
The venerable flow-volume relationship of the lung of was originally described by Bob Hyatt and Donald Fry in 1958 [Citation1]. Hyatt had planned to go in the private practice-specifically family medicine-so what had originally planned to be a short encounter with science turned into a lifelong passion for investigating the mechanics of the lung [Citation2]. One of the things that always characterized Bob Hyatt’s approach to research was linkage of laboratory findings to practical clinical medicine and it is hard to think of something more practical than the flow volume loop! Once during a scientific meeting, I asked Bob what caused him to focus his attention on the relationship between flow and volume as opposed to pressure and flow. Bob’s response was that the shape of the flow volume relationship just looked quite interesting, he noted the flattening of the loop in patients with COPD and he thought that one could actually learn something by just assessing the shape. Moreover, you did not have to insert an esophageal balloon, that is certainly not very practical for every patient that walks into the clinic. We have been looking at the shape of the flow volume curve ever since.
The inspiratory part of the flow volume loop is generally underappreciated and certainly underutilized [Citation3]. Indeed, the inspiratory limb of the flow volume loop was left out of spirometry recommedations until relatively recently [Citation4]. To decrease the time spent with patients in the clinic and to deal with issues of contamination most pulmonary function laboratories only obtain expiratory limb of the flow volume loop and/or I find most physicians rarely examine the loops. Again, Bob Hyatt’s seminal work in this area showed us that the shape of the flow volume loop on inspiration can be highly instructive clinically [Citation5]. One of the most common uses of the inspiratory loop is the characteristic truncation seen in patients with vocal cord dysfunction or central airway lesions [Citation3]. Like the early part of expiration, inspiration is very effort dependent but in addition clearly reflects the caliber of the large conducting airways. However, the spirometry recommendations are generally silent on the issue and so there is little guidance on how best to perform a maximum inspiratory maneuver. For instance, is it better to first expired fully to residual volume (RV) and then inspire to total lung capacity (TLC) then expire forcefully expire or does one perform the expiratory part of the loop and then perform maximal inspiratory maneuvers? An argument could be made either way. While most agree that patients with asthma or COPD differ in a number of indices obtained from expiratory spirometry, any differences during maximal inspiratory are rarely considered and investigated.
In the current issue of the Journal, Okazawa and colleagues [Citation6] report pulmonary function results from patients with either COPD (N = 143) or Asthma (N = 142) who had attended their university hospital clinic over a period of six years. COPD was assessed in the usual fashion and included; smoking (average 50 pack years), a ratio of forced expiratory volume in one second to forced vital capacity (FEV1/FVC) below 70%, imagining consistent with emphysema, which was predominately centralobular as might be expected, and the usual drug prescriptions for patients with COPD. Bronchial asthma was assessed as recommended by the GINA document and included either a bronchodilator response or a positive methacholine challenge test. As we will see later on, the bronchial asthma group was unique as it included smoking asthmatics. Spirometry, i.e. flow-volume maneuvers, where obtained in the standard fashion except for the fact that the patient preformed a maximum inspiration starting at end expiration or functional residual capacity (FRC) followed by a maximum expiratory maneuver from TLC and down to RV. Their clinical experience suggested that performing maximum inspiration by first expiring to RV is not reproducible especially in the older subjects. In my experience testing patients with asthma and COPD, these patients with reactive airways the deflation to RV also triggers paroxysmal coughing likely do to activating rapidly adapting irritant receptors [Citation7,Citation8]. This deflation-induced coughing makes getting a good flow-volume loop nearly impossible Hence, the interesting technical finding from this study is a practical means to determine maximum inspiratory maneuver and from this the peak inspiratory flow (PIF) could be determined.
Comparing the flow-volume loops between the two airway disease entities reveals marked differences in indices derived from the flow-volume relationships; however, the two major discriminators where the ratio of peak inspiratory flow to maximal flow at 50% vital capacity (PIF/MEF50) and the venerable FEV1/FVC ratio. The odds ratio for determining that patient had COPD for FEV1/FVC was 6.5 when adjusting for age, sex and smoking status. Now this finding is not surprising as this is the major and robust index used to describe COPD, provides external validity and has been commented upon many times in the literature and in this journal [Citation9–11]. Next let us consider the intriguing additional benefit of assessing PIF. Now here things got interesting because the authors did something real unique because of the unusual group of patients they evaluated since it allowed them to compare smoking groups; smoking asthmatics and COPD patients. For these two groups of smokers and when adjusted for age and sex, the FEV1/FVC and the PIF/MEF50 where both significant with similar odds ratios (COPD: OR 4.3, Asthma: OR 4.6). Use of MEF25 produced similar results. When the authors evaluated the total population, the additional benefit of considering both FEV1/FVC and PIF/MEF50 yielded an OR of 12.4. Moreover, when these dual criteria were applied to the two smoking groups the resultant OR was 20.7!
The comparisons of flow-volume relationships between COPD and asthma reported in this paper are fascinating, striking and likely to be clinically relevant. The intrathoracic airways are markedly influenced by volume change as concisely discussed in the introduction for this paper. What are the pathophysiologic implications of these findings? I was taken with these results because they provided a clear picture of the difference between mechanical properties of the airway walls between asthma and COPD. In the case of the asthmatic who has produced expiratory flow one is left with the conclusion that the airways and narrowed likely due to structural alteration of the airway wall. Hardening of the airway if you will. On the other hand, the airways of the COPD patient are clearly different. The best explanation is that these airways, due to loss of parenchymal tethers, are now quite dispensable; hence, upon expiration COPD airways narrow whereas upon inspiration they are tethered open.
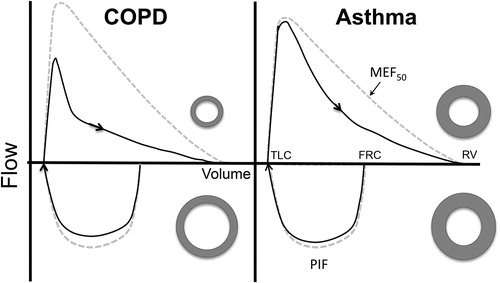
(see also Figure 1 in Okazama et al.) captures the differences between the two diseases. For a COPD patient there is a relative preservation of inspiratory flow in the face of losses of expiratory flow. When translated to changes in airway caliber it suggests that on inspiration the airways are tethered open whereas during expiration, as everyone knows, airways are compressed likely caused by the physical changes in the dispensability of the airway wall due mostly due to the loss of tethering [Citation12]. On the other hand, for a patient with asthma, there is probably less of a preservation of inspiratory flow in the face of loss of expiratory flow. This is all likelihood as we [Citation13] and others [Citation14] have shown is due to structural remodeling, specifically fibrosis, of the airway wall (see hypothetical airways in ). The current study suggests that airways of COPD and bronchial asthma are strikingly different when losses of expiratory flow are put into the context of maximal inspiratory flow. Clearly the use of inspiratory flow provides a simple means to distinguish between the mechanical properties of airways in these two different diseases.
Figure 1. Flow-volume relationships for a theoretical patient with COPD (left hand panel) and for a patient with asthma (right hand panel) preformed using the technique for maximal inspiration described by Okazawa at all (4). Following a period of quiet breathing the patient takes a maximum inspiration from functional residual capacity (FRC) to total lung capacity TLC with a maximum expiration to residual volume (RV). From the expiratory limb the forced expiratory volume in one second (FEV1), forced vital capacity (FVC) are determined and maximum expiratory flow rate at 50% vital capacity (MEF50) is measured. In addition, maximum inspiratory flow (PIF) is measured from the inspiratory limb. For the patient with asthma, expiratory flow is diminished likely due to thickening of the airways with minimum compression during expiration and minimal tethering during inspiration. On the other hand, for the patient with COPD expiration is diminished in part due to compression of airways due to lost of parenchymal tethering; that is, the airways are functionally more dispensable. On inspiration the same airway is pulled open as illustrated by the adjacent donut shapes. As result the FEV1/FVC is reduced in both cases but more so the case of the patient was COPD. PIF/ MEF50 is increased in both cases; the more so in the case of patients with COPD, because of the relative preservation of inspiratory flow. As a result, using both indices would be predicted to better discrimination between the two forms of airways disease.
What are the clinical implications of these findings? Determining whether a person has asthma or COPD establishes the first line of therapeutic options to be considered. These options are clearly not the same as recommendations for these diseases clearly indicate. Sensitivity and specificity analysis performed in this investigation clearly show that spirometry once again is highly effective in determining the difference between two common airway diseases. Perhaps this analysis could be used to guide first line therapy. The combination of FEV1/FVC and PIF/MEF50 was particularly impressive in separating the two smoking groups; accordingly, given the current interest in asthma-COPD overlap (ACO) syndrome, does this approach suggest an opportunity to both better understand and treat ACO? In particular, the smoking asthmatic presents a common clinical challenge, as it is so often unclear whether they have asthma or COPD.
Will these exciting findings be put into immediate clinical practice? Unfortunately, I suspect this will not happen. Near-term they will be a reluctance to perform inspiratory spirometry because of fear of contamination and transmission of viral infections such as COVID-19. This is certainly what happened when HIV became such a concern since it led to the introduction of spirometer filters. This uniform practice persists even the absence of compelling evidence that inspiring from a spirometer would result in acquiring an infectious disease. The current COVID-19 pandemic has resulted in nearly complete shuttering of pulmonary function laboratories labs worldwide. They will be slow to reopen and I think we should worry that many labs may never reopen. Secondly, use of spirometry in general is not widespread. A situation seems that seems crazy in the face of the fact that difficult to access, high-end diagnostic tests such CT are so widely used; whereas, spirometry languishes. The solution is education and advocacy of to ourselves and to other healthcare professionals.
Declaration of interest
C.G. Irvin is a scientific consultant for Medical Graphics Corporation. In the last year, he has received speaker fees/honoraria from various Universities. He is funded by the American Lung Association and NIH (T32 HL076122) and is an employee of the University of Vermont and the University of Vermont Medical Center.
Additional information
Funding
References
- Hyatt RE, Schilder DP, Fry DL. Relationship between expiratory flow and degree of lung inflation. J Appl Physiol. 1958;13(3):331–336. doi:10.1152/jappl.1958.13.3.331.
- Wu TD, McCormack MC, Mitzner W. The history of pulmonary Function. In: Kaminsky DA, Irvin CG, editors. Pulmonary function testing. Cham, Switzerland: Humana Press/Springer International Publishing AG; 2018. p. 15–42.
- Ruppel GL. The inspiratory flow-volume curve: The neglected child of pulmonary diagnostics. Respir Care. 2009;54(4):448–449.
- Miller MR, Hankinson J, Brusasco V, et al. Standardization of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805.
- Miller RD, Hyatt RE. Obstructing lesions of the larynx and trachea: clinical and physiological characteristics. Mayo Clin Proc. 1969;44(3):145–161.
- Okazawa M, Imaizumi K, Mieno Y, et al. Ratio of maximal inspiratory to expiratory flow aids in the separation of COPD from asthma. COPD. 2020. doi:10.1080/15412555.2020.1742679
- Widdicombe J. Functional morphology and physiology of pulmonary rapidly adapting receptors (RARs). Anat Rec. 2003;270A(1):2–10. doi:10.1002/ar.a.10003.
- Lavorini F, Chellini E, Bigazzi F, et al. The clinical value of deflation cough in chronic coughers with reflux Symptoms. Chest. 2016;149(6):1467–1472. doi:10.1016/j.chest.2016.01.008.
- Irvin CG. Classifying the severity of COPD: are we there yet? COPD. 2017;14(5):463–464. doi:10.1080/15412555.2017.1359244.
- Coton S, Vollmer WM, Bateman E, et al. Severity of airflow obstruction in chronic obstructive pulmonary disease (COPD): proposal for a new classification. COPD. 2017;14(5):469–475. doi:10.1080/15412555.2017.1339681.
- Swanney MP, Ruppel G, Enright PL, et al. Using the lower limit of normal for the FEV1/FVC ratio reduces the misclassification of airway obstruction. Thorax. 2008;63(12):1046–1051. doi:10.1136/thx.2008.098483.
- Irvin CG. Pulmonary physiology. 2nd ed. In: Barnes PJ, Drazen JM, Rennard SI, et al., editors. Asthma and COPD: basic mechanisms and clinical management. Boston (MA): Elsevier Academic Press; 2009. p. 55–69.
- Neveu WA, Allard JL, Raymond DM, et al. Elevation of IL-6 in the allergic asthmatic airway is independent of inflammation but associates with loss of central airway function. Respir Res. 2010;11(1):28–33. doi:10.1186/1465-9921-11-28.
- Bosse Y, Riesenfeld EP, Pare PD, et al. It’s not all smooth muscle: non-smooth-muscle elements in control of resistance to airflow. Annu Rev Physiol. 2010;72(1):437–462. doi:10.1146/annurev-physiol-021909-135851.