
ABSTRACT
In West Africa, social factors influence whether couples with unmet need for family planning act on birth-spacing desires. Tékponon Jikuagou is testing a social network-based intervention to reduce social barriers by diffusing new ideas. Individuals and groups judged socially influential by their communities provide entrée to networks. A participatory social network mapping methodology was designed to identify these diffusion actors. Analysis of monitoring data, in-depth interviews, and evaluation reports assessed the methodology's acceptability to communities and staff and whether it produced valid, reliable data to identify influential individuals and groups who diffuse new ideas through their networks. Results indicated the methodology's acceptability. Communities were actively and equitably engaged. Staff appreciated its ability to yield timely, actionable information. The mapping methodology also provided valid and reliable information by enabling communities to identify highly connected and influential network actors. Consistent with social network theory, this methodology resulted in the selection of informal groups and individuals in both informal and formal positions. In-depth interview data suggest these actors were diffusing new ideas, further confirming their influence/connectivity. The participatory methodology generated insider knowledge of who has social influence, challenging commonly held assumptions. Collecting and displaying information fostered staff and community learning, laying groundwork for social change.
Introduction
Social network theory and related intervention approaches catalyse social networks to diffuse new ideas, attitudes, and behaviours. Within social networks are key diffusion actors, who by reason of their social influence and/or social connections serve as catalysers. Successful evidence-based applications of social network theory exist in public health ranging from tobacco (Valente, Citation2003) and substance abuse cessation (Curtis & Edwards, Citation1995) to HIV prevention and behaviour change (Broadhead et al., Citation1998; Kim et al., Citation2015; Neaigus, Citation1998; Smith & Christakis, Citation2008; Weeks, Clair, Borgatti, Radda, & Schensul, Citation2002). The influence of social networks on family planning use (Behrman, Kohler, & Watkins, Citation2002; Kohler, Behrman, & Watkins, Citation2001; Valente, Watkins, Jato, Van Der Straten, & Tsitsol, Citation1997; Boulay & Valente, Citation1999) and the importance of mass media to aid network diffusion (Boulay, Storey, & Sood, Citation2002) have been well documented.
A focus on unmet need for family planning – women and men who want to limit or space births but take no action to do so – offers a lens to address upstream determinants of family planning use. Evidence from West Africa indicates that although knowledge and service accessibility influence family planning use, social factors play equally important roles, preventing individuals from acting on their reproductive desires (Akinfeleye, Charles, & Omideyi, Citation1997). Literature on unmet need in Africa and elsewhere affirms the need to acknowledge social networks and cultural contexts, particularly power relations and gender norms as key influences on reproductive health behaviour (Bongaarts & Bruce, Citation1995; Gayen & Raeside, Citation2007; Greene & Biddlecom, Citation2000; Mosha & Ruben, Citation2013; Paz Soldan, Citation2004).
In southwest Benin, formative research indicated that women and men rarely speak to each other about fertility and family planning and couple decision-making is uncommon. Fertility and family planning decisions are made within a larger sphere of relationships – including the husband–wife dyad, household members, and kin and peer networks – under the influence of community norms. Family planning-related stigma often prevents women and men from talking publicly about family planning or acknowledging use (Buesseler & Diakité, Citation2013). In such contexts, social network approaches can address contextual and relationship issues that prevent couples who want to space or limit births from using contraception.
In response, Tékponon Jikuagou is testing a package of community-based social network activities () in Couffo Department, Benin, to reduce social barriers that prevent women and men from addressing unmet need. On an individual level, the intervention aims to increase the acceptability of discussions about fertility desires and family planning use. On a social-normative level, the package aims to increase perceptions of community approval of family planning use.
Figure 1. Package of social network interventions.

This approach is distinguished from many demand creation efforts because it is not message-based and does not use a blanket approach to community mobilisation. Instead, the social network intervention works with and through a small set of community network actors who may be more effective diffusers of new ideas and mobilisers of public dialogue than those usually identified, such as formal leaders or health workers or groups created for project purposes. Theories of change underpinning the first approach, such as the health belief model, often focus on ensuring information is available to encourage individuals to seek services (Brewer & Rimer, Citation2008). The theory of change underpinning this social network approach focused on communication for social change to diffuse new ideation through social networks, breaking down social barriers to discussing and seeking services (Heaney & Israel, Citation2008).
The package contains five components to catalyse discussion and diffusion of new ideas and attitudes through social networks while creating linkages between influential groups and family planning services:
Engage communities in social network mapping. A participatory data collection and analysis methodology – the focus of this article – lays the foundation for network action. Communities identify and rank existing groups and individuals in terms of influence on health, well-being, and community connectivity. Influential actors are approached and, if interested, provide entrée to larger social networks as influencers and connectors.
Support influential groups in reflective dialogue. Groups conduct an activity each time they meet using a set of 15 cards that contain either a story or activity. Trigger questions engage members in reflective dialogues on attitudes and values relating to fertility and family planning. In one story card, for example, a young mother seeks advice on how to broach the topic of family planning with her husband. One activity card involves the group in an ‘agree–disagree’ exercise with thought-provoking statements relating to family planning beliefs. Members are asked to share (diffuse) their reflections with others outside the group, breaking down barriers to public discourse.
Encourage influential individuals to act. Influential people (called influentials in this article) identified during mapping receive an orientation on unmet need and a set of infographics highlighting paradoxes of unmet need. One depicts the proportion of women who want to space births but have never visited a health centre. As opinion leaders, people commit to helping their communities address these issues in public and private venues through actions they determine. For example, a store owner might engage regular clients in discussions about unmet need in the community.
Use radio to create an enabling environment. Recordings of actors reading Tékponon Jikuagou stories and recordings of community groups discussing the stories are broadcast to expand reach beyond those involved in group discussions.
Link family planning providers with influential groups. Formative research indicated limited interaction between influential groups and providers. To create new network connections and improve flow of information about family planning methods and services, opportunities are included, that is, family planning providers are invited to attend a group session and answer questions.
Mathematical modelling and evaluated social network projects indicate that 25% and 50% exposure should lead to shifts in community norms (Jackson & Yariv, Citation2005; Kim et al., Citation2015). Thus, the pilot assumed that approximately three groups and five influentials would be sufficient to diffuse new ideas to about half the adult population in a village over a 12-month period, reaching a tipping point of normative change. Gender synchronisation was assured by selecting equal proportions of women's, men's, and mixed-sex groups in each village; selection of individual influencers was left open-ended in terms of male–female participation, depending on who community members selected.
Social network analysis has emerged as a useful tool to describe and define influential and/or well-connected networks and central network actors, and their relationship to health outcomes (Smith & Christakis, Citation2008). Network analysis uses either sociocentric or egocentric perspectives. The first provides information useful for generalising about relationships in a defined group, that is, a village. The second is useful for generalising about features of personal networks. Tékponon Jikuagou was most interested in a sociocentric perspective.
Social network analysis has been used in public health and social sciences for over 50 years to understand social (rather than individual) determinants of health outcomes. Applied both qualitatively and quantitatively, it uses mapping techniques to visually depict key network relationships. Social network analysis has recently evolved to allow more empirical, analytic complexity, due to development of network-oriented software that can account for relationships between individuals embedded in social networks and model interdependencies between network and individual behavioural dynamics from both egocentric and sociocentric perspectives (Burk, Steglich, & Snijders, Citation2007). The resulting visual outcomes – computer-generated network maps – are powerful tools for describing relationships, demarcating connectors and influentials in given networks. Analysis is most often accomplished through ethnographic methods, or census or population-based surveys (allowing sociocentric and egocentric analysis, respectively). While both traditions yield rich information, data collection and analysis are costly, time-consuming, and cannot provide actionable knowledge of network actors in a timely manner for programme use.
This article explores how we developed and tested the social network mapping methodology used in the intervention. Our community-driven social network intervention required a two to three day approach that would lead, within a few days of data collection, to identifying a small set of connectors and influential actors. As an intervention aiming to catalyse a social change process, we needed a method that would engage communities in data collection and was grounded in principles of gender equity. The challenge was how to translate mapping and analysis concepts into a participatory methodology that maximised community-insider knowledge and analysis of social organisation. It had to be easy to use and acceptable to communities, use visual methodologies to ensure participation by low-literacy groups with differing social perspectives, and lead to accurate identification of the key male and female network actors.
The resulting community social network mapping methodology was designed using Participatory Learning and Action (PLA) principles and techniques. Besides focusing on visual approaches to diminish power differentials and create more democratic processes, PLA aligned with the project's social change approaches: fostering community reflection and analysis of social factors influencing unmet need; sparking public discourse, debate, and diffusion; ensuring gender synchronisation by working with men and women; and taking a learning-to-action approach.
As the community social network mapping methodology was the foundation of the social network intervention, we needed to assess its validity and reliability (Golafshani, Citation2003; Reason, Citation2006). With a view to scale up if the intervention proved successful, we needed to understand its acceptability to those engaged in the social mapping process. The project was funded to go from pilot to expansion using an implementation science approach to broker the gaps that existed between theory and effective practice (Fixen, Naoom, Blase, Friedman, & Wallace, Citation2005). Implementation research assessed outcome variables such as acceptability, adoption, appropriateness, and feasibility (Peters, Adam, & Alonge, Citation2013). Regular data collection and participatory analysis by research and implementation staff were embedded in the implementation process to allow use of real-time data to make decisions (Lobb & Colditz, Citation2013), rather than waiting until project close to make recommendations for future efforts, as is commonly done. Thus, to assess the mapping methodology we drew from existing project monitoring data and staff learning reflections, and supplemented this information with data from a larger set of studies, including formative research and several evaluations conducted to design and refine the pilot intervention, as well as an ongoing cohort study of women and men to track changes in unmet need status and social diffusion over time. Cross-sectional base and endline household surveys in intervention and control health zones assessed the effectiveness of the package in bringing about individual and network change. Preliminary post-pilot intervention findings are included in the analysis as confirmatory evidence of the effectiveness of the mapping methodology.
Study design and methods
Study design
We used a descriptive design to answer two key questions: (1) Was the mapping methodology acceptable to community users and to project field staff? (2) Did it result in valid and reliable data for use in establishing the social network base for the intervention?
We defined and operationalised these terms:
User acceptability – the extent to which users approve of the methodology. Operationally, the methodology should fully engage community users. It should be easy to use by staff and adhere to a principle of social equity in participation by key population segments.
Validity or credibility – the extent to which the methodology accurately measures (i.e. identifies) socially influential groups and individuals. Operationally, the methodology should lead to identification of well-connected and influential groups and individuals. To assess internal validity, we compared the mapping results with those we would expect from social network theory. Social network theory, for example, posits that socially influential actors would not necessarily be formally recognised, which suggests that an approach that identifies non-formal actors is accurately mapping well-connected and influential network actors.
We were also interested in construct validity – how well the approach translates a concept into a functioning reality. Operationally, did the mapping approach to identify influential groups and individuals translate into selected actors diffusing new ideas through their networks?
Reliability or auditability – the consistency of the approach in measuring (i.e. identifying) influential groups and people over time. Operationally, across many villages the mapping methodology should identify a wide variety of influential groups and individuals as it would in any one village.
Data triangulation allowed determination of concordance and confidence in our conclusions.
Data sources and analysis
Data for the assessment exercise came from a variety of sources, noted in , including the following:
Detailed notes from the interim evaluation that included facilitated group discussions with network actors (group discussion leaders and influentials) at different points during the pilot phase. Project research, monitoring, and evaluation (RME) staff with the assistance of two trained research assistants conducted the discussions and analysed the notes. These studies assessed ease of use and acceptability of intervention activities.
Process data generated or collected by field staff were verified and compiled by project RME staff. RME staff analysis of the process documentation consisted of manual review organised along the questions guiding the descriptive study, summarising data and quantifying results where appropriate:
output data from the monitoring system including frequency of group meetings, discussion themes, and reports of information diffusion outside the group;
reports of village social network mapping exercises, including visual outputs of group listing and ranking exercises, discussion summaries, and observations of meeting dynamics;
reports of influential orientation meetings, including summaries of types of people identified as influential (occupation, sex, etc.) and lists of their commitments to act;
group member inventory collected by discussion leaders to understand similar characteristics of group members and influentials; and
notes from semi-annual, facilitated group learning reflection discussions with staff on what was working/not working during implementation, and observed community changes due to the intervention.
Transcripts of two rounds of in-depth interviews from a cohort of 50 women and men living in the project area with different unmet need status. The cohort study tracked changing need status and factors, including diffusion of new ideas and actions, resulting from intervention activities. Interviews were conducted and transcribed by a Benin research firm contracted by the project, with training and oversight by project RME staff. ATLAS.ti was used to code the transcripts and facilitate analysis.
Table 1. Data sources used to assess validity and reliability of the mapping process and outputs.
Institutional Review Board (IRB) approval was received from Georgetown University and the Comité d'Ethique de la Recherche, Institut des Sciences Biomédicales Appliquées en Santé in Bénin for all research studies. Consent was sought from staff to participate in learning reflection events and from community members interviewed in programme-related studies. No names are found in discussion transcripts or reports.
In the absence of a comparison group, we compared results of applying the methodology to what would be expected from social network theory. Social network theory focuses on the web of social relationships that surround individuals. Sociologists have described these relationships in terms of (1) creating and using social capital (collectively expressed as norms of reciprocity and social trust); (2) exercising social influence (the process by which thoughts and actions are changed by actions of others) and (3) providing social support (exchanges through social relationships and interpersonal transactions) (Heaney & Israel, Citation2008).
Our comparison centred on the question, ‘According to network theory, who should have social influence in networks?’ Social capital theory predicts influence occurs within and between different levels of social systems – relationships with family members and peers, relationships involving social differences such as gender and ethnicity, and relationships involving hierarchical differences, such as between government civil servants and civil society (Ferlander, Citation2007). Social influence theory predicts influential people or groups are those with whom one identifies, while acknowledging that influence is also exerted by what the majority in a reference group thinks, and by people who are perceived as experts (Rashotte, Citation2006). Social support theory is based on relationships of exchange and support, mostly from close family members, peers, and neighbours (Heaney & Israel, Citation2008).
Our social network intervention touched on all three aspects of social influence. Thus, social network theory would posit that influential network actors selected by the project's social network mapping methodology would include a mix of influentials operating at different social levels and playing formal and informal expert or opinion-leader roles. It would include a variety of groups that represented a range of indigenous and government or non-governmental organisation (NGO)-created groups with characteristics noted above. We proposed that if the mapping results yielded a preponderance of formally recognised influentials and groups, the methodology was likely not identifying truly influential, connected network actors with influence in the areas of health and well-being.
Community social network mapping methodology
The project's core network intervention was based on identifying actors who would serve as catalysts of change (people and groups who are either influential, i.e. are opinion leaders or normative guardians, and/or well-connected, i.e. having many relationships within a social network). Network density was another concept of interest; dense networks have many connected people and thus are likely to diffuse ideas faster than dispersed networks. Early on we concluded that PLA methodologies could not distinguish between connectors and influencers – in real life there is often overlap – hence we chose to work with a mix of groups and individuals judged most influential or connected, allowing us to engage both influencers and connectors. While our intervention design did not exploit network density, we were interested in learning about social organisation and cohesion and included questions to measure these attributes in mapping exercises.
The resulting methodology
Steps in the social network mapping methodology are summarised in and reflect the primary aim of the tool to identify women's and men's groups and influential individuals as catalysts for change.
Table 2. Summary of steps in the community social network mapping methodology.
Formative research indicated that key social influencers in fertility and family planning were both female and male, and included spouses, parents and in-laws, and close friends. The research also highlighted power and gender differentials at play in communication and decision-making related to fertility and family planning. Thus, PLA exercises for social network mapping and analysis were designed to ensure that gender and social relationships were explicitly embedded in the methodology (Steps 1, 2, and 3). Women, men, youth, elderly, and socially marginalised voices were to be represented during listing and ranking exercises. Later, staff compiled and used these results (Step 4) to select the most influential and connected groups and individuals. Staff then visited potentially selected groups and influentials (Step 5) to confirm the extent of connectivity and influence using Venn diagramming before invitations to participate were offered. Additional detail may be found in the resulting Guide to Community Social Network Mapping (http://irh.org/resource-library/guide-to-social-mapping/). Using good PLA practice, care was taken to record visual outputs, key discussion points, and staff observations after each session. This documentation created one of the data sources for later analysis of the methodology.
Several photos illustrate the mapping process. The visual output of a group listing and ranking exercise in one village (Step 2) is seen in . The number of ‘x’ reflects one group's ranking of the degree of influence and connectedness of each listed group. shows a men's group creating a social map and identifying (listing) influentials in their village (Step 3). Several groups are engaged in mapping in any particular village to ensure representation of different social perspectives. In , a women's group designated as influential receives a follow-up visit by staff (Step 5). During the visit group members are engaged in Venn diagramming to reconfirm their connectivity and influence in relation to other groups in their village.
Figure 2. Results of listing and ranking exercise (Step 2) for one village, presenting women's, men's, and mixed groups by different variables, including levels of connectivity and influence.
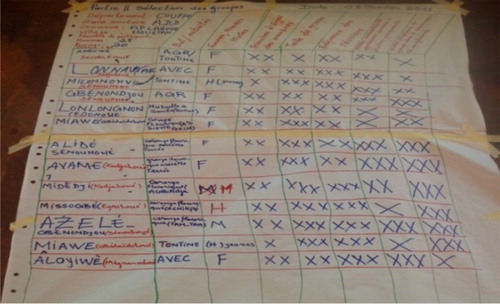
Figure 3. Representative men's group creating a social map and identifying influential individuals (Step 3).

Figure 4. Meeting with an influential women's group to validate connectivity and influence through Venn diagramming (Step 5).

Results
To assess the acceptability, validity, and reliability of the new methodology, we considered the following questions.
(1) Did the community social network mapping methodology demonstrate its acceptability? That is: Were community users fully engaged as participants? Did staff find it easy to use? Did it ensure social equity in participation by key population segments?
Analysis of the reports prepared after each mapping exercise and notes from staff learning reflection discussions indicate that communities were engaged in creating and discussing their visual outputs and there was equitable participation in network analysis discussions by women, men, and youth. People stayed until the end of the exercises. Large numbers of people chose to participate, generally ranging from 15 to 30 people. These reports also indicated that child spacing and family planning were of great interest, indicating the methodology was sufficiently sensitive to avoid controversy in a context with widespread family planning stigma. Staff comments from several mapping reports, below, reflect consistent patterns across villages:
Women, men, elderly, wise ones (‘les sages’) and young people actively participated in different steps of the mapping. (Social network mapping report, Avegodo village)
The pertinence of child spacing is very apparent … these communities live every day with the consequences of births too closely spaced and taboos around discussing family planning in public … (Social network mapping report, Aflantan village)
Feedback from project staff during semi-annual, group facilitated learning reflection discussions indicated that the exercises and discussions were easy to implement and worth the time invested. They allowed data collection while concurrently sensitising communities about a new project. Mapping was an efficient process yielding actionable knowledge that could immediately be used. Moreover, this exercise helped identify informal groups and people influential in the community but often overlooked by village leaders and project staff. Below are several quotes from a learning reflection discussion held in September 2013, in which staff discussed what was working or not working during implementation and observed community changes due to the intervention. The quotes reflect the efficiency of the method and its ability to yield new network information:
Before no one knew how groups were identified. But the mapping criteria made it possible to identify groups … and helped with [creating] an identity of these groups … engagement of the group also gave them a legitimate identity. It made some groups visible that were not visible before. (Staff person, group learning reflection discussion)
Sometimes we are told a village doesn't have any influential or key individuals [at the initial sensitization meeting]. But when facilitators [project staff] enter and do a mapping, they [village people] identify key influentials. (Staff person, group learning reflection discussion)
(2) Did using the methodology result in valid and reliable data to use in establishing the social network intervention base?
Recall that these groups and people were the bedrock of the social network approach. Thus, our primary question while designing this methodology was whether it would lead to valid and reliable results. Did this approach identify influential groups and individuals? Did they effectively diffuse new attitudes and ideas relating to fertility and unmet need? Did the approach yield consistent results across villages?
(2a) Did the community social network mapping methodology lead to identification of the most influential groups and individuals?
To answer this question we review evidence of validity from process and evaluation data to determine which actors were identified by the mapping methodology and compare results with presumed results of social network theory.
One way to answer this question is to understand whom communities judged as influential and connected groups and individuals. Social network theory would posit that social influence is different from government or other formal influence. That is, groups and people with formal community roles may or may not be socially influential, and non-formal leaders and informal groups could also be judged influential. Findings suggest this methodology was valid – influential and connected groups and individuals were identified.
Data from evaluation and group leader reports indicate that groups selected as influential were a mix of formal and informal groups that existed prior to mapping and were engaged in a variety of livelihood and social activities. Less than half the influential groups (43%) were established or linked to NGO efforts. Only one-quarter of influential groups had a health agent as member. For equity reasons, the project mandated that each village have equal proportions of women's, men's, and mixed-sex groups. Mapping reports indicated that group purposes varied by assumed gender roles: most women's groups were organised around food processing and storage, animal husbandry, and sales. Men's groups were engaged in food production, storage, family counselling, sports, and village security. Social network theory would posit that a mix of formal and informal groups should exist. The mapping methodology with its explicit gender and social perspectives should and did yield a range of influential group types.
Data from reports of orientation visits with influentials in five of six arrondissements (about 75 villages) indicate that they were most frequently engaged in farming, while others were involved in small businesses, traditional healing, and religious leadership. No particular age group was noted, ranging from youth to elderly. Monitoring data allow further exploration – the 459 influential leaders were equally divided by sex. Interestingly, few health workers were judged influential. Again, social network theory would posit this variety.
(2b) Were selected actors playing diffusion roles, and how far-reaching was diffusion?
Construct validity was also assessed to determine if the conceptual approach translated well in application, that is, whether the results of this methodology – selected groups and individuals – were diffusing new ideas and attitudes engendered by reflective dialogues, and if so, what was the extent of diffusion. Social change and network theory posit that influential groups would diffuse outward to members’ larger social networks and influential individuals would use their social position as opinion leaders to engage others in conversations about unmet need and family planning, thereby creating general community acceptance of discussion of these ideas, and further break down stigma related to talking about and using family planning.
Our analysis suggests that the results yielded by this mapping methodology are valid. Data from the process, evaluation, cohort in-depth interview data, and staff learning reflection discussions indicate that diffusion is occurring beyond immediate social networks of group members, is spreading widely within networks, and has been sustained over the months the intervention has been operating. This is also corroborated by endline data presented at the end of this section:
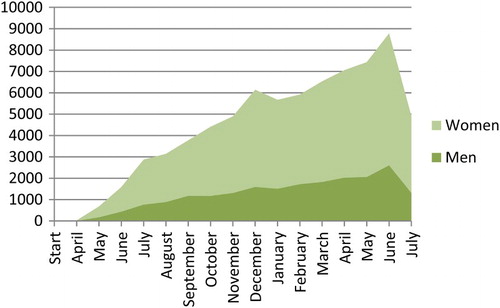
The monitoring system included one indicator to track group diffusion effect. At the end of each group session, members are asked to share with family and friends key themes from the dialogues, such as their thoughts about partner and family support or opposition for family planning use. At the next meeting the group discussion leader asks if members did speak beyond the group. Monitoring data from 90 villages, shown cumulatively in , indicates that group member conversations about Tékponon Jikuagou-related topics are diffusing at a growing rate. When disaggregating these data by sex (not shown), men are diffusing more actively than women.
Figure 5. Number of group members reporting they talked with peers or family after participating in a reflective dialogue session.
Source: Project monitoring system.
Results of the interim evaluation and in-depth interviews from the men and women's cohort (two interview rounds over one year) confirmed that ideas are diffusing beyond individuals directly engaged in reflective discussions. Data from cohort interviews are particularly interesting because participants were selected based on unmet need and social connection status rather than identification as members of an influential group or as an influential within the community. It appears that even individuals not participating in one of the selected groups are reached by the discussions. Illustrated in the quotes, below, the range of reported changes is far-reaching. There are more public discussions about family planning among women and men. Couple communication is changing and increasing. Changes are also occurring in men's and women's perceptions of gender roles and decision-making roles around family planning:
Comments across focus groups indicated that TJ [Tékponon Jikuagou] messaging was reaching people beyond groups. Many catalyzers emphasized that TJ activities brought new participants to groups, who often actively engaged in discussions. Others spoke about how group members diffused messages to their own networks … . One woman catalyzer explained that discussions about couples were particularly popular, saying that, ‘people come because of the stories about couples, and they go to their homes and speak to their neighbours who come also to the following meeting.’ (Interim evaluation report)
I have these new ideas [from child spacing and family planning discussions in one of my groups] that I now discuss with others and I even went to another [neighbouring] village to explain the bases of these methods to them. (Male participant in cohort interview)
Often … [to reach new people] I wait under a tree or more often I go to the market or field where people meet, so they can grow wiser (‘évoluer’) with me. I seize the opportunity to talk with them about FP [family planning]. The only thing is I don't know them personally and we have no prior relationship. (Female participant in cohort interview and Tékponon Jikuagou group member)
Before I didn't understand but now I deeply understand and see that for us to be happy we need to speak about this subject … .Before I would get mad but now I calm myself and we discuss and come to agreement on a point. (Male participant in cohort interview)
Yes, there are changes, because before, our husbands did not know that they could communicate with us, but they are doing it now. (Female participant in cohort interview)
While results suggest diffusion is occurring via influential individuals, the extent of diffusion is not clear from available data. The project made a decision to not collect systematic activity data from influential individuals for management and cost reasons, given the sheer number of influentials (almost 500) and because influentials commit to actions of their choosing and act independently. However, available information indicated diffusion: influential people interviewed for the interim evaluation reported they were acting on their commitments. For example, one traditional healer reported speaking about family planning and women's health to a wide audience in a public setting. Another influential, an older woman, reported she was counselling couples in conflict. During learning reflection discussions, staff also reported that influentials they visited were carrying out the activities to which they had committed.
Preliminary analysis of a household survey (1080 women and 1080 men interviewed at base and end line) using logistics regression, odds ratios, and means testing indicate that the social network package significantly increased discussions on family planning, experience-sharing among women and men, and information-seeking. Normative change had also occurred: significant increases in communication on family planning and in perceptions that women's and men's networks approved of family planning use were observed in women's and men's networks. A significant increase occurred in use of modern contraception and met need for family planning. These population-based findings confirm that the mapping methodology led to valid and reliable results in that influential groups and individuals were critical diffusion actors. Community women were greatly influenced by group participation while for men, reach by influentials was very important. From a gender synchronisation perspective, the survey findings indicate the importance of having a package of network interventions to equalise access to women's and men's networks.
(2c) Were the results consistent across villages?
To answer this question we review evidence of reliability from process and evaluation data to determine whether the methodology yielded similar results across sites. Monitoring data reveal that a wide variety of groups were selected across all villages, posited by social network theory. Likewise, a wide variety of influential types were selected across health sub-zones, with the exception of one zone that reported only formal leaders as influential. Thus, the findings suggest the methodology is reliable, working similarly across villages.
Discussion
Even as countries continue to invest in family planning programmes to improve service and information access, unmet need for family planning in West Africa is growing. In Benin, modern contraceptive use among women in union has slightly increased between 2006 and 2012, from 7% to 8%. Unmet need has grown, from 27% to 33% (Institut National de la Statistique et de l’Analyse Économique, Citation2007, Citation2013). Distrust of modern methods, reliance on traditional methods perceived to have no harmful health effects, and failure to include men's perspectives and other social determinants help to fuel unmet need (Cleland, Harbison, & Shah, Citation2014). This reality argues for new programme paradigms that recognise the many social barriers and facilitating factors operating at different levels – individual, family, community, and society – that prevent people from acting on their desires to space or limit births. A key advantage of a social network paradigm is that it allows cultural realities of how family planning decision-making and action to come into play, rather than imposing outsider perspectives.
The community social network mapping methodology represents a unique and useful tool to generate knowledge that can be used to catalyse a community-based social network intervention. The PLA approach allowed emic, insider knowledge of cultural realities and learning to emerge. Thus, the mapping methodology generated knowledge that was both visual and valid within a project aiming to catalyse a process of social change and development. It ensured that groups and influential individuals not formally recognised but socially influential were recognised, not only by the project but by the community. It challenged outsider knowledge of who was socially influential and best-suited to play a catalyser role for health and family well-being within networks.
Our analysis indicates that this methodology was well accepted by staff and involved communities in a meaningful way. Engaging community members in a participatory and visual inventory and analysis of influential groups and people created a more democratic and open process to analyse influence and connectivity within their communities and made visible unseen influential actors, leading to enhanced community understanding of its own social context. The mapping approach led to valid and reliable information upon which to base a social network intervention. The appropriate groups and people were selected by communities as influential and diffusion impact is evident. How valid and reliable the methodology was in selecting influentials could only be partially answered with available data. Preliminary endline survey findings confirmed that selected groups and individuals were important diffusion actors.
In terms of intervention research, this paper reports rigorous use of programme data to provide real-time answers to questions about the acceptability, validity, and reliability of an intervention tool to identify socially connected and influential individuals and groups. Although the context did not allow an experimental design to address these questions, systematic analysis and triangulation of rich, existing project data provided robust evidence to guide implementation. Rather than waiting for end-of-pilot results, this approach allowed timely checks on the mapping process and assessed how well it identified influential network actors as it was being rolled out.
In terms of practice, this experience highlights the importance of a learning agenda as part of project monitoring and evaluation. Regular check-in points created space to review data, assess progress, raise new questions, and seek responses. Because project monitoring, evaluation, and small evaluation studies were embedded in the implementation process, data were readily available for decision-making and truth or reality checks. An integral part of the monitoring, learning, and evaluation system, the mapping methodology not only collected information but fostered learning among staff and within communities, and resulted in democratic action that effectively laid the groundwork for social change processes.
Finally, the participatory visual methodology has contributed to grounded theory development of the project's change theory. We learned about what constitutes influential networks and network actors more broadly, and in the process challenged some commonly held assumptions about influence. Most of the influentials selected had nothing to do with health or family planning in their professional lives. Health providers themselves were rarely part of influential groups and infrequently selected as an influential individual. Although not tested, we postulate that if we had been content to focus on key informant interviews and focus group discussions with formal leaders and service providers to identify influential network actors, it would have been unlikely that all selected groups and individuals judged influential by communities would have been identified and selected. As the social network intervention package goes to scale under different conditions, we will be cognizant of distinguishing influential social actors from project-created or government-created actors that may or may not be socially influential in the community's eyes. These findings have more general implications for community-based health programmes aiming to address normative and behaviour change. Looking forward, we hope to test this theoretical assumption under study conditions using social network analysis.
Disclosure statement
No potential conflict of interest was reported by the authors.
ORCID
Susan Igras http://orcid.org/0000-0001-9836-9479
Mariam Diakité http://orcid.org/0000-0002-0671-0180
Rebecka Lundgren http://orcid.org/0000-0002-9607-5722
Additional information
Funding
References
- Akinfeleye, R., Charles, J. O., & Omideyi, A. K. (1997). Sociocultural factors affecting attitude and behavior regarding population and family life issues in Nigeria. Lagos: UNFPA. Retrieved from http://snap3.uas.mx/RECURSO1/unfpa/data/docs/unpf0063.pdf
- Behrman, J. R., Kohler, H. P., & Watkins, S. C. (2002). Social networks and changes in contraceptive use over time: Evidence from a longitudinal study in rural Kenya. Demography, 39(4), 713–738. doi: 10.1353/dem.2002.0033
- Bongaarts, J., & Bruce, J. (1995). The causes of unmet need for contraception and the social content of services. Studies in Family Planning, 26(2), 57–75. doi:10.2307/2137932
- Boulay, M., Storey, J. D., & Sood, S. (2002). Indirect exposure to a family planning mass media campaign in Nepal. Journal of Health Communication, 7(5), 379–399. doi: 10.1080/10810730290001774
- Boulay, M., & Valente, T. W. (1999). The relationship of social affiliation and interpersonal discussion to family planning knowledge, attitudes, and practices. International Family Planning Perspectives, 25(3): 112–118 & 138.
- Brewer, N. T., & Rimer, B. K. (2008). Perspective on health behaviors: Theories that focus on individuals. In K. Glantz, B. K. Rimer, & K. Viswanath (Eds.), Health behavior and health education: Theory, research and practice (pp. 149–162). San Francisco, CA: Jossey Bass.
- Broadhead, R., Heckathorn, D. D., Weakliem, D. L., Anthony, D. L., Madray, H., Mills, R. J., & Hughes, J. (1998). Harnessing peer networks as an instrument for AIDS prevention: Results from a peer-driven intervention. Public Health Reports, 113(1), 42–56. Retrieved from http://www.ncbi.nlm.nih.gov/
- Buesseler, H., & Diakite, M. (2013). Premiers résultats de l’évaluation rapide des obstacles au recours à la planification familiale. Washington, DC: Georgetown University Institute for Reproductive Health. Retrieved from http://irh.org/wp-content/uploads/2013/11/TJ_Benin_Formative_Research_Report_FR.pdf
- Burk, W. J., Steglich, C. E., & Snijders, T. A. (2007). Beyond dyadic interdependence: Actor-oriented models for co-evolving social networks and individual behaviors. International Journal of Behavior Development, 31, 397–404. doi:10.1177/0165025407077762
- Cleland, J., Harbison, S., & Shah, I. H. (2014). Unmet need for contraception: Issues and challenges. Studies in Family Planning, 45(2), 105–122. doi:10.1111/j.1728-4465.2014.00380
- Curtis, S. P., & Edwards, A. (1995). HIV in UK prisons: A review of seroprevalence, transmission and patterns of risk. International Journal of Sexually Transmitted Disease and AIDS, 6(6), 387–391. doi:10.1177/095646249500600602
- Ferlander, S. (2007). The importance of different forms of social capital for health. Acta Sociologica, 50(2), 115–128. doi: 10.1177/0001699307077654
- Fixen, D. L., Naoom, S. F., Blase, K. A., Friedman, R. M., & Wallace, F. (2005). Implementation science: A synthesis of the literature. Tampa: University of South Florida, Louis de la Parte Florida Mental Health Institute, National Implementation Research Network (FMHI publication 231).
- Gayen, K., & Raeside, R. (2007). Social networks, normative influence and health delivery in rural Bangladesh. Social Science & Medicine, 65, 900–914. doi:10.1016/j.socscimed.2007.03.037
- Golafshani, N. (2003). Understanding reliability and validity in qualitative research. The Qualitative Report, 8(4), 597–607. Retrieved from http://www.nova.edu/ssss/QR/QR8–4/golafshani.pdf
- Greene, M. E., & Biddlecom, A. E. (2000). Absent and problematic men: Demographic accounts of male reproductive roles. Population and Development Review, 26(1), 81–115. Retrieved from http://www.jstor.org/stable/172453 doi: 10.1111/j.1728-4457.2000.00081.x
- Heaney, C. A., & Israel, B. A. (2008). Social networks and social support. In K. Glantz, B. K. Rimer, & K. Viswanath (Eds.), Health behavior and health education: Theory, research and practice (pp. 189–207). San Francisco, CA: Jossey Bass.
- Institut National de la Statistique et de l’Analyse Économique (INSAE). (2007). [Bénin] et Macro International Inc. 2007: Enquête Démographique et de Santé (EDS-III) - Bénin 2006. Calverton, MD: Institut National de la Statistique et de l’Analyse Économique et Macro International.
- Institut National de la Statistique et de l’Analyse Économique (INSAE). (2013). et ICF International, 2013. Enquête Démographique et de Santé du Bénin 2011--2012. Calverton, MD: INSAE et ICF International.
- Jackson, M. O., & Yariv, L. (2005). Diffusion on social networks. Économie publique, 16 (2005/1), mis en ligne le 21 avril 2006. Retrieved October 13, 2012, http://economiepublique.revues.org/1721
- Kim, D. A., Hwong, A. R., Stafford, D., Hughes, A., O'Malley, J., Fowler, J. H., & Christakis, N. A. (2015). Social network targeting to maximise population behaviour change: A cluster randomised controlled trial. The Lancet. doi:10.1016/S0140-6736(15)60
- Kohler, H. P., Behrman, J. R., & Watkins, S. C. (2001). The density of social networks and fertility decisions: Evidence from South Nyanza District, Kenya. Demography, 38(1), 43–58. doi: 10.1353/dem.2001.0005
- Lobb, R., & Colditz, G. A. (2013). Implementation science and its application to population health. Annual Review of Public Health, 34, 235–251. doi:10.1146/annurev-publhealth-031912-114444
- Mosha, I. H., & Ruben, R. (2013). Communication, knowledge, social network and family planning utilization among couples in Mwanza, Tanzania. African Journal of Reproductive Health, 17(3), 57–69. Retrieved from http://www.ajrh.info/vol17_no3/17_3_article6.pdf
- Neaigus, A. (1998). The network approach and interventions to prevent HIV among injection drug users. Public Health Reports, 113(Suppl. 1), 140–150. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1307736/
- Paz Soldan, V. A. (2004). How family planning ideas are spread within social groups in rural Malawi. Studies in Family Planning, 35(4), 275–290. doi:10.1111/j.0039-3665.2004.00031
- Peters, D. H., Adam, T., & Alonge, O. (2013). Implementation research: What it is and how to do it. British Medical Journal, f6753, 1–7. doi:10.1136/bmj.f6753
- Rashotte, L. S. (2006). Social influence. In G. Ritzer & J. Michael Ryan (Eds.), The Blackwell encyclopedia of sociology (Vol. IX, pp. 4426–4429). Oxford: Blackwell.
- Reason, P. (2006). Choice and quality in action research practice. Journal of Management Inquiry, 15(2), 187–203. doi:10.1177/1056492606288074
- Smith, K. P., & Christakis, N. A. (2008). Social networks and health. Annual Review of Sociology, 34, 405–429. doi:10.1146/annurev.soc.34.040507.134601
- Valente, T. (2003). Social network influences on adolescent substance use: An introduction. Connections, 25(2), 11–16. Retrieved from http://www.insna.net/PDF/Connections/v25/2003_I-2–3.pdf
- Valente, T. W., Watkins, S. C., Jato, M. N., Van Der Straten, A., & Tsitsol, L. P. M. (1997). Social network associations with contraceptive use among Cameroonian women in voluntary associations. Social Science & Medicine, 45(5), 677–687. doi: 10.1016/S0277-9536(96)00385-1
- Weeks, M. R., Clair, S., Borgatti, S. P., Radda, K., & Schensul, J. J. (2002). Social networks of drug users in high-risk sites: Finding the connections. AIDS and Behavior, 6(2), 193–206. doi:1090-7165/02/0600-0193/0