
ABSTRACT
Background
Identification of national research agendas for mental health and disability can be supported by well-designed research priority-setting studies. Few low- and middle-income countries (LMICs) have undertaken such studies.
Objective
To identify mental health and disability research priorities in Ghana.
Methods
A mixed methods study comprising a rapid review, research priority ranking survey, and research capacity needs assessment survey was employed. Participants in the surveys included five expert pools identified from online search and existing database on mental health civil society organisations/non-governmental organisations. The research priority ranking was completed in two stages, using the Child and Nutrition Research Initiative (CHNRI) method to identify priority questions for immediate and short term (0 to 5 years) and medium to long term (>5 years) in stage two. Both surveys were deployed online using google forms. Analysis for the ranking survey involved computing total scores from the CHNRI criteria and generating ranks for the research questions.
Results
A total of 68 experts (97% response rate), generated 94 and 92 questions for the short and long term, respectively. Forty experts (58% response rate) completed the ranking stage. The top 10 ranked research questions included: 4 questions addressing health systems; 2 questions on epidemiology; and 4 questions on interventions. All research questions were considered urgent and should be conducted in the immediate to short term (0–5 years). The methodological capacity of researchers to conduct disability and mental health research is weak.
Conclusion
Our approach has generated an agenda for mental health and disability research priorities for Ghana and demonstrated that it is feasible to employ a systematic methodology for research priority setting that includes key parameters of context and research capacity.
Responsible EDITOR
Stig Wall
Background
Mental, Neurological and Substance Use (MNS) [Citation1] conditions are key drivers of increased morbidity and mortality in the world over [Citation2]. The burden of these conditions has been increasing in main low-and-middle-income countries (LMIC) [Citation3]. While these increases are being recorded, most people living with MNS conditions do not receive the required treatments, and in Ghana, this treatment gap is estimated to be as high as 98% [Citation4]. This neglect is primarily due to the low priority that has been accorded mental health in the public health agenda [Citation5].
Research on mental health is increasingly recognised as integral to the strengthening of national health systems [Citation6] to respond to the treatment gap. The huge disparity in research investment was identified several decades ago and is referred to as the 10/90 gap: less than 10% of global funding for research is spent on diseases that affect more than 90% of the world’s population [Citation7,Citation8]. Despite some successes, this trend remains, particularly for mental health [Citation3]. These disparities in research will pose significant challenges in achieving the sustainable development goals [Citation9]. There is an urgent need to develop national research agendas that align with knowledge gaps [Citation6].
The identification of national research agendas for mental health and disability can be supported by well-designed research priority-setting studies. Priority setting exercises are promising for surfacing vital evidence [Citation10]. They are an important step in identifying the most pressing mental health challenges in a given setting [Citation11,Citation12], in order to address the 10/90 gap and ensure the most efficient use of resources. These studies have largely been carried out at global or regional levels [Citation13], and at the level of the broad area of health, but as argued in other reports, priority-setting methodology needs to reflect the context [Citation14], country-specific needs [Citation15], and be iterative [Citation16]. The field of health research priority setting is relatively new and few LMICs have established these processes [Citation17,Citation18], particularly for mental health. There are however notable initiatives such as the WHO’s Global Health R&D Observatory [Citation19], Lancet Commission on Global Mental Health [Citation3], and Grand Challenges in Global Mental Health [Citation20]. In the field of mental health, there have been very few reported country-level research priority setting initiatives [Citation21,Citation22]. In Ghana, there have been previous attempts by the Mental Health Authority of Ghana [Citation23] and the Ghana Health Service [Citation24] to identify priorities for health research, but these were primarily for operational purposes and thus were not peer-reviewed and published. Important limitations were noted, including the lack of clarity in the selection of stakeholders. The proper selection of stakeholders is important because it is difficult to judge the validity of the priorities identified without adequate stakeholder involvement [Citation14]. The Government of Ghana passed a Disability Act in 2006 (Act 715 [Citation25]) and ratified the Convention on the Rights of Persons with Disabilities in 2012, affirming its recognition of the rights of persons with disabilities. The Act stipulates the establishment of a National Council on Persons with Disability (NCPD). A key function of NCPD is to promote studies and research on issues of disability and provide education and information to the public on issues of disability, but we are not aware of a clear research agenda to guide the conduct of research.
Ghana Somubi Dwumadie (Ghana Participation Programme) is a four-year disability programme in Ghana, with a specific focus on mental health. This programme is funded with UK aid from the UK government [Citation26]. The conduct of research priority setting studies for mental health and disability is one of the key strategies for influencing change.
There are several published methods describing different approaches for setting priorities for health research, but a common observation is that there is no single best practice [Citation27,Citation28]. The Child and Nutrition Research Initiative (CHNRI) method [Citation29], is arguably the most used approach in setting mental health research priorities [Citation21]. The Combined Approach Matrix (CAM) [Citation30] has also been used, but unlike CHNRI, it does not follow a standard prioritization process [Citation31]. The Council on Health Research and Development (COHRED) method [Citation28] combines elements of CHNRI and CAM. However, little is known about how to strengthen the standard research prioritization process with key contextual information such as the level of research activity, capacity, and funding. It is also not clear if the individual CHNRI criteria will receive equal endorsement in terms of usefulness in determining research priorities in the Ghanaian context. The lessons from this enhanced process are transferable and can inform other African countries who may wish to conduct similar priority setting studies, particularly for mental health.
The aim of this paper was to identify mental health and disability research priorities for Ghana within the context of the prevailing research ecosystem.
Methods
Study design. Two study designs were employed: first, a rapid review on mental health and disability research in Ghana over the last 10 years; and second a structured cross-sectional survey on priority mental health and disability research questions for the short to medium term and long term. Ethical approval for the study was obtained from the Ghana Health Service Ethics Review Committee (GHS-ERC025/08/20) and King’s College London Research Ethics Committee (LRS-20/21-20,866). The two studies are described below. The schedule of activities and steps is shown in .
Figure 1. Flowchart of mental health and disability research priority ranking process.
Study 1: rapid review
Search strategy
Standard rapid review strategies [Citation32] were employed. The detailed methodology on the rapid review is provided in our companion paper (in preparation). In summary, a comprehensive search of electronic databases (PubMed, Embase, PsycINFO, Scopus and Cochrane) was done to identify relevant studies on mental health and disability conducted in or on Ghana over the 10 years from 2010 to 2020. The key search terms used in this review are ((‘mental health’ [MeSH Terms] OR (‘mental health’ [MeSH Terms] OR (‘mental’ [All Fields] AND ‘health’ [All Fields]) OR ‘mental health’ [All Fields])) OR ‘disability’ [All Fields]) AND (‘Ghana’ [MeSH Terms] OR ‘Ghana’ [All Fields]). The full search strategy is included in the appendix. Reference lists of selected articles and relevant systematic reviews were screened to identify any other relevant articles that were missed during the initial database search. All types of studies were included regardless of the study design and the study population. Following a rigorous selection, 375 articles were retrieved, and the relevant data extracted using a standard data extraction form.
Study 2: MH research priority ranking survey
Design: This was an iterative cross-sectional survey conducted over two stages.
Stage 1: Identification of relevant research questions
This stage involved two key steps as described below.
Step 1: Stakeholder mapping and grouping process: Study participants were identified through a process of stakeholder mapping and grouping to ensure a broad range of respondents for the study. The mapping exercise was conducted through online searches and a personal database maintained by a colleague who has been conducting various ethnographic mental health research in Ghana for the past 15 years [Citation33] on mental health service providers to identify potential experts in the following pools: (a) Expert pool 1: Clinicians; (b) Expert pool 2: Researchers/academia; (c) Expert pool 3: Non-Governmental Organisations/Civil Society Organisations in mental health and disability; (d) Expert pool 4: Policy makers; and (e) Expert pool 5: Funders, multilateral and unilateral organisations. Our stakeholder mapping identified and oversampled 153 potential respondents. However, based on the response rate from similar previous surveys [Citation21], we anticipated up to 70 complete responses.
Step 2: Data collection and processing: An online survey was conducted from 6 November to 20 November 2020. Respondents from all the expert pools were asked to provide responses to two questions on research priorities: (1) please identify your top 3 research questions in mental health and disability in the immediate and short term (0–5 years); and (2) please identify your top 3 research questions in mental health and disability in the medium to long term (>5 years).
In order to explore current research capacity needs in relation to the identified research priorities in Ghana, we derived a set of research domains developed for a mental health research capacity needs assessment in six low- and middle-income countries as part of the Emerging Mental Health systems in low- and middle-income countries (Emerald) project [Citation34]. These questions were deployed only to respondents from expert pool 2 (researchers/academia) and the leadership of research/academic institutions. Participants were asked to respond to two separate but interlinked questions. In the first question, participants were asked to rate (on a 5-point Likert scale; 1 = very weak; 2 = weak; 3 = OK but could be improved; 4 = Strong; 5 = very strong) the current institutional capacity to conduct research in 16 pre-selected areas: Health Services Research; Disability Research; Global Mental Health Research; Qualitative Research; Population Level Surveys; Economic Evaluation; Evaluation of Complex Interventions; Analysis of complex population datasets; Health economics evaluation; Implementation science; Empowering service users in research; Action Research; Research on stigma and discrimination; Public engagement; Ethical conduct of research; and Social and Behaviour Change Communication. In the second question, participants were asked to rate (on a 3-point likert scale; 1 = low priority; 2 = moderate priority; 3 = high priority), the level of priority for building capacity to conduct research in the above pre-selected areas. We had planned to conduct qualitative interviews with relevant stakeholders to elicit views on the interface between policy and research, key challenges for research capacity, and priorities for development but this was not done because of the challenges posed by COVID-19.
Data were downloaded onto an Excel spreadsheet and transferred to STATA for analysis.
In stage 1 of the survey, 68 participants (97.0% response rate) identified 186 research questions comprising 94 and 92 for the immediate, short-term, and medium-to-long-term Mental Health and Disability Research Priorities, respectively (Supplementary Table 1). An examination of the two sets of questions by timeline showed that the same set of questions were noted for both timeframes. These were thus combined, and a uniform set of questions taken forward to the ranking stage. The investigators (CL, AK, LS, BW) pruned and rationalised the research questions, removing duplicates, merging the same or similar questions, and restructuring statements into questions. This process resulted in 55 mental health and disability research questions, which were grouped in five thematic areas (Supplementary Table 2) and taken forward to stage 2 for scoring and ranking.
Stage 2: scoring and ranking of research questions
In the second stage, the rationalised 55 research questions were emailed to all 68 stakeholders that participated in the first survey via Google Forms to score based on the Child and Nutrition Research Initiative (CHNRI) criteria. The CHNRI is a priority-setting methodology developed by Rudan et al. (2007) that had been previously used to establish mental health priorities on a global level [Citation35]. The CHNRI criteria include: (1) the likelihood of answerability in an ethical way, (2) the likelihood of efficacy and effectiveness, (3) the likelihood of deliverability and affordability, (4) the maximum potential for disease burden reduction, and (5) the likely impact of equity in the population. Thus, for each research question, participants were asked to rate the relevance of each criterion by selecting one of the following response options: 1. ‘Yes’, 2. ‘No’, 3. ‘I Don’t know’ or 4. ‘Not Applicable’. Given these criteria were applied for the first time in the Ghanaian context, the study examined the applicability of the criteria in terms of their individual usefulness (measured by frequency of endorsement) in identifying research priorities. Additionally, participants were asked to indicate if a particular research question should be addressed within the immediate and short term [0–5 years] or medium to long term [>5 years].
More than half (40/68) of participants returned completed questionnaires. The rationalised 55-question list is presented in supplementary Table 2. All the included questions received at least five ratings based on the 5 CHNRI criteria described.
Analysis
Estimation of score for ranking
For this analysis a ‘Yes’ response to any of the 5 CHNRI criteria was coded 1, and all other response options coded 0. Thus, for each research question, the total possible score is 5. This translates to a total score of 275 for the 55 questions. Scores across each respondent were summed and a total score and proportion generated for each research question. Mean scores for each question were also computed and reported along with the score proportion. The mean scores and proportions were ranked, and the top 10 research questions identified.
Estimation of most endorsed CHNRI criteria
Similarly, for this analysis, a ‘Yes’ response to any of the 5 CHNRI criteria was coded 1, and all other response options coded 0. Thus, across respondents the total possible score for each CHNRI criteria is 40. Scores for each CHNRI criteria were summed across respondents and a total score generated for each research question. Mean scores were generated for each CHNRI criteria across all questions, and test of difference in means conducted.
Determination of mean existing research capacity and priority score
In order to determine the current research capacity needs in relation to the identified research priorities in Ghana, mean scores and standard deviations were generated for existing research capacity over a range of scores from 1 to 5 for each of the 16 pre-identified research areas. A similar analysis was conducted to generate mean scores and standard deviations to identify priority research domains across each research area.
Additional chi-square analysis was conducted to determine differences in demographic characteristics between participants in stage 1 (survey 1) and stage 2 (survey 2). Probability values of p < 0.05 were considered to be statistically significant differences that could not have been due to chance.
Results
Rapid review
Key relevant findings from our rapid review are provided. The detailed results on the rapid review are provided in our companion paper (in preparation). In summary, of the 375 articles included in this review, 232 (62.0%) of the articles were on mental health, while the remaining 143 (38.0%) were on disability.
Mental health research output and funding
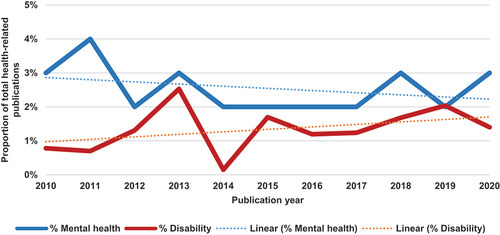
shows that within the ten-year period (2010–2020), there has been a general decline in reported studies on mental health as a proportion of total health-related research publications. The current trend however shows an increasing trajectory between 2019 and 2020. Supplementary figure 1, however, shows that within the same period, there has been a steady increase in absolute numbers of reported studies on mental health in Ghana. Comparatively, there were more studies on mental health than studies on other disabilities.
Figure 2. Mental health and disability research publications as a proportion of total health-related publications over a 10-year period.
The review also identified 13 key themes covered in mental health research. Of these, a significant majority (69.0%) focused on the epidemiology (prevalence, determinants) of mental health conditions and events. On the contrary, very little research has been conducted around health policy and systems (5.0%), including mental health workforce, service delivery collaboration (with traditional and faith-based healers), and policy and legislation.
In terms of design, most of the mental health studies included in this review were either observational quantitative studies (n = 130, 56.0%) or observational qualitative studies (n = 79, 34.0%). There were very few interventional studies (n = 6, 3%). In terms of research funding, 98 (42.0%) of the articles were from studies that had received external funding support, and 16.0% were unfunded.
Other disabilities research output and funding
shows that within the ten-year period (2010–2020), there has been a steady increase in reported studies (N = 143) on disability (excluding mental health) as a proportion of total health-related research publications. This observation is consistent with trends in the actual number of studies conducted on disabilities within the same period (supplementary figure 1), with a clear increase recorded between 2016 and 2019.
Similar to the profile of studies on mental health, understanding the epidemiology (prevalence, determinants) of disability in Ghana was the most common (54.0%) research theme identified in the scoping review. Few studies have researched on issues of stigma and discrimination (7.6%), and no reported research was conducted on the implementation of policies and rights of persons with disabilities as stipulated in the 2006 Ghana’s Disability Act 715.
Further, most of the studies were observational in design (n = 70, 49.0%), and there were no experimental studies. Forty-eight (34.0%) studies had persons with disabilities as the primary study subjects. A significant number of studies had also focused on caregivers as the primary subjects (n = 25, 17.0%) and their role in providing care for persons with disabilities. In terms of sex, 130 (91.0%) articles were all gender inclusive (i.e. study participants included women and men), 13 (9.0%) articles had women only study participants, and no study was focused on men only. Fifty-two (36.4%) disability articles were from studies that were funded from external sources, and 24 (17.0%) were unfunded.
Research priority ranking surveys
Characteristics of participants
presents the demographic characteristics comparing participants who completed the first stage and those who completed the second stage. Participants across the two surveys had similar characteristics, except the type of expert; stage two had significantly fewer experts in the clinician pool. Across both surveys, there were significantly more participants aged between 25 and 44 years, with more males than females. The majority had a post-graduate education up to diploma or masters. A significant majority of the experts were clinicians, with 1 in 5 from Non-Governmental Organisations or civil society organisations.
Table 1. Socio-demographic characteristics of study participants in first and second-stage surveys.
Priority research areas
summarises the top 10 priority research questions, the corresponding broad research themes, CHNRI criteria scores, and recommended timelines for addressing the research questions. The majority of the top 10 priority research questions focused on health systems and interventions research with specific questions on scale-up of mental health and disability services. Experts also prioritised epidemiological questions to understand the consequences of stigma, and social determinants of mental health. Research questions around public health emergencies, such as COVID-19 and community engagement did not feature in the top 10 priority questions.
Table 2. Top 10 priority research questions and their thematic areas for Ghana.
Participants assigned almost equal importance to the five CHNRI priority rating criteria as applied to each research question. All of the top 10 research questions were considered urgent and should be conducted in the immediate and short term (0–5 years).
Priority mental health conditions
Participants in survey 2 also identified mental health conditions that need to be prioritised for research in Ghana. Almost half (47.5%) of the participants identified all the major mental, neurological and substance [Citation1] use conditions as needing equal prioritisation for research. However, for specific MNS conditions, research on depression (17.5%) was most prioritised, followed by substance use disorder (12.5%), epilepsy (10%), bipolar disorder (7.5%), and Schizophrenia (5%).
Research capacity survey
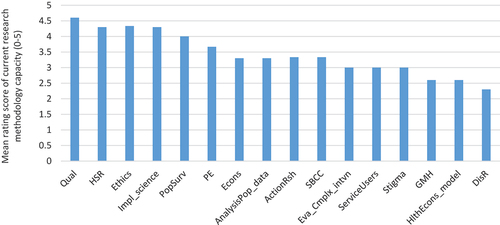
Directors of two of the three health researcher centres of Ghana Health Service, and a senior faculty member of a public university in Ghana provided responses for this survey. shows the mean research capacity score for each research domain. Six out of the 16 domains assessed were rated as weak to average (</ = 3) capacity for research. The remaining 10 domains were rated as above average to strong. As illustrated in the progressively decreasing bars, capacity for disability research (mean = 2.3; SD = 1.15), global mental health research (mean = 2.6; SD = 0.57), and health economics modelling (mean = 2.6; SDD = 1.15) was particularly weak.
Figure 3. Distribution of mean research capacity score by research domains.
Discussion
The top ten research priorities ranked by answerability, effectiveness, deliverability, equity and potential impact on burden of mental health conditions for Ghana include understanding the social determinants of mental health, scale-up and equitable access including human resources for mental health and disability services, and interventions for mental health and disability. These were identified within a context of constrained mental health and disability research output, informed by poor research methodology capacity, and slow increase in funding.
The gamut of illustrative research questions or aims can be summarised under three broad themes. First, the results underscore the importance of strengthening the understanding of the epidemiology of mental health conditions in Ghana. Questions around the aetiology of mental health conditions, with a particular emphasis on the social determinants of these conditions are recommended as needing immediate attention. Understanding and properly researching the epidemiology of mental health and other disabilities is an important goal because of the established links between physical and mental health; 46% of the people with a mental health condition also have a long-term physical condition, and the reverse is also well documented with 30% with long term physical conditions having a mental health condition [Citation36]. But also, because we still do not know how co-morbidities interact with each other and with social factors [Citation10]. These multi-morbidities have economic costs [Citation37,Citation38]. Second, our results strongly support a health systems and policy approach to mental health services. Experts supported urgent research that supports the scale-up of mental health and disability services. An important related question worth researching is how to improve equitable (sex/place of residence/socioeconomic status) access to mental health and disability services. This is also supported by the findings from our rapid review that suggest the lack of studies that examine disaggregated effects, and few studies (only four studies) that address challenges with the woefully inadequate mental health workforce in Ghana. These are important goals for Ghana and many LMICs given the widely recognised major challenges in reaching all the people who need care and support, as well as enabling them timely access to evidence-based treatment and support [Citation10,Citation39]. Research in scaling up mental health and disability services would lessen the effect of stigma and discrimination on timely access to mental health services [Citation40].
Experts further recommended research questions around human resources for mental health services delivery. For example, the role of cadres of mental health professionals, such as community mental health officers in providing mental health services was identified as an important research question. Third, our results clearly identify the key role of intervention development, implementation, and evaluation as a priority research area in Ghana. Experts were particularly keen on research that compares the effectiveness of community-based versus facility-based approaches for the treatment and management of mental health conditions. These priority areas of research for Ghana are in step with the current thinking of Global Mental Health; the thematic areas align with recommendations from the Grand Challenges of Global Mental Health research report [Citation20], and the Lancet Commission on Global Mental Health and Sustainable Development [Citation3]. The priority research thematic areas identified for Ghana are consistent with other reports from South America (Brazil and Chile) [Citation21,Citation22], and importantly, also the mental health research agenda policy of the Mental Health Authority of Ghana. To illustrate, in the Brazil study, 4 out of the top 10 ranked research priorities relate to intervention studies (effectiveness, cost-effectiveness, and policy); intervention studies were also identified as high priority in Ghana. A notable point of difference is the prioritisation of research on mental health and disability policy and legislation with a focus on human-rights; this was an explicit priority for Ghana but not Brazil and Chile. The interest in research around human rights in Ghana was probably influenced by WHO’s quality rights in mental health project that has attracted a good amount of interest in Ghana [Citation41].
The results of this priority-setting agenda for Ghana are to a large extent reflective of the mental health and disability research profile of Ghana for the 10-year period between 2010 and 2020. Our rapid review and research capacity survey show clear gaps that can benefit from the formulated research agenda in this study. First, peer-reviewed mental health and disabilities research has not improved since 2010, and the research agenda provides an important framework to help reverse this trend in the next 10 years. Second, the priority for intervention studies if heeded will be important to address the deficit of intervention studies, currently at only 3% for mental health and 0% for disabilities research. Third, and quite relevant to point two, there is a clear lack of both methodological and local funding capacity to design and conduct Global Mental Health and disability research in Ghana; the research agenda identifies some priorities if this trend is to be reversed in the next 10 years.
Our study has several strengths. This is the first study in Ghana to systematically document and report on a priority-setting agenda, adopting a rigorous participatory methodology. Priority-setting methodology needs to reflect the context [Citation14] and country-specific needs [Citation15,Citation16], and our rapid review provided this crucial information and a useful validation of the identified priority areas; previous priority-setting studies have been unable to do this. We also addressed the issue of time-framing as an important parameter in judging the urgency with which to tackle important research questions; this is additionally useful for planning around allocation of funding for research. Further, we validated the findings from the first step of the priority-setting survey and the rapid review with key stakeholders in a workshop before proceeding to the ranking stage. In addition, our selection of experts was systematic and based on an existing local directory of mental health civil society organisations and NGOs. Finally, we employed the CHNRI methodology, an objective and widely used priority ranking tool. The CHNRI criteria have content validity for use in the Ghanaian context and are assigned equal importance in determining mental health and disability research priorities.
Nevertheless, we note several limitations for course-correction in the future. First, the response rate (58%) for the priority ranking was encouraging compared to other similar studies in Brazil (56%) and Chile (36%) but not optimal. The potential for response bias and a threat to the internal validity of our results cannot be ruled out. Second, in our attempt to reduce the number of initial submissions of research questions and improve the response rate for the ranking survey, the research team pruned and grouped questions. We may have missed important questions and thus introduced a systematic error in the choice of response options. Third, we were unable to follow through with our planned qualitative interviews with experts for the research capacity survey. This was entirely due to COVID-19 restrictions at the time. These limitations notwithstanding, our approach is a significant improvement over previous studies, and the first report of this kind in the sub-Saharan Africa region.
Conclusion
We conclude with thoughts on the approach and implications. Our approach to the research priority-setting agenda for Ghana shows it is feasible to employ a systematic participatory methodology that includes key parameters of context and research methodology capacity. We encourage maintaining this process of setting research priorities. The implications of our priority-setting results indicate a strong and urgent need to focus on well-funded research areas that have the potential to significantly reduce the burden of MNS disorders and the wide treatment gap of 98%. This could be achieved if we move beyond priority setting exercises, which are without doubt promising for surfacing vital evidence, to identify clear goals and measurable targets [Citation10].
Author contributions
Conceptualization: BW, CL. Data acquisition: BW, KA, GM, LS. Data analysis: BW, KA, GM. Data interpretation: BW, KA, GM, CL. Drafting: BW. Critical revision: BW, KA, GM, LS, CL. All authors read and approved the final manuscript.
Ethics and consent
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Paper context
Evidence before this study
There are several published methods describing different approaches for setting priorities for health research. Little is known about how to strengthen standard research prioritization processes with key contextual information such as level of research activity, capacity, and funding.
Added value of this study
This study is the first to report findings on how to use a scoping review to enhance standard research prioritization processes.
Implications of the findings
Ghana’s context-informed research agenda provides an important framework to identify the most pressing mental health challenges.
Supplemental Material
Download MS Word (21.7 KB)Acknowledgements
This study is an output of the Ghana Somubi Dwumadie (Ghana Participation Programme- [email protected]). We thank the following Ghana Somubi Dwumadie partners: Options (Alice Tilton, Lyla Adwan-Kamara) for their roles in reviewing the research priorities report used for the validation meeting and their comments on drafts of this paper. We thank all the participants who contributed data for this study.
Disclosure statement
None of the authors have any competing interest
Supplementary Material
Supplemental data for this article can be accessed online at https://doi.org/10.1080/16549716.2022.2112404.
Additional information
Funding
References
- Njamnshi AK, Bissek A-CZ-K, Yepnjio FN, et al. A community survey of knowledge, perceptions, and practice with respect to epilepsy among traditional healers in the batibo health district, Cameroon. Epilepsy Behav. 2010;17:95–12. Epub 2009/11/22. PubMed PMID: 19932640.
- GBD, Collaborators M. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet Psychiatry. 2022;9:137–150. Epub 2022 Jan 10. PubMed Central PMCID: 35026139; PMCID: PMC8776563.
- Patel V, Saxena S, Lund C, et al. The Lancet Commission on global mental health and sustainable development. Lancet. 2018;392:1553–1598. Epub 2018/10/14. PubMed PMID: 30314863.
- Eaton J, Ohene S. Providing Sustainable Mental Health Care in Ghana: A Demonstration Project. In: Forum on Neuroscience and Nervous System Disorders; Board on Health Sciences Policy; Board on Global Health; Institute of Medicine; National Academies of Sciences, Engineering, and Medicine. Providing Sustainable Mental and Neurological Health Care in Ghana and Kenya: Workshop Summary. Washington (DC): National Academies Press (US); 2016 Feb 25. F.
- Thornicroft G, Cooper S, Bortel TV, et al. Capacity building in global mental health research. Harv Rev Psychiatry. 2012;20:13–24. Epub 2012/02/18. PubMed PMID: 22335179; PubMed Central PMCID: PMC3335140.
- CHRD. Commission for Health Research and Development: essential link to equity in development. New York: Oxford University Press; 1990.
- Saxena S, Lora A, Morris J, et al. Mental health services in 42 low- and middle-income countries: a WHO-AIMS cross-national analysis. Psychiatr Serv. 2011;62:123–125. Epub 2011/02/03. PubMed PMID: 21285088.
- Betancourt TS, Chambers DA. Optimizing an era of global mental health implementation science. JAMA Psychiatry. 2016;73:99–100. Epub 2016/01/01. PubMed PMID: 26720304.
- AMS. Challenges and priorities for global mental health in the sustainable development goals (SDG) era- Workshop report. London: The Academy of Medical Sciences, 2018.
- Wykes T, Bell A, Carr S, et al. Shared goals for mental health research: what, why and when for the 2020s. J Ment Health. 2021;1–9. Epub 20210509. doi: 10.1080/09638237.2021.1898552. PubMed PMID: 33966543.
- Saxena S, Paraje G, Sharan P, et al. The 10/90 divide in mental health research: trends over a 10-year period. Br J Psychiatry. 2006;188:81–82. PubMed PMID: 16388075.
- Saraceno B, Saxena S. Bridging the mental health research gap in low- and middle-income countries. Acta Psychiatr Scand. 2004;110:1–3. PubMed PMID: 15180773.
- WHO. Priority setting methodologies in health research. Geneva: World Health Organisation; 2008.
- Terry RF, Charles E, Purdy B, et al. An analysis of research priority-setting at the world health organization - how mapping to a standard template allows for comparison between research priority-setting approaches. Health Res Policy Syst. 2018;16:116. Epub 20181129. PubMed PMID: 30486845; PubMed Central PMCID: PMC6264050.
- WHO. The world health report. Research for universal health coverage. Geneva: World Health Organisation, 2013.
- Lancet Global Mental Health G, Chisholm D, Flisher AJ, Lund C, et al. Scale up services for mental disorders: a call for action. Lancet. 2007;370:1241–1252. Epub 2007/09/07. PubMed PMID: 17804059.
- Tomlinson M, Chopra M, Hoosain N, et al. A review of selected research priority setting processes at national level in low and middle income countries: towards fair and legitimate priority setting. Health Res Policy Syst. 2011;9:19. Epub 20110515. PubMed PMID: 21575144; PubMed Central PMCID: PMC3115910.
- Reveiz L, Elias V, Terry RF, et al. Comparison of national health research priority-setting methods and characteristics in Latin America and the Caribbean, 2002-2012. Rev Panam Salud Publica. 2013;34:1–13. PubMed PMID: 24006014.
- WHO’s Global Health R&D Observatory [Internet]. 2013 [cited 2022 Mar 20]. Available from: https://www.who.int/observatories/global-observatory-on-health-research-and-development.
- Collins PY, Patel V, Joestl SS, et al. Grand challenges in global mental health. Nature. 2011;475:27–30. Epub 2011/07/08. PubMed PMID: 21734685; PubMed Central PMCID: PMC3173804.
- Gregorio G, Tomlinson M, Gerolin J, et al. Setting priorities for mental health research in Brazil. Braz J Psychiatry. 2012;34:434–439. PubMed PMID: 23429814.
- Zitko P, Borghero F, Zavala C, et al. Priority setting for mental health research in Chile. Int J Ment Health Syst. 2017;11:61. Epub 20171002. PubMed PMID: 29026439; PubMed Central PMCID: PMC5625763.
- GoG. MENTAL HEALTH ACT, 2012 AN ACT to provide for mental health care and for related matters. In: Health Mo, editor. Accra, Ghana; 2012.
- RDD. Ghana national health research agenda (2015-2019) Accra: Ghana Health Services, 2015.
- GoG. PERSONS WITH DISABILITY ACT, 2006 AN ACT to provide for persons with disability, to establish a National Council on Persons with Disability and to provide for related matters. Ministry Gender, Children and Social Protection. In: MoGCSP, editor. Accra (Ghana); 2006.
- GSD. Ghana Somubi Dwumdie: a four-year disability inclusion programme in Ghana 2021 [cited 2021 Dec 12]. Available from: https://www.ghanasomubi.com.
- Viergever RF, Olifson S, Ghaffar A, et al. A checklist for health research priority setting: nine common themes of good practice. Health Res Policy Syst. 2010;8:36. Epub 20101215. PubMed PMID: 21159163; PubMed Central PMCID: PMC3018439.
- Montorzi G, de Haan S, IJsselmuiden C. Priority setting for research for health: a management process for countries. In: Council on Health Research for Development (COHRED), editor. Geneva (Switzerland); 2010.
- Rudan I, Gibson JL, Ameratunga S, et al. Setting priorities in global child health research investments: guidelines for implementation of CHNRI method. Croat Med J. 2008;49:720–733. PubMed PMID: 19090596; PubMed Central PMCID: PMC2621022.
- Ghaffar A, Francisco A, Matlin S. The Combined Approach Matrix: a priority-setting tool for health research. Geneva: JOUR; 2003.
- Ghaffar A. Setting research priorities by applying the combined approach matrix. Indian J Med Res. 2009;129:368–375. PubMed PMID: 19535830.
- Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169:467–473. Epub 20180904. PubMed PMID: 30178033.
- Read UM, Adom-Boakye NA. Mental health resource directory Ghana. 2020.
- Semrau M, Alem A, Abdulmalik J, et al. Developing capacity-building activities for mental health system strengthening in low- and middle-income countries for service users and caregivers, service planners, and researchers. Epidemiol Psychiatr Sci. 2018;27:11–21. Epub 2017/10/03. PubMed PMID: 28965528; PubMed Central PMCID: PMC6998877.
- Tomlinson M, Rudan I, Saxena S, et al. Setting priorities for global mental health research. Bull World Health Organ. 2009;87:438–446. Epub 2009/07/01. PubMed PMID: 19565122; PubMed Central PMCID: PMC2686213.
- Naylor C, Parsonage M, McDaid D, et al. Long term conditions and mental health: the cost of co-morbidities. The King’s Fund and Centre for Mental Health. 2012.
- Ismail K, Winkley K, Stahl D, et al. A cohort study of people with diabetes and their first foot ulcer: the role of depression on mortality. Diabetes Care. 2007;30:1473–1479. Epub 20070315. PubMed PMID: 17363754.
- Zuidersma M, Ormel J, Conradi HJ, et al. An increase in depressive symptoms after myocardial infarction predicts new cardiac events irrespective of depressive symptoms before myocardial infarction. Psychol Med. 2012;42:683–693. PubMed PMID: 22571951.
- Weobong B, Ae-Ngibise K, Sakyi L, et al. Towards implementation of context-specific integrated district mental health care plans: a situation analysis of mental health services in five districts in Ghana (Preprint). Int J Ment Health Syst. 2021. DOI:10.21203/rs.3.rs-1175369/v1
- Marshall M, Lewis S, Lockwood A, et al. Association between duration of untreated psychosis and outcome in cohorts of first-episode patients: a systematic review. Arch Gen Psychiatry. 2005;62:975–983. PubMed PMID: 16143729.
- WHO. World Health Organization. QualityRights in mental health, Ghana. 2019 [cited 2022 Jul 06]. Available from: https://qualityrights.org/in-countries/ghana/.
