in US-NCAP frontal crashes.
Some interesting trends in the injury risk distributions with respect to the occupant weight, stature, BMI, and/or age are shown in . The results for the 50 female models are represented by hollow red circles, the 50 male models are represented by shaded blue circles, and 3 human models corresponding to the ATD sizes are represented with triangles. The area of each circle indicates the magnitude of the weighting for each occupant.
Figure 5. Injury risk distributions with respect to occupant characteristics. Note: The 5th and 50th and 95th are corresponding to the sizes of three adult ATDs, namely small female, midsize male, and large male.
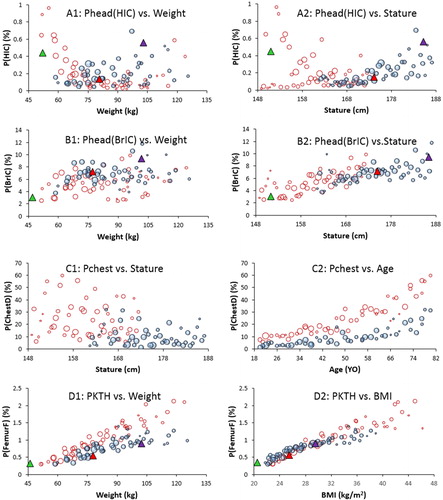
As shown in , using HIC as the head injury predictor there is a U-shaped relation between body weight and head injury risk, indicating that both lighter and heavier occupants experienced higher head injury risks than midsize occupants. Interestingly, the stature effects on head injury risk showed a significant difference between HIC and BrIC. In particular, shorter and taller occupants generated higher HIC values than midsize occupants, except for short obese female occupants, whose HIC values were typically low (). A positive correlation was observed between stature and BrIC (), suggesting that taller occupants tend to have higher BrIC. No strong BMI or age effects on head injury risks were observed, although BrIC predicted much higher head injury risks than HIC in all simulations.
The effects of occupant body weight, stature, BMI, and age on neck injury risks are not strong based on either neck force or Nij, although Nij predicted much higher neck injury risks than neck force. It should be noted that the injury risk is not zero at zero Nij and Nij tends to overestimate the neck/cervical spine injury risks based on field data analysis (Digges et al. Citation2013).
As shown in and 5-C2, a strong sex effect on chest injury risks is observed regardless of whether the age effect is considered in the injury risk curve. The simulations predicted that female occupants had higher chest injury risks than male occupants, although such effects may be partially due to the average body size difference between women and men. In addition, when the age effect was considered in the injury risk curve, the simulation results showed a strong age effect on chest injury risks. The age effect for female models was larger than that for male models, and the variation in chest injury risks was substantially greater among older occupants than among younger occupants.
As shown in and 5-D2, a very strong correlation was observed between BMI and KTH injury risk. A similar correlation was also observed between body weight and the KTH injury risk. The stature and age effects were not strong for KTH injury risk.
Discussion
This study is the first to use a large set of human body models to investigate the combined effects of age, sex, stature, and BMI on injury risks in frontal crashes and is the first to use a validated driving posture model to rigorously position a large set of morphed human models into a driving compartment.
Generally speaking, the simulations suggested that age, sex, stature, and BMI all significantly affect the occupant injury risks in U.S. NCAP frontal crash condition. In particular, age has a dominant effect on occupant chest injury risk, because being older will significantly increase the mean and variation in the chest injury risks among the population. This larger variation in older occupants may be partially due to the fact that older occupants tend to have chest injury risks closer to 50% in the simulated conditions. The simulation results also suggested that female occupants would have higher chest injury risks than male occupants, but this effect may be partially due to their relatively small body size. In this study, a constant shoulder belt load limiter was used for all simulations. Consequently, similar forces were transferred through the seat belt to the chest of all occupants. Regardless of the occupant interaction with the airbag, this constant seat belt force alone may help to explain why short female drivers showed higher chest injury risks due to chest deflection than taller male drivers. Interestingly, the simulations showed different stature effects on head injury risks based on HIC and BrIC. Based on HIC, shorter and taller occupants would have higher head injury risks than mid-stature occupants, except for short obese females, whose head injury risks were generally low. However, based on BrIC, being taller would increase the head injury risk, because the head would rotate more forward for taller occupants than for shorter occupants. The BMI effect is highly significant for KTH injury risks, because being more obese will increase mass-induced body excursions and produce poor lap belt fit due to a large abdomen. All of these trends in injury risks are broadly consistent with previous analyses of field crash data (Bose et al. Citation2011; Boulanger et al. Citation1992; Kent, Henary, and Matsuoka Citation2005; Morris et al. Citation2002, Citation2003; Rupp et al. Citation2013; Zhu et al. Citation2010). These results indicate that restraint system designs that can adapt to occupant age, sex, stature, and body shape have a great potential to improve occupant protection for individuals with body sizes and shapes different from those of available ATDs.
This study had several limitations. The statistical geometric models only include the rib cage, pelvis, femur, tibia, and external body shape; therefore, bones in other body regions, such as the skull, cervical spine, and feet, were morphed by the external body surface without accurate bone geometry prediction. Furthermore, the characteristics of the joints in the hip, knee, and cervical spine were not changed among the morphed models. None of the morphed human models was validated against any cadaver tests, and the material properties were held constant with age, sex, stature, and body shape. The methods used in the past for human model validation are in need of improvement, because the results of parametric human model simulations demonstrate that the scaling methods based on body size and weight that have been used for corridor generation are not valid. Specifically, the parametric human modeling results show that body mass scaling does not appropriately account for variations in response due to body shape. To replace these outdated methods, we have presented preliminary results of subject-specific model validation, in which the human model was morphed into the geometry of specific cadavers (Hwang, Hu, et al. Citation2016; Zhang, Cao, Wang, et al. Citation2017). The morphed human models generally produce results with accuracy similar to that of the baseline model, but the biofidelity of the morphed human models certainly requires further investigation.
This study only used one vehicle model and crash condition; therefore, the findings only represent that particular vehicle and may not be generalized in the whole vehicle fleet and the range of crash conditions. However, the injury trends suggested by this study are generally consistent with other studies based on field crash data.
The injury measures used in this study are global measures (e.g., HIC, BrIC, Nij, chest deflection, and femur force) typically used for ATDs. Whether these injury measures are suitable for the GHBMC model for predicting injury risks needs further evaluation. Other injury measures, such as multipoint thoracic injury criterion, spine load, and tibia load, can be considered in evaluating injury risks in the future. Tissue-level strain and stress may also be considered, which might be more accurate in predicting human injury risks than global measures. However, tissue-level injury criteria and the associated injury risk curves are not currently available and will likely require significant effort to develop.
The injury risk curves used in this study were based on simple scaling methods using the bone dimensions, and age effects were not considered in predicting injuries to the head, neck, and lower extremities. This approach has 2 major weaknesses. First, the published injury risk curves result from various scaling and processing methods applied to cadaver data that our modeling results suggest may not be valid (for example, mass scaling). Second, our efforts to adjust these functions originally developed for midsize male ATDs for use with other body sizes were based on simple linear functions of geometry that are almost certainly inadequate to capture the true variation in tolerance with body size. For example, we assume a constant linear relationship between femur strength and cross-sectional area, but the true relationship is almost certainly more complex and may interact with sex, age, and other variables. Further investigations will be needed to define more suitable injury risk curves for diverse populations. Nevertheless, our further analysis showed that even if scaling was not considered in the injury risk curves, the general trends in the injury risks are still consistent to those with scaling. It indicated that morphing-produced occupant size, shape, and seating posture dominated the trends in injury risks.
Finally, driving posture and belt position vary widely even among individuals with the same overall stature and body weight, though the current driving posture model only estimates the average among them and the belt fit procedure can be improved in the future. Furthermore, the driving posture model was developed based on volunteers with BMIs between 16.9 and 33.5 kg/m2, but the models were extrapolated to provide predictions for BMI over 40 kg/m2. The nonlinear differences in restraint system interaction observed in the current study suggest that a particular difference in torso recline, fore–aft seat position, or belt placement may have little consequence for some occupants but large effects for others. Further research is needed to differentiate among the effects of body size, body shape, posture, and position.
In summary, this study used a large set of FE human models (n = 103) with a wide range of age, stature, and body shape for men and women for U.S. NCAP frontal crash simulations considering driving posture variations due to occupant attributes. The simulations suggested that driver stature and body shape affect occupant interactions with the restraints, occupant kinematics, and injury risks in severe frontal crashes, whereas driver age affects the human tolerance and in turn affects driver injury risks. In particular, U-shaped relations between occupant stature/weight and head injury risk were observed. Chest injury risk was strongly affected by age and sex, with older female occupants having the highest risk. A strong correlation was also observed between BMI and KTH injury risk, though none of the occupant parameters meaningfully affected neck injury risks. The morphed human models and the crash simulations demonstrated the feasibility of using a mesh morphing method to generate a large set of human models to represent a diverse population for evaluation of occupant injury risks. The simulation results suggest that restraint optimization should include additional consideration of occupants who differ substantially in size and shape from the ATDs commonly used for vehicle safety assessment. New restraints that adapt to occupant age, sex, stature, and body shape may improve crash safety for all occupants.
Additional information
Funding
References
- Bose D, Segui-Gomez M, Crandall JR. Vulnerability of female drivers involved in motor vehicle crashes: an analysis of U.S. population at risk. Am J Public Health. 2011;101:2368–2373.
- Boulanger BR, Milzman D, Mitchell K, Rodriguez A. Body habitus as a predictor of injury pattern after blunt trauma. J Trauma. 1992;33:228–232.
- Digges K, Dalmotas D, Prasad P. An NCAP star rating system for older occupants. Paper presented at: 23rd International Technical Conference on the Enhanced Safety of Vehicles (ESV); 2013; Seoul, Republic of Korea.
- Fryar C, Gu Q, Ogden C, Flegal K. Anthropometric reference data for children and adults: United States, 2011–2014. Vital Health Stat. 2016;3(39):1–46.
- GHBMC. User Manual: M50 Occupant Simplified Version 1.8.4 for LS-DYNA. Global Human Body Models Consortium, LLC. 2016.
- Hu J, Klinich KD, Manary MA, et al. Does unbelted safety requirement affect protection for belted occupants? Traffic Inj Prev. 2017;18(S1):S85–S95.
- Hu J, Rupp J, Reed M. Focusing on vulnerable populations in crashes: recent advances in finite element human models for injury biomechanics research. Journal of Automotive Safety and Energy. 2012;3:295–307.
- Hu J, Zhang K, Fanta A, Hwang E, Reed M. Effects of male stature and body shape on thoracic impact response using parametric finite element human modeling. Paper presented at: 25th International Technical Conference on the Enhanced Safety of Vehicles (ESV); 2017; Detroit, MI.
- Hu J, Zhang K, Fanta A, et al. Stature and body shape effects on driver injury risks in frontal crashes: a parametric human modelling study. Paper presented at: IRCOBI Conference; 2017; Antwerp, Belgium.
- Hwang E, Hallman J, Klein K, Rupp J, Reed M, Hu J. Rapid Development of Diverse Human Body Models for Crash Simulations Through Mesh Morphing. 2016. SAE Technical Paper 2016-01-1491.
- Hwang E, Hu J, Chen C, et al. Development, evaluation, and sensitivity analysis of parametric finite element whole-body human models in side impacts. Stapp Car Crash J. 2016;60:473–508.
- Jolivet E, Lafon Y, Petit P, Beillas P. Comparison of kriging and moving least square methods to change the geometry of human body models. Stapp Car Crash J. 2015;59:337–357.
- Kent R, Henary B, Matsuoka F. On the fatal crash experience of older drivers. Annu Proc Assoc Adv Automot Med. 2005;49:371–391.
- Kent R, Lee SH, Darvish K, et al. Structural and material changes in the aging thorax and their role in crash protection for older occupants. Stapp Car Crash J. 2005;49:231–249.
- Klein KF. Use of Parametric Finite Element Models to Investigate Effects of Occupant Characteristics on Lower-Extremity Injuries in Frontal Crashes [PhD dissertation], Ann Arbor, MI: University of Michigan; 2015.
- Klein KF, Hu J, Reed MP, Hoff CN, Rupp JD. Development and validation of statistical models of femur geometry for use with parametric finite element models. Ann Biomed Eng. 2015;43:2503–2514.
- Morris A, Welsh R, Frampton R, Charlton J, Fildes B. An overview of requirements for the crash protection of older drivers. Annu Proc Assoc Adv Automot Med. 2002;46:141–156.
- Morris A, Welsh R, Hassan A. Requirements for the crash protection of older vehicle passengers. Annu Proc Assoc Adv Automot Med. 2003;47:165–180.
- Park J, Reed MP, Hallman JJ. Statistical models for predicting automobile driving postures for men and women including effects of age. Hum Factors. 2016;58:261–278.
- Reed MP, Manary MA, Flannagan CA, Schneider LW. Effects of vehicle interior geometry and anthropometric variables on automobile driving posture. Hum Factors. 2000;42:541–552.
- Reed MP, Manary MA, Flannagan CA, Schneider LW. A statistical method for predicting automobile driving posture. Hum Factors. 2002;44:557–568.
- Reed MP, Parkinson MB. Modeling variability in torso shape for chair and seat design. Paper presented at: ASME International Design Engineering Technical Conferences; 2008; New York, NY.
- Rupp JD, Flannagan CAC, Leslie AJ, Hoff CN, Reed MP, Cunningham RM. Effects of BMI on the risk and frequency of AIS 3+ injuries in motor-vehicle crashes. Obesity. 2013;21(1):E88–97.
- Schoell SL, Weaver AA, Urban JE, et al. Development and validation of an older occupant finite element model of a mid-sized male for investigation of age-related injury risk. Stapp Car Crash J. 2015;59:359–383.
- Schwartz D, Guleyupoglu B, Koya B, Stitzel JD, Gayzik FS. Development of a computationally efficient full human body finite element model. Traffic Inj Prev. 2015;16(Suppl. 1):S49–S56.
- Shi X, Cao L, Reed MP, Rupp JD, Hoff CN, Hu J. A statistical human rib cage geometry model accounting for variations by age, sex, stature and body mass index. J Biomech. 2014;47:2277–2785.
- Shi X, Cao L, Reed MP, Rupp JD, Hu J. Effects of obesity on occupant responses in frontal crashes: a simulation analysis using human body models. Comput Methods Biomech Biomed Eng. 2015;18:1280–1292.
- Vavalle NA, Schoell SL, Weaver AA, Stitzel JD, Gayzik FS. Application of radial basis function methods in the development of a 95th percentile male seated FEA model. Stapp Car Crash J. 2014;58:361–384.
- Wang Y, Cao L, Bai Z, et al. A parametric ribcage geometry model accounting for variations among the adult population. J Biomech. 2016;49(13):2791–2798.
- Zhang K, Cao L, Fanta A, et al. An automated method to morph finite element whole-body human models with a wide range of stature and body shape for both men and women. J Biomech. 2017;60:253–260.
- Zhang K, Cao L, Wang Y, et al. Impact response comparison between parametric human models and postmortem human subjects with a wide range of obesity levels. Obesity. 2017;25:1786–1794.
- Zhu S, Kim JE, Ma X, et al. BMI and risk of serious upper body injury following motor vehicle crashes: concordance of real-world and computer-simulated observations. PLoS Med. 2010;7:e1000250.