Abstract
Introduction. Freons generally have a low order of toxicity, but exposure to relatively high concentrations (>100 ppm) may produce adverse effects on health. Currently, intoxication reports are unintentional inhalation of CFCs. We report an unintentional ingestion of a mixture of CFCs and the results of a rat study. Case Report. A 43-year-old man was admitted to the Emergency Department with a chief complaint of acute abdominal pain that developed minutes after he ingested a clear liquid in a water glass, which contained a mixture of Freon and water. Subsequent surgical evaluation revealed perforation of the stomach and necrosis of the stomach wall. He developed a transient rise in his hepatic transaminases, which resolved spontaneously, and fully recovered from his surgery. Methods. A murine model of the injury was created to evaluate threshold concentration and effect of time on injury grade. Results. Injury grade increased with delay to histologic analysis from 8 to 24 hours after exposure to Freon. Increasing amounts of Freon also increased the lesion grade score. Conclusions. Patients ingesting Freon need to be closely evaluated for risk of gastric damage and perforation.
Introduction
“Freon” is a registered trademark of Dupont and refers to chlorinated and fluorinated hydrocarbon solvents. Depending on the room temperature they could be clear, colorless liquids or gases. These chlorofluorocarbons (CFCs) are widely used as a refrigerant in air conditioners and freezers, aerosol propellants, and degreasing agents. CFC's are highly lipophilic (fat/blood partition coefficient 10) and possess anesthetic action. Freons generally have a low order of toxicity, covering acute, sub-acute, sub-chronic and chronic toxicity, genotoxicity, teratogenicity, and carcinogenicity (Citation3). However exposure to relatively high concentrations (>100 ppm) may produce adverse effects on health. Currently, intoxication reports are unintentional inhalation of CFCs (Citation4,Citation5). We report an unintentional ingestion of a mixture of CFCs occurred when a healthy man mistook a bottle in a refrigerator for a bottle of plain water. This resulted in freezing, tissue necrosis, and multiple perforations of the stomach. The patient recovered after surgery to remove the damaged tissue and reestablished the gastrointestinal tract. An experimental rat study was performed in order to identify the physio-histopathology of the compound-related lesion. This study followed the principles in accordance with the guide of the Centro de Investigaciones Toxicológicas in which the experiments were carried out, and the National Research Council's guide (ANMAT) for the care and use of laboratory animals.
Case report
The patient, a 43-year-old man, was admitted to Bernardino Rivadavia Hospital, Buenos Aires, Argentina due to an accidental ingestion of a mixture of CFCs. The patient that had been healthy previously with an unremarkable medical and surgical history denied any history of alcohol or drug abuse. He took a drink of a colorless liquid that he thought was water. He shivered and felt an acute pain with ardor burning sensation from the mouth to the epigastric area minutes later after ingestion. On arrival at the hospital, the initial physical examination showed the patient's blood pressure was 140/90 mm Hg, heart rate was 95 bpm, respiration rate of 25/min, and his oral temperature was 37.1°C. Auscultation of the lungs was unremarkable. The neurological examination was normal regarding six areas of assessment: mental status, cranial nerves, motor, sensory, coordination, and reflexes.
During the physical exam, generalized abdominal rigidity was observed, with rebound tenderness in the epigastric area and tympanitic to percussion in the upper right quadrant of the abdomen. Bowel sounds were present and the liver and spleen were not palpable. There was no difficulty in swallowing. The admission laboratory studies results were sodium 141 mmol/L, potassium 3.8 mmol/L, BUN 49 mg/dL, glucose 93 mg/dL, total protein 7.1 g/dL, albumin 4.3 g/dL, alkaline phosphatase 74 U/L, aspartate aminotransferase (AST) 30 U/L, alanine aminotransferase (ALT) 10 U/L, total bilirubin 1.1 mg/dL, direct bilirubin 0.1 mg/dL, lipase 20 U/L, amylase 46 U/L, white blood cell count 12.800/μL, hemoglobin 13.5 g/L, and hematocrit 41.0%. Serologic investigation was negative for HIV, Chagas disease, and syphilis. The plain X-rays of the chest and abdomen showed the presence of air in the sub-diaphragm (pneumoperitoneum) (). The findings of free air prompted surgical consultation and exploratory laparotomy, with a presumptive diagnosis of gastric perforation. A supraumbilical laparotomy was performed, finding liquid in the peritoneal cavity and a 2 × 3 cm perforation in the lesser curvature of the stomach, which was sutured.
Fig. 1. Chest x-ray in upright position, showing the presence of free air under the inter-hepatic-diaphragm at the base of the right lung (Jobert sign).
The patient's condition improved with hydration and antibiotics (ceftriaxone 1g every 12 hours for 7 days). Omeprazole (20 mg/day) and a gastric mucous protector prophylaxis were administrated. No significant abnormal findings were observed in laboratory analysis during the days after surgery, except that the liver enzymes (AST, alkaline phosphatase, ALT) were increased about 2-fold of normal limits. The postoperative gastric fiberoptic endoscopy showed two notable excavated ulcers with hemorrhagic fundi in the subcardial and back face of the gastric body. The esophagus and the first two portions of duodenum were preserved. The patient was discharged on the tenth hospital day after interventions with improving laboratory values: total protein 6.9 g/dL, albumin 4.1 g/dL, cholesterol 123 mg/dL, alkaline phosphatase 92 U/L, AST 36 U/L, ALT 22 U/L, total bilirubin 1.0 mg/dL, direct bilirubin 0.2 mg/dL, lipase 22 U/L, amylase 49 U/L, prothrombin time (PT) 90%, partial thromboplastin time (APTT) 33 sec, white blood cell count 6.400/μL, hemoglobin 12.8 g/L, and hematocrit 38.5%. The follow-up visit at 3 months, which consisted of routine clinical examinations, laboratory tests, fiberoscopy, and neurological evaluations showed complete healing of the gastric ulcers and patient's liver function returned to normal.
Establishment of the model of stomach damage
Female Wistar rats weighing 360–390 g were used; they were fed a commercial diet. Some animals were fasted for 16 hours before the administration of Freon, meanwhile in others food was offered until the administration; water was allowed ad libitum. Freon (0.25 up to 2.0 mL) was given by a bulb-tipped gastric gavage needle. Rats were killed 8 or 24 Hours after Freon administration. The stomach was excised and opened by the main curvature; photographs were obtained before and after opening the stomach. Then the stomach was mounted on a piece of cardboard and fixed in buffered-formalin. Several samples were obtained and identified from multiples areas, embedded in paraffin and cut in sections that were stained with haematoxylin-eosin. The experimental procedure and the damage results are shown in .
Table 1. Incidence and severity of stomach lesions in female Wistar rats
Histological examination
The gross findings vary from not obvious changes up to hemorrhagic areas in the anterior and posterior fore-stomach as well as in the greater curvature (). No changes were observed in the glandular stomach. No gastric perforations were found.
Fig. 2. Rat fasted for 16 hours, received 0.5 mL of Freon, and was killed 8 hours later. Gross view of the outer surface of the stomach. Red discoloration due to congestion and hemorrhage in an area of the stomach.

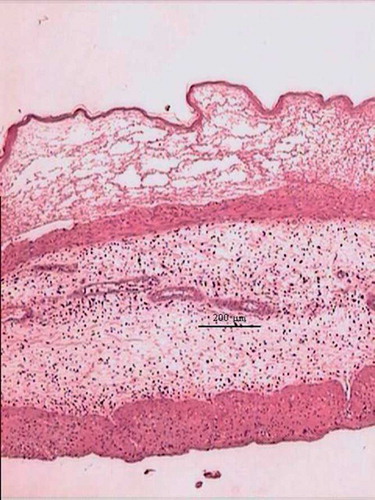
The microscopic changes were located in the fore-stomach, mainly in the epithelium, and consisted in acute inflammation with formation of intraepithelial vesicles that contained proteins, fibrin, leucocytes and/or red cells (). Necrosis of the epithelium was frequently found. Edema of the submucosa with variable infiltration of leucocytes was observed. In some rats, damage of the muscularis mucosae was observed. An increased damage was shown in high dose and fasted animals. No significant difference was observed in the histopathological images between the early versus late sacrificed groups.
Fig. 3. Rat fasted for 16 hours, received 2.0 mL of Freon, and was killed 24 hours later. Fore-stomach. Intraepithelial vesicle, edema of the sub-mucosa and inflammatory reaction. H.E.
Discussion
To our knowledge, this is the first case of ingestion of Freon reported in Argentina, although similar cases have been reported in the literature. Haj and colleagues reported the findings of the perforation of the stomach due to trichlorofluoromethane (Freon 11) ingestion by an adult male (Citation1). The authors concluded that the freezing action of Freon 11 is the cause of tissue necrosis. The patient recovered after surgical intervention. Thys et al. reported an acute neurological symptomatology (major dizziness) after accidental ingestion of Freon 134A for recreational purposes (Citation2). This main adverse effect was of short duration and the patient was discharged after 24 hours.
In the present case, there was no evidence of either neurological symptomatology or injuries in the upper airway tract, such as frostbite. Also there was no respiratory comprise regarding the possibility of liquid aspiration, entering the lungs, which may result in a potentially fatal condition (Footnote6). The mechanism of the necrosis and perforation of the stomach may be explained in the basis of the freezing effect of Freon, which results in anoxic changes. The presence of hydrochloric acid and pepsin may be an important factor in the extent of the injury regarding the protective mucous is broken or diminished. It is supposed that the antral spasm caused pooling of the corrosive at the antrum of the stomach and the damage primarily occurred there. Another reason for the greater susceptibility of the stomach is its columnar epithelium, whereas the esophagus has a more resilient squamous epithelium. As shown in the rat study, the degree of mucosal injury depended on the amount and the concentration ingested, the amount of food in the stomach at the time of ingestion and in lesser extent on the time elapsed since the ingestion of Freon. In this case, the management of gastric damage was operative and there was no treatment beyond what was done in the surgical intervention. Although the patient showed increases in serum liver enzymes, these abnormal findings were transient and did not demonstrate hepatotoxicity. At a 3-month follow-up, the patient was asymptomatic and was thriving well.
Acknowledgments
The authors thank Ana Uceda for the technical assistance.
Notes
6. EPA. 2003. Technical support document: Toxicology FREON. Office of Environmental Health Hazard Assessment. Environmental Protection Agency (revised 09/24/03).
References
- Haj M, Burstein Z, Horn E, Stamler B. Perforation of the stomach due to trichlorofluoromethane (Freon 11) ingestion. Isr J Med Sci 1980; 16(5)392–394
- Thys F, Hantson P, Hoet P, Janssens F, Verschuren F, Marion A, El Gariani A, Meert P, Reynaert M. Acute neurologic symptomatology after accidental ingestion of Freon 134A. Eur J Emerg Med 2001; 8(1)78–79
- http://fluoridealert.org/pesticides/1,1,1,2-tetrafluoroe.toxnet.htm, TOXNET profile from Hazardous Substances Data Bank, 12 July 2007
- Kubota T, Miyata A. Acute inhalational exposure to chlorodifluoromethane (Freom 22): A report of 43 cases. Clin Tox 2005; 43: 305–308
- Loh I, Chang Y, Liou S, Chang J, Chen H. Case report: Hexachloroethane smoke inhalation: A rare cause of severe hepatic injuries. Environ Health Persp 2006; 114(5)763–765