

ABSTRACT
Objectives: Detectable minimal residual disease (MRD) after therapy for acute lymphoblastic leukemia (ALL) is the strongest predictor of hematologic relapse. This study evaluated outcomes of patients with B-cell precursor ALL with MRD of ≥10−4
Methods: Study population was from ALL study groups in Europe managed in national study protocols 2000–2014. MRD was measured by polymerase chain reaction or flow cytometry. Patients were age ≥15 years at initial ALL diagnosis. Patients were excluded if exposed to blinatumomab within 18 months of baseline or prior alloHSCT.
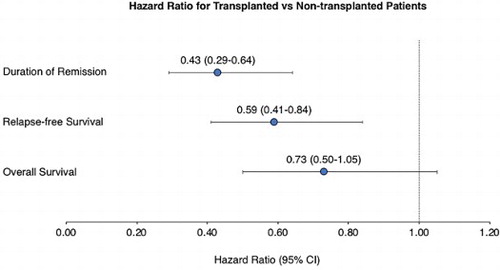
Results: Of 272 patients in CR1, baseline MRD was ≥10−1, 10−2 to <10−1, 10−3 to <10−2, and 10−4 to <10−3 in 15 (6%), 71 (26%), 109 (40%), and 77 (28%) patients, respectively. Median duration of complete remission (DoR) was 18.5 months (95% confidence interval [CI], 11.9–27.2), median relapse-free survival (RFS) was 12.4 months (95% CI, 10.0–19.0) and median overall survival (OS) was 32.5 months (95% CI, 23.6–48.0). Lower baseline MRD level (P ≤ .0003) and white blood cell count <30,000/µL at diagnosis (P ≤ .0053) were strong predictors for better RFS and DoR. Allogeneic hematopoietic stem cell transplantation (alloHSCT) was associated with longer RFS (hazard ratio [HR], 0.59; 95% CI, 0.41–0.84) and DoR (HR, 0.43; 95% CI, 0.29–0.64); the association with OS was not significant (HR, 0.72; 95% CI, 0.50–1.05).
Discussion: In conclusion, RFS, DoR, and OS are relatively short in patients with MRD-positive ALL, particularly at higher MRD levels. AlloHSCT may improve survival but has limitations. Alternative approaches are needed to improve outcomes in MRD-positive ALL.
GRAPHICAL ABSTRACT
Disclosure statement
N.G. has received research funds and honoraria and has served on advisory boards, for Amgen, Pfizer, Celgene and Novartis. H.D. has received honoraria and/or research funding from Amgen, Agios, Seattle Genetics, Celgene, Sunesis, Roche, Pfizer, Ambit-Daiichi Sankyo, Shire-Baxalta, Ariad-Incyte, Karyopharm, Abbvie, Novartis, Kite, Otsuka, Celator-Jazz, Astellas, Menarini, Cellectis, Janssen, ImmunoGen, and Servier. S.G. has served on advisory boards and received honoraria from Amgen. M.B. has served as an advisor for Amgen and Incyte and on speakers’ bureaus for Amgen, Pfizer and Roche, and received research funding from Amgen, Affimed, and Regeneron. R.F. has been on advisory boards and speakers bureaus for Amgen, Pfizer, Janssen, Novartis, AbbVie, Celgene, Sandoz, Celltrion, Roche, Incyte. C.K., M.S., J.M.S, and G.Z. are employees and stockholders of Amgen. G.M. has served as an advisor to Amgen, Ariad/Incyte, Pfizer, Roche, Celgene, Janssen, and Jazz Pharmaceuticals, on speakers’ bureaus for Novartis, Pfizer, and Celgene, and received travel compensation from Daiichi Sankyo, Roche, and Shire. A.R. received support from Amgen, Pfizer, Novartis, and Celgene for travel, sponsored lectures, and advisory board meetings. J.-M.R. has received research funds and honoraria, and served on advisory boards, for Amgen, Pfizer, Shire, and Ariad. R.B. received honoraria for participation in advisory boards for Amgen, Pfizer, Shire, and Incyte. E.P. received support for advisory board meetings from Amgen, Roche and Celgene. M.D., D.H. declare no conflicts of interest.
ORCID
Michael Doubek http://orcid.org/0000-0002-1269-6282
Elena Parovichnikova http://orcid.org/0000-0001-6177-3566
Josep-Maria Ribera http://orcid.org/0000-0003-1042-6024