
Abstract
Background:
Due to the silent and unpredictable nature of obliterating arteriopathy of the lower limbs (OALL) in diabetics, its screening remains essential. The objective of this study was to evaluate the diagnostic performance of the ankle-brachial index (ABI) in the detection of OALL in diabetics.
Methods:
This was a descriptive and comparative cross-sectional study over a period of one year. Type 2 diabetics seen in the Endocrinology Department of the Joseph Raseta Befelatanana University Hospital Center, on whom it was possible to perform arterial Doppler ultrasound of the lower limbs, were included.
Results:
A total of 109 cases of type 2 diabetes were included. The average value of the ABI was 1.06 ± 0.14. ABI ≤ 0.90 and > 1.40 was found in 22.4% and 14.9% of cases, respectively. The prevalence of OALL was 29.8% on arterial Doppler. It was asymptomatic in 50% of cases. The diagnostic performance of the ABI to detect OALL was as follows: for a threshold ≤ 0.90 with CI = 95%: Specificity = 100% [95–100] and 100% [94.9–100], Sensitivity = 71.4% [44.9–88.4] and 77.8% [54.1–91.3], left and right respectively; for a threshold > 1.40 with CI = 95%: Specificity = 92.4% [84.8–96.4] and 90% [81.8–94.8], Sensitivity = 0.0% [0. 0–21.1] and 0.0% [0.0–21.1]), left and right respectively.
Conclusion:
The ABI is a simple and non-invasive tool for early detection of OALL in diabetics. Doppler ultrasound of the lower limbs is always necessary in the event of associated mediacalcosis.
Introduction
Atherosclerosis has become the leading cause of death among diabetics. Indeed, diabetes is an important risk factor for coronary atherosclerosis and peripheral arterial disease, independent of other cardiovascular risk factors. In addition, atherosclerosis in diabetics is more diffuse, more severe and manifests at an earlier age by about 10 years.Citation1 One of the components of the ‘diabetic foot’ with neuropathy and infection, obliterating arteriopathy of the lower limbs (OALL), is the main factor in major amputation in diabetics.Citation2 Amputations are linked to arterial insufficiency in 92% of cases, with diabetes being the cause in 50% of cases. It is estimated that the number of amputees for lower limb arterial insufficiency will increase by 50% by 2030 and 100% by 2050.Citation3 Particularly in Africa, the diabetic foot is responsible for great morbidity and mortality. Its healing is significantly influenced by the presence of arteriopathy.Citation4 Therefore, OALL must be sought and detected systematically and early in diabetics in the same way as other degenerative complications.
OALL is frequently associated with involvement of other territories: coronary, cerebral, carotid or aortic.Citation2 Due to its silent nature and its unpredictable evolution, its treatment is often delayed, up to and including amputation, which is completely avoidable. This remains an underdiagnosed and insufficiently treated pathology, particularly in countries with limited resources, whilst in developed countries there is a lot of technical progress both in availability and accessibility in the diagnosis and treatment of OALL, such as angiography and angioplasty. In Madagascar, a country with limited resources, the search for a diagnostic tool adapted to the reality on the ground to allow an early diagnosis of OALL remains a real challenge.
The measurement of the ankle-brachial index (ABI) is a simple test to perform, inexpensive, reproducible and non-invasive, allowing the diagnosis of OALL in symptomatic patients, as well as the estimation of cardiovascular risk in asymptomatic patients.Citation5,Citation6 Also, a good indication for its use would lead to impacts in terms of cost per justified prescription of arterial echo-Doppler of the lower limbs, which is still difficult to achieve in our country and frequently refused by the patient because of its relatively high cost.
The present study was undertaken to evaluate the diagnostic performance of the ABI in the context of OALL screening in diabetics to improve the management of this pathology in countries with limited resources.
Materials and methods
We carried out a descriptive and comparative cross-sectional study at the Endocrinology Department of the Joseph Raseta Befelatanana University Hospital Center, Antananarivo, Madagascar. The study was conducted over a period of one year, from April 1, 2019 to March 31, 2020. We included in the study patients with known or newly diagnosed type 2 diabetes, hospitalised or coming to an outpatient setting and having had measurement of the ABI and an arterial echo-Doppler of the lower limbs carried out. Patients who refused to be examined and presenting a local pathology of the lower limbs that prevents the measurement of the ABI (gangrene, wound, pain, …) were excluded from our study. Our sampling was done according to a simple random mode without replacement. The individual already chosen cannot be chosen again and has been registered only once.
The diagnosis of diabetes was made according to the criteria of the American Diabetes Association. The typing of diabetes as ‘type 2’ was based on the patient’s age (> 40 years), overweight or obese or in the presence of a family history of type 2 diabetes.Citation7
For the measurement of the ABI, we used:
a Bistos Hi-Dop Vascular Doppler Bt-200® with an 8.0 MHz probe (Seoul, Korea);
an ultrasonic transmission gel;
a manual blood pressure monitor with a 50 cm cuff;
a stethoscope and a calculator.
The measurements were taken by an investigator, twice successively on the posterior tibial and pedal artery on each limb. The ABI of each limb was calculated according to the American Heart Association recommendation by dividing the value of the highest ankle systolic pressure between that of the posterior tibial artery and the pedal artery by the highest systolic humeral pressure.Citation6 After measurement of the ABI, the proposal is made to patients regarding arterial echo-Doppler of the lower limbs.
The parameters studied were sociodemographic data, the diabetic disease, other cardiovascular risk factors, the vascular history, the vascular clinical examination, the ABI, the results of the arterial echo-Doppler of the lower limbs and the diagnostic performance of ABI compared with arterial echo-Doppler of the lower limbs.
Regarding the treatment of diabetes, the most used oral agents were metformin and sulfonylureas. The insulin therapy regimens were: 2 injections morning and evening of mixed insulin; 2 morning and midday injections of rapid-acting insulin with 1 injection of mixed insulin or one injection of slow-acting insulin combined with oral agents (bed-time regimen). The basal-bolus regimen was rarely used due to its high cost. HbA1c and serum lipids were measured using the enzymatic method.
The diagnosis of retinopathy is made in the presence of abnormalities on examination of the vitreous and the fundus after pupillary dilation. The presence of diabetic nephropathy is attested from a bundle of arguments associating microalbuminuria and/or proteinuria, with or without elevation of serum creatinine, and the presence of diabetic retinopathy. The diagnosis of diabetic peripheral neuropathy is suggested by symmetrical distal sensory symptoms beginning in the lower limbs and/or impaired foot sensitivity on examination with a 10 g monofilament. The existence of ischaemic stroke and ischaemic heart disease was confirmed respectively by the cerebral scanner, and the elevation of ultrasensitive troponin with an abnormality on the electrocardiogram in terms of repolarization disorder and/or on the transthoracic echocardiography in terms of kinetic disorder. The diabetic foot was evoked in the presence of trophic disorders following nerve, arterial and often infectious damage occurring on the foot of a diabetic.
We adopted the interpretation of ABI proposed by the American Heart Association.Citation5 It was said to be normal if it was between 0.91 and 1.40. The presence of OALL and incompressible arteries was suggested in the presence of of an ABI ≤ 0.90 and > 1.40 respectively. The severity of OALL is classified according to the value obtained for each leg as proposed by Poitier et al. The OALL was said to be well compensated (light obstruction), moderately compensated (moderate obstruction) or severe (critical ischemia) if the ABI was between 0.70 and 0.90, 0.40 or 0.69 and < 0.40, respectively.Citation8
We used Microsoft Excel® 2013 (Microsoft Corp, Armonk, NY, USA) and R® version 3.6.1 software (R Foundation for Statistical Computing, Vienna, Austria). Quantitative variables were expressed as mean ± standard deviation, median, minimum and maximum, and qualitative variables as numbers and proportion (percentage). The statistical test of proportion comparison was made using the chi-square test if the conditions are met, otherwise using Fisher’s exact test, as appropriate.
The diagnostic performances of the ABI were evaluated by comparison with that of the gold standard, which is arterial echo-Doppler of the lower limbs with a confidence interval of 95% and a value of p < 0.05, which is considered to be statistically significant. The tools used were:
Sensitivity (Fraction of True Positives): proportion of positive individuals effectively detected by the test. In other words, sensitivity measures how well the test performs when used on positive individuals.
Specificity (fraction of true negatives): proportion of negative individuals effectively detected by the test. In other words, specificity measures how well the test performs when used on negative individuals.
Positive predictive value (PPV): proportion of cases effectively positive among the positives detected by the test. PPV = Sensitivity × Prevalence / [(Sensitivity × Prevalence + (1 − Specificity) (1 − Prevalence)].
Negative predictive value (NPV): proportion of effectively negative cases among the negatives detected by the test. VPN = Specificity (1 − Prevalence) / [Specificity (1 − Prevalence) + (1-Sensitivity) Prevalence].
This work was carried out after obtaining the agreement of the director of the establishment, and the head of department. Oral information was provided to each subject participating in the study. The investigations were undertaken only after each participant had signed a free and informed consent form. The data collected were anonymized before being processed by computer.
Results
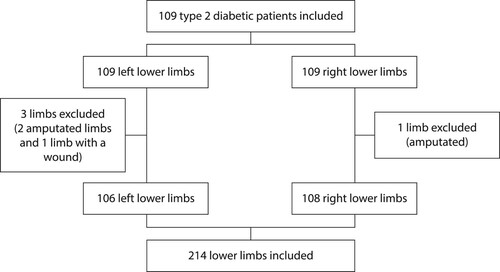
In total, we retained 109 patients with 214 lower limbs for pulse palpation, ABI measurement and arterial echo-Doppler, including 106 limbs on the left and 108 limbs on the right ().
Figure 1: Study population.
represents the general characteristics of the study population. The average age of the patients was 60.4 ± 8.4 years with extremes of 43–77 years. The sex ratio (male/female) was 1.13. The mean body mass index was 24 ± 3.1 kg/m², with a minimum of 17 kg/m² and a maximum of 34 kg/m². The known mean duration of diabetes progression was 8 ± 6.9 years. The rates of use of oral antidiabetics alone and insulin therapy alone were 32.1% and 24.8% respectively. All our patients had benefited from an Hb A1c assay, the average of which was 9.1% ± 2.7 (76 mmol/mol). Diabetes was mostly complicated by nephropathy and retinopathy in 43.1% and 35.8% of cases respectively.
Table 1: General characteristics of the study population (N = 109)
The main cardiovascular risk factors associated with diabetes were hypertension (67.8%), dyslipidaemia (78.3%) and sedentary lifestyle (59.6%) ().
Table 2: Associated cardiovascular risk factors (N = 109)
In terms of vascular history, nine patients (8.3%) had previous amputations and no patient underwent vascular surgery. On clinical vascular examination of the lower limbs, 1.8% of patients presented with chronic ulceration and 5.5% with trophic disorders. The femoral pulses of both limbs were all perceived. The popliteal, posterior tibial and anterior tibial pulses were not palpable in 2.9%, 8.5% and 9.4% of cases respectively on the left and in 0.9%, 6.4% and 7.4% of cases respectively on the right.
summarises the results of ABI measurements and arterial echo-Doppler. The average ABI was 1.06 ± 0.14 with a minimum of 0.48 and a maximum of 1.63. It was ≤ 0.90 in 9.4% and 13% of cases in the left and right lower limbs, respectively. Among the 24 limbs with OALL according to the ABI, 50% were stage I, 5% stage IIa, 15% stage IIb, 0% stage III and 30% stage IV according to the Fontaine and Leriche classification. According to the ABI, OALL was well and moderately compensated in 66.7% and 33.3% of cases, respectively. On arterial echo-Doppler, the prevalence of OALL was 29.8% including 13.1% on the left and 16.7% on the right.
Table 3: Results of ankle-brachial index measurements and arterial echo-Doppler
shows the diagnostic performance study of the ABI with the OALL compared with the result of the arterial echo-Doppler. A threshold value ≤ 0.90 of the ABI is not very sensitive (71.4% on the left and 77.8% on the right) to detect OALL. While it is very specific, confirming the OALL almost 100%. A threshold value > 1.40 of the ABI was also not sensitive to detect OALL, whereas the specificity is good with 92.4% on the left and 90% on the right. However, an ABI < 1.40 does not completely exclude OALL (VPN at 81.8% on the right and 85.8% on the left).
Table 4: Diagnostic performance of the ankle-brachial index with obliterating arteriopathy of the lower limbs compared with the result of the arterial echo-Doppler
Discussion
The average age of our patients was 60 years with a peak frequency between 50 and 69 years (72.1%). This was slightly higher than that of Konin et al. in Abidjan Côte d’Ivoire,Citation9 and Codjo et al. in Parakou, Benin,Citation10 whose average age of patients was 55.8 and 53.7 years, respectively. However, the peak age beyond 50 years was also observed in 71.4% and 66.3% of cases respectively. Indeed, arteriopathy is rare before the age of 50 (less than 5%), increases exponentially from the age of 60 to reach more than 20% after the age of 70.Citation11 Nevertheless, it should not be limited to older diabetics to screen for OALL in diabetics, especially in the presence of other cardiovascular risk factors.
The male predominance (sex ratio = 1.13) in our study matched that of the literature. However, diabetes increases the risk of obliterating arteriopathy of the lower limbs (by 4 in men and 6 in women).Citation12 Other authors have also noted a slightly higher prevalence among women in low-income countries, particularly of African origin, and a similar prevalence among women and men in high-income countries.Citation11 Thus, OALL must be detected unambiguously in both genders.
The diabetes of our patients evolved over less than 10 years in 61.5% of cases, with an average duration of 8 years. Codjo et al., as well as Konin et al., also observed in most cases the diabetes evolving over less than 10 years, respectively 77.5% and 76%.Citation9,Citation10
In our study, only 21.1% of patients followed lifestyle and dietary measures, whereas the latter constitute the main pillars of the management of diabetes according to the recommendations.Citation13 Among our diabetics, 32.1% took an oral agent alone, 24.8% insulin alone and 22% a combination of oral agent and insulin. In the study by Konin et al., patients received an oral agent in 56.5% and insulin in 43.5% of cases.Citation9 In the study by Codjo et al., 98% were on oral agent monotherapy and 2% on combined oral agent and insulin.Citation10
The average glycated haemoglobin of our patients was 9.1%, of which 88.2% were greater than 6.5%. In Parakou, diabetes was unbalanced (HbA1c ≥ 7%) in 57.6% of cases.Citation11 The study carried out in Spain in type 2 diabetics found an average HbA1c of 7.35 ± 1.63%.Citation14 In the Malmberg et al. study, a significant correlation was reported between the incidence of vascular complications and the HbA1c level.Citation15 Any 1% increase in HbA1c was associated with a 28% increase in the risk of OALL occurring.Citation16 Therefore, the search for arteriopathy is essential in the face of any glycaemic imbalance.
In our study, most patients suffered from several simultaneous complications. Nephropathy was the most observed (43.1%), followed by retinopathy (35.8%) and diabetic foot (25.7%). Indeed, retinopathy is present in 75% of cases in type 2 diabetes with diabetic nephropathy according to the literature.Citation17 Alves-Cabratosa et al. found in their study 5.5% nephropathy, 1.96% retinopathy and 0.8% neuropathy.Citation14 For diabetic foot, complications still seem to be very common in Madagascar, with sometimes very serious consequences. The best prevention remains early detection of podiatric risk and respecting the various rules of foot hygiene. We have already targeted much focus on this subject in our diabetics in 2014.Citation18
Hypertension was found in 67.8% of our patients. Similarly, Alves-Cabratosa et al. in Spain had found 67.9% of hypertension in their patients.Citation14 In Africa, 51.6% of the patients of Codjo et al.,Citation10 and 41.6% of the patients of Konin et al.Citation9 were hypertensive. Indeed, the prevalence of hypertension in diabetic patients is more than three times higher than that of non-diabetic patients of the same gender and age. It was found in 60% of known diabetics, 40% in newly diagnosed diabetics and 30% non-diabetics.Citation19 In addition, the other mechanism that may be linked to this hypertension in our diabetics is the high prevalence of diabetic nephropathy. In addition, hypertension associated with diabetes multiplies the risk of OALL by 2.5 in men and 5.7 in women.Citation5 It also increases the risk of macroangiopathy 2.9-fold in men and 3.9-fold in women.Citation20 Therefore, screening for OALL in hypertensive diabetics should therefore be systematic, reinforced and improved.
Among our 46 patients who were able to perform a lipid assessment, 36 (78.3%) had dyslipidaemia. African studies carried out on diabetic subjects in Abidjan and Benin showed respectively 16% and 6.3% dyslipidaemia.Citation9,Citation10 A study carried out on the general population in Senegal constituting 18.3% of diabetics and another study in Spain found respectively 71.2% and 15.99% of dyslipidaemia.Citation21,Citation22 Even if the lipid abnormality seems to vary greatly from one study to another, it has been demonstrated that the prevalence of dyslipidaemia is high in type 2 diabetes, both qualitatively and quantitatively.Citation12 In addition, the total cholesterol/HDL-cholesterol ratio was the most powerful indicator of dyslipidaemia to predict OALL with risk multiplied by 3.9.Citation11 Thus, patients with lipid disorders should be targeted particularly in the search for OALL.
In our study, 32.1% of patients were overweight and 3.7% obese, noting that these were all obese androids. According to an African statistic, a prevalence of obesity was lower, ranging from 14% to 35% in black Africans.Citation9 However, in the Occident, a study conducted in Newcastle, UK found an average BMI of 33.9 kg/m2 in diabetics.Citation23 Even if the role of obesity or overweight in OALL is still debated, inconsistent and controversial, the literature specifies that fat located in the abdomen is considered particularly toxic and predisposes to metabolic and cardiovascular diseases.Citation11 Therefore, screening for OALL should not be neglected.
Some 8.3% of our population have already undergone amputation for OALL or diabetic foot. Our result agrees with the literature, which estimated that 5–10% of diabetics will undergo an amputation in their lifetime,Citation24 with a risk 17–40 times higher than that of that of that of non-diabetics.Citation25
In our study, chronic ulceration was found in 1.8% of cases. According to Bartus and Margolis, the incidence of foot ulcers in diabetics ranges from 1.0% to 4.1%.Citation26 The absence of pain in diabetics also promotes the occurrence of repeated trauma and unnoticed wounds, explaining the discovery at the irreversible stage of OALL.
Regarding pulse palpation, the distal pulses can be eradicated while the popliteal pulse is still present in arteriopathy of the lower limbs. Indeed, Collins et al. found in their study that the sensitivity of pulse obliteration to detect OALL was low (17.8–32.4%) compared with ABI, while its specificity was good (97.8–98.7%).Citation27 Moreover, according to Lazareth et al., pulse palpation remains of interest, particularly when there is an eradication of two distal pulses with a sensitivity of 94.4% and a specificity of 90%.Citation28
In our series, the ABI ≤ 0.90 reflecting OALL and > 1.40 reflecting mediacalcosis were found respectively in 9.4% and 8.3% of the limbs on the left and in 13% and 6.6% of the limbs to the right. In the study by Konin et al., the ABI was less than or equal to 0.90 in 14.93% of cases on the right and 7.14% of cases on the left and was greater than 1.3 in 18.2% of cases.Citation9 Codjo et al. found OALL in 41.9% of cases and mediacalcosis in 12% of cases.Citation10 It appears that the ABI could detect many cases of arteriopathy in diabetics given the variety of clinical presentations of OALL. Its use was limited in diabetics due to the high frequency of mediacalcosis inducing an elevation of the ABI.
In our study, 50% of patients with OALL were classified as Leriche–Fontaine stage I (asymptomatic), 30% stage IV and 20% stage II (intermittent claudication). This was consistent with data from the literature, where the asymptomatic stage is the most frequent clinical presentation (20–50%).Citation29 However, intermittent claudication would be found in only 10–35% of patients who presented with atypical exertional pain.Citation30 The presence of distal sensory polyneuropathy explains the poor symptomatology in diabetics. In this context, it will be preferable to use the current High Authority for Health (HAS) classification. The latter considers clinical and haemodynamic criteria classifying patients into stress ischaemia, permanent ischaemia and chronic critical ischaemia.Citation31 However, we did not have all the technical means of a microcirculatory study to use this current classification. Very few data make it possible to clearly establish the natural evolution of asymptomatic to symptomatic OALL, but the annual degradation of ABI has been estimated at −0.01 to −0.02.Citation32 Therefore, regularly ABI measurement plays an important role in screening to complete the interrogation and the clinical examination, to monitor both asymptomatic and symptomatic OALL.
According to the measurement of the ABI, the OALL of our patients was of mild and medium severity in 66.7% and 33.3% of cases respectively. In Senegal, 67.7% of OALL was well compensated, 23.5% moderately compensated and 8.8% critical ischemia.7 Similarly in Spain, OALL of mild severity predominated (79.6%), followed by moderate (17.7%) and severe (2.7%).Citation14
On echo-Doppler results, OALL was well compensated, poorly compensated and associated with mediacalcosis in 11.2%, 10.5% and 8.3% of our patients, respectively. Mediacalcosis was objectified in 24.3% of our patients. The concomitant presence of mediacalcosis and OALL is not so rare in diabetics, whereas the existence of these calcium deposits could mask the OALL.Citation33 Echo-Doppler was therefore the only non-invasive examination capable of detecting both OALL and mediacalcosis.
In our study, the prevalence of OALL was 22.4% on IPS and 29.8% on arterial Doppler. Globally, it is currently estimated that more than 200 million individuals are affected by this disease worldwide.Citation11 This prevalence was high in diabetics (13.6%) compared with the general population (4%).Citation34 Moreover, the ABI seems physiologically a little lower, around 0.02 in women and in subjects of African origin.Citation35
Using echo-Doppler as the gold standard, ABI had good specificity (100%) and low sensitivity (71.4–77.8%) for detecting OALL in our study. This good predictive value of the ABI ≤ 0.90 has been validated by several studies since its first use. According to the literature, specificity varied from 93% to 99% and sensitivity from 53% to 89%.Citation36–39 This low sensitivity of the IPS in diabetics could be explained by the incompressibility of the artery in these subjects linked to the high frequency of mediacalcosis.Citation23,Citation40 This made the value of the ABI falsely high. In addition, a high ABI value (> 1.3–1.4) seems to have to be interpreted as a sign of an underlying OALL and requires continued non-invasive exploration in search of arterial lesions.Citation41 Thus, in diabetics, a normal ABI does not formally eliminate arteriopathy, hence the importance of carrying out a complete examination. Another study also specified that the presence of OALL is also defined on an ABI < 0.9 but also on an ABI > 1.4.Citation42 The decrease in the diagnostic efficiency of the ABI in diabetics may also be due to the anatomical particularity of the location of the OALL in the distality of the lower limbs.
In addition, other authors had found that the specificity and sensitivity of the ABI remained low ranging, respectively from 30% to 83.3% and from 69.3% to 83.7% considering angiography as reference examination.Citation43,Citation44
Conclusion
To conclude, the prevalence of OALL was high in type 2 diabetics. The sensitivity of ABI was low compared with arterial echo-Doppler of the lower limbs in the detection of OALL, while it maintained its good specificity and its strong positive predictive value. The presence of mediacalcosis was the main factor in the reduction of the diagnostic efficiency of ABI in diabetic populations. Thus, arterial echo-Doppler remains the reference examination for the morphological and haemodynamic study of the arteries of the lower limbs. It is also essential for the conduct of treatment.
Generalisation of the measurement of ABI would make it possible to adequately detect a subpopulation still asymptomatic and at high cardiovascular risk. In Madagascar, where health structures do not allow easy access to additional examinations, the validation of a simple, accessible and non-invasive measurement tool such as the IPS is essential.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Guilmot JL, Diot E, Boissier C. Diabetic arteriopathy. Microcirculation, an inevitable therapeutic objective. J Mal Vasc. 2001;26(2):135–41.
- Edmonds ME, Shanahan C, Petrova NL. Diabetic peripheral arteriopathy: a tale of two diseases. Front Diabeties Basel, Karger. 2018;26:60–9.
- Zingg M, Nicodème JD, Uçkay I, et al. Lower limb amputation: indication, preoperative workup and complications. Rev Med Suisse. 2014;10(455):2409–13.
- Abbas ZG, Lutale JK, Game FL, et al. Comparison of four systems of classification of diabetic foot ulcers in Tanzania. Diabet Med. 2008;25(2):134–7.
- Doobay AV, Anand SS. Sensitivity and specificity of the ankle-brachial index to predict future cardiovascular outcomes: a systematic review. Arterioscler Thromb Vasc Biol. 2005;25(7):1463–69.
- Aboyans V, Criqui MH, Abraham P, et al. Measurement and interpretation of the ankle-brachial index: a scientific statement from the American Heart Association. Circulation. 2012;126(24):2890–909.
- American Diabetes Association. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes-2019. Diabetes Care. 2019;42(Suppl 1):S13–28.
- Potier L, Abi Khalil C, Mohammedi K, et al. Use and utility of ankle brachial index in patients with diabetes. Eur J Vasc Endovasc Surg. 2011;41(1):110–16.
- Konin C, Essam N'loo AS, Adoubi A, et al. Peripheral arterial disease of the lower limbs in African diabetic patients: ultrasonography and determining factors. J Mal Vasc. 2014;39(6):373–81.
- Codjo HL, Adoukonou TA, Wanvoegbe A, et al. Prevalence of peripheral artery disease among diabetics in Parakou in 2013. Ann Cardiol Angeiol (Paris). 2016;65(4):260–4.
- Aboyans V, Sevestre MA, Désormais I, et al. Epidemiology of lower extremity artery disease. Presse Med. 2018;47(1):38–46.
- Bourron O. Lower limb arterial disease in patients with diabetes. Rev Prat. 2019;69(6):620–5.
- American Diabetes Association. 6. Glycemic targets: standards of medical care in diabetes-2019. Diabetes Care. 2019;42(Suppl 1):S61–70.
- Alves-Cabratosa L, Comas-Cufí M, Ponjoan A, et al. Levels of ankle-brachial index and the risk of diabetes mellitus complications. BMJ Open Diabetes Res Care. 2020;8(1):e000977.
- Malmberg K, Rydén L, Wedel H, et al. Intense metabolic control by means of insulin in patients with diabetes mellitus and acute myocardial infarction (DIGAMI 2): effects on mortality and morbidity. Eur Heart J. 2005;26(7):650–61.
- American Diabetes Association. Peripheral arterial disease in people with diabetes. Diabetes Care. 2003;26(12):3333–41.
- American Diabetes Association. 11. Microvascular complications and foot care: standards of medical care in diabetes-2019. Diabetes Care. 2019;42(Suppl 1):S124–38.
- Raharinavalona SA, Ramalanjaona HR, Andrianera N, et al. Podiatric risk screening in patients with type 2 diabetes in Antananarivo. Pan Afr Med J. 2017;27:213.
- Laakso M. Hypertension and macrovascular disease - the killing fields of NIDDM. Diabetes Res Clin Pract. 1998;39(Suppl):S27–33.
- Kannel WB, McGee DL. Diabetes and cardiovascular disease. The Framingham study. JAMA. 1979;241(19):2035–8.
- Pessinaba S, Mbaye A, Kane A, et al. Screening for asymptomatic peripheral arterial occlusive disease of the lower limbs by measuring the ankle-brachial index in the general population (Senegal). J Mal Vasc. 2012;37(4):195–200.
- Ramos R, Quesada M, Solanas P, et al. Prevalence of symptomatic and asymptomatic peripheral arterial disease and the value of the ankle-brachial index to stratify cardiovascular risk. Eur J Vasc Endovasc Surg. 2009;38(3):305–11.
- Casey SL, Lanting SM, Chuter VH. The ankle brachial index in people with and without diabetes: intra-tester reliability. J Foot Ankle Res. 2020;13(1):21.
- Besse JL, Leemrijse T, Deleu PA. Diabetic foot: the orthopedic surgery angle. OrthopTraumatol Surg Res. 2011;97(3):314–29.
- Fard AS, Esmaelzadeh M, Larijani B. Assessment and treatment of diabetic foot ulcer. Int J Clin Pract. 2007;61(11):1931–8.
- Bartus CL, Margolis DJ. Reducing the incidence of foot ulceration and amputation in diabetes. Curr Diab Rep. 2004;4(6):413–18.
- Collins TC, Suarez-Almazor M, Peterson NJ. An absent pulse is not sensitive for the early detection of peripheral arterial disease. Fam Med. 2006;38(1):38–42.
- Lazareth I, Taieb JC, Michon-Pasturel U, et al. Ease of use, feasibility and performance of ankle arm index measurement in patients with chronic leg ulcers. Study of 100 consecutive patients. J Mal Vasc. 2009;34(4):264–71.
- Norgren L, Hiatt WR, Dormandy JA, et al. Inter-society consensus for the management of peripheral arterial disease (TASC II). Eur J Vasc Endovasc Surg. 2007;33(Suppl 1):S1–75.
- McDermott MM, Guralnik JM, Ferrucci L, et al. Functional decline in lower-extremity peripheral arterial disease: associations with comorbidity, gender, and race. J Vasc Surg. 2005;42(6):1131–7.
- Haute Autorité de Santé. Clinical management of occlusive artheromatous arterial disease of the lower limbs (indications for drugs, revascularization and rehabilitation) - April 2006 - guidelines. J Mal Vasc. 2006;31(4 Pt 1):206–17.
- Mahé G, Jaquinandi V. Diagnosis of lower limb peripheral artery disease. Presse Med. 2018;47(1):47–55.
- Edwards RB, Jaffe W, Arrowsmith J, et al. Calciphylaxis: a rare limb and life-threatening cause of ischaemic skin necrosis and ulceration. Br J Plast Surg. 2000;53:253–5.
- Chevtchouk L, Silva MHSD, Nascimento OJMD. Ankle-brachial index and diabetic neuropathy: study of 225 patients. Arq Neuropsiquiatr. 2017;75(8):533–8.
- Aboyans V, Salazar J, Lacroix P. Obliterating arterial disease of the legs in women. Presse Med. 2010;39(2):263–70.
- Schröder F, Diehm N, Kareem S, et al. A modified calculation of ankle-brachial pressure index is far more sensitive in the detection of peripheral arterial disease. J Vasc Surg. 2006;44(3):531–6.
- Alnaeb ME, Boutin A, Crabtree VP, et al. Assessment of lower extremity peripheral arterial disease using a novel automated optical device. Vasc Endovascular Surg. 2007–2008;41(6):522–7.
- Williams DT, Harding KG, Price P. An evaluation of the efficacy of methods used in screening for lower-limb arterial disease in diabetes. Diabetes Care. 2005;28(9):2206–10.
- Clairotte C, Retout S, Potier L, et al. Automated ankle-brachial pressure index measurement by clinical staff for peripheral arterial disease diagnosis in nondiabetic and diabetic patients. Diabetes Care. 2009;32(7):1231–6.
- Suzuki E, Kashiwagi A, Nishio Y, et al. Increased arterial wall stiffness limits flow volume in the lower extremities in type 2 diabetic patients. Diabetes Care. 2001;24(12):2107–14.
- Abouhamda A, Alturkstani M, Jan Y. Lower sensitivity of ankle-brachial index measurements among people suffering with diabetes-associated vascular disorders: A systematic review. SAGE Open Med. 2019;7:2050312119835038.
- Wu CK, Yang CY, Tsai CT, et al. Association of low glomerular filtration rate and albuminuria with peripheral arterial disease: the National Health and Nutrition Examination Survey, 1999–2004. Atherosclerosis. 2010;209(1):230–4.
- Janssen A. Pulsatility index is better than ankle-brachial Doppler index for non-invasive detection of critical limb ischaemia in diabetes. Vasa. 2005;34(4):235–41.
- Niazi K, Khan TH, Easley KA. Diagnostic utility of the two methods of ankle brachial index in the detection of peripheral arterial disease of lower extremities. Catheter Cardiovasc Interv. 2006;68(5):788–92.