
ABSTRACT
Background and Objectives
Haemophilia comprises a continuum of blood disorders that often include joint and muscular dysfunction, which may lead to a constellation of activity limitations and participation restrictions. However, there is scant research incorporating functional assessment scales into the common language provided by the International Classification of Functioning, Disability and Health (ICF). This study aims to identify the ICF categories to include in an item bank of functioning aspects relevant for haemophilia.
Design and Methods
A systematic search was carried out in July 2021 based on the PubMed MEDLINE, CLINICAL, and Cochrane databases for qualified articles, investigating haemophilia-specific scales and the scales recommended by the World Federation of Haemophilia (WFH) linked to ICF categories between 2001 and 2021. Well-trained healthcare professionals in the haemophilia field and ICF evaluation conducted group discussions to determine the ICF items for haemophilia.
Results
A total of 112 out of 176 items measuring function were collected for the haemophilia ICF item bank, including 32 items for body function (b), 45 items for activity and participation (d), 27 items for environmental factors (e), and 8 items for body structure(s).
Interpretation and Conclusions
We recommend that future haemophilia research use the haemophilia-specific ICF item bank, which could capture a whole spectrum of functional measurements and facilitate multidisciplinary and worldwide communication. This study also indicates that further development and analysis of the psychometric properties of the 112 haemophilia-related ICF items is warranted.
Introduction
Haemophilia is a congenital bleeding disorder in which the person is deficient in clotting factor VIII or factor IX and is categorized into haemophilia A and B accordingly. The clinical hallmark of haemophilia is recurrent spontaneous bleeding episodes, as well as cumulative joint and muscle damage. Persons with haemophilia (PWH) experience intra-articular and intramuscular bleeding, which can enormously affect their quality of life [Citation1,Citation2]. Effective management of multisystemic bleeding in PWH necessitates the collaboration of a multidisciplinary team and the utilization of outcome measures that are easily understood by healthcare professionals. Furthermore, the cost associated with the administration of expensive clotting factor therapy to PWH places a significant financial burden on society; thus, the optimization of resource allocation based on outcomes becomes imperative [Citation3]. In light of these considerations, the development of standardized outcome assessments is crucial for patients, physicians and Medicare payers.
With advancements in the treatment of bleeding symptoms, PWH can medicate their spontaneous bleeding with sufficient coagulation factor replacement therapy (CFRT). In a period of improvement in clinical efficacy, Manco-Johnson et al. [Citation4] expounded that annual bleeding rates (ABRs) might not capture the full spectrum of haemophilia-related impairments. PWH have to overcome obstacles and live with disabilities of this lifelong chronic health condition. Thus, periodically and comprehensively evaluating how people live with haemophilia using clinical measures becomes fundamental for the healthcare system.
Although clinical measures have added days to the lives of PWH in the past few decades, more attention has been paid to developing patient-related outcome measures (PROMs) regarding well-being and functioning [Citation5]. Several disease-specific and age-appropriate PROMs have been constructed for children and adolescents with haemophilia focusing on health-related quality of life [Citation6,Citation7]. For example, the original version of the haemophilia-specific health-related quality-of-life questionnaire (Haemo-QoL) can measure quality of life from multidimensional aspects, but this prolonged evaluation will have a negative effect on response rate and data quality [Citation8]. Other haemophilia-specific assessment tools, such as the Haemophilia Joint Health Score (HJHS), World Federation of Hemophilia (WFH) physical examination score or Gilbert score, require strict professional training, which undoubtedly raises barriers for practitioners in low-income countries [Citation9,Citation10].Haemo-QoL-A and Haemophilia Activities List (HAL) developed in different countries might result in a lack of application accuracy in the context of different socioeconomic, cultural, and custom-related backgrounds [Citation11,Citation12]. Furthermore, haemophilia has been associated with many medical conditions, such as diabetes, hypertension, hepatitis, and acquired immunodeficiency syndrome [Citation8,Citation13]. All of these clinical issues related to haemophilia rather than specific to the disease should be considered to provide a more comprehensive picture of the functional limitations in PWH. Therefore, ‘haemophilia-specific outcomes’ should be addressed as ‘haemophilia-related outcomes’. Consequently, although numerous haemophilia-specific outcome measure scales are available, they still pose a major challenge to multidisciplinary communication and clinical practice in healthcare systems. The WFH has recommended adherence to the International Classification of Functioning, Disability and Health (ICF) model put forth by the World Health Organization (WHO) to facilitate a comprehensive evaluation of all ramifications associated with the disorder and promote interdisciplinary collaboration [Citation14].
The ICF framework
In 2001, the ICF was a theoretical framework and classification system promulgated by the WHO to describe human experiences regarding health and health-related conditions. It allows the medical world to exchange information concerning health and well-being using the same terminology and definitions. Standardized terminology could reduce misunderstanding and ambiguity and improve communication efficiency. To date, ICF has provided more than 1,400 categories for this purpose, which are used to comprehensively measure human functioning in four categories across body function (b), body structure (s), activity and participation (d), environment, and individual factors (e). Within each of these four components, the ICF is structured hierarchically, with each component consisting of domains (chapters in ICF). Each domain then consists of second-level categories, which in turn consist of third-level categories, and so on. The domain represents the broadest level, with the third-level category being the more fine-grained functional aspects underneath the second-level category. For example, there are the following items in the Activities and Participation classification:
· d5 Self-care (domain/chapter)
· d510 Washing oneself (2nd-level category)
· d5101 Washing whole body (3rd-level category)
The ICF core set is a combination of ICF items that are formulated for a specific disease or health state and more comprehensively reflect the function and health state of a specific population. It can be divided into two versions of core sets: the comprehensive version and the brief version. The comprehensive version of the ICF core set embodies a broad and detailed description of the functionality of specific health conditions. The brief ICF core set is derived from a comprehensive ICF core set, which facilitates an effective description of specific disease functional status. Currently, there is no ICF core set for evaluating PWH. Although ICF is promising in the functional evaluation of PWH [Citation5,Citation20], scant literature has provided a summary of haemophilia-related ICF categories.
Owing to these knowledge gaps, current haemophilia-specific assessment scales might not provide clinicians with a comprehensive picture of functioning performance in PWH. Moreover, due to the applicable population, sensitivity, reliability, and cultural differences of different scales [Citation21,Citation22], it is not appropriate to compare and communicate using different scales. The purpose of this review is to identify a functioning category bank relevant to haemophilia.
Methods
There were two stages for identifying the haemophilia-related ICF items:
Stage 1. Sorting out haemophilia outcome measures using the ICF linking rules
First, items from the ICF core sets were selected. PWH have joint degeneration, muscle bleeding, and other functional limitations similar to osteoarthritis and musculoskeletal injuries. In addition, several generic ICF core sets may reflect the functional limitations of PWH in general. Based on this functional characteristic of haemophilia, the ICF core sets were selected by medical personnel who specialize in haemophilia and are trained in applying ICF.
Next, ICF items linked to haemophilia-related PROMs or HRQoL with ‘Linking rules’ were identified. The ‘Linking rules’ are a set of rules to link information from questionnaires and clinical examinations to ICF categories to filter or estimate the ICF category. Researchers have linked the ICF category to items in the WFH-recommended haemophilia specificity scale (HJHS, Functional Independence Score in Hemophilia/FISH, HAL) and the the EuroQol-5 Dimension (EQ-5D) and the Short form 36 health survey questionnaire (SF-36). These scales have been validated in the functional measurement of haemophilia and have been widely used in clinical studies. We conducted a systematic literature review following the PRISMA guidelines. The full text of the retrieved publications was screened, and the ICF categories linked to the scales were included in the item bank.
Search strategy
A comprehensive literature search performed in the PubMed, MEDLINE, CLINICAL, and Cochrane databases (articles published between January 2001 and May 2020) was conducted by two independent researchers. We also browsed the database back to 1946 to avoid missed case reports. The keywords used were [(haemophilia OR hemophilia) AND (outcome measures) AND (International Classification of Functioning, Disability and Health, OR ICF)], [(haemophilia OR hemophilia) AND (International Classification of Functioning, Disability and Health, OR ICF)], [(Haemophilia Joint Health Score, OR HJHS) AND (International Classification of Functioning, Disability and Health OR ICF)], [(The Functional Independence Score in Hemophilia) AND (International Classification of Functioning, Disability and Health, OR ICF)], [(SF-36) AND (International Classification of Functioning, Disability and Health, OR ICF)], [(EQ-5D) AND (International Classification of Functioning, Disability and Health, OR ICF)] and [(Haemophilia Activities List) AND (International Classification of Functioning, Disability and Health, OR ICF)]. The reference lists of the resulting articles were scanned to identify further relevant studies.
Eligibility criteria
The inclusion and exclusion criteria for studies were as follows:
Study design: There were no strict study design requirements in this review. Reviews regarding the haemophilia-related outcome measures and cross-sectional studies linked to ICF categories were considered. Conference abstracts without the full text and unpublished studies were excluded.
Participant characteristics: Patients diagnosed with haemophilia irrespective of sex and age were included.
Outcome measures: The outcomes include ICF items on body structure (s), body function (b), activity and participation (d), and environmental factors (e), which link to the categories in haemophilia-specific outcome measure scales or other scales recommended by the WFH. The full text of the retrieved publications was screened, and the ICF categories linked to the scales were included in the item bank whenever they appeared once.
Study selection
All literature found in the databases and reference lists was reviewed according to the eligibility criteria by two independent researchers. Initially, titles and abstracts were screened to determine the eligibility of studies. All eligible studies’ full text was assessed to determine whether they met the inclusion criteria. Any disagreements or discrepancies between the two reviewers were resolved via face-to-face discussion or Zoom meeting. When a general consensus could not be achieved, a third independent reviewer participated in the discussion to address conflicts.
ICF item collection
Items were extracted and collected by one author according to the following criteria: PubMed unique identifier, title, first author, publication year, journal, DOI, outcome measure scales, and the number of each ICF component. Another author further confirmed all of the information. summarizes the sources of ICF categories and the number of each category, together with its original manuscript.
Table 1. Source of ICF categories.
Stage 2. Constructing the candidate haemophilia-related ICF core set
A haemophilia-related ICF item bank was constructed according to the following three steps.
First, we removed 15 ‘unspecified’ ICF categories at the second or third level. ‘Unspecified’ are categories that allow for coding of functioning information that belong to a specific overarching domain of the ICF but lack sufficient detail to be able to link with a specific category. Their definitions are unclear to investigators.
Second, the haemophilia item bank is expected to be applicable to all age groups. ICF-CY is the ICF version for children and youth, therefore, items only existing in the ICF-CY were omitted involving ‘d161 Directing attention’, ‘d835 School life and related activities’, and ‘d880 Engagement in play’.
Finally, BF.G., C.F., and F.L., who have been trained in applying ICF, discussed whether the ICF categories should be reserved for the item bank. The consensus on the final ICF categories was achieved among the 3 health professionals (a chief physician, a therapist manager, and a therapist who specialized in haemophilia rehabilitation).
The selection of items met the following criteria:
If there were multiple corresponding 3rd-level categories under the 2nd-level category and these 3rd-level categories were not able to represent the full meaning of the 2nd-level category, only 2nd-level categories were retained to have a more encompassing category.
If there was only one 3rd-level category under the corresponding 2nd-level category, the 2nd-level categories with a more general concept were adopted.
If a collection of several 3rd-level categories represented a comprehensive concept of a specific 2nd-level category, the 3rd-level categories will remained and the specific 2nd-level item was removed.
Results
Study selection
A total of 127 manuscripts were found in the databases. After removing 23 duplicate articles and 88 studies after title and abstract review, the remaining 16 articles were screened in detail by two authors. Haemophilia studies without an ICF linking process or linking ICF items were excluded. A total of 5 articles were retained for analysis. The flowchart of article screening is provided in . Moreover, illustrates a summary of haemophilia-related outcome measures in the concept of the ICF framework.
Figure 1. Flowchart of screening the eligible articles.
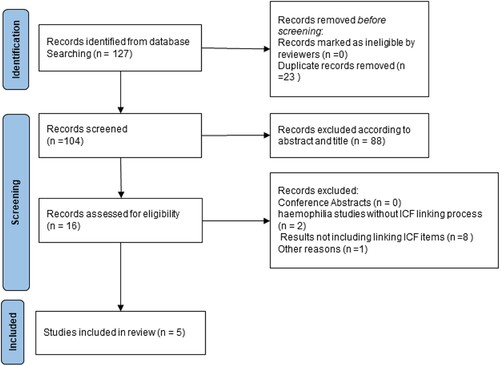
Table 2. ICF-based Haemophilia Outcome Measures.
Stage 1. Sorting out haemophilia outcome measures using the ICF linking rules
Haemophilia-related ICF items were defined in the following three components involving 6 existing ICF core sets, 3 studies regarding haemophilia-specific ICF categories, and 2 studies about ICF categories linked to scales recommended by the WFH.
Existing ICF core set
Haemophilic arthropathy is considered a degenerative joint disease secondary to joint bleeding, characterized by synovial hypertrophy, cartilage, and bone destruction [Citation35]. Pathologically, haemophilic arthritis is similar to osteoarthritis (OA) and rheumatoid arthritis (RA) [Citation36–38]. Furthermore, de Kleijn et al. [Citation39] established a preliminary core set of clinical assessment tools for evaluating the functional status of adults with haemophilia based on a literature search of OA and RA studies. Due to prominent orthopaedic disorders and chronic health status in PWH, ICF items from the OA comprehensive ICF core set [Citation23], ICF generic-7 set [Citation24], rehabilitation set [Citation25], minimal generic set of environmental factors [Citation25], ICF core sets for RA [Citation26], and musculoskeletal post-acute comprehensive ICF core set [Citation27] were considered for the item bank. A total of 270 ICF categories were collected from 6 ICF core sets.
ICF items linked to categories in the haemophilia-related PROMs
Second, we collected 71 ICF categories that corresponded to items in the haemophilia-related PROMs via the ICF linking rules from three sources in which the PROMs were identified among the 5 publications that were included in the review [Citation5,Citation20,Citation28]. According to the linking rules, Riva et al. [Citation5] compared ICF categories with haemophilia-specific PROMs that can be categorized into three different groups: HRQoL, treatment satisfaction (TS), and level of functioning (FUN). The disease-specific HRQoL questionnaire consisted of the Haemo-QoL, Madtap, and Haem-A-QoL. The Hemophilia Patient Satisfaction Scale (Hemo-Sat) was selected to quantify TS. HAL and Haemophilia & Exercise Project Test Questionnaire (HEP-Test-Q) were chosen to manifest the FUN. Content comparisons of PROM were completed based on the ICF and the ICF for children and youth version (ICF-CY). The haemophilia-related ICF items were extracted from these three groups of PROMs. Finally, we extracted 70 ICF items for haemophilia comprising 8 domains and 62 items on the second or above level.
Haemo-QoL, as a disease-specific questionnaire, has three age-related versions. The 4 – to 7-year-old version contains 21 items in 8 domains, the 8- to 12-year-old version has 64 items in 10 domains, and the 13- to 16-year-old version involves 77 items in 12 domains. Responses to the 4- to 7-year-old version of the Haemo-QoL are measured on a 3-point Likert scale, while the other two versions are measured on 5-point Likert scales in line with ICF response options. Given the consistency with the ICF generic qualifier scale, Krasuska et al. [Citation28] adopted two versions of the Haemo-QoL for 8- to 12-year-olds and 13- to 16-year-olds to perform item linking. In this linkage process, these two disease-specific questionnaires were linked to the ICF or the ICF-CY. Five ICF categories were chosen for evaluating children and adolescents with haemophilia.
In addition, De la Corte-Rodriguez and Rodriguez-Merchan [Citation20] completed a narrative review of the ICF categories in the context of haemophilia. They incorporated 7 ICF categories into their clinical assessments regarding one mild haemophilic case and one severe case. All mentioned items were collected for further determination.
ICF items linked to categories in the other HRQoL scales
We screened other HRQoL scales linked to ICF in haemophilia. This study solely considered SF-36 and EQ-5D recommended by the WFH [Citation40]. Cieza & Stucki [Citation19] incorporated six HRQoL scales, including QL-I, WHOQOL-BREF, WHODASII, NHP, EQ-5D, and SF-36 into ICF categories in the context of haemophilia. They identified 13 ICF categories and 21 ICF categories at the second level or above associated with the EQ-5D and SF-36, respectively. Twenty-eight ICF categories were ultimately confirmed after the removal of replicated categories. The degree of agreement was calculated by kappa statistics. Kappa statistics demonstrated high consistency of interexpert classification agreement depending on the ten linking rules (kappa = 0.82∼0.98).
Bernardelli et al. [Citation16] linked the Visual Analogue Scale to the ICF category, including ‘b280 Sensation of pain’ and its associated categories on the third and fourth levels. They also associated the SF-36 with 22 ICF categories. A total of 23 ICF items demonstrated high consistency of interexpert linking agreement results (kappa = 0.93).
After removing the duplicated ICF items, for our review, 176 ICF categories were collected from 11 sources ().
Table 3. Mapping of outcome measure themes to ICF category codes.
Stage 2. Constructing the candidate haemophilia-related ICF core set
Following the three criteria mentioned above, 46 ICF projects were eliminated. As a result, 112 ICF items were identified, as shown in .
Due to a more generalized conception of ‘d410 Changing basic body position’, its subordinate categories were deleted, including ‘d4101 Squatting’, ‘d4102 Kneeling’, and ‘d4105 Bending’. We also removed the 3rd-level categories of the following 2nd-level items: ‘b140 Attention functions’, ‘b280 Sensation of Pain’, ‘b710 Mobility of joint functions’, ‘d455 Moving around’, ‘d640 Doing housework’, ‘d750 Informal social relationships’, ‘d920 Recreation and leisure’, ‘s730 Structure of upper extremity’, ‘s750 Structure of lower extremity’, and ‘s760 Structure of trunk’.
The following 2nd-level categories were included: ‘b130 Energy and drive functions’, ‘b180 Experience of self and time functions’, ‘b430 Haematological system functions’, ‘b455 Exercise tolerance functions’, ‘b780 Sensations related to muscles and movement functions’, ‘d510 Washing oneself’, ‘d570 Looking after one’s health’, ‘e120 Products and technology for personal indoor and outdoor mobility and transportation’, ‘e580 Health services, systems and policies’, and ‘s770 Additional musculoskeletal structures related to movement’. The ‘e1101 Drug’ was considered an exception and was the most frequent item in previous ICF studies of haemophilia.
We adopted ‘d4300 Lifting’ and ‘d4302 Carrying in the arms’ as separate functioning items, rather than ‘d430 Lifting and carrying objects’. Similarly, ‘d4500 Walking short distances’, ‘d4501 Walking long distances’, and ‘d4502 Walking on different surfaces’ were accepted due to containing more details than ‘d450 Walking’.
Table 4. Haemophilia-related ICF Comprehensive Core Set.
Discussion
Previous efforts have been concentrated on reducing mortality and expanding life expectancy for patients with haemophilia. With the advent of major advances in haemophilic treatment, issues regarding potential long-term complications in PWH are starting to emerge. Haemophilia-related impairments impact not only body structure but also levels of activity and participation. Accordingly, a comprehensive and international framework is required for patient-oriented outcome measures and rehabilitation interventions. ICF, as an international common language of functioning, has the potential to unite outcome measures that allow comparability and pooling of results nationally and internationally. This review performed a systematic search regarding the outcome measures in haemophilia activity and participation. The purpose of this study summarized haemophilia-related ICF categories in previous original studies to generate a common functional language for clinical application in future haemophilia studies to allow functional comparisons of PWH across all ages, all settings, and all cultures.
A valid assessment of function is crucial to managing haemophilia-related functional deficits and informing decision-making that could impact individual rehabilitation progress. To promote and provide long-term health assessment and rehabilitation in haemophilia, all aspects of health that influence life experience, including joint impairments, functional limitations, and participation restrictions, should be assessed. Researchers have developed evaluation tools for ‘body scores’, such as the HJHS, Gilbert score, and active range of motion (AROM) [Citation21]. ‘Functional scores’ could be represented by FISH and HAL. The Haemo-QOL-A is designed for quality-of-life measures. Nonspecific assessment tools for haemophilia, such as the SF-36 and EQ-5D, are also applied in haemophilia. Considering the low prevalence of haemophilia, such haemophilia-related instruments should also be cross-culturally applicable to validation studies. Moreover, haemophilia is an underlying medical condition that should be measured considering numerous other possible diseases over the life course. Therefore, a new strategy for standardization and validation is needed.
Body function and body structure
In general, there are item differences in age-specific haemophilia questionnaires, such as the Haemo-QoL and the Haemo-QoL-A. Haemo-QoL covers ‘school’ and ‘recreation and leisure’ instead of ‘haemophilia treatment’, as used in the Haemo-QoL-A. However, Riva et al. [Citation5] also mentioned that the most frequently used categories were ‘b152 Emotional functions’ and ‘e1101 Drugs’, which were mainly found in adults and children, respectively.
During the literature review, we found that ‘b152 Emotional functions’ and ‘b280 Sensation of pain’ have the highest frequency among all ICF categories in 9 out of 11 counts across all studies.
The HJHS is a widely used instrument for physical function in haemophilia and consists of 8 items and a global gait score. It takes approximately 20-40 minutes for a skilled therapist to perform a complete assessment; however, the results do not include ‘b152 Emotional functions’. This means that this important item may be overlooked when assessing a patient's body function. Finding other tools to assess a patient's emotional functioning may take more time, which is clinically unfriendly.
Activity and participation
Considering activity and participation, ‘d230 Carrying out daily routine’, ‘d450 Walking’, and ‘d850 Remunerative employment’ have the highest frequency among the activity and participation components, which are mentioned in 7 out of 9 articles.
WFH recommends the use of HAL for the assessment of patient activity and participation, which includes seven domains but is also missing in the areas of ‘d850 Remunerative employment’, ‘d310 Communicating with - receiving - spoken messages’, etc.
Environmental and personal factors
An environmental factor could be a facilitator or barrier to individual functioning. ‘e320 Friend’ had the highest frequency among categories in the environmental factors. The only environmental factor at the fourth level was ‘e1101 Drugs’. In terms of the environment, there are currently no assessment tools specific to haemophilia. However, in the case of PWH, clotting factors ‘e1101 Drugs’, ‘e570 Social security services, systems and policies’, and ‘e450 Individual attitudes of health professionals’ are all integral assessment aspects.
Comparison with other studies
Although a number of ICF-based instruments have been developed to assess functional outcomes in haemophilia, the measurement error, responsiveness, interpretability and cross-cultural validity of these instruments remain to be further tested [Citation22]. Riva et al. outlined the Patient-rated Outcomes (PROs) instruments for haemophilia and compared them with the ICF to provide assistance in selecting the appropriate instrument in the clinic [Citation5]. Fisher et al. evaluated the reliability and validity of an outcome tool for haemophilia in different patient groups, but a core set of ‘outcome measures’ remains to be defined [Citation21]. PROMIS item banks have been developed for many patient-related outcomes and have been validated in patient and healthy populations. Benefiting from the use of item response theory, any number of items from the item bank can be selected to generate a short table whose scores can be compared with any other item in the same item bank. However, the PROMIS item bank has not been formally validated for use in haemophilia populations, and in clinical use, the PROMIS still needs to be combined with haemophilia-specific scales [Citation41]. Overall, the use of an item bank describes the patient's health experiences, offers appropriate functional items as rehabilitation targets, outlines the resources required to improve specific aspects of human functioning, and reflects changes in functional status after the intervention. The utilization of ICF enhances common understanding and communication among team members in multidisciplinary collaboration. The ICF also provides us with a more comprehensive assessment perspective for haemophilia.
Study limitations
Our search strategy was designed to look for haemophilia-specific outcome measure studies involving functional impairment and HRQoL. It might not fully reflect other aspects of outcome measures. For example, there are several walking-related items in the item bank, but there are no categories that reflect the impact of gait abnormalities on patients’ mental states, such as self-efficacy or self-confidence.
Furthermore, due to a lack of sufficient haemophilia studies, we did not set eligibility criteria for linking rules used in the previous studies.
As the goal of generating nonage-specific applicable haemophilia ICF items, we only included the overlapping ICF and ICF-CY items in the final scale. The haemophilia core set of 112 ICF items is an age-generic measure designed for use in extensive clinical studies and for comparing data across ages, but it is not an age-specific instrument. Finally, although the activities and participation categories in this report were utilized for item response modeling in our recent paper [Citation42], the psychometric characteristics of the full set of 112 categories remained unexplored.
Conclusion
Based on a thorough literature search and professional linking work, this review identified ICF categories linked to the content of available instruments in PWH. The 112 reported categories were proposed to initially develop a comprehensive haemophilia ICF core set. Further testing on psychometric properties such as validity, reliability, and item difficulties needs to be undertaken to confirm clinically friendly and valid haemophilia-related ICF-based outcome measures.
Author contributions
F.L., SG.L. and ZL.J. conceived the original research idea. BF.G., C.F., and F.L. designed and performed the literature review and wrote the manuscript. All authors discussed the conclusions and commented on the manuscript.
Article summary
This systematic review aims to identify the International Classification of Functioning, Disability and Health (ICF) categories that are linked to outcome measures for the care of persons with haemophilia (PWH).
The haemophilia-specific ICF core set, consisting of 112 categories, was developed as a common language to measure functioning in PWH.
Data sharing statement
The datasets presented in this article are readily available. Requests to access the datasets should be directed to the corresponding author.
Acknowledgments
We would like to thank Amanda Ferland, Doctor of Physical Therapy for helping with our proofreading, and contributing valuable criticisms to the final version of the manuscript.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Mahlangu J, Oldenburg J, Callaghan MU, et al. Health-related quality of life and health status in persons with haemophilia A with inhibitors: a prospective, multicentre, non-interventional study (NIS). Haemophilia. 2019;25(3):382–391.
- Oldenburg J, Tran H, Peyvandi F, et al. Health-related quality of life and health status in adolescent and adult people with haemophilia A without factor VIII inhibitors—A non-interventional study. Haemophilia. 2021;27(3):398–407.
- Fischer K, Steen Carlsson K, Petrini P, et al. Intermediate-dose versus high-dose prophylaxis for severe hemophilia: comparing outcome and costs since the 1970s. Blood. 2013;122(7):1129–1136.
- Manco-Johnson MJ, Warren BB, Buckner TW, et al. Outcome measures in haemophilia: beyond ABR (annualized bleeding rate). Haemophilia. 2021;27(S3):87–95.
- Riva S, Bullinger M, Amann E, et al. Content comparison of haemophilia specific patient-rated outcome measures with the international classification of functioning, disability and health (ICF, ICF-CY). Health Qual Life Outcomes. 2010;8(1):139.
- Pollak E, Mühlan H, VON Mackensen S, et al. The haemo-Qol index: developing a short measure for health-related quality of life assessment in children and adolescents with haemophilia. Haemoph Off J World Fed Hemoph. 2006;12(4):384–392.
- Von Mackensen S, Bullinger M, Group H-Q. Development and testing of an instrument to assess the quality of life of children with haemophilia in Europe (haemo-QoL). Haemophilia. 2004;10(s1):17–25.
- Pandey B, Barnes RFW, Sun HL, et al. Risk of diabetes in haemophilia patients compared to clinic and non-clinic control cohorts. Haemoph Off J World Fed Hemoph. 2022;28(3):445–452.
- St-Louis J, Abad A, Funk S, et al. The hemophilia joint health score version 2.1 validation in adult patients study: a multicenter international study. Res Pract Thromb Haemost. 2022;6(2):e12690.
- Gilbert MS. Prophylaxis: musculoskeletal evaluation. Semin Hematol. 1993;30(3 Suppl 2):3–6.
- Rentz A, Flood E, Altisent C, et al. Cross-cultural development and psychometric evaluation of a patient-reported health-related quality of life questionnaire for adults with haemophilia. Haemoph Off J World Fed Hemoph. 2008;14(5):1023–1034.
- van Genderen FR, Westers P, Heijnen L, et al. Measuring patients’ perceptions on their functional abilities: validation of the Haemophilia Activities List. Haemoph Off J World Fed Hemoph. 2006;12(1):36–46.
- Lövdahl S, Henriksson KM, Baghaei F, et al. Hypertension and cardiovascular diseases in Swedish persons with haemophilia - A longitudinal registry study. Thromb Res. 2019;181:106–111.
- International Classification of Functioning, Disability and Health (ICF). https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health (accessed December 21, 2022).
- Cieza A, Fayed N, Bickenbach J, et al. Refinements of the ICF linking rules to strengthen their potential for establishing comparability of health information. Disabil Rehabil. 2019;41(5):574–583.
- Bernardelli RS, Santos BC, Scharan KO, et al. Application of the refinements of ICF linking rules to the Visual Analogue Scale, Roland Morris questionnaire and SF-36. Cienc Saude Coletiva. 2021;26(3):1137–1152.
- Fréz AR, Abdallah AA, Riedi C, et al. Proposed Use of the international classification of functioning, disability and health to evaluate quality of life after an amputation. Fisioter Em Mov. 2014;27(1):49–56.
- Prodinger B, Cieza A, Williams DA, et al. Measuring health in patients with fibromyalgia: content comparison of questionnaires based on the international classification of functioning, disability and health. Arthritis Rheum. 2008;59(5):650–658.
- Cieza A, Stucki G. Content comparison of health-related quality of life (HRQOL) instruments based on the international classification of functioning, disability and health (ICF). Qual Life Res. 2005;14(5):1225–1237.
- De la Corte-Rodriguez H, Rodriguez-Merchan EC. The ICF (International Classification of Functioning, Disability and Health) developed by the WHO for measuring function in hemophilia. Expert Rev Hematol. 2016;9(7):661–668.
- Fischer K, Poonnoose P, Dunn AL, et al. Choosing outcome assessment tools in haemophilia care and research: a multidisciplinary perspective. Haemophilia. 2017;23(1):11–24.
- Timmer MA, Gouw SC, Feldman BM, et al. Measuring activities and participation in persons with haemophilia: a systematic review of commonly used instruments. Haemoph Off J World Fed Hemoph. 2018;24(2):e33–e49.
- Kurtaiş Y, Őztuna D, Küçükdeveci AA, et al. Reliability, construct validity and measurement potential of the ICF comprehensive core set for osteoarthritis. BMC Musculoskelet Disord. 2011;12(1):255.
- Ehrmann C, Prodinger B, Stucki G, et al. Icf generic Set as New standard for the system wide assessment of functioning in China: a multicentre prospective study on metric properties and responsiveness applying item response theory. BMJ Open. 2018;8(12):e021696.
- Prodinger B, Cieza A, Oberhauser C, et al. Toward the international classification of functioning, disability and health (ICF) rehabilitation set: a minimal generic set of domains for rehabilitation as a health strategy. Arch Phys Med Rehabil. 2016;97(6):875–884.
- Stucki G, Cieza A, Geyh S, et al. ICF Core Sets for rheumatoid arthritis. J Rehabil Med. 2004;36(0):87–93.
- Scheuringer M, Stucki G, Huber EO, et al. ICF Core Set for patients with musculoskeletal conditions in early post-acute rehabilitation facilities. Disabil Rehabil. 2005;27(7–8):405–410.
- Krasuska M, Riva S, Fava L, et al. Linking quality-of-life measures using the International Classification of Functioning, Disability and Health and the International Classification of Functioning, Disability and Health-Children and Youth Version in chronic health conditions: the example of young people with hemophilia. Am J Phys Med Rehabil. 2012;91(13 Suppl 1):S74–S83.
- Gouw SC, Timmer MA, Srivastava A, et al. Measurement of joint health in persons with haemophilia: a systematic review of the measurement properties of haemophilia-specific instruments. Haemophilia. 2019;25(1):e1–e10.
- Pettersson H, Ahlberg A, Nilsson IM. A radiologic classification of hemophilic arthropathy. Clin Orthop. 1980;149:153–159.
- Poonnoose PM, Thomas R, Keshava SN, et al. Psychometric analysis of the functional independence score in haemophilia (FISH). Haemoph Off J World Fed Hemoph. 2007;13(5):620–626.
- Wharfe G, Buchner-Daley L, Gibson T, et al. The Jamaican haemophilia registry: describing the burden of disease. Haemoph Off J World Fed Hemoph. 2018;24(4):e179–e186.
- Skinner MW, Chai-Adisaksopha C, Curtis R, et al. The Patient Reported Outcomes, Burdens and Experiences (PROBE) Project: development and evaluation of a questionnaire assessing patient reported outcomes in people with haemophilia. Pilot Feasibility Stud. 2018;4:58.
- Remor E. Development and psychometric testing of the Hemophilia Well-being Index. Int J Behav Med. 2013;20(4):609–617.
- Roosendaal G, van Rinsum AC, Vianen ME, et al. Haemophilic arthropathy resembles degenerative rather than inflammatory joint disease. Histopathology. 1999;34(2):144–153.
- Blobel C, Haxaire C, Kalliolias G, et al. Blood-Induced arthropathy in hemophilia: mechanisms and heterogeneity. Semin Thromb Hemost. 2015;41(08):832–837.
- Valentino LA. Blood-induced joint disease: the pathophysiology of hemophilic arthropathy. J Thromb Haemost. 2010;8(9):1895–1902.
- Gualtierotti R, Solimeno LP, Peyvandi F. Hemophilic arthropathy: current knowledge and future perspectives. J Thromb Haemost. 2021;19(9):2112–2121.
- de Kleijn P, van Genderen FR, van Meeteren NLU. Assessing functional health status in adults with haemophilia: towards a preliminary core Set of clinimetric instruments based on a literature search in rheumatoid arthritis and osteoarthritis. Haemoph Off J World Fed Hemoph. 2005;11(4):308–318.
- Srivastava A, Santagostino E, Dougall A, et al. WFH guidelines for the management of hemophilia. Haemophilia. 2020;26(s6):1–158.
- van Balen EC, Haverman L, Hassan S, et al. Validation of PROMIS Profile-29 in adults with hemophilia in The Netherlands. J Thromb Haemost. 2021;19(11):2687–2701.
- Feng C, Geng B-F, Liu S-G, et al. Activity and participation in haemophiliacs: item response modelling based on international classification of functioning, disability and health. Haemoph Off J World Fed Hemoph. 2023;29(1):308–316.