
Abstract
Large population-based cohort studies offer the chance to assess a broad number of diseases and intermediate phenotypes and to estimate their frequencies in the general population. Because of their large sample size new symptom clusters and interactions of genetic, environmental and clinical factors in the onset and course of disease can be described. The German National Cohort (GNC) is one of the mega cohorts with a study-specific concept for the assessment of different psychiatric diseases and a focus on affective disorders and on emotional and cognitive functions. Aim of this manuscript is to describe different design approaches for a priorisation in the assessment of phenotypes for psychiatric and/or neurological disorders in large cohorts and to introduce the concept of studying emotional and cognitive functions and related disorders in GNC.
Introduction
Large, prospective population based studies, so called mega cohorts, are a relatively new type of study, initiated or conducted in increasing numbers in health research around the world over the last 15 years (Manolio et al. Citation2020). While there is no clear-cut definition of the term ‘mega cohort’ most of these studies include 100,000 participants or more. The UK Biobank is the best known example for a mega cohort and had recruited 500,000 individuals in the UK between 2007 and 2010. Mega cohorts, especially when they are population-based, have several advantages over traditional smaller population based cohorts. The large number of participants allows to analyse the effect of combinations of risk factors on disorders and other outcome variables with sufficient statistical power, which is crucial for example for the identification of two or three-way interactions. Infrequent and rare diseases can be assessed as well as disease subtype classifications for more frequent diseases, tasks that cannot be performed in smaller cohorts. In case of biomaterial collections and analysis, especially for genomics and other omics analyses, mega cohorts provide an important advantage through their large sample size. But similar to smaller studies, mega cohorts have to adjust their examination program and, thus, the depth of phenotyping, to the study aims, logistics and funding. Among the disadvantages are the high absolute costs for conduction and logistics of a mega cohort, even if synergies might help to reduce per capita expenses with rising participant numbers. Thus, the definition of the overall aim and the number and depth of research areas to be studied in detail is of major importance, since the available participant time is limited. illustrates the relation between broadness of scope of a virtual study and the depth of phenotypes assessed, showing the inverse relation between the two. The broader the focus of a study that includes many different research areas or diseases, the shorter or less detailed are the phenotypes assessed and the participant time allocated to examinations of one specific phenotype.
Figure 1. The relation between depth of phenotype characterisation and number of diseases or research areas that are in the focus of a study.
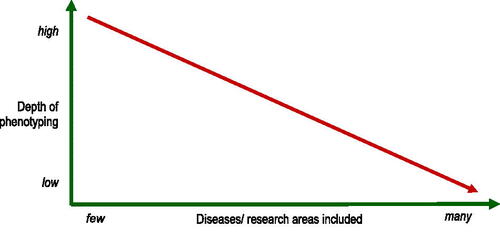
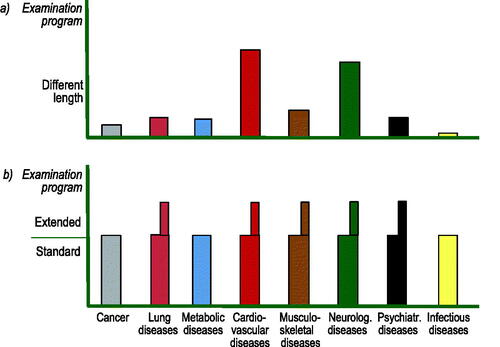
In contrast, studies focussing on just one or only few disorders, can allocate examination time to these areas and perform an in-depth assessment of the relevant phenotypes. The investigators of a new study must decide a priori about research areas and length of participant examinations and, thus, determine the depth of phenotyping on the basis of these two variables. A common approach is to only prioritise few research areas, those of highest interest, while others are only assessed superficially, as illustrated in .
Figure 2. Two different approaches to prioritise phenotype depth in large population studies.
From a scientific point of view the question how deep participants in mega cohorts are phenotyped is therefore important, given the long-term use of these data for research purposes. The UK Biobank study for example used an examination program that lasted about 90 minutes for the initial 500,000 participants and assessed many phenotypes by applying very short or screening versions of established scales (e.g. PHQ-2) to meet the limited examination time. Other mega cohorts were a priori designed to study specific research areas such as ageing and allocated most of the participants time to the examination and phenotyping within this specified area.
The German National Cohort (NAKO) (German National Cohort Consortium Citation2014) (Bamberg et al. Citation2015) is the largest population-based cohort study in Germany and has recruited 205,000 randomly selected participants in 16 German regions across the country. In the planning phase between 2010 and 2012 the planning committee decided to adopt a different approach to the question of phenotype depth (). The overall NAKO goal is to assess risk factors and determinants of major (‘frequent and/or severe’) diseases on a population level, operationalised in eight major disease groups. Thus, NAKO has a very broad research scope. It was therefore decided to develop two examination programs for the participants. Level 1 (L1) is the acronym for the standard program that lasted about four hours at each study centre and Level 2 (L2) the one for an extended program lasting in total about six hours. The investigators allocated similar amounts of examination and interview time to each of the eight research areas in the standard program. To increase depth of phenotyping additional examinations for most, but not all, research areas were added in the extended program. To allow an efficient cost benefit ratio it was decided that 80% of the future participants receive the standard program and 20% the standard plus the extended L2 program (). L2 participants were randomly chosen within each study region among all participants prior to sending the initial invitation. This approach is different from most other mega cohorts, but has the advantage of recruiting a large sample size, examined for a broad range of phenotypes and research areas while still providing an in-depth phenotyping for a random 20% of study participants. Broad and deep in this context refers to the assessment of diseases as well as to risk or protective factors.
NAKO objectives, design and examinations
The German National Cohort has four objectives, (a) the identification of pathways from lifestyle and environmental risk factors to major diseases, (b) the analysis of geographic and socio-economic disparities in health risks, (c) the improvement of prediction models for those at increased risk of specific diseases and (d) the identification of bio- and imaging-markers for subclinical disease (German National Cohort Consortium Citation2014). The scope on frequent and/or severe diseases includes eight disorder groups, cardio-vascular disorders, metabolic and lung diseases, cancer, muscle-sceletal diseases, psychiatric and neurologic disorders and syndromes and infectious diseases. At baseline, NAKO had set up 18 study centres in 16 German regions, including rural, suburban and metropolitan communities. In five of the study centres dedicated 3.0 Tesla Siemens MRI scanners were set up for a whole-body MRI of L2 study participants (Bamberg et al. Citation2015). Before baseline random samples of the defined source population for each study centre were drawn in the respective city or community registry, stratified by five-year age groups and gender. The age criterion was 20 to 69 at the time of sampling. Age groups 40–69 years were oversampled, giving the lower age groups 20 to 39 years a slightly lower weight than higher ages. All participants received a written invitation for participation with up to three reminders by mail or phone. The examination program and procedures at each study centre were completely standardised and based on a list of more than 50 Standard Operation Procedures (SOP). For each of the eight major disease groups different measurements, scales, question sets or instruments were used. Study nurses were trained and certified for each examination. A series of pilot studies, conducted in 2011 and 2012, had tested different devices, e.g. for actigraphy, automated blood pressure measurement or neuropsychological tests, in order to base the final decision for a device or measurement on results of these tests. Baseline examinations started in early summer 2014 and ended in summer 2019. About 2.5 years after baseline each participant received a written questionnaire to report the onset of new diseases since the first examination. In 2019 the first follow-up examination started for which all participants are re-invited, on average five years after baseline. This follow-up had to be paused for three months in spring 2020 due to the SARS-CoV-2 pandemia and will be continued until 2023. In addition, a linkage with their health insurance data is pending for each participant consenting to this procedure.
NAKO’s assessment of psychiatric conditions
Psychiatric and neurologic disorders and conditions are among the eight main research areas within NAKO. This is highly relevant since the spectrum of conditions and disorders within this area convey a huge individual and societal burden. According to the World Health Organisation (WHO) these conditions account for 13% of the global burden of disease and 30% of that due to non-communicable diseases. One out of five individuals, in total more than 700 million people, currently lives with one or more of the disorders. Among them are 150 million people with depression, 38 million with epilepsy, and 90 million with a substance abuse disorder (World Health Organisation Citation2013). Depression alone accounts for 1.8% of all disability adjusted life years (DALYS), an increase of 61.1% compared to 1990 (Vos et al. Citation2020).
Scales, measurements and question sets in this area within the examination programs of the NAKO allow a broad phenotyping of different emotional and cognitive functions important in the mental health assessment of a population. The different instruments used in the standard program were supplemented by those for in-depth phenotyping, e.g. a structured psychiatric interview for major depression, among those participants who received the extended program. In addition, 30,000 of those with the extended examination program also received a whole body MRI, including sequences of the brain.
describes the scales, measurements and question sets applied for the research area of psychiatric diseases in NAKO, shown according to the way of application. In a computer-assisted face-to-face medical interview study nurses assessed lifetime histories of different psychiatric disorders, performed a brief screening for major depression, using a structured psychiatric interview and asked a set of questions on subjective memory complaints. The participants’ self-reports were performed on touch screens and included a number of different scales. Among them were three scales from the Patient Health Questionnaire (PHQ) for depressive and anxiety symptoms as well as perceived stress (Kroenke et al. Citation2001; Citation2003; Spitzer et al. Citation2006). It also included a 15-item questionnaire on the ‘Big-5 Personality’ items (Gerlitz and Schupp Citation2005), the German version of the childhood trauma screener (Grabe et al. Citation2012) as well as question sets on the individual social network and instrumental activities of daily living (IADL). The latter was limited to those aged 60 years and older. The applied neuropsychological test battery included different tests to address the domains of memory and executive functions as well as tests for fine motor movements and attention as well as numerical reasoning. The different instruments, measurements and tests listed in are described in more detail in separate, following manuscripts.
Table 1. Method of administration and components of the examination program in the research area of psychiatric diseases in the German National Cohort (NAKO) baseline examination 2014–2019, according to the standard and extended programs (L1 and L2).
Mood disorders and cognition in the NAKO
In this issue of the World Journal of Biological Psychiatry a series of articles report the different instruments and first findings from the research area of psychiatric diseases and of cognitive function in the GNC. Data base for these papers are the first 101,667 NAKO participants, the so called ‘data freeze 100K’, providing a solid base for a series of first findings.
Streit et al. introduce the different scales and instruments used to assess depressive symptoms and their severity, classify depression and the subtype of major depression and report the associations of the resulting outcomes with anxiety, childhood trauma and stress. They illustrate the overlap and differences between these instruments in the assessment of depressive mood.
Erhardt et al. report on the scales applied to document anxiety and panic attacks in the examination program of GNC and analysed the associations of the two conditions with depression, stress and childhood trauma.
Klinger-König et al. introduce the childhood trauma screener which was used to assess physical or sexual traumatisation or neglect during childhood and adolescence in NAKO participants. They show the strong relations of early trauma with depression and anxiety in their analyses.
Kleineidam et al. introduce to and analyse the neuropsychological test battery used to assess cognitive function in the examination of NAKO participants. They provide closer insights into its associations with sex, age and education.
Schmiedek et al. finally, illustrate the use of a numerical reasoning test to assess fluid intelligence, implemented as a time efficient touch screen module in the L2 examination program. They show relations of this test with age, sex, and education, as well as its association to executive cognitive functions in GNC participants.
Conclusions
Modularly organised phenotyping of emotional and cognitive functions, disorders and subtypes of diseases offer an effective way of classifying common standard and more detailed phenotypes in mental health research. This efficacy is especially important in so-called mega cohorts with repeated examinations conducted in the general population since they allow the assessment of disease incidences also for rare disorders and conditions, as well as the definition of new symptom clusters as risk for disease and the identification of new gene-environment interactions in the onset of disorders. However, basis for all these analyses remains a broad phenotyping in the data collection as illustrated in the first findings from the German National Cohort in this issue.
Statement of interest
None to declare.
Additional information
Funding
References
- Bamberg F, Kauczor H-U, Weckbach S, Schlett CL, Forsting M, Ladd SC, Greiser KH, Weber M-A, Schulz-Menger J, Niendorf T, et al. 2015. Whole-body MR imaging in the german national cohort: rationale, design, and technical background. Radiology. 277(1):206–220.
- Gerlitz J-Y, Schupp J. 2005. Zur Erhebung der Big-Five-basierten Persönlichkeitsmerkmale im SOEP Dokumentation der Instrumentenentwicklung BFI-S auf Basis des SOEP-Pretests. DIW Research Notes. 4. Berlin.
- German National Cohort Consortium. 2014. The German National Cohort: aims, study design and organization. Eur J Epidemiol. 29(5):371–382.
- Grabe H, Schulz A, Schmidt C, Appel K, Driessen M, Wingenfeld K, Barnow S, Spitzer C, John U, Berger K, et al. 2012. Ein Screeninginstrument für Missbrauch und Vernachlässigung in der Kindheit: der Childhood Trauma Screener (CTS). Psychiat Prax. 39(03):109–115.
- Kroenke K, Spitzer RL, Williams JB. 2001. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 16(9):606–613.
- Kroenke K, Spitzer RL, Williams JBW. 2003. The Patient Health Questionnaire-2: validity of a two-item depression screener. Med Care. 41(11):1284–1292.
- Manolio TA, Goodhand P, Ginsburg G. 2020. The international hundred thousand plus cohort consortium: integrating large-scale cohorts to address global scientific challenges. Lancet Digit Health. 2(11):e567–e568.
- Spitzer RL, Kroenke K, Williams JBW, Löwe B. 2006. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 166(10):1092–1097.
- Vos T, Lim SS, Abbafati C, Abbas KM, Abbasi M, Abbasifard M, Abbasi-Kangevari M, Abbastabar H, Abd-Allah F, Abdelalim A, et al. 2020. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 396(10258):1204–1222.
- World Health Organisation, editor. 2013. Mental Health Action Plan 2013–2020. Geneva, Switzerland: WHO Document Production Services.