
Abstract
Introduction: UNAIDS’ Vision 90:90:90 is a call to ‘end AIDS’. Developing predictive foresight of the unpredictable changes that this journey will entail could contribute to the ambition of ‘ending AIDS’. There are few opportunities for managing unpredictable changes. We introduce ‘weak signal detection’ as a potential opportunity to fill this void. Method: Combining futures and complexity theory, we reflect on two pilot case studies that involved the Archetype Extraction technique and the SenseMaker® Collector™ tool. Results: Both the piloted techniques have the potentials to surface weak signals – but there is room for improvement. Discussion: A management response to a complex weak signal requires pattern management, rather than an exclusive focus on behaviour management. Conclusion: Weak signal detection is a window of opportunity to improve resilience to unpredictable changes in the HIV/AIDS landscape that can both reduce the risk that emerges from the changes and increase the visibility of opportunities to exploit the unpredictable changes that could contribute to ‘ending AIDS’.
Résumé
Introduction: L'ONUSIDA’ Vision 90:90:90 est un appel à ‘“mettre fin au SIDA”. Développement de prospects prédictives des changements imprévisibles ce voyage entraînera pourrait contribuer. Il y a peu de possibilités de gestion des changements imprévisibles. Nous introduisons »la détection de signaux faibles' comme une opportunité potentielle de combler cette lacune. Méthode: combinant la science des futures et la théorie de la complexité nous réfléchissons sur deux études de cas pilotes qui impliquent la Technique d'Extraction d'Archétype et l'outil SenseMaker® Collector™. Résultats: les deux techniques pilotes ont le potentiel de faire surface aux signaux faibles – mais il y a de la place pour de l'amélioration. Discussion: la gestion d'un signal faible complexe nécessite une gestion de formes, plutôt que de se concentrer exclusivement sur les modes de comportement. Conclusion: détection des signaux faibles constitue une fenêtre d'opportunité pour améliorer la résilience aux changements imprévisibles qui surviennent dans le paysage SIDA qui peuvent à la fois réduire le risque qui émerge de ces changements et accroître la visibilité des opportunités à exploiter les changements imprévisibles qui pourraient contribuer à « mettre fin au SIDA”.
Introduction
In 2014, UNAIDS produced two hard-hitting reports that focus on ‘ending AIDS’. One of the reports – The Gap Report – asks the question: ‘How do we close the gap between the people moving forward and the people being left behind?’ and then says: ‘We have a fragile five-year window [2015–2020] to build on the rapid results that have been made. The next five years will determine the next 15 [of the trajectory of the epidemic]’ (UNAIDS Citation2014b:iv–v). The other report – Fast Track – reinforces these points before providing a global overview of what has been achieved – and what is required – to ‘end AIDS’. The overarching ambition, which was agreed at the International AIDS Conference in Australia, 2014, is known as ‘Vision 90:90:90’ (UNAIDS Citation2014a:iii), which means ‘90% of people know their status; 90% of those that are HIV positive are on treatment; 90% of those on treatment are virally suppressed’ (Motsoaledi Citation2014). The reason for this re-orientation is that it has been predicted that ‘without scale-up [to 90:90:90], the AIDS epidemic will continue to outrun the response, increasing the long-term need for HIV treatment and increasing future costs’ (UNAIDS Citation2014a:4).
The South African National Department of Health (NDoH) has embarked on an expanded combination prevention approach as a contribution to achieving the global ambition of ‘ending AIDS’. Combination strategies that fit local contexts is now the sine qua non of HIV prevention because ‘[biomedical] HIV programmes are dramatically strengthened when they are combined with social and structural approaches’ (UNAIDS Citation2014a:6; also see Hankins and de Zalduondo Citation2010).
In South Africa, the Vision 90:90:90 ambition means a significant scale up of existing measures being taken to reduce the aggregate national viral load that is inclusive of treatment, behavioural, structural and educational measures (Motsoaledi Citation2014). This initiative is extremely welcome, but one that we suggest will be fraught with implementation challenges as the South African healthcare system rolls out these different, inter-related initiatives within such a compressed – ‘five year’ – time-frame.
We will argue that the concept of ‘weak signal detection’ can add value to the management of the next five years of the HIV/AIDS landscape because Vision 90:90:90 requires accelerated combination interventions and a social transformation in the uptake of these opportunities.
In order to make this argument, we will explore the notion of weak signal detection before reflecting on our own – albeit localised and imperfect – experiences of piloting weak signal detection. Our own experiences revealed that while weak signal detection efforts can add value to working in localised contexts, the methods are sometimes imprecise and demanding – as other commentators have noted (Rossel Citation2012). Despite these challenges, we will argue that there is both practical and strategic utility in improving the techniques and applying the approach at different scales as a contribution to achieving Vision 90:90:90.
The conceptual foundations of the article are represented in .
Fig. 1. The conceptual foundations. Source: authors’ contribution.
The theoretical framework is influenced by concepts transposed from complexity theory and futures science and, through this kaleidoscope, we will argue that the approach can contribute to achieving Vision 90:90:90 by building national resilience in the form of both anticipatory surveillance capacity and an adaptive response capacity. We will also suggest that it is possible to strategically align these processes to the NDoH's eHealth vision of facilitating ‘real-time information for decision-making’ (NDoH Citation2012:5).
Dynamic adaptive landscapes
As has been noted above, UNAIDS is calling for a seismic shift so that the possibility of ‘ending AIDS’ by 2030 becomes a reality. In the last 30 years of the epidemic, there have been macro-, meso- and micro-changes in the epidemiological landscape and, as with many epidemics (Galea, Riddle & Kaplan Citation2010), the complexity of these processes has been confounding (Stillwaggon Citation2012). Despite a call that was made almost a decade ago to embrace these complexities (Piot, Bartos, Larson, Zewdie & Mane Citation2008), the HIV/AIDS landscape continues to be one that is turbulent and difficult to negotiate. It is logical to begin our discussion from the premise that we cannot expect the next five years to be less turbulent – which is why UNAIDS warns that a complacent ‘business as usual’ approach (UNAIDS Citation2014b:242) risks the ‘epidemic springing back even stronger’ (Citation2014a:iii).
A dynamic South African AIDS landscape
Many of the changes in the South African HIV/AIDS landscape have been triggered by the NDoH's – and other organisations' – efforts to address the epidemic. Significant results are now occurring across the nation (Shisana et al. Citation2014) – yet unexpected changes have also occurred: for example, ‘overall condom use at last sex increased significantly from 2002 to 2008 and then significantly decreased in 2012 among all three age groups and for both sexes except among females aged 50 years and older’ (Shisana et al. Citation2014:xxxiv). This type of unexpected change undermines the NDoH's plans for reducing the aggregate national viral load – making this unpredictable component of the landscape relevant if Vision 90:90:90 is to be achieved.
Not only is the HIV/AIDS landscape influenced by the way in which interventions intersect with local communities and the way in which communities – and the localised ‘sensori-memorabilia’ within those communities (Burman, Mamabolo, Aphane, Lebese & Delobelle Citation2013:22) – respond to interventions; it is also influenced by other dynamic networks such as migration (Lurie & Williams Citation2014), drug resistance (Rossouw Citation2014) and interconnected chronic health challenges (Deeks, Lewin & Havlir Citation2013). We therefore suggest that it is logical to conceptualise the landscape as being a complex, adaptive epidemiological landscape and the implications of this claim are explored below.
HIV/AIDS and complexity theory
Increasingly, direct and indirect links are being made between healthcare and complexity (Carey & Crammond Citation2015; Jayasinghe Citation2011; Martin, Grady, Deaconking, McMahon, Zarabzadeh, & O'Shea Citation2011). Complexity theory is an integrated and interdisciplinary perspective that views both natural and social phenomena as dynamic, interactive, patterned, yet sometimes unpredictable, and interconnected relational processes contained within a system of interest (Stacey Citation1996) – with ‘complexity’ referring ‘to the nature of the problem not the degree of difficulty’ (Stirzaker, Biggs, Roux & Cilliers Citation2010:600). Typically, complexity is situated in a system known as a complex adaptive system – which has been summarised in the following way ().
Table 1. Complex Adaptive Systems.
shows that complexity theorisers emphasise processes, relationships and uncertainty rather than relying exclusively on a positivist cause and effect, problem and solution, linear logic enabling an expansive ‘multi-ontology’ perspective (Snowden Citation2005). Another opportunity provided by complexity is the distinction between ordered and unordered properties of a system (Kurtz & Snowden Citation2003). Ordered properties of a system are those properties which can be categorised as ones with discernible links to Newtonian ‘cause and effect’. Unordered properties tend to be ones where the ‘cause–effect’ link is indeterminate and causality is only discernible in retrospect.
HIV/AIDS: a complex adaptive epidemiological landscape?
Almost a decade ago, it was argued that it is necessary to work with the complexity of the HIV/AIDS landscape, rather than ignore it. This requires a new set of methodologies and strategies to shift linear models and paradigms to ones that are able to construct ‘analytical tools … to capture these dynamics’ (Piot et al. Citation2008:853), also see Leach, Scoones and Stirling (Citation2010).
Since that time there have been limited – but diverse – responses to the call to apply complexity theory to the HIV/AIDS epidemic (Burman, Aphane & Delobelle Citation2015; Burman, Aphane, Mtapuri & Delobelle Citation2015; Burman, Moerschell, Mamabolo, Aphane & Delobelle Citation2015; Fiorella Citation2013; Lich, Ginexi, Osgood & Mabry Citation2013; Silvestri Citation2013). Situated amongst the call for new tools and methodologies and attempts to articulate responses have been some compelling critiques of HIV/AIDS policies and approaches that ignore these complexities (Nguyen, Bajos, Dubois-Arber, O'Malley & Pirkle Citation2011; Stillwaggon Citation2012). For the purposes of developing our argument, we focus on two key concepts drawn from complexity theory – emergence and autopoiesis.
Emergence
Emergence and autopoiesis are key themes that have dominated complexity theory for over half a century (Weaver Citation1948). Emergence, in this context means ‘when bringing together component parts results in something that simply could not have happened, and situations where, from a human point of view, something novel and surprising appears from a situation that is not even suggestive of this novelty’ (Galatzer-Levy Citation2002:708). Emergence – as used by complexity theorists – means the phenomena that arise from interactions of systems may either be novel forms of emergence or forms of emergence that are long-term phenomena.
Typically, this involves a process when the intersection of new, or existing, systems creates weak interconnections – including feedback – between, or within, system components. Interconnections may at first be random and are thus short-lived, but sometimes the interconnections develop into interdependencies that take on self-sustaining, autopoietic lives of their own – as Weaver (Citation1948:538) hinted at in his conceptualisation of ‘organised complexity’ that ‘involve[s] a sizeable number of factors which are interrelated into an organic whole … .not in a helter skelter fashion [as in disorganised complexity]’ in 1948 (emphasis in original).
Autopoiesis
Autopoiesis is an expression first used in the 1970s to explain the way in which cells self-sustain and self-organise themselves as an adaptive survival mechanism (Maturana & Varela Citation1980). The expression – not without its detractors (Tastle Citation1992) – has gradually been incorporated into the lexicon of complexity theory (Cilliers Citation1998, Citation2005; Luhmann Citation1995) and is used to denote the way in which ‘[t]hrough successive repetition a system achieves autopoiesis, a process that transforms itself into itself through recursive closure that is regulated by communication’ (Hatt Citation2008:320). From recurrent patterned connections, and associated feedback loops, behaviours or phenomena occur that transforms a weakly connected ‘self’ into a qualitatively different – and sustainable – ‘locked-in self’ (Vergne Citation2013) that moves from a state of unstable interconnections towards a state of stabilised interdependency. Patterned interdependencies create visible, surface descriptors that are outcomes of the relationships amongst different components of a system. These interdependencies result in visible recurrences, such as crowd surging or flocking birds, once they have developed sustainable, interdependent relationships (Ramalingham Citation2013). Interconnections, on the other hand, only produce short-lived phenomena (Hatt Citation2008).
From the perspective of the HIV/AIDS epidemic, some visible patterns contribute to sustaining the epidemic by enabling the virus to replicate and migrate from one human body to another – such as non-adherence to antiretroviral medication (Stricker et al. Citation2014) and inconsistent condom use (Shisana et al. Citation2014). Other visible patterns contribute to ‘ending AIDS’ by dampening the ability of the virus to replicate and successfully migrate from one body to another – such as adherence to antiretroviral medication (Rodger, Bruun & Cambiano Citation2014); consistent and appropriate condom use (Merson, O'Malley, Serwadda & Apisuk Citation2008) and prevention of mother-to-child transmission in South Africa (Barron et al. Citation2013).
The patterns that enable, or hinder, the ability of the HI virus to replicate – thereby influencing the trajectory of the epidemic – typically involve multiple interactions between different parts of the epidemiological system and the interactions are ‘complex’ because ‘at least some of these components have non-linear relationships between them’ (Stirzaker et al. Citation2010) ().
Fig. 2. The virus–human–environment ‘system’ – complex patterned interactions create emergent phenomena associated with HIV/AIDS. Source: Burman, Aphane & Delobelle (Citation2015:16).
provides a generic representation of the complexity that the epidemic displays. Autopoietic interdependencies and feedback within and between the ‘virus–human–environment system’ produces emergence that sustain the epidemic – and has simultaneously influenced the historical identities of the epidemic. More-often-than-not, responses to the epidemic are triggered by – and respond to – patterned, visible forms of emergence ().
Table 2. Phenomena that emerge from within components or between components of the human–virus–environment heuristic.
Autopoietic interdependencies that defy easy explanation through traditional Newtonian science – especially when they intersect at multiple scales – are central to grappling with the unexpected outcomes of a particular series of complex events (Lorenz Citation1972; Walby Citation2007) (see , column 4). One of the more successful attempts at dealing with these complex relationships is the way in which periconception decision-making amongst serodiscordant, or discordant, couples is now managed in South Africa – although it is –as yet–an imperfect process (Barker, Barron, Bhardwaj & Pillay Citation2015; Matthews et al. Citation2013). However, from a complexity perspective, many of the ‘extraordinary changes in the AIDS landscape achievements’ (UNAIDS Citation2014b) can be attributed to the deliberate management of patterns that sustain phenomena that influence the trajectory of the epidemic.
Typically, a new intervention typology has the effect of replacing one set of patterns that enable the virus to replicate, with a new set of patterns that reduce the virus’ ability to flourish. In the early stages of the intervention, the new patterns demonstrate weak interconnections, but with time – through the process of autopoiesis – the relationships that hold successful interventions together develop into self-energising interdependencies. Autopoiesis is the process that strengthens novel connections as they mature into interdependent forms of emergence and is thus a critical mediator of intervention success or failure.
Many interventions indirectly reinforce the process of autopoiesis by focusing on the visible, surface descriptors of change – such as health promotion campaigns, but, as far as we are aware, there is no evidence that any interventions deliberately attempt to identify weak signal indicating shifts in patterned interactions or interdependencies; nor are there management strategies within the HIV/AIDS landscape designed to respond to these changes. It is for this reason that we now turn to weak signal detection and the Cynefin framework (Snowden & Boone Citation2007).
Weak signal detection
Weak signal detection – first coined by Ansoff (Citation1975) in ‘Managing Strategic Surprise by Response to Weak Signals’ – is an ongoing process of scanning an environment for clues that indicate that discrete changes in the environment are occurring. For futures scientists, detecting any evidence of novel emergence is described as a ‘weak signal’ – ‘(external or internal) events and developments that are still too incomplete to allow an accurate estimate of their impact and/or to determine a full adapted response [are detectable]’ (Ansoff Citation1975, cited in Sidhom & Lambert Citation2011:40). Weak signal detection is a method that illuminates – or surfaces – the development of new interconnections; existing interconnections or interdependencies and changes in the strengths, or influence, of the interconnections between and within the system – and is thus an opportunity to identify opportunities to influence the trajectory of the epidemic, albeit working at discrete scales.
The reason for scanning the environment for these discrete changes is that these changes hold the potentials to develop into more significant phenomena as they intersect with a planned ambition. This intersection – if it co-evolves into a significant phenomenon – has the potential to either reinforce the planned vision, or to obstruct it. Futures scientists have been devising and documenting mechanisms to better understand and improve weak signal detection (Harris & Zeisler Citation2002; Kaivo-oja Citation2012; Sidhom & Lambert Citation2011) so that foresight can be developed and responded to, based on their understandings of the process of autopoiesis (Mendonça, Cardoso & Caraça Citation2012).
The significance of detecting weak signals is that when working with complex adaptive systems it is possible at particular historical junctures to show – or at least identify clues – that a change process is beginning which may require a management response. Differentiating between the types of management response to weak signals is the next issue to be addressed.
Management responses to ‘weak signals’
In a seminal article called ‘A Leader's Framework for Decision Making', Snowden and Boone (Citation2007) argue that many decisions can be improved by correctly identifying the context within which decisions are being made — called the Cynefin framework (). The framework is influenced by the work of Klein (Citation2008:457), who described how people make decisions using the ‘recognition-primed decision (RPD) model [which] describes how people use their experience in the form of a repertoire of patterns’. Specifically, Klein suggests that when people want to make a decision and ‘can quickly match the [decision making] situation to the patterns they have learned’ they typically take this first option – rather than take stock of the situation and make a decision based on a more holistic scanning of the context within which the situation is embedded (Klein Citation2008:457).
Fig. 3 The Cynefin framework. Source: http://en.wikipedia.org/wiki/Cynefin.
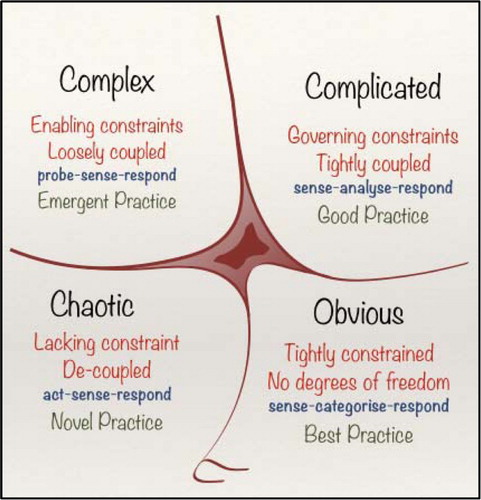
Snowden and Boone's work provides a heuristic that decision-makers can apply to evaluate the contextual situation prior to making a decision – thus avoiding the ‘first pattern fit’ that could lead to an inappropriate decision. The heuristic is split into four quadrants which represent different decision-making contexts. The ‘obvious’ and ‘complicated’ quadrants represent the realm of ordered Newtonian science where decision-making is constrained by rationality because cause and effect is discernible. The ‘complex’ and ‘chaotic’ domains represent ‘unordered’ contexts where the constraints of rationality are lifted – by different degrees – because cause and effect is only discernible in retrospect, which means that ‘the agents and the system constrain one another, especially over time. This means that we cannot forecast or predict what will happen’ (Snowden & Boone Citation2007:70).
In the ‘unordered’ contexts, it is ‘futile’ to look for solutions to problems based on the presumptions associated with the ‘ordered’ Newtonian legacy (Wilson & Holt Citation2001). There is a fifth domain situated in the middle of the Cynefin framework called ‘disorder', where no consensus as to the nature of the problem dominates. Each of the domains contains generic management responses that are appropriate to the different domains and can be applied to a generalised HIV/AIDS epidemic ().
Table 3. The Cynefin framework and HIV/AIDS.
Each decision is prompted by a signal. Some signals prompt clearly defined management responses because the solution is already known; other signal responses are more ‘complicated’ because the solution is available, but elusive; other signal responses are ‘complex’ because there is no known solution and some signal responses require crisis management because the situation is ‘chaotic’ and requires stabilisation prior to managing it.
At first glance, applying this framework to the HIV/AIDS landscape suggests that many of the challenges associated with ‘ending AIDS’ are now realisable. However, in the naturalistic, ‘real-world’, contexts of interdependencies and interconnections that enable the virus to flourish – the situation points to ambiguity (see ). The ambiguity contained within points to the inherent complexity of managing a generalised epidemic and emphasises the importance of the fifth – disordered – domain of the Cynefin framework. ‘The way out of this realm is to break down the situation into constituent parts and assign each to one of the other four realms. Leaders can then make decisions and intervene in contextually appropriate ways’ (Snowden & Boone Citation2007:71).
Overview of the above
Influenced by future scientists’ interest in anticipatory awareness of what might occur in the future – and UNAIDS’ Vision 90:90:90 of what could occur by 2030 – we have introduced some concepts that include landscapes in transition and complexity theory, including emergence and autopoiesis. Emergence tells us something about what can happen when systems intersect – but not about the potential impact of that emergence. Autopoiesis is the glue that turns weak interconnections into patterned – long term – interdependencies that generate sustainable phenomena. We have thus argued that visible, surface descriptors associated with the HIV/AIDS landscape are sustained by less visible patterns of interactions and that some of these patterns are robust, ‘organised’ autopoietic patterns, after Weaver (Citation1948), and other patterns are weaker – or ‘disorganised’ – but could coalesce into organised patterns as they intersect with the epidemiological landscape (Ansoff Citation1975).
Managing these patterns could contribute to achieving Vision 90:90:90 and so we introduced two implementation frameworks – weak signal detection and the Cynefin framework. Weak signal detection, albeit in imperfect form, has been used to improve ‘decision-making’ using foresight in a many different contexts (Kaivo-oja Citation2012). The Cynefin framework is a decision-making heuristic that enables appropriate management responses to signals. Combining weak signal detection with the Cynefin framework represents an avenue for introducing these concepts into the management of complex, adaptive HIV/AIDS landscapes. From this theoretical position, we now turn to our own field experiences of identifying and responding to weak signals.
Case material
Two case studies are presented. The case studies were undertaken in the Limpopo Province of South Africa during 2011–2013. The work took place in a community of approximately 35,000 people called Ga-Dikgale in the Capricorn district. The case studies include techniques that are believed to offer opportunities to surface weak signals and the more discrete properties of the system of interest. The first approach that was piloted is called Archetype Extraction and the second involved the use of the SenseMaker® Collector™ tool (Raford Citation2012).
Ethics approval
All research ethics were observed in conducting the study. Prior to both rounds of data collection, permission for ethical clearance was obtained from the Turfloop Research and Ethics Committee, University of Limpopo. The participants were assured of their anonymity and confidentiality before both written and verbal consents were obtained from them to take part in the study.
Archetype extraction
Archetype extraction involves eliciting micro-narratives from a group of people about a specific theme and asking them to ‘make sense’ of the experience (James & Minnis Citation2004). Narrative investigations are considered to be a mechanism to surface ‘tacit knowledge’ – after Nonaka and Takeuchi (Citation1995) –based on the assumption that narrative is the ‘bridge between tacit and explicit knowledge’ (Linde Citation2001:160). For the purposes of the pilots, the focus was on any tacit influence – rather than just knowledge – that shaped the feedback patterns within a particular system of interest.
The methodology is based upon a two-step process. The first step is called the Discovery Phase, based on a group discussion called an Anecdote Circle Anecdote Circle and the second phase is the Sense-Making Phase. The Discovery Phase elicits the visible phenomena the participants associate with the theme under discussion, including characters, behaviours and places. The Sense-Making Phase is designed to surface the less-visible themes that the participants associate with the phenomena identified in the Discovery Phase, such as enabling or constraining values, assumptions and biases that are ‘tacitly’ associated with the visible phenomena, which become the basis of the archetypes. Once the archetypes have been constructed by the participants, they are named and an artist is then requested to sketch the archetype – as directed by the participants. All of the findings are coded throughout the process so that links between the archetype and the earlier phases can be identified during the analysis. For a detailed account of the process, see Maree, Roux and Marais (Citation2006).
It is claimed that from this technique ‘representations of culture’ – including the patterns that sustain a particular cultural form – are surfaced (Snowden Citation2002:4). Six pilots were undertaken over an 18-month period with participants comprising male and female groups between the ages of 18 and 24 that work in drop-in-centres. Each group was composed of no more than 25 people. The focus of each workshop was HIV/AIDS and the local community. The findings of the Archetype Extraction technique were then situated on the Cynefin framework by the research team so that a contextualised management response was prepared.
SenseMaker®
In this case study, an attempt was made to surface development-related issues from people in rural Limpopo using the SenseMaker® Collector™ tool – not just HIV/AIDS-related issues. SenseMaker® is capable of managing vast amounts of data which can be retrieved in real-time. In this instance, over 1000 respondents were asked to provide micro-narratives that were based on empirical experiences of their own – or one that they were aware of. Once the micro-narrative was provided, the respondents were asked to code their narrative against a set of pre-chosen signifiers.
The data were subsequently loaded into the SenseMaker® Collector™ tool, which enables ‘qualitative input in the form of stories, anecdotes and narratives (which have the potential to convey rich social meaning and are easily recalled and communicated), with quantitative indices allowing for this data to be quickly coded, classified and analyzed’ (Raford Citation2012:118). It also provides a visual platform that ‘enable[s] users to view patterns and anomalies not otherwise visible through conventional methods for analysis of narrative information’ (Casella, Magara, Kumasi, Guijt & van Soest Citation2014:18). The SenseMaker® tool enables the immediate retrieval of the original narrative during the analysis process so that specific details can be analysed once the patterns are more thoroughly understood. For a detailed account of applying the SenseMaker® Collector™ tool, see Casella et al. (Citation2014) and GlobalGiving (Citation2014).
Results
Archetype Extraction
The Archetype Extraction process surfaced a diverse range of themes that the community members associated with HIV/AIDS in their area. It was possible to situate the themes on the Cynefin framework so that a management response could be identified. The themes included community ‘assets’ and ‘challenges’ that could be responded to. provides an overview of the dominant recurring themes – or patterns – that emerged and a management response typology that is aligned to the Cynefin framework heuristic.
Table 4. Themes that were surfaced through the Archetype Extraction technique.
provides an overview of the dominant recurring patterns that the Archetype Extraction technique elicited. It demonstrates that there are many ‘assets’ that can be built upon – or reinforced – and also many ‘challenges’. The management responses to the ‘assets’ are typically ordered responses which are responsive to good – or best – practices, so that the impact of the assets can be increased. The management responses to the ‘challenges’ are typically unordered – containing some ‘non-linear relationships’ between the component parts (Stirzaker et al. Citation2010) – and therefore, following Snowden and Boone (Citation2007), require pattern management responses to destabilise or disrupt the discrete patterns that sustain the visible challenges identified by the participants because there is no good or best practice to hand.
Weak signal detection
From the perspective of the researchers, the prevalence of mental health challenges – often labelled as ‘hopelessness’ by the participants – was considered a weak signal because of the extent of reporting. Many of the images included graphic representations of people ‘hanging themselves up’ (committing suicide by hanging) and depressed young people. However, while the participants were extremely concerned by the recent emergence of mental health challenges, it was no longer a surprise to them.
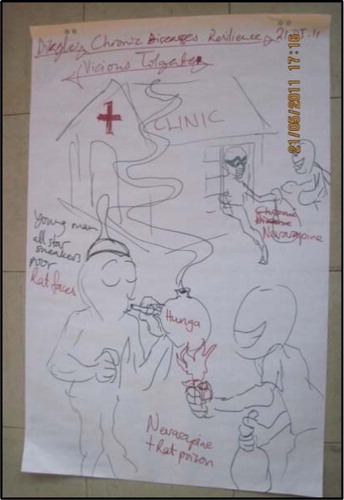
A second weak signal that emerged was called the ‘Vicious Tollgate’ (). This archetype represented the use of a recreational drug known as ‘Whoonga', which is believed to contain a cocktail of antiretroviral medication, rat poison and alcohol. Coding this archetype back to the Discovery Phase suggested that lazy community members, crooks and patients were associated with the archetype.
Fig. 4. The Vicious Tollgate: surfacing Whoonga in 2011. Source: authors’ contribution.
The third ‘weak signal’ that emerged was an image of a government worker (). This archetype was considered to be a weak signal because it was the only representation that appeared to point directly at the role of government from all the workshops.
Fig. 5. The ‘Opinionated Idiot’ archetype. Source: authors’ contribution.

However, when the associations were identified from the coding, it became evident that the participants were linking ‘opinionated idiots’ to the community. During a subsequent discussion with the participants, it became evident that these associations did reflect frustrations with government responsiveness, but also to the way in which the conflict between traditional values and the opportunities provided by biomedical opportunities was a challenge in the area ().
Fig. 6. The Cycle of Treatment-Seeking Behaviour in Ga-Dikgale. Source: authors’ contribution.
represents the reported reality of treatment-seeking against the way the participants believe – rationally – what ‘should’ happen amongst their community. When asked to rate the confidence in the different treatment options on a scale of one to five (with five being the most confidence), they rated hospital – or clinic-based sources with a five, prophets with a three and traditional healers with a one.
After a circuitous journey, it became clearer that one of the major, emergent weak signals was the participants’ frustration of how their community was to negotiate the ‘traditional/modern’ value system in the sphere of health – and that this challenge referred to other chronic conditions, not just HIV/AIDS.
SenseMaker®
The focus of the research that is reported on was ‘development in general’ – not HIV/AIDS, per se. SenseMaker® enables the data to be analysed in a number of different ways (Raford Citation2012). As was explained in the methodology, the micro-narratives that are collected are indexed by the storyteller against a set of pre-defined signifiers. The signifiers we report on are: development issues that the community ‘see regularly’; issues that they ‘see occasionally’ and issues that ‘have never seen before’.Footnote1 A total of just over 1300 micro-narratives were indexed against these signifiers ().
Fig. 7. Development themes coded by ‘regularity’ (n = 1087 micro-narratives). Source: authors’ contribution.

Each of the dots in represents a micro-narrative, and SenseMaker® enables the end-user to manipulate the data in many ways. shows the same data, filtered by ‘things the community will never accept’ coupled with ‘experiences people have never seen before’.
Fig. 8. The same data filtered by ‘something the community will never accept. Source: authors’ contribution.
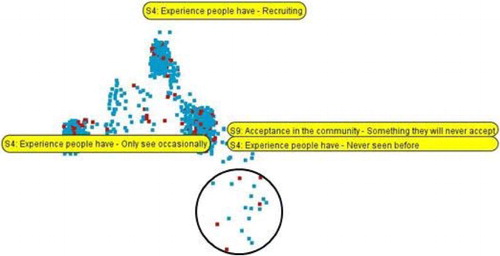
The small cluster in the bottom right-hand corner of the triangle may represent the development of a weak signal within the data set (Casella et al. Citation2014). By selecting the stories highlighted in the circle provides the user with immediate access to the micro-narratives for deeper analysis about what the weal signal represents. The same data can also be represented using another application of SenseMaker® called ‘Landscape’ ().
Fig. 9. The same data when viewed through ‘Landscape’. Source: authors’ contribution.
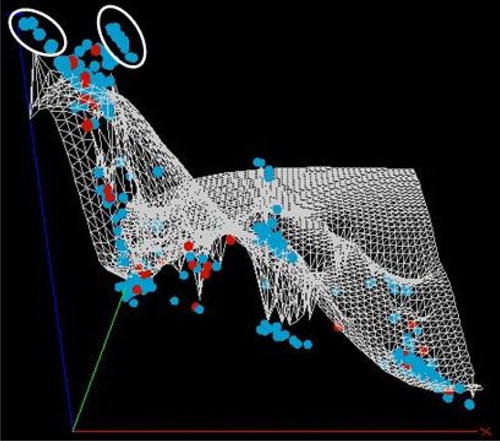
The axes in are the same as the signifiers shown in . The possible weak signals are highlighted in the white circles. Analysis of the content of the micro-narratives surfaces the more detailed patterns and included: corruption, jealousies, disillusionment with volunteerism and irritation with the poor infrastructure within the community (water, electricity and roads).
There is no doubt that applying SenseMaker® in this way provided an extremely creative method for surfacing a massive amount of data in very manageable ways that combines both quantitative and qualitative data. However, it is uncertain to the authors as to whether this application of SenseMaker® surfaced any definitive weak signals.
Discussion
Archetype Extraction
The Archetype Extraction technique did elicit a useful environmental scan that provided pre-hypothesis insights from the perspective of the community. Granted, the workshops were framed within a health theme in a top-down manner, but the rest of the workshop content was driven by empirical realities and the values of the participants. The process enabled the researchers to conduct a scan of the health-related landscape in the area and captured many complexities that local people associated with that particular landscape.
The technique also surfaced some weak signals within that community, which included mental health issues, Whoonga and the challenge of negotiating ‘tradition and modernity’ in the context of managing a chronic disease. The Whoonga weak signal is the most striking example of the value that this technique can surface. A Google Scholar search in 2011 –when the data was collected –for ‘Whoonga’ and ‘South Africa’ revealed 8 ‘hits’ and the same search in 2014 revealed 49 hits – for example, see Grelotti et al. (Citation2014).Footnote2 We suggest that this demonstrates that the weak signal focus is relevant when working with ‘long wave events’ (Fourie & Follér Citation2012) – such as the HIV/AIDS epidemic – because when novel forms of emergence begin to develop, communities are probably the first group of people to notice some of the weak signals, as is reported above.
The Archetype Extraction technique emphasised – with the benefit of retrospect – that it was possible to surface weak signals, as well as providing insights into other issues that were considered relevant to the localised HIV/AIDS landscape from the perspective of the participants. Analysis of the findings using secondary literature and on-going community discussions enabled a slightly more nuanced analysis that suggests that of the three weak signals detected, two exhibit strong patterned interdependencies – mental health and the treatment-seeking cycle challenge – and Whoonga exhibits weaker interconnections.
Combining the Archetype Extraction technique with the Cynefin framework enabled a management response to be articulated.
However, the technique comes with caveats:
The workshops are a cognitive overload for those involved and this makes the process very demanding on participants;Footnote3
Working with an artist necessarily involves the possibility that his, or her, bias can influence the representations of the archetypes;
The images – which some have claimed can be used in the future to prompt debate (Snowden Citation2002) – were subsequently of little research value in our context. Attempts were made to prompt further community discussions using the images but all of these efforts produced minimal returns. In retrospect, the sketches (see ) were justifiable, but the resources required to develop the sketches into quality graphics (see ) are unjustifiable;
Scale. While Archetype Extraction was manageable at the localised scale of one community – it is difficult to imagine how this technique can contribute to Vision 90:90:90, if applied as a standalone technique.
The final caveat is the potential of the research team to respond to the findings. We were able to respond to the mental health challenge by initiating one MDev thesis (Aphane Citation2015). However, in the eyes of the community, this is not a timely response, nor the one they were hoping for. The issue of Whoonga appears to have been short lived because it is no longer considered relevant by the community and the challenge of negotiating ‘tradition and modernity’ remains an on-going challenge.
In reality, an impact-oriented Community Engagement unit – such as the one that drove the pilots – is not well placed to respond with either the speed or resources to deliver a ‘real-time’ response that can have immediate impact in such instances.
SenseMaker®
Our experiences with SenseMaker® did elicit some phenomena that could be described as weak signals – such as people becoming disillusioned with ‘volunteerism’. However, our experience was a single application and not a historical application of it. For this reason, we briefly describe a much larger application in East Africa – for more details, see GlobalGiving (Citation2014).
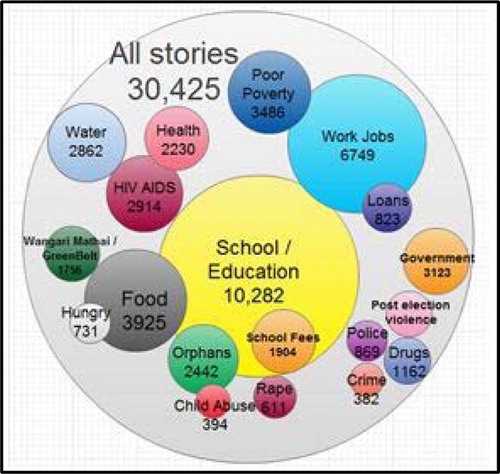
GlobalGiving collected approximately 30,000 micro-narratives from 2010 to 2013. By cross referencing their data with other software, they were able to generate maps that showed the characteristics of a massive area by themes that were relevant to the communities they were involved with () and also to generate visual representations of the weight that community respondents attributed to different development challenges ().
Fig. 10. Themes from Uganda and Kenya and the number of beds per clinic represented by the size of the circle. Source: Maxmeister (Citation2014).
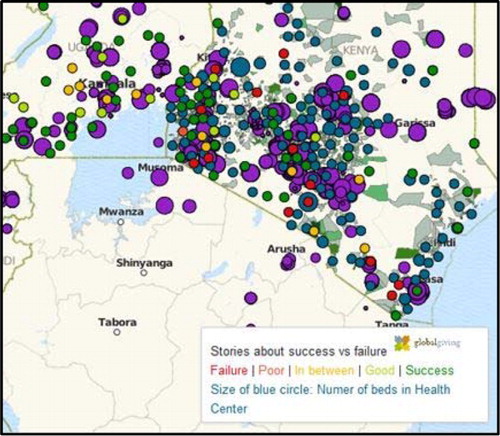
Fig. 11. The number of times different themes were mentioned in micro-narratives in the GlobalGiving project. Source: Maxmeister (Citation2014).
The GlobalGiving data demonstrate how SenseMaker® enables data analysis at multiple scales. This is particularly relevant to one of UNAIDS action points that they believe to be an essential component of ‘ending AIDS’. Specifically, they argue that in Action Point # 4 that it is necessary to ‘Focus on local epidemics and populations’ and then recommend
It is important to continue to collect and analyse data at the subnational level, district by district, and in cities to identify areas of high incidence of HIV infection and the socio-behavioural reasons that contribute to people becoming newly infected with HIV. With local information, HIV services can be scaled up and saturated to meet community needs. (UNAIDS Citation2014b:301)
Our experience with SenseMaker® suggests the software, if appropriately applied, has the capacity to contribute to UNAIDS’ call for complementary analyses of the epidemic at multiple scales. Other experiences, such as the GlobalGiving experience (Whittle Citation2010), demonstrates that it is possible to elicit and analyse thousands of community ‘voices’ and perspectives – emphasising that the SenseMaker® Collector™ tool has extraordinary potential.
However, we still emphasise that a historical – or longitudinal – application of SenseMaker® can add more value ().
Fig. 12. Historical data using Landscape. Source: Cognitive Edge training materials, available at http://cognitive-edge.com/uploads/presentations/CE%20Accreditation%20SENSEMAKER%20feb%2008.pdf. Reproduced with permission.
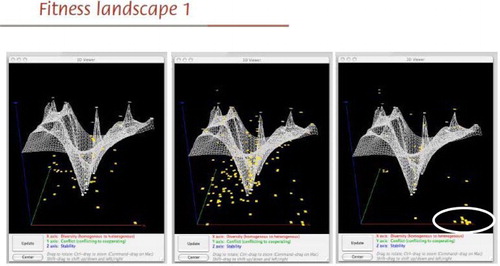
is reproduced from training materials and the axes labels are unknown. The purpose of the representation is to demonstrate a longitudinal application of SenseMaker®. The circle in the bottom left-hand corner of the final image represents a new cluster of voices emerging. These could represent weak signals that would require management attention if SenseMaker® was being used to contribute to Vision 90:90:90.
As with the Archetype Extraction technique, our application of SenseMaker® came with caveats:
As has been noted above, our application included only one round of data collection and our intuition informs us that the value-add of SenseMaker® lies as in a longer term commitment so that historical data can be captured and applied;
The application of SenseMaker® implicitly requires stepping outside of the Gaussian box and an understanding of Power Laws, thus the ability to move towards embracing abductive thinking, as much as more traditional forms of inductive or deductive thinking – see Snowden (Citation2011) and Andriani and McKelvey (Citation2007) for more details of the relevance of Power Laws to developing strategic foresight. A more thorough understanding of this would have added value to the preparation phases of this project.
Could the application of SenseMaker® – or similar software – become a realistic proposition?
SenseMaker® has now been used in multiple fields including: scenario planning in the United Arab Emirates (UAE) (Raford Citation2012); water and sanitation in Ghana (Casella et al. Citation2014) and gender by an international development agency (DFID Citation2014). Our experience of SenseMaker® was laborious because the micro-narratives were collected using voice recorders and then transcribed and loaded into SenseMaker®. By far the most efficient way of doing this is to do it directly online.
With the exponential growth in connectivity and ‘smart’ technologies, it is now possible to imagine mass data collection in South Africa. For example, thousands of students across the country are involved with community outreach or engagement activities – all of whom have access to the internet. Likewise, community healthcare workers are becoming increasingly connected. If the SenseMaker® Collector™ tool were used to host diaries from all of these people working within communities, then the data that would emerge would be sizeable and the flexibility of SenseMaker® would enable real-time analyses at multiple scales across the country. Given the wealth of global lessons learnt about the application of this tool, it is now possible to imagine applying it to South Africa's eHealth strategy in a pilot format as a mechanism for contributing to Vision 90:90:90.
The complexity of achieving Vision 90:90:90 in a five-year time-frame
It is argued that achieving Vision 90:90:90 is now plausible because of the unprecedented biomedical opportunities to ‘end AIDS’ (UNAIDS Citation2014b). However, recent evidence shows that there is a significant gap between prevention efforts and the opportunities that the biomedical gains provide (Michielsen, Chersich, Luchters, De Koker, Van Rossem & Temmerman Citation2010), with the ‘number of newly infected people each year continu[ing] to outnumber those who gain access to treatment’ (Pandor Citation2014). This is just one of many existing challenges that will intersect with achieving Vision 90:90:90. Not only are there existing challenges to achieving Vision 90:90:90; new challenges are likely to emerge in unpredictable ways. This makes the ‘five-year’ journey a complex journey.
Negotiating a complex journey
We have demonstrated that it is possible to move beyond an exclusive focus on visible descriptors of phenomena by surfacing the discrete patterns that influence the descriptor – also known as ‘first’ and ‘second-order’ change (Bishop, Dzidic, Breen & Bishop Citation2013). This is especially relevant in complex scenarios because in this context ‘second’-order change represents an autopoietic driver of social practices (Auerbach, Parkhurst & Caceres Citation2011; Burman, Moerschell, et al. Citation2015). UNAIDS informs us that ‘[i]ncreasingly we are seeing multiple epidemics in countries. Never has it been more important to focus on location and population – to be at the right place for the right people’ (UNAIDS Citation2014b:5). These locations and populations often produce contexts that are characterised by – and emphasise –the ‘extreme complexity of health and disease’ (Peter Piot in UNAIDS Citation2015:58).
Negotiating multiple, complex journeys requires an epistemological shift from the over-reliance on Newtonian ‘good’ or ‘best’ practices that are effective for constrained, ‘ordered’ challenges to management responses that can also embrace ‘organised’ and ‘disorganised’ forms of unconstrained, complexity – characterised by non-linearity, emergence and unpredictability. Snowden and Boone (Citation2007) argue that this type of challenge is best approached through participatory management of the emergent, discrete patterns, regardless of whether the patterns are the result of disorganised interconnections or organised interdependencies. The purpose of managing these patterns is to either reduce or increase autopoietic tendencies, or to reinforce, or destabilise, existing autopoietic interdependencies so that the direction of change can be influenced (Becker Citation2011). This is reinforced by Coleman, Vallacher, Nowak and Bui-Wrzosinska (Citation2007:1459), who argue that ignoring the second-order ‘mechanisms that continually reinstate the [original condition] are likely to be futile, resulting only in short-term changes’.
With time and experience, the unordered, complex challenges may shift and become more ordered – with an associated ameliorative ‘good’ or ‘best’ practice. Until that time, it is necessary to expect that ‘pattern management’ should dominate the responses to the complexities situated within the diverse epidemiological landscapes. Evidence of what this approach might look like are few and far between (Dickens Citation2012) – but working with communities who ‘know’ their HIV/AIDS landscape (Wilson & Halperin Citation2008) seems key (Chu & Selwyn Citation2011; Dybul Citation2014) – ‘because prevention efforts are shaped by the specificities of what they [communities] value’ (Kippax, Stephenson, Parker & Aggleton Citation2013:1368).
Key policy recommendations
Given that the epidemic is now considered to be at a tipping point moment that could culminate in ending AIDS and that achieving this means that ‘a business-as-usual approach or simply sustaining the AIDS response at its current pace cannot end the epidemic’ (UNAIDS Citation2014b:296), we have two recommendations.
The first suggestion is that it is now necessary to critically examine the logic of only focusing on the visible descriptors of high risk groups – as most policy documents suggest – if Vision 90:90:90 is to be achieved.
We recommend that when there are clear-cut, effective responses to ordered challenges associated with high risk contexts – then a focus on the visible descriptors is an appropriate management focus. However, when challenges are unordered, it is more of an appropriate management response to focus on the underlying patterns – simultaneously remaining mindful of the visible descriptors. This requires that the ‘development of innovative new approaches for HIV prevention’ (SANAC Citation2012:70) includes transdisciplinary migrations into relatively uncharted epistemological waters, such as complexity and futures science, so that patterned dynamics can be captured – and worked with – to contribute to Vision 90:90:90. This could be achieved by incorporating software such as SenseMaker® into national surveys – such as the four-year South African National HIV Prevalence, Incidence and Behaviour Survey – so that real-time ‘patterned’ data, representing multiple scales of intersecting data reflecting the different components of the national epidemic is generated and exploited to achieve Vision 90:90:90.
The second recommendation focuses on UNAIDS' call for a qualitatively unique shift from a ‘response mode’ to a ‘mission mode' (UNAIDS Citation2014b:299). The eight action points are all recommendations that focus on the visible, first-order, surface descriptors of actions. We have argued that beneath the surface descriptors there are discrete, second-order, forces that will influence the descriptor. One relevant, discrete mediator of Vision 90:90:90 is – almost certainly – the absence of any evidence that demonstrates that, within the analytical HIV/AIDS landscape, people are considering the possibility that Power Laws are better positioned to explain some of the visible characteristics of the epidemic than traditional Gaussian assumptions. If ‘the “Achilles heel:” of the bell curve is the word independent’ – Buchanan in Ramalingham (Citation2013:217) – and, as we have seen, so much of the landscape is intimately connected through feedback and relationships, the time is ripe to consider a think tank scenario to fill this anomaly.
Conclusion
We have provided a transdisciplinary journey that includes a complexity and futures orientation that could contribute to achieving Vision 90:90:90. This transdisciplinary migration has included a theoretical foundation and some empirical findings to support the case. We have argued that when managing a complex, adaptive landscape, the development of an anticipatory surveillance system that is capable of identifying weak signals has been shown to add value in other contexts. We suggest that real-time, adaptive response capacity is required to act on the weak signals that emerge – or already exist – within the HIV/AIDS landscapes can add value to Vision 90:90:90. We have also suggested that software – such as SenseMaker® – can be used to develop real-time data that can dovetail with the South African eHealth strategy and that a real-time response is critical because of the five-year time-frame.
The rationale for this is implicitly embodied within the claim by UNAIDS that the next five years are critical to achieving the end of AIDS and we suggest that the compressed journey will necessarily entail radical forms of change. Many of the changes that will be encountered are distinctly complex and therefore require both transdisciplinary and epistemological migrations, underwritten by the ontological dexterity to embrace both the ordered and unordered ‘faces’ of the epidemic.
By combining weak signal detection techniques with the Cynefin framework could provision decision-makers with a national management tool for developing anticipatory resilience to changes that might occur amongst the patterns below the surface of the HIV/AIDS landscape – thus contributing to achieving Vision 90:90:90. Without such innovative migrations and implementation strategies, we suggest that achieving Vision 90:90:90 will be similar to the history of the epidemic: a turbulent and difficult landscape to negotiate.
Acknowledgements
This work is based on the research supported by the National Research Foundation and VLIR-UOS. This work would have not been possible without the cooperation of Nancy Letsoalo and community support in Ga-Dikgale. Any opinion, finding and conclusion (or recommendation) expressed in this material is that of the authors and the NRF, VLIR-UOS and WWS do not accept any liability in this regard. We also acknowledge the work of the artist who developed the image: Mr Tawanda Mhandu.
Additional information
Funding
Notes
1. Please note: the word ‘recruiting’ was inadvertently used in the original loading of the filters into SenseMaker and should read ‘recurring’ — which is how the survey was worded.
2. Whoonga is also known as ‘Nyaope’ and a similar search replacing ‘Whoonga’ with ‘Nyaope’ revealed 9 hits for 2011, 85 hits for 2014 and 22 hits for Limpopo and Nyaope. Despite the variation in numbers, the point remains the same.
3. Pilots were also undertaken with staff members of the University of Limpopo and staff members with a South African parastatal and all of the participants reported that the technique is demanding.
References
- Abu-Raddad, L. J., Barnabas, R. V., Janes, H., Weiss, H. A., Kublin, J. G., Longini, I. M. Jr., et al. (2013). Have the Explosive HIV Epidemics in Sub-Saharan Africa Been Driven by Higher Community Viral Load? AIDS, 27(6), 981–989. doi:10.1097/QAD.0b013e32835cb927
- Anderson, R. A., Crabtree, B. F., Steele, D. J., & McDaniel, R. R. Jr., (2005). Case Study Research: The View from Complexity Science. Qualitative Health Research, 15(5), 669–685. doi:10.1177/1049732305275208
- Andriani, P. & McKelvey, B. (2007). Beyond Gaussian Averages: Redirecting International Business and Management Research Toward Extreme Events and Power Laws. Journal of International Business Studies, 38(7), 1212–1230. doi:10.1057/palgrave.jibs.8400324
- Ansoff, H. I. (1975). Managing Strategic Surprise by Response to Weak Signals. California Management Review, 18(2), 21–33. doi: 10.2307/41164635
- Aphane, M. (2015). Lay Opinions and Knowledge of Dikgopheng Community about Mental Illness in Polokwane Municipality, (Development Masters), Polokwane, University of Limpopo.
- Auerbach, J. D., Parkhurst, J. O. & Caceres, C. F. (2011). Addressing Social Drivers of HIV/AIDS for the Long-Term Response: Conceptual and Methodological Considerations. Global Public Health, 6(Suppl 3), S293–S309. doi:10.1080/17441692.2011.594451
- Axelrod, R. M. & Cohen, M. D. (2000). Harnessing Complexity: Organizational Implications of a Scientific Frontier, New York, Basic Books.
- Barker, P., Barron, P., Bhardwaj, S. & Pillay, Y. (2015). The Role of Quality Improvement in Achieving Effective Large-Scale Prevention of Mother-to-child Transmission of HIV in South Africa. AIDS, 29(Suppl 2), S137–S143. doi:10.1097/QAD.0000000000000718
- Barron, P., Pillay, Y., Doherty, T., Sherman, G., Jackson, D., Bhardwaj, S., et al. (2013). Eliminating Mother-to-child HIV Transmission in South Africa. Bulletin of the World Health Organization, 91(1), 70–74. doi:10.2471/BLT.12.106807
- Becker, J. (2011). Evaluating a Complex and Uncertain Future. World Futures, 67, 30–46. doi: 10.1080/02604027.2010.532755
- Bishop, B. J., Dzidic, P. L., Breen, L. J. & Bishop, B. (2013). Multiple-level Analysis as a Tool for Policy: An Example of the Use of Contextualism and Causal Layered Analysis. Journal of Community Psychology, 4(2), 1–13.
- Boisot, M. & Child, J. (1999). Organizations as Adaptive Systems in Complex Environments: The Case of China. Organization Science, 10(3), 237–252. doi:10.1287/orsc.10.3.237
- Burman, C. J., Aphane, M. & Delobelle, P. (2015). Reducing the Overall HIV-burden in South Africa: Is ‘Reviving ABC’ an Appropriate Fit for a Complex, Adaptive Epidemiological HIV Landscape? African Journal of AIDS Research, 14(1), 13–28. doi:10.2989/16085906.2015.1016988
- Burman, C. J., Aphane, M., Mtapuri, O. & Delobelle, P. (2015). Expanding the Prevention Armamentarium Portfolio: A Framework for Promoting HIV-conversant Communities within a Complex, Adaptive Epidemiological Landscape. SAHARA-J: Journal of Social Aspects of HIV/AIDS, 12(1), 18–29. doi:10.1080/17290376.2015.1034292
- Burman, C. J., Mamabolo, R., Aphane, M., Lebese, P. & Delobelle, P. (2013). The South African Developmental Landscape: Restricted Potentials or Expansive, Complex Adaptive Opportunities? The Journal for Transdisciplinary Research in Southern Africa, 9(1), 17–38.
- Burman, C. J., Moerschell, L., Mamabolo, R., Aphane, M. & Delobelle, P. (2015). Re-imagining Decision Making: Addressing a Discrete Social Driver of HIV/AIDS Through the Lens of Complexity Science. African Journal of AIDS Research, 14(1), 75–84. doi:10.2989/16085906.2015.1016983
- Camazine, S., Deneubourg, J., Franks, N., Sneyd, J., Theraulaz, G. & Bonabeau, E. (2001). Self-organization in Biological Systems, Princeton, NJ, Princeton University Press.
- Capra, F. (2002). The Hidden Connections: Integrating the Biological, Cognitive, and Social Dimensions of Life into a Science of Sustainability, New York, Doubleday Books.
- Carey, G. & Crammond, B. (2015). Systems Change for the Social Determinants of Health. BMC Public Health, 15, 662. doi:10.1186/s12889-015-1979-8
- Casella, D., Magara, P., Kumasi, T. C., Guijt, I. & van Soest, A. (2014). The Triple-S Project Sensemaker® Experience: A Method Tested and Rejected, The Hague, IRC.
- Chu, C. & Selwyn, P. A. (2011). An Epidemic in Evolution: The Need for New Models of HIV Care in the Chronic Disease Era. Journal of Urban Health, 88(3), 556–566. doi:10.1007/s11524-011-9552-y
- Cilliers, P. (1998). Complexity and Postmodernism: Understanding Complex Systems, New York, Routledge.
- Cilliers, P. (2005). Knowledge, Limits and Boundaries. Futures, 37(7), 605–613. doi:10.1016/j.futures.2004.11.001
- Coleman, P. T., Vallacher, R. R., Nowak, A. & Bui-Wrzosinska, L. (2007). Intractable Conflict as an Attractor: A Dynamical Systems Approach to Conflict Escalation and Intractability. American Behavioral Scientist, 50(11), 1454–1475. doi:10.1177/0002764207302463
- Deeks, S. G., Lewin, S. R. & Havlir, D. V. (2013). The End of AIDS: HIV Infection as a Chronic Disease. The Lancet, 382(9903), 1525–1533. doi:10.1016/s0140-6736(13)61809-7
- DFID. (2014). Using SenseMaker to Understand Girls’ Lives: Lessons Learnt, London, The UK Department for International Development.
- Dickens, P. M. (2012). Facilitating Emergence: Complex, Adaptive Systems Theory and the Shape of Change. (PhD thesis), New England, Antioch University.
- Dybul, M. (2014). Better and Smarter Investments. Retrieved from http://www.theglobalfund.org/en/blog/2014-07-22_Better_and_Smarter_Investments/ (Accessed 27 November 2014).
- Fiorella, K. J. (2013). Considering the Complexity in HIV/AIDS and the Environment. American Journal of Public Health, 103(9), e1. doi:10.2105/AJPH.2013.301433
- Fourie, P. & Follér, M. L. (2012). AIDS Hyper-epidemics and Social Resilience: Theorising the Political. Contemporary Politics, 18(2), 254–268. doi:10.1080/13569775.2012.674342
- Galatzer-Levy, R. M. (2002). Emergence. Psychoanalytic Inquiry, 22(5), 708–727. doi:10.1080/07351692209349014
- Galea, S., Riddle, M. & Kaplan, G. A. (2010). Causal Thinking and Complex System Approaches in Epidemiology. International Journal of Epidemiology, 39(1), 97–106. doi:10.1093/ije/dyp296
- GlobalGiving. (2014). Global Giving Story Tools. http://www.globalgiving.org/story-tools/ (Accessed 18 December 2014).
- Grelotti, D. J., Closson, E. F., Smit, J. A., Mabude, Z., Matthews, L. T., Safren, S. A., et al. (2014). Whoonga: Potential Recreational Use of HIV Antiretroviral Medication in South Africa. AIDS and Behavior, 18(3), 511–518. doi:10.1007/s10461-013-0575-0
- Grimsrud, A. T., Cornell, M., Egger, M., Boulle, A. & Myer, L. (2013). Impact of Definitions of Loss to Follow-up (LTFU) in Antiretroviral Therapy Program Evaluation: Variation in the Definition can have an Appreciable Impact on Estimated Proportions of LTFU. Journal of Clinical Epidemiology, 66(9), 1006–1013. doi:10.1016/j.jclinepi.2013.03.013
- Hankins, C. A. & de Zalduondo, B. O. (2010). Combination Prevention: A Deeper Understanding of Effective HIV Prevention. AIDS, 24(4), S70–S80. doi:10.1097/01.aids.0000390709.04255.fd
- Hardee, K., Gribble, J., Weber, S., Manchester, T., Wood, M., Defoort, C., et al. (2013). Reclaiming the ABCs: The Creation and Evolution of the ABC Approach. Population-E, 63(2), 285–318. http://populationaction.org/wp-content/uploads/2012/01/ABCs_8.5×11.pdf
- Harris, S. D. & Zeisler, S. (2002). Weak Signals: Detecting the Next Big Thing – Where's the Next Major Innovation Coming From? Being Alert for Weak Signals Could Clue you in. Futurist, 36(6), 21–28.
- Hatt, K. (2008). Considering Complexity: Toward a Strategy for Non-linear Analysis. Canadian Journal of Sociology, 34(2), 313–348.
- Holland, J. (1998). Emergence – From Chaos to Order, Reading, MA, Addison-Wesley.
- James, C. H. & Minnis, W. C. (2004). Organizational Storytelling: It Makes Sense. Business Horizons, 47(4), 23–32. doi:10.1016/s0007-6813(04)00045-x
- Jayasinghe, S. (2011). Conceptualising Population Health: From Mechanistic Thinking to Complexity Science. Emerging Themes in Epidemiology, 8(1), 7. http://www.ncbi.nlm.nih.gov/pubmed/21247500. doi:10.1186/1742-7622-8-2
- Johnson, S. (2001). Emergence: The Connected Lives of Ants, Brains, Cities, and Software, New York, Addison-Wesley.
- Kaivo-oja, J. (2012). Weak Signals Analysis, Knowledge Management Theory and Systemic Socio-cultural Transitions. Futures, 44(3), 206–217. doi:10.1016/j.futures.2011.10.003
- Kauffman, S. (2005). At Home in the Universe: The Search for Laws of Self-Organization and Complexity, New York, Oxford University Press.
- Kippax, S., Stephenson, N., Parker, R. G. & Aggleton, P. (2013). Between Individual Agency and Structure in HIV Prevention: Understanding the Middle Ground of Social Practice. American Journal of Public Health, 103(8), 1367–1375. doi:10.2105/AJPH.2013.301301
- Klein, G. (2008). Naturalistic Decision Making. Human Factors: The Journal of the Human Factors and Ergonomics Society, 50(3), 456–460. doi:10.1518/001872008X288385
- Kurtz, C. F. & Snowden, D. J. (2003). The New Dynamics of Strategy: Sense-Making in a Complex and Complicated World. IBM Systems Journal, 42(3), 462–483. doi: 10.1147/sj.423.0462
- Leach, M., Scoones, I. & Stirling, A. (2010). Governing Epidemics in an Age of Complexity: Narratives, Politics and Pathways to Sustainability. Global Environmental Change, 20(3), 369–377. doi:10.1016/j.gloenvcha.2009.11.008
- Lee, M. E. (1997). From Enlightenment to Chaos: Toward Nonmodern Social Theory. In R. A. Eve, S. Horsfall & M. E. Lee (Eds.), Chaos, Complexity, and Sociology: Myths, Models, and Theories, pp. 15–29, Thousand Oaks, CA, Sage.
- Lich, K. H., Ginexi, E. M., Osgood, N. D. & Mabry, P. L. (2013). A Call to Address Complexity in Prevention Science Research. Prevention Science, 14(3), 279–289. doi:10.1007/s11121-012-0285-2
- Linde, C. (2001). Narrative and Social Tacit Knowledge. Journal of Knowledge Management, 5(2), 160–171. doi:10.1108/13673270110393202
- Lorenz, E. (1972). Predictability: Does the Flap of a Butterfly's Wings in Brazil Set off a Tornado in Texas. American Association for the Advancement of Science, Washington, DC.
- Luhmann, N. (1995). Social Systems, Stanford University, Stanford University Press.
- Lurie, M. N. & Williams, B. G. (2014). Migration and Health in Southern Africa: 100 Years and Still Circulating. Health Psychology and Behavioral Medicine, 2(1), 34–40. doi:10.1080/21642850.2013.866898
- Maree, G. A., Roux, D. J. & Marais, M. A. (2006). Beneath the Surface of Conscious Patterns: Using Narrative to Characterise the Culture of Innovation at a Leading R&D Organisation. The South African Council for Scientific and Industrial Research (CSIR). http://researchspace.csir.co.za/dspace/bitstream/10204/1042/1/maree1_2006_D.pdf
- Martin, C., Grady, D., Deaconking, S., McMahon, C., Zarabzadeh, A. & O'Shea, B. (2011). Complex Adaptive Chronic Care – Typologies of Patient Journey: A Case Study. Journal of Evaluation in Clinical Practice, 17(3), 520–524. doi:10.1111/j.1365-2753.2011.01670.x
- Martin, C. & Sturmberg, J. (2005). General Practice-Chaos, Complexity and Innovation. Medical Journal of Australia, 183(2), 106–109.
- Matthews, L. T., Crankshaw, T., Giddy, J., Kaida, A., Smit, J. A., Ware, N. C., et al. (2013). Reproductive Decision-Making and Periconception Practices Among HIV-positive Men and Women Attending HIV Services in Durban, South Africa. AIDS and Behavior, 17(2), 461–470. doi:10.1007/s10461-011-0068-y
- Maturana, H. R. & Varela, F. J. (1980). Problems in the Neurophysiology of Cognition. Autopoiesis and Cognition, 42, 41–47. doi:10.1007/978-94-009-8947-4_5
- Maxmeister, M. P. (2014, December 22). [GlobalGiving Project].
- McDaniel, R. R. & Driebe, D. J. (2001). Complexity Science and Health Care Management. In J. D. Blair, M. D. Fottler & G. Savage (Eds.), Advances in Health Care Management, Vol. 2, pp. 11–36, Stamford, CT, JAI.
- Mendonça, S., Cardoso, G. & Caraça, J. (2012). The Strategic Strength of Weak Signal Analysis. Futures, 44(3), 218–228. doi:10.1016/j.futures.2011.10.004
- Merson, M. H., O'Malley, J., Serwadda, D. & Apisuk, C. (2008). The History and Challenge of HIV Prevention. The Lancet, 372(9637), 475–488. doi:10.1016/s0140-6736(08)60884-3
- Michielsen, K., Chersich, M. F., Luchters, S., De Koker, P., Van Rossem, R. & Temmerman, M. (2010). Effectiveness of HIV Prevention for Youth in Sub-Saharan Africa: Systematic Review and Meta-analysis of Randomized and Nonrandomized Trials. AIDS, 24(8), 1193–1202. doi:10.1097/QAD.0b013e3283384791
- Mkhize-Kwitshana, Z. L. & Mabaso, M. L. H. (2014). The Neglected Triple Disease Burden and Interaction of Helminths, HIV and Tuberculosis: An Opportunity for Integrated Action in South Africa. South African Medical Journal, 104(4), 258. doi:10.7196/samj.7947
- Modjarrad, K. (2013). HIV and Helminths: Time for a New Direction. The Lancet Infectious Diseases, 13(10), 835. doi: 10.1016/S1473-3099(13)70239-1
- Motsoaledi, A. (2014). Budget Vote in Parliament. http://www.polity.org.za/article/plans-to-turn-the-tide-on-hivaids-by-2030-2014-07-23 (Accessed 13 November 2014).
- National Department of Health. (2012). eHealth Strategy South Africa 2012–2016. D. o. Health (Ed.), (pp. 36). Pretoria.
- Nguyen, V. K., Bajos, N., Dubois-Arber, F., O'Malley, J. & Pirkle, C. M. (2011). Remedicalizing an Epidemic: From HIV Treatment as Prevention to HIV Treatment is Prevention. AIDS, 25(3), 291–293. doi:10.1097/QAD.0b013e3283402c3e
- Nonaka, I. & Takeuchi, H. (1995). The Knowledge-creating Company: How Japanese Companies Create the Dynamics of Innovation, Oxford, Oxford University Press.
- Pandor, N. (2014). http://www.polity.org.za/article/sa-naledi-pandor-says-investment-in-research-and-development-for-hiv-prevention-remains-critical-2014-10-28 (Accessed 18 December 2014).
- Parkhurst, J. O. & Whiteside, A. (2010). Innovative Responses for Preventing HIV Transmission: The Protective Value of Population-Wide Interruptions of Risk Activity. Southern African Journal of HIV Medicine, 11(1), 19–21.
- Pettifor, A., MacPhail, C., Corneli, A., Sibeko, J., Kamanga, G., Rosenberg, N., et al. (2011). Continued High Risk Sexual Behavior Following Diagnosis with Acute HIV Infection in South Africa and Malawi: Implications for Prevention. AIDS and Behavior, 15(6), 1243–1250. doi:10.1007/s10461-010-9839-0
- Piot, P., Bartos, M., Larson, H., Zewdie, D. & Mane, P. (2008). Coming to Terms with Complexity: A Call to Action for HIV Prevention. The Lancet, 372(9641), 845–859. doi:10.1016/S0140-6736(08)60888-0
- Pronyk, P. M., Hargreaves, J. R., Kim, J. C., Morison, L. A., Phetla, G., Watts, C., et al. (2006). Effect of a Structural Intervention for the Prevention of Intimate-Partner Violence and HIV in Rural South Africa: A Cluster Randomised Trial. The Lancet, 368(9551), 1973–1983. doi:10.1016/s0140-6736(06)69744-4
- Raford, N. (2012). Crowd-sourced Collective Intelligence Platforms for Participatory Scenarios and Foresight. Journal of Futures Studies, 17(1), 117–128.
- Ramalingham, B. (2013). Aid on the Edge of Chaos, Oxford, Oxford University Press.
- Rodger, A., Bruun, T. & Cambiano, V. (2014). HIV Transmission Risk Through Condomless Sex if HIV+ Partner on Suppressive ART: PARTNER study. Paper presented at the 21st Conference on Retroviruses and Opportunistic Infections, Boston. http://www.natap.org/2014/CROI/CROI.htm
- Rossel, P. (2012). Early Detection, Warnings, Weak Signals and Seeds of Change: A Turbulent Domain of Futures Studies. Futures, 44(3), 229–239. doi:10.1016/j.futures.2011.10.005
- Rossouw, T. M. (2014). Monitoring Early Warning Indicators for HIV Drug Resistance in South Africa: Challenges and Opportunities. Clinical Infectious Diseases. http://www.ncbi.nlm.nih.gov/pubmed/24585563 doi:10.1093/cid/ciu114
- SANAC. (2012). National Strategic Plan on HIV, STIs and TB 2012–2016, Pretoria, South African National AIDS Council.
- Shannon, K., Strathdee, S. A., Goldenberg, S. M., Duff, P., Mwangi, P., Rusakova, M., et al. (2014). Global Epidemiology of HIV Among Female Sex Workers: Influence of Structural Determinants. The Lancet, 385(9962), 55–71. doi:10.1016/s0140-6736(14)60931-4
- Shisana, O., Rehle, T., Simbayi, L., Zuma, K., Jooste, S., Zungu, N., et al. (2014). South African National HIV Prevalence, Incidence and Behaviour Survey, 2012, Cape Town, HSRC Press.
- Sidhom, S. & Lambert, P. (2011). Information Design for ‘Weak Signal’ detection and Processing in Economic Intelligence: A Case Study on Health Resources. Journal of Intelligence Studies in Business, 1(1), 40–48.
- Silvestri, G. (2013). Embracing the Complexity of HIV Immunology. Immunological Reviews, 254(1), 5–9. doi:10.1111/imr.12081
- Snowden, D. J. (2002). Archetypes as an Instrument of Narrative Patterning. Info Today, 209–216.
- Snowden, D. J. (2005). Multi-ontology Sense Making: A New Simplicity in Decision Making. Informatics in Primary Care, 13(1), 45–54.
- Snowden, D. (2011). Good Fences Make Good Neighbors. Information, Knowledge, Systems Management, 10(1), 135–150.
- Snowden, D. J. & Boone, M. E. (2007). A Leader's Framework for Decision Making. Harvard Business Review, 85(11), 68–76.
- Stacey, R. (1995). The Science of Complexity: An Alternative Perspective for Strategic Change Processes. Strategic Management Journal, 16(6), 477–495. doi:10.1002/smj.4250160606
- Stacey, R. (1996). Complexity and Creativity in Organizations, San Francisco, Berrett-Koehler Publishers.
- Stillwaggon, E. (2012). Complex Epidemics, Simplistic Tools: The Failure of AIDS Policy in Africa. In L. Swan, R. Gordan & J. Seckbach (Eds.), Origin(s) of Design in Nature, Vol. 23, pp. 773–791, London, Springer.
- Stirzaker, R., Biggs, H., Roux, D. & Cilliers, P. (2010). Requisite Simplicities to Help Negotiate Complex Problems. Ambio, 39(8), 600–607. doi:10.1007/s13280-010-0075-7
- Stricker, S. M., Fox, K. A., Baggaley, R., Negussie, E., de Pee, S., Grede, N., et al. (2014). Retention in Care and Adherence to ART are Critical Elements of HIV Care Interventions. AIDS and Behavior, 18(Suppl 5), S465–475. doi:10.1007/s10461-013-0598-6
- Tastle, W. J. (1992). To Debate or Not to Debate. International Journal of General Systems, 21(2), 129–130. doi:10.1080/03081079208945064
- UNAIDS. (2014a). Fast Track (pp. 40), Geneva, Joint United Nations Programme on HIV/AIDS.
- UNAIDS. (2014b). The Gap Report (pp. 422), Geneva, Joint United Nations Programme on HIV/AIDS.
- UNAIDS. (2015). How AIDS Changed Everything, Geneva, Joint United Nations Programme on HIV/AIDS.
- Vergne, J. P. (2013). QWERTY is Dead, Long Live Path Dependence! Research Policy, 42, 1191–1194. doi: 10.1016/j.respol.2013.03.009
- Walby, S. (2007). Complexity Theory, Systems Theory, and Multiple Intersecting Social Inequalities. Philosophy of the Social Sciences, 37(4), 449–470. doi:10.1177/0048393107307663
- Weaver, W. (1948). Science and Complexity. Scientific American, 36(4), 536–544.
- Whittle, D. (2010). If you Can Flip a Coin, can you be an Expert? http://www.denniswhittle.com/2010/09/if-you-can-flip-coin-can-you-be-expert.html.
- Wilson, D. & Halperin, D. T. (2008). “Know Your Epidemic, Know Your Response”: A Useful Approach, if we get it Right. The Lancet, 372(9637), 423–426. doi:10.1016/s0140-6736(08)60883-1
- Wilson, T. & Holt, T. (2001). Complexity Science: Complexity and Clinical Care. BMJ, 323(7314), 685–688. doi:10.1136/bmj.323.7314.685