
ABSTRACT
Purpose:
Vitamin B12 deficiency is a cause of preventable growth and developmental retardation in children. In this respect, alternative methods such as oral and sublingual treatments are being tried. We aimed to compare the efficacy of oral, sublingual, and intramuscular vitamin B12 treatments in children aged 0–3 years.
Methods:
The study included 158 patients with serum vitamin B12 deficiency (serum vitamin B12 level <300 ng/L) aged 0–3 years retrospectively. According to the vitamin B12 treatment modalities, the patients were divided into three groups as oral cyanocobalamin (group 1), sublingual methylcobalamin (group 2), and intramuscular cyanocobalamin (group 3).
Results:
The mean values of vitamin B12 levels increased to above 300 ng/L in all three groups. This increase was statistically significant for Group 1,2 and 3 (p<0.05).
Conclusion:
Sublingual methylcobalamin was determined as effective as oral and intramuscular cyanocobalamin improving vitamin B12 levels aged 0–3 years.
What's already known about this topic?
It is already known that intramuscular and oral cyanocobalamin treatments are effective in vitamin B12 deficiency of children.
What does this article add?
Sublingual methylcobalamin treatment, which is a new treatment method, was found to be as effective as oral and intramuscular cyanocobalamin treatments. To our knowledge, there is no study about sublingual treatment in children and comparing oral cyanocobalamin, intramuscular cyanocobalamin, sublingual methylcobalamin.
Introduction
Vitamin B12 is a vitamin that has an important role in cellular metabolisms like DNA synthesis and other significant events[Citation1]. Vitamin B12 deficiency is the most common cause of childhood megaloblastic anemia and is often nutritional. Clinical manifestations related to vitamin B12 deficiency are seen in children at the first two years of age[Citation2]. Diagnosing and treating vitamin B12 deficiency in childhood protects the child from developing neurological and developmental problems[Citation3].
The standard vitamin B12 treatment that has been known and applied for years is the parenteral vitamin B12 treatment. As a result of the studies in the world and our country over the years, it has been shown that oral vitamin B12 treatment is as effective as intramuscular therapy in adults[Citation4–7]. Intramuscular injections are painful and prone to complications, and at the same time, they need to be applied at the hospital, so recently oral administration is preferred more frequently[Citation4]. Therefore, oral vitamin B12 treatment, which is painless and easily applied is recently been used in children. In some studies, it was shown that oral cyanocobalamin therapy in children as was as effective as intramuscular treatment[Citation8,Citation9]. Although the effectiveness of sublingual therapy in adults has been demonstrated, limited studies are showing the efficacy of sublingual methylcobalamin therapy in children, which is easier to apply than oral cyanocobalamin therapy [Citation10,Citation11].
In our study, it was aimed to retrospectively compare the efficacy of oral, sublingual, and intramuscular vitamin B12 treatments applied to children aged 0–3 years who were admitted to Başkent University hospital with vitamin B12 deficiency.
Material-method
The hospital files of patients that were admitted to Baskent University Ankara Hospital Department of Pediatrics Outpatient Clinics were evaluated retrospectively between January 2017 and August 2020. The patients between 0–3 ages and with vitamin B12 values are <300 ng/L were included in the study. The lower limit of vitamin B12 was accepted as 300 ng/L according to previous literature[Citation8,Citation12]. Age, sex, method of administration of vitamin B12 treatment, hemoglobin, platelet, vitamin B12 values before and after treatment will be evaluated retrospectively. The patients were divided into three groups according to the vitamin B12 treatment modalities.
1- Oral cyanocobalamin therapy group (Group 1)
The children were given 1000 μg ampules of oral cyanocobalamin (Dodex®Deva,) every day for the first week, every other day for 2 weeks, 2 days/week for 2 weeks, followed by once a week for three months.
2- Sublingual Methylcobalamin therapy group (Group 2)
The children were given 1 puff of sublingual methylcobalamin (Ocean methylB12®, Orzax), 1000 μg, every day for the first week, every other day for 2 weeks, 2 days/week for 2 weeks, followed by once a week for three months. This preparation is a food supplement.
3- Intramuscular cyanocobalamin therapy group (Group 3)
The children were given 100 μg (1/10) of 1000 μg ampule intramuscular cyanocobalamin (Dodex®, Deva,) intramuscularly, every day for the first week, every other day for 2 weeks, 2 days/week for 2 weeks, followed by once a week for three months.
The groups were evaluated for the laboratory parameters before and after three types of vitamin B12 therapies.
Statistical method
For descriptive statistics, continuous variables were expressed as mean ± standard deviation, (minimum-maximum), and categorical variables as frequency (n) and percentage (%). Numerical variables were evaluated for normality of data distribution using the Shapiro–Wilk test. Provided that the data has a normal distribution, One-way Analysis of Variance (ANOVA) was used to compare post-treatment vitamin B12, Hb, Plt values of the groups, and Paired t-test was used to compare pre and post-treatment vitamin B12, Hb, Plt values. The level of significance was accepted as p<0.05. Analyses were performed using IBM SPSS version 25.0. The data is available upon request.
Results
In all, 158 children aged between 0–3 ages were included. The mean age of the children included in our study was 12.8 ± 7.2 (1-36) months. 51.9% of the participants were girls and 48.1% were boys. There were 89 (56.3%), 46(29.1%) and 23 (14.6%) children in groups 1,2 and 3 respectively. Female/male ratios of oral cyanocobalamin group, sublingual methylcobalamin group, intramuscular cyanocobalamin groups were 44/45, 25/21, and 13/10. The mean ages of groups 1,2 and 3 were 13 ± 7 (4-33), 13 ± 7 (3-35), and 12 ± 8 (1-33) axes respectively. It was observed that hemoglobin (Hb), platelet count, and vitamin B12 values have measured an average of 80 ± 10 days (69-95) after the initiation of vitamin B12 treatment in children. Hemoglobin (Hb)(g/dl), platelet count (plt)(x109/L), and vitamin B12 (ng/L) levels of children before and after treatment are summarized in and .
Figure 1. Participants’ vitamin B12 values before and after oral cyanocobalamin, intramuscular cyanocobalamin, and sublingual methylcobalamin vitamin B12 treatments. Group 1: Oral cyanocobalamin therapy group, Group 2: Sublingual Methylcobalamin therapy group, Group 3: Intramuscular cyanocobalamin therapy group.
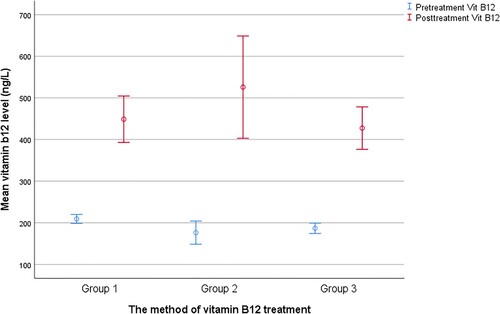
Table 1. Vitamin B12, Hemoglobin And Platelet Levels Before And After Treatment Among Groups.
Vitamin b12 levels
In our study, the efficacy of treatment with oral, intramuscular cyanocobalamin, and sublingual methylcobalamin in children aged 0–3 with vitamin B12 deficiency were compared. After vitamin B12 therapy, serum vitamin B12 levels increased significantly in all patients, and there was a statistically significant difference between the treatment groups (p<005). Pre-treatment vitamin B12 values; 201.1 ± 63.2 ng/L,176.1 ± 64.2 ng/L and 187 ± 49.2 ng/L in groups 1,2 and 3 respectively. Post-treatment vitamin B12 levels; 449.2 ± 285.2 ng/L, 526.1 ± 284.1 ng/L and 427.1 ± 172.1 ng/L in groups 1,2 and 3 respectively.
After oral and intramuscular cyanocobalamin and sublingual methylcobalamin treatments; mean vitamin B12 levels increased to above 300 ng/L. This increase was statistically significant for all three treatment groups (p = 0.007, p <0.001, p <0.001).
Complete blood count parameters
Only twelve participants (%7,2) were found to have anemia (Hb<10 g/dl) before vitamin B12 treatment. After treatment of third-month improvement ratio of oral cyanocobalamin treatment, sublingual methylcobalamin treatment, and intramuscular cyanocobalamin treatment was determined as 3 (%3,4)/85, –/100 and 1(%4,3)/22.
A statistically significant difference was found in Hb values between pre and post-treatment of oral cyanocobalamin treatment of group 1 (p < 0.05). Although we observed an increase in Hb values after intramuscular and sublingual treatment modalities, this increase was not statistically significant (p = 0.150, p = 0.092). The platelet counts examined did not vary either among groups and pre and post-treatment periods (p > 0.05)
Discussion
Vitamin B12 deficiency is common in children and can cause serious problems if left untreated. Therefore, its treatment and follow-up are important. Although intramuscular vitamin B12 treatment is an effective treatment in children, it has disadvantages such as pain at the injection site and the need to be done in a hospital environment[Citation13]. This situation may affect the children's compliance and continuity with the treatment. For this reason, parents prefer oral treatment that is easy to apply and painless in children more often.
In various studies conducted in our country and around the world, it has been shown that oral vitamin B12 treatment is as effective as intramuscular therapies[Citation9,Citation14,Citation15]. On the other hand, many studies have determined that sublingual treatments with sublingual absorption are effective and advantageous[Citation16]. However, there are a limited number of studies regarding oral vitamin B12 treatment in children. In the literature, Bahadır et al. evaluated forty-seven children (1 moth-17 years) with vitamin B12 levels below 200 ng/L were divided into groups according to the children's age and duration of the treatment[Citation9]. Children were categorized as Group 1 (1-20 months), Group 2 (6-17 years), Group 1A&2A (treatment for 4 months duration), and Group 1B&2B (treatment for 8 months duration).
The oral vitamin B12 therapy was administered as 1000 μg oral vitamin B12, every day for the first week, every other day for 2 weeks, 2 days a week for 2 weeks, followed by once a week. Oral vitamin B12 (1000 μg) for 4 months was found to be effective. Sezer et al. assessed 79 children aged 6 months to 18 years with vitamin B12 levels <300 ng/L[Citation8]. In their study children were treated orally with a combination of a multivitamin tablet daily or vitamin B12 ampules. After oral vitamin B12 therapy, the vitamin B12 level increased from 182 ± 47.6 ng/L to 482 ± 318 ng/L.
In our study, the efficacy of oral and intramuscular cyanocobalamin and sublingual methylcobalamin treatment methods in 0–3 years old children with vitamin B12 deficiency were compared. Mean pre-treatment vitamin B12 levels of oral cyanocobalamin, intramuscular cyanocobalamin, and sublingual methylcobalamin groups were found as 201.1 ± 63.2 ng/L, 176.1 ± 64.2 ng/L, 187 ± 49.2 ng/L respectively. After the oral cyanocobalamin, intramuscular cyanocobalamin, and sublingual methylcobalamin treatment the vitamin B12 levels were detected as 449.2 ± 285.2 ng/L, 526.1 ± 284.1 ng/L, 427.1 ± 172.1 ng/L. Our results were consistent with the previous studies in children comparing oral and intramuscular vitamin B12 therapies8. Despite there are studies comparing oral and intramuscular vitamin B12 treatments, few studies are comparing sublingual vitamin B12 treatment with others[Citation11].
The first study that is comparing sublingual therapy with intramuscular and peroral is recently published in children between 5–18 ages[Citation11]. Kartal T et al compared the efficacy of sublingual and intramuscular administration of vitamin B12 in terms of normalizing serum cyanocobalamin levels aged 5–18 years[Citation11]. Pre-treatment mean values of serum cyanocobalamin level were increased from 146.7 ± 40.5 ng/L to 565.5 ± 108.1 ng/L in the sublingual group. In conclusion, sublingual methylcobalamin treatment was observed to correct serum vitamin B12 levels similar to intramuscular and sublingual cyanocobalamin treatment. Our results were found to be consistent with this study. Our study also adds additional information to this one as we evaluated mainly breastfed infants as our study evaluated children between 0–3 years.
In another point of view of comparing methyl versus cyanocobalamin; there are studies reflecting some potential disadvantages of cyanocobalamin. Freeman et al argued that cyanocobalamin should be withdrawn from the market for reasons related to tobacco amblyopia and other optic neuropathies and noted that cyanocobalamin was replaced by hydroxocobalamin in the WHO essential drugs list[Citation17,Citation18]. In another study, it was found that patients with renal failure may have high levels of thiocyanate and cyanide with vitamin B12 therapy[Citation19,Citation20]. Spence et al. reported that the harm from cyanocobalamin among study participants with renal failure obscured the benefit of vitamin B to lower homocysteine levels in stroke prevention[Citation21–24]. For these reasons, methylcobalamin therapy may be preferred to cyanocobalamin therapy in children.
In our study, we showed that sublingual methylcobalamin treatment, which is easy and comfortable to apply, was as effective as intramuscular and oral cyanocobalamin treatments.
Our research will guide other studies in terms of detecting the effectiveness of vitamin B12 treatments in children aged 0–3 years, which is a critical window period in terms of growth and development.
Conclusion
This study determined the effectiveness of sublingual methylcobalamin treatment in children aged 0–3 years. Treatment of vitamin B12 deficiency is important in children 0–3 aged, which is a critical period for growth and development. Because of the disadvantages of intramuscular vitamin B12 therapy, treatment may not be completed or applied regularly. Sublingual vitamin B12 therapy is effective, easy to apply, and painless. In this respect, our research will guide further research.
Limitations of our study
Our study has several limitations. Since our study was retrospective, methylmalonic acid and homocysteine levels of the patients were not measured. We have compared the treatment results of two drugs and one food supplement (sunlingual methylcobalamin) for the efficacy in increasing post-treatment vitamin B12 levels, at least some of the babies may have swallowed the sublingual methylcobalamin which was uncontrollable. However, we still think our study results are adding some data regarding our experience as the sublingual drug is widely used in routine pediatric practice in Turkey. Another limitation is the retrospective design of our study and we think that further randomized and controlled studies with a high number of subjects comparing these drugs in terms of efficacy and developmental/neurocognitive outcomes of treatment modalities Despite these limitations, we think that we think that our study is valuable as it has shown that sublingual vitamin B12 administration is as effective as oral and intramuscular cyanocobalamine treatment.
Declaration
Ethics declarations
Ethical approval
This study was approved by the Baskent University Medical and Health Sciences Research Committee (Project number: KA20/385).
Consent to participate
The participant has consented to the submission to this journal.
Consent for publication
The participant has consented to the submission to this journal.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Availability of data and material
Raw data are available upon reasonable request (correspondence author).
Additional information
Funding
References
- Tefferi A, Pruthi RK. The biochemical basis of cobalamin deficiency. Mayo Clin Proc. 1994;69(2):181–186.
- Roschitz B, Plecko B, Huemer M, et al. Nutritional infantile vitamin B12 deficiency: pathobiochemical considerations in seven patients. Arch Dis Child Fetal Neonatal Ed. 2005;90:281–282.
- Brocadello F, Levedianos G, Piccione F, et al. Irreversible subacute sclerotic combined degeneration of the spinal cord in a vegan subject. Nutrition. 2007;23:622–624.
- Nyholm E, Turpin P, Swain D, et al. Oral vitamin B12 can change our practice. Postgrad Med J. 2003;79:218–219.
- Chan CQH, Low LL, Lee KH. Oral vitamin B12 Replacement for the treatment of pernicious anemia. Front. Med. 2016;3:38.
- Andres E, Zulfiqar AA, Serraj K, et al. Systematic review and pragmatic Clinical approach to oral and nasal vitamin B12 (cobalamin) treatment in patients with vitamin B12 deficiency related to gastrointestinal disorders. J. Clin. Med. 2018;7:304.
- Boran M, Boran Ö, Yılmaz N, et al. Vitamin B12 replasman tedavisi; oral? İntramüsküler? Harran Üniversitesi Tıp Fakültesi Dergisi (Journal of Harran University Medical Faculty). 2020;17(1):19–23. DOI: https://doi.org/10.35440/hutfd.628409.
- Sezer RG, Bozaykut A, Akoğlu HA, et al. The efficacy of oral vitamin B12 Replacement for nutritional vitamin B12 deficiency. J Pediatr Hematol Oncol. 2018 Mar;40(2):e69–e72.
- Bahadir A, Reis PR, Erduran E. Oral vitamin B12 treatment is effective for children with nutritional vitamin B12 deficiency. J Paediatr Child Health. 2014;50:721–725.
- Thakkar K, Billa G. Treatment of vitamin B12 deficiency-methylcobalamine? cyancobalamine? hydroxocobalamin?-clearing the confusion. Eur J Clin Nutr. 2015 Jan;69(1):1–2. doi:https://doi.org/10.1038/ejcn.2014.165. Epub 2014 Aug 13. PMID: 25117994.
- Tuğba-Kartal A, Çağla-Mutlu Z. Comparison of sublingual and intramuscular administration of vitamin B12 for the treatment of vitamin B12 deficiency in children. Rev Invest Clin. 2020 Dec;72(6):380–385.
- Means RT, Fairfield KM. Clinical manifestations and diagnosis of vitamin B12 and folate deficiency. Uptodate. April-2021. Erişim adresi: https://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-vitamin-b12-and-folate- deficiency?search = vitamin%20b12%20deficiency&source = search _result&selected. Erişim tarihi: 20/05/2021.
- Graham ID, Jette N, Tetroe J, et al. Oral cobalamin remains medicine's best kept secret. Arch Gerontol Geriatr. 2007 Jan-Feb;44(1):49–59.
- Chandelia S, Chandra J, Narayan S, et al. Addition of cobalamin to iron and folic acid improves hemoglobin rise in nutritional anemia. Indian J Pediatr. 2012;79:1592–1596.
- Verma D, Chandra J, Kumar P, et al. Efficacy of oral methylcobalamin in treatment of vitamin B12 deficiency anemia in children. Pediatr Blood Cancer. 2017;64.
- Parry-Strong A, Langdana F, Haeusler S, et al. Sublingual vitamin B12 compared to intramuscular injection in patients with type 2 diabetes treated with metformin: a randomised trial. N Z Med J. 2016 Jun 10;129(1436):67–75.
- Freeman AG. Cyanocobalamin–a case for withdrawal: discussion paper. J R Soc Med. 1992;85:686–687.
- Freeman AG. Hydroxocobalamin versus cyanocobalamin. J R Soc Med. 1996;89:659.
- Koyama K, Yoshida A, Takeda A, et al. Abnormal cyanide metabolism in uraemic patients. Nephrol Dial Transplant. 1997;12:1622–1628.
- Hasuike Y, Nakanishi T, Moriguchi R, et al. Accumulation of cyanide and thiocyanate in haemodialysis patients. Nephrol Dial Transplant. 2004;19:1474–1479.
- Spence JD, Yi Q, Hankey GJ. B vitamins in stroke prevention: time to reconsider. Lancet Neurol. 2017;16:750–760.
- Spence JD, Bang H, Chambless LE, et al. Vitamin intervention for stroke prevention trial: an efficacy analysis. Stroke. 2005;36:2404–2409.
- House AA, Eliasziw M, Cattran DC, et al. Effect of B-vitamin therapy on progression of diabetic nephropathy: a randomized controlled trial. JAMA. 2010;303:1603–1609.
- Spence JD, Eliasziw M, House AA. B-Vitamin therapy for diabetic nephropathy: reply. JAMA. 2010;304:636–637.