
Abstract
Objectives: Earlier research has shown that the rear row is safer for occupants in crashes than the front row, but there is evidence that improvements in front seat occupant protection in more recent vehicle model years have reduced the safety advantage of the rear seat versus the front seat. The study objective was to identify factors that contribute to serious and fatal injuries in belted rear seat occupants in frontal crashes in newer model year vehicles.
Methods: A case series review of belted rear seat occupants who were seriously injured or killed in frontal crashes was conducted. Occupants in frontal crashes were eligible for inclusion if they were 6 years old or older and belted in the rear of a 2000 or newer model year passenger vehicle within 10 model years of the crash year. Crashes were identified using the 2004–2015 National Automotive Sampling System Crashworthiness Data System (NASS-CDS) and included all eligible occupants with at least one Abbreviated Injury Scale (AIS) 3 or greater injury. Using these same inclusion criteria but split into younger (6 to 12 years) and older (55+ years) cohorts, fatal crashes were identified in the 2014–2015 Fatality Analysis Reporting System (FARS) and then local police jurisdictions were contacted for complete crash records.
Results: Detailed case series review was completed for 117 rear seat occupants: 36 with Maximum Abbreviated Injury Scale (MAIS) 3+ injuries in NASS-CDS and 81 fatalities identified in FARS. More than half of the injured and killed rear occupants were more severely injured than front seat occupants in the same crash. Serious chest injury, primarily caused by seat belt loading, was present in 22 of the injured occupants and 17 of the 37 fatalities with documented injuries. Nine injured occupants and 18 fatalities sustained serious head injury, primarily from contact with the vehicle interior or severe intrusion. For fatal cases, 12 crashes were considered unsurvivable due to a complete loss of occupant space. For cases considered survivable, intrusion was not a large contributor to fatality.
Discussion: Rear seat occupants sustained serious and fatal injuries due to belt loading in crashes in which front seat occupants survived, suggesting a discrepancy in restraint performance between the front and rear rows. Restraint strategies that reduce loading to the chest should be considered, but there may be potential tradeoffs with increased head excursion, particularly in the absence of rear seat airbags. Any new restraint designs should consider the unique needs of the rear seat environment.
Introduction
Passenger vehicle deaths in the United States have declined dramatically over the last few decades (Insurance Institute for Highway Safety [IIHS] Citation2016) and much of the recent improvements can be attributed to vehicle design changes primarily driven by regulatory and consumer information test programs (Farmer and Lund Citation2015). Despite vehicle design improvements, more than 23,000 passenger vehicle occupants died in 2016 in the United States, 54% of which were due to frontal impacts (IIHS 2016), suggesting that there is still an opportunity for improved protection in this crash mode. IIHS and the National Highway Traffic Safety Administration (NHTSA) evaluate vehicles in an array of frontal crash configurations including full-width, moderate, and small overlap. Each of these tests evaluates protection afforded to front seat occupants without consideration for the injury assessment of rear seat occupants.
In the United States in 2016, nearly 2,000 occupants were killed in the rear seat of passenger vehicles, accounting for 8% of all passenger vehicle occupant deaths that year (IIHS 2016). Earlier research has shown that the rear row is safer for occupants than the front row (Braver et al. Citation1998; Durbin et al. Citation2005), but there is evidence that improvements in front seat occupant protection in more recent vehicles have reduced the safety advantage of the rear seat versus the front seat (Bilston et al. Citation2010; Durbin et al. Citation2015; Kuppa et al. Citation2005; Sahraei et al. Citation2010; Winston et al. Citation2007). In a recent study that compared the risk of death in the rear seat with passengers in the front seat, restrained rear seat occupants were at a 46% higher risk of death compared with front-row passengers in model year 2007 and newer vehicles (Durbin et al. Citation2015). In the same study, children ages 9 to 12 years had an elevated risk of death in the rear compared with the front (risk ratio [RR] = 1.83; 95% confidence interval [CI], 1.18–2.84) and there was some evidence that adults ages 55 years and older may be at elevated risk, but the authors could not exclude the possibility of no difference (RR = 1.41; 95% CI, 0.94–2.13). In frontal crashes, after adjusting for occupant age, impact direction, and other factors, there was no elevated risk of death for rear- vs. front-row occupants (RR = 0.96; 95% CI, 0.75–1.23), but frontal impacts accounted for the largest proportion (34%) of fatalities in restrained rear seat occupants.
Several studies have looked at injury patterns for child and adult rear seat occupants in frontal crashes. In studies of frontal tow-away crashes that occurred between 1991 and 2003, the chest was the most frequently Abbreviated Injury Scale (AIS) 3+ injured body region for restrained adults (Kuppa et al. Citation2005; Parenteau and Viano Citation2003), whereas the most common AIS 3+ injuries for restrained children were to the upper extremity followed by the head for children ages 6 to 8 years and the chest followed by the head for children ages 9 to 15 years (Kuppa et al. Citation2005). A trauma center–based study of 29 restrained rear seat occupants ages 9 years and older found that the chest followed by the abdomen were the most commonly injured body regions and were generally attributed to interaction with the vehicle belt (Beck et al. Citation2016). The vehicle model year in the study ranged from 1989 to 2010 with an average model year of 1998.
The current study sought to identify factors that contribute to serious and fatal injuries in restrained rear seat occupants in frontal crashes in newer model year vehicles. Review of seriously injured occupants focused on occupants ages 6 years or older who were restrained using the vehicle seat belts, with or without a booster seat. Review of fatally injured occupants focused on 2 vulnerable populations: children ages 6 to 12 years and adults ages 55 or older.
Methods
A case series review of belted rear seat occupants who were seriously injured or killed in frontal crashes was conducted. Occupants were eligible for inclusion if they were ages 6 years or older using the vehicle seat belt with or without a booster seat in the second or third row of a passenger vehicle and involved in a frontal crash. Passenger vehicles were included if they were model year 2000 or newer and no older than 10 years at the time of the crash. For this study, a crash is defined as an impact between the occupant’s vehicle and a crash partner, and a case represents a single occupant of interest.
Crashes were identified using 2 data sources: the 2004–2015 National Automotive Sampling System Crashworthiness Data System (NASS-CDS) and Fatality Analysis Reporting System (FARS). For cases identified in FARS, local police jurisdictions were contacted for complete crash records. Due to this resource-intensive process, FARS cases focused on 2 vulnerable populations identified in Durbin et al. (Citation2015): Belt-restrained children and older occupants. Cases from NASS-CDS included all belted occupants ages 6 years and older to provide additional insight into serious injuries in occupants ages 13 to 54 years.
Injury and fatal crash identification in the NASS-CDS
Injury and fatal crashes were identified using the 2005–2015 NASS-CDS and included all eligible occupants with AIS 3 or greater injuries. At the time of the study, 2015 NASS-CDS data were the most recent complete year of data available due to NHTSA’s transition to a new crash investigation data system, the Crash Investigation Sampling System. Occupants who sustained fatal injuries were included. Frontal impacts were defined based on the highest severity general area of damage (GAD1 = F), and cases were excluded if there were no pictures or full vehicle inspection of the case vehicle.
For each case, pictures, narratives, contact points, and other investigation data were reviewed to determine the probable injury causation scenario for each AIS 3+ injury. Maximum injury severity of the rear seat occupant was also compared with the maximum injury severity of the front seat occupants in the same crash. All results are reported as unweighted data.
Fatal crash identification in FARS and data collection
Fatal crashes were identified using the 2014–2015 FARS, the most recent FARS data available at the time the study began. A fatal crash was defined as a collision of one or more vehicles in which an occupant ages 6 to 12 years or 55 years and older died within 30 days of the crash. Occupants were excluded when the cause of death was not a direct result of the impact (e.g., drowning from lack of an ability to swim). Then, police jurisdictions associated with each crash were contacted to obtain the police accident report, crash investigation documentation including scene and vehicle photographs, relevant interviews, documentation of the scene and vehicle damage, and occupant restraint and injury data. Jurisdictions were only contacted if personal information such as the driver’s name was known, because in most cases it was necessary to obtain reports. Additionally, California, Iowa, Kentucky, New Hampshire, Minnesota, and Utah had laws that prohibited the release of crash reports for the study; agencies in these states were not contacted. All reports included ages of the occupants and their seating positions, restraint and airbag use, vehicle identifications, and impact type. In total, 182 valid crash records were obtained and reviewed, and 81 cases were in frontal impacts eligible for study. More detailed information on the data collection for the entire data set can be found in Figure A1 (see online supplement).
Crash descriptions and photos were reviewed to determine survivability. The authors assessed the crashes individually and met to reach a consensus on each. Crashes were considered unsurvivable if the impact caused a complete reduction of the respective occupant space. Crashes were considered survivable if the occupant space was partially or fully maintained or adjacent or similarly loaded occupants survived with a nonincapacitating injury. Cases for which there were no photos available or that did not meet these criteria were labeled as undeterminable. Maximum injury severity of the rear seat occupant was also compared with the maximum injury severity of the front seat occupants in the same crash. Injury severity of the front seat occupants was based on the police-reported injury severity using the KABCO scale. Therefore, occupants with K-level injuries sustained the same injury severity as case occupants and all other injury classifications were considered less severe.
Results
A detailed case series review was completed for 117 rear seat occupants: 36 with Maximum Abbreviated Injury Scale (MAIS) 3+ injuries in NASS-CDS and 81 fatalities identified in FARS. For cases identified in FARS, crash reports of frontal crashes were obtained from 29 different states. The information included in the fatal crash reports varied by state or jurisdictional data-sharing practices. Police accident reports were available for all 81 cases, pictures documenting the vehicle damage and crash scene were available for 47 cases, and electronic data recorder (EDR) data were available for 12 cases.
shows the distribution of occupant, vehicle, and crash information for the sample of crashes in the study. The majority of occupants in all cohorts were female and seated in the second-row outboard positions. Two occupants from NASS-CDS, ages 13 and 17 years, and 2 occupants from FARS, ages 7 and 9 years, were seated in the third row. Most occupants were using the lap–shoulder belt at the time of the crash. Six of 8 occupants restrained by a lap belt only had a shoulder belt available that was not worn properly (e.g., worn under the arm or behind the back) but explicit misuse was only documented in 2 cases: One in which the shoulder belt was behind the back and one in which the lap–shoulder belt was shared with an additional noncase occupant but lap belt only use was coded. More than half of the case occupants were seated in passenger cars. Thirteen of 36 vehicles in NASS-CDS cases and the majority of FARS cases were in vehicles model year 2008 or newer.
Table 1. Distribution of occupant, vehicle, and crash information for the study sample.
Crash severity
Estimates of crash severity for the study sample are shown in . Delta-V was available in 30 NASS-CDS cases, including 7 cases based on EDR data and 12 FARS cases based on EDR data. For NASS-CDS cases, delta-V ranged from 19 to 105 km/h with a median delta-V of 43 km/h. For FARS cases, longitudinal delta-V ranged from 44 to 129 km/h with a median delta-V of 62 km/h. Figures A2 and A3 (see online supplement) show the case vehicles representing the least severe crashes in the 2 data sets, an estimated 19 km/h crash in NASS-CDS and a 44 km/h crash identified in FARS.
Table 2. Crash severity based on delta-V (estimated or EDR-measured delta-V, when available),Table Footnotea survivability assessment for FARS cases, and injury severity of the rear seat occupant relative to the injury severity of the front seat occupants.
FARS cases were able to be assessed for survivability if sufficient photo evidence of the case vehicle was available or if the investigative report contained detailed scene descriptions, impact speed, or outcomes for other occupants that clearly conveyed the crash’s severity. Of the 81 FARS cases, 12 were rated as unsurvivable, 44 as survivable, and 25 could not be determined due to a lack of evidence.
Cases were also assessed for the injury severity of the case occupant relative to the front seat occupants in the same crash (). In NASS-CDS cases, the rear seat case occupant had a MAIS score higher than the MAIS score of front seat occupants in 21 of 36 cases. Eleven of the FARS cases were crashes that were fatal for all occupants in the vehicle, but 39 cases had crashes where the case occupant was the only fatality.
Injuries
shows the injured body regions by age group for NASS-CDS and FARS cases. Case occupants in NASS-CDS sustained an average of 2.5 AIS 3+ injuries in an average of 1.5 body regions. Six of these occupants, all ages 64 years or older, sustained fatal chest injuries in noncatastrophic crashes. Injury information varied widely in FARS cases, with autopsy or hospital injury records available for 18 cases and other medical information available for another 19 cases. Comprehensive injury information was available for some cases, but others provided more generic information such as “blunt force trauma” or “neck injury.” Standardized injury severity coding such as AIS codes was not available for any FARS cases. However, documented superficial injuries such as chest bruising or extremity fractures generally consistent with AIS 1 or 2 injuries were not included in injury counts.
Figure 1. Injured body regions of case occupants stratified by age and data source. FARS counts limited to cases with documented injuries (n = 17 for 6–12 years and n = 20 for 55+ years).
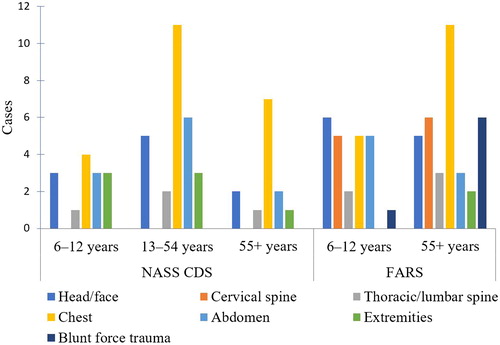
In both data sets, the injured body regions most commonly documented were the chest, head, and abdomen. Serious chest injury was present in 22 NASS-CDS occupants, including 4 of 10 occupants ages 6 to 12 years, 11 of 19 occupants ages 13 to 54 years, and 7 of 7 occupants ages 55 years and older. The type and severity of chest injury differed by age: Children ages 6 to 12 years sustained lung contusions; occupants ages 13 to 54 years sustained lung contusions (6 cases), hemo/pneumothorax (8 cases), and rib fractures (4 cases); and occupants ages 55 and older sustained an average of 3 chest injuries each, including rib fractures (6 cases), hemo/pneumothorax (4 cases), lung contusions (4 cases), and heart or vessel damage (4 cases). Chest injuries were documented in 7 and 11 of the child and older occupant FARS cohorts, respectively.
Nine NASS-CDS occupants and 18 FARS occupants sustained a serious head injury. Abdomen injuries were present in 10 and 8 occupants in NASS-CDS and FARS, respectively. In NASS-CDS cases, 9 occupants sustained hollow organ injuries, 1 sustained an abdominal vessel injury, and 2 sustained solid organ injuries. Thoracic/lumbar spine injuries were present in 4 injured occupants and 5 fatalities.
Serious cervical spine injuries were not present in NASS-CDS cases but were documented in 11 of the fatal cases, including 5 of 17 children and 6 of 20 older occupants. Cervical spine injuries were documented as atlanto-occipital dislocation/disarticulation in 5 cases, cervical spine fracture in 2 cases, and “massive neck trauma,” “neck instability,” “broken neck,” or “neck injury” in the remaining 4 cases. More detailed information on cases with cervical spine injury is included in Appendix B (see online supplement).
For occupants with head and chest injuries, shows concomitant AIS 3+ injuries to the head, cervical spine, chest, and abdomen. Of the 12 children ages 6 to 12 years in FARS who sustained head injuries, 5 sustained concomitant injuries to the chest, and 3 additionally sustained injuries to the cervical spine and abdomen. Five of the 7 children who sustained chest injury also sustained a head injury. Of the 6 occupants in FARS ages 55 years or older with head injuries, 3 sustained concomitant injuries to the cervical spine and 2 sustained concomitant injuries to the chest. Two of the 11 older occupants who sustained chest injuries also had concomitant head injuries.
Table 3. Concomitant AIS 3+ injuries to the head, cervical spine, chest, and abdomen in occupants with head and chest injuries.
Injury causation scenarios in NASS-CDS cases
The most probable injury causation scenarios were determined for each documented AIS 3+ injury in NASS-CDS cases. documents these scenarios by body region for the head/face, chest, and abdomen, stratified by occupant age. Injury causation scenarios were similar for all or most injuries within a given body region; therefore, one dominant scenario is listed per region. Eight of 10 occupants with head injuries sustained them via contact with the vehicle interior, specifically the front seatback for 6 of the 10. Two head injuries in older occupants were due to inertial loading. Across all age groups, 20 of 22 occupants with chest injuries sustained them due to shoulder belt loading. Abdominal injuries were primarily caused by lap belt loading, with evidence of submarining in 8 of 12 occupants.
Table 4. Injury causation scenarios for injured head/face, chest, and abdomen body regions for NASS-CDS cases.
Factors contributing to fatal injuries in FARS
Cases identified in FARS had limited pictures, occupant contact information, and injury descriptions. Therefore, probable injury causation scenarios were not identified. Each case was reviewed for possible factors contributing to head, chest, and abdomen injuries (). Multiple factors may contribute to a single injured body region, so counts may not total case counts. Of the 37 fatalities with documented injuries, 7 were determined to be unsurvivable due to catastrophic intrusion, 16 were survivable, and 14 were indeterminable. For cases considered survivable, intrusion was ruled out as a contributing factor in 11 cases, a possible factor in 2 cases, and could not be determined in 3 cases.
Table 5. Possible factors contributing to head, chest, and abdomen injuries in FARS fatality cases. Multiple factors may contribute to a single injured body region.
Twelve of the child fatalities had documented head injuries, including 6 in unsurvivable crashes due to catastrophic intrusion into the occupant’s space and 1 in which noncatastrophic intrusion may have been a contributing factor. Intrusion was a probable factor in 2 occupants with head injuries in the older cohort, including 1 with catastrophic/unsurvivable intrusion. Another case likely had excessive head excursion from using the lap belt only. Six case occupants, 3 in each of the child and older occupant cohorts, had documented cervical spine injuries in addition to the head injury.
Chest injuries were documented in 7 and 11 of the child and older occupant cohorts, respectively, and shoulder belt loading was the most common contributing factor (4 child and 7 older occupant). Two fatalities in the older cohort were documented as obese, which was likely an additional contributing factor. Catastrophic/unsurvivable intrusion was a factor in 2 child and 2 older cohort FARS cases involving chest injury.
In the cohort of child fatalities, 1 case occupant was using a lap belt only and had abdomen and lower spine injuries, suggesting submarining. Three case occupants were using the lap–shoulder belt and had documented bowel injuries and associated solid organ injuries and/or chest injuries, suggesting that belt loading was a factor, but the contribution of lap versus shoulder belt loading to the injury could not be determined. In the cohort of older occupant fatalities, 3 case occupants sustained abdomen injuries to the spleen or liver and associated chest injuries, suggesting that shoulder belt loading was a factor.
Discussion
This study examined the crash and restraint factors that contributed to injuries and deaths of rear-seated restrained occupants in frontal impacts in newer model year vehicles. The primary factors leading to injury were belt restraint loading and impact with vehicle interiors, and factors in fatally injured cases included belt restraint loading and unsurvivable crash severity. Rear seat occupants sustained serious and fatal injuries in crashes in which front seat occupants were less severely injured, suggesting a discrepancy in restraint performance between the front and rear rows. For fatal cases, 80% of the crashes with enough data to make a determination were considered survivable, suggesting that improved occupant protection measures may result in improved injury outcomes.
Crash severity for many of the fatal crashes was limited to a judgment of survivability, with delta-V captured from EDRs in only 12 cases. Estimated delta-Vs were available for most NASS-CDS cases. For cases with estimated or measured delta-Vs, the median delta-V was 42 km/h for injury cases and 62 km/h for fatalities, which is in line with or even less severe than many delta-Vs in current U.S. frontal crash test programs (Aylor et al. Citation2006; Locey et al. Citation2010; Sherwood et al. Citation2010; Stucki and Fessahaie Citation1998), although it is important to consider that calculated delta-Vs are likely to underestimate the actual delta-V experienced by the vehicle for offset crashes (Nolan et al. Citation1998; Sherwood et al. Citation2010; Stucki and Fessahaie Citation1998). In the fatal cases, about 4 out of 5 cases with enough information to make a determination were considered to be survivable, but that proportion dropped to 3 out of 4 cases for fatally injured children. The prevalence of survivable crashes in this study is in contrast to a previous study of younger fatally injured children in child restraints, in which half of the crashes were so severe that they were considered unsurvivable (Sherwood et al. Citation2003).
Shoulder belt loading was the probable cause of 20 of the 22 NASS-CDS cases with chest injuries and contributed to 11 of the 18 FARS cases with documented chest injuries. Chest injuries were prominent in seriously and fatally injured occupants of all ages, although the type of injury varied by occupant age, with children sustaining lung contusions and older occupants sustaining rib fractures, heart, and vessel injuries. These differences in chest injury patterns are consistent with previous literature (Arbogast et al. Citation2012). The overall incidence of chest injuries is consistent with earlier studies of restrained rear seat occupants in older vehicles in which the chest was the most commonly injured body region for occupants ages 9 years and older (Beck et al. Citation2016; Kuppa et al. Citation2005; Parenteau and Viano Citation2003). Studies examining chest injury causation in the rear seat have also found shoulder belt loading as the primary cause of chest injury (Arbogast et al. Citation2012; Beck et al. Citation2016; Kuppa et al. Citation2005). Restraint strategies that reduce loading to the chest, such as belt force limiters, should be considered for the rear seat environment, but there may be potential tradeoffs with increased head excursion (Brumbelow et al. Citation2007). In NASS-CDS cases, only 4 of 22 occupants with chest injuries also sustained head injuries, suggesting that the shoulder belt engagement prevented the head from hitting the vehicle interior. However, in FARS cases, 5 of 7 children and 2 of 11 older occupants with chest injuries also sustained head injuries. Four of these children and both older occupants showed some indication of head contact, underscoring the consequences of head excursion. The current regulation governing seat belt assemblies (FMVSS 209) limits the belt system elongation in the rear even when force limiters are present (NHTSA Citation2001), which may limit head excursion at the expense of increased loading. Novel restraints such as inflatable belts, rear airbags, or alternate belt designs may provide increased protection (Forman et al. Citation2009; Hu et al. Citation2017; Sundararajan et al. Citation2011), but any new restraint designs must consider the specific characteristics of rear seat populations and second and third row designs.
Lap belt loading/submarining was the primary cause of abdominal injuries in NASS-CDS, but no fatal cases had enough information to clearly indicate submarining. Abdominal injuries were documented in 7 injury cases and 8 fatal cases and were present in all age groups. Previous research on the rear seat has suggested that abdominal injuries are more common in belt-restrained children and younger adults (Beck et al. Citation2016; Kuppa et al. Citation2005). Children who are too small for the seat belt to fit properly are at particular risk of abdominal injury (Durbin et al. Citation2001; Nance et al. Citation2004). However, submarining-related abdominal injuries were present in 6 NASS-CDS occupants ages 13 years or older, suggesting that submarining behavior in the rear seat is not unique to the smallest occupants.
Impact with vehicle interior components was the primary cause of head and facial injuries in NASS-CDS for occupants ages 6 to 54 years. Seven NASS cases documented head injury from impact with the front seatback or interior pillars. Occupants ages 55 years and over only suffered head injuries due to inertial loading. In FARS cases, intrusion and associated neck injury were the primary causes of head and facial injuries. Head impacts with vehicle interiors are primarily the result of excessive excursion; restraint designs targeted at improving protection for rear seat occupants should also include consideration for limiting head excursions. Prior research on optimized belt designs has found that chest loading from the seat belt can be reduced while also maintaining head excursions (Forman et al. Citation2008). Research on other novel belt designs, such as inflatable belts, has shown that impact direction can greatly influence head excursions with these designs (Edwards and Nash Citation2017).
Cervical spine injuries were documented in 11 fatal cases, 5 child cases and 6 older occupant cases, but no instances of AIS 3+ cervical spine injuries were documented in NASS-CDS cases. The most well-documented injuries included 5 cases with atlanto-occipital dislocation. Although cervical spine injuries are complex with multiple possible mechanisms, atlanto-occipital dislocation injuries have been documented as occurring from distraction, hyperextension, hyperflexion, rotation, or a combination of these loading conditions (Adams Citation1992; Hall et al. Citation2015; Montaine et al. 1991). Half of the cases with atlanto-occipital separation or other severe cervical injury showed no evidence of head contact, including no extracranial contusion, fracture, or other traumatic brain injury that would indicate blunt impact to the face or frontal or parietal aspects of the skull. The remaining 5 cases all had evidence of head contact ranging from abrasion to skull fracture. Injury causation scenarios were not determined for fatal cases due to insufficient case information. However, 10 of 11 of these occupants were lap–shoulder belt restrained and 8 had associated chest injuries, suggesting that the shoulder belt heavily loaded the chest, which may indicate a distraction/flexion mechanism due to inertial loading from the head.
Some limitations should be considered when interpreting the findings of this study. NASS-CDS cases provide detailed injury and crash investigation details, but only 36 cases in 11 years of data met the inclusion criteria for the study. Cases were reviewed individually and not weighted to represent the tow-away crash population, so injury descriptions and distributions are limited to the specific sample and should not be extrapolated. For fatalities identified in FARS, case reviews were limited by inconsistent documentation of crash damage and injuries. In addition, due to limited resources, fatal case review was limited to 2 vulnerable populations, children and older occupants, and their fatal crash experiences should not be extended to rear seat occupants of all ages.
Despite these limitations, the current study provides insight into the factors that contribute to serious and fatal injuries in restrained rear-seated occupants in frontal crashes and points to possible countermeasures. The prevalence of serious and fatal injuries from belt restraint loading, particularly in crashes in which front seat occupants sustained less severe injuries, suggests a discrepancy in restraint performance between the front and rear rows and a need to reduce loading to the chest in rear seating positions. However, the presence of head injuries from contact with the vehicle interior points to the need to consider potential tradeoffs of reduced chest loads with increased head excursion, particularly in the absence of rear seat airbags. Any new restraint designs should consider the unique needs of the rear seat environment.
Supplemental Material
Download PDF (896.1 KB)Acknowledgment
The authors thank the Preusser Research Group for their work in case identification and data collection.
Additional information
Funding
Related Research Data
References
- Adams VI. Neck injuries: I. Occipitoatlantal dislocation—a pathologic study of twelve traffic fatalities. J Forensic Sci. 1992;37:556–564.
- Arbogast KS, Locey CM, Zonfrillo M. Differences in thoracic injury causation patterns between seat belt restrained children and adults. Ann Adv Automot Med. 2012;56:213–221.
- Aylor DA, Nolan JM, Zuby DS, Baker BC. How the 64.4 km/h (40 mi/h) frontal offset deformable barrier crash test relates to real-world crash severity. Paper presented at: Expert Symposium of Accident Research (ESAR); 2006; Hannover, Germany.
- Beck B, Bilston LE, Brown J. Injury patterns of rear seat occupants in frontal impact: an in-depth crash investigation study. Inj Prev. 2016;22(3):165–170.
- Bilston LE, Du W, Brown J. A matched-cohort analysis of belted front and rear seat occupants in newer and older model vehicles shows that gains in front occupant safety have outpaced gains for rear seat occupants. Accid Anal Prev. 2010;42:1974–1977.
- Braver ER, Whitfield R, Ferguson SA. Seating positions and children's risk of dying in motor vehicle crashes. Inj Prev. 1998;4(3):181–187.
- Brumbelow ML, Baker BC, Nolan JM. Effects of seat belt load limiters on driver fatalities in frontal crashes of passenger cars. In: Proceedings of the 20th International Technical Conference on the Enhanced Safety of Vehicles. Washington, DC: NHTSA; 2007.
- Durbin DR, Arbogast KB, Moll EK. Seat belt syndrome in children: a case report and review of the literature. Pediatr Emerg Care. 2001;17:474–477.
- Durbin DR, Chen I, Smith R, Elliott MR, Winston FK. Effects of seating position and appropriate restraint use on the risk of injury to children in motor vehicle crashes. Pediatrics. 2005;115:e305–e309.
- Durbin DR, Jermakian JS, Kallan MJ, et al. Rear seat safety: variation in protection by occupant, crash and vehicle characteristics. Accid Anal Prev. 2015;80:185–192.
- Edwards M, Nash C. Inflatable shoulder belts and inboard upper anchor shoulder‐belt geometry in far‐side oblique impacts. Paper presented at: International Research Council on Biomechanics of Injury (IRCOBI); 2017; Antwerp, Belgium.
- Farmer CM, Lund AK. The effects of vehicle redesign on the risk of driver death. Traffic Inj Prev. 2015;16:684–690.
- Forman J, Lopez-Valdes F, Lessley D, et al. Rear seat occupant safety: an investigation of a progressive force-limiting, pretensioning 3-point belt system using adult PMHS in frontal sled tests. Stapp Car Crash J. 2009;53:49–74.
- Forman J, Michaelson J, Kent R, Kuppa S, Bostrom O. Occupant restraint in the rear seat: ATD responses to standard and pre-tensioning, force-limiting belt restraints. Ann Adv Automot Med. 2008;52:141–154.
- Hall GC, Kinsman MJ, Nazar RG, et al. Atlanto-occipital dislocation. World J Orthop. 2015;6:236–243.
- Hu J, Reed MP, Rupp JD, Fischer K, Lange P, Adler A. Optimizing seat belt and airbag designs for rear seat occupant protection in frontal crashes. Stapp Car Crash J. 2017;61:67–100.
- Insurance Institute for Highway Safety. General Statistics Fatality Facts. 2016. Available at: http://www.iihs.org/iihs/topics/t/general-statistics/fatalityfacts/overview-of-fatality-facts. Accessed March 14, 2019.
- Kuppa S, Saunders J, Fessahaie O. Rear seat occupant protection in frontal crashes. In: Proceedings of the 19th International Technical Conference on the Enhanced Safety of Vehicles (ESV). Washington, DC: NHTSA; 2005.
- Locey CM, Garcia-Espana JF, Toh A, Belwadi A, Arbogast KB, Maltese MR. Homogenization of vehicle fleet frontal crash pulses from 2000–2010. Ann Adv Automot Med. 2012;56:299–311.
- Montane I, Eismont FJ, Green BA. Traumatic occipitoatlantal dislocation. Spine (Phila Pa 1976). 1991;16(2):112–116.
- Nance ML, Lutz N, Arbogast KB, et al. Optimal restraint reduces the risk of abdominal injury in children involved in motor vehicle crashes. Ann Surg. 2004;239:127–131.
- NHTSA. Letter of Interpretation about Load Limiters and the Belt Elongation Requirements of Federal Motor Vehicle Safety Standard No. 209, Seat Belt Assemblies [legal interpretation]. 2001. Available at: https://www.nhtsa.gov/interpretations/24256ogm. Accessed March 14, 2019.
- Nolan JM, Preuss CA, Jones SL, O’Neill B. An update on relationships between computed delta-Vs and impact speeds for offset crashes. Paper presented at: 16th International Conference on Enhanced Safety of Vehicles; June 1998; Windsor, Canada.
- Parenteau C, Viano DC. Field data analysis or rear occupant injuries part I: adults and teenagers. Paper presented at: SAE World Congress; 2003; Detroit, MI.
- Sahraei E, Digges K, Marzougui D. Reduced protection for belted occupants in rear seats relative to front seats of new model year vehicles. Annu Proc Assoc Adv Automot Med. 2010;54:149–158.
- Sherwood CP, Ferguson SA, Crandall JR. Factors leading to crash fatalities to children in child restraints. Ann Assoc Adv Automot Med. 2003,47:343–359.
- Sherwood CP, Zuby DS, Nolan JM, Aylor DA. The accuracy of velocity change estimates in small overlap frontal crashes. Paper presented at: Expert Symposium of Accident Research (ESAR); 2010; Hannover, Germany.
- Stucki S, Fessahaie O. Comparison of Measured Velocity Change in Frontal Crash Tests to NASS Computed Velocity Change. 1998. SAE Technical Paper 980649. Warrendale, PA: Society of Automotive Engineers.
- Sundararajan S, Rouhana SW, Board D, et al. Biomechanical assessment of a rear-seat inflatable seatbelt in frontal impacts. Stapp Car Crash J. 2011;55:161–198.
- Winston F, Xie D, Durbin D, Elliot MR. Are child passengers bringing up the rear? Evidence for differential improvements in injury risk between drivers and their child passengers. Ann Adv Automot Med. 2007;51;113–127.
